
Abstract
The neural mechanisms involved in motor timing are subcortical, involving mainly cerebellum and basal ganglia. However, the role played by these structures in predictive motor timing is not well understood. Unlike motor timing, which is often tested using rhythm production tasks, predictive motor timing requires visuo-motor coordination in anticipation of a future event, and it is evident in behaviors such as catching a ball or shooting a moving target. We examined the role of the cerebellum and striatum in predictive motor timing in a target interception task in healthy (n = 12) individuals and in subjects (n = 9) with spinocerebellar ataxia types 6 and 8. The performance of the healthy subjects was better than that of the spinocerebellar ataxia. Successful performance in both groups was associated with increased activity in the cerebellum (right dentate nucleus, left uvula (lobule V), and lobule VI), thalamus, and in several cortical areas. The superior performance in the controls was related to activation in thalamus, putamen (lentiform nucleus) and cerebellum (right dentate nucleus and culmen—lobule IV), which were not activated either in the spinocerebellar subjects or within a subgroup of controls who performed poorly. Both the cerebellum and the basal ganglia are necessary for the predictive motor timing. The degeneration of the cerebellum associated with spinocerebellar types 6 and 8 appears to lead to quantitative rather than qualitative deficits in temporal processing. The lack of any areas with greater activity in the spinocerebellar group than in controls suggests that limited functional reorganization occurs in this condition.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
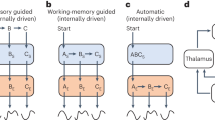
Many everyday skills, such as sports, video-gaming, and the operation of motor vehicles or machinery require precise timing [1, 2]. Neurological disorders that disrupt motor timing lead to dysmetric or inaccurate movements [3, 4]. While there is a general consensus that the neural mechanisms involved in motor timing are mainly subcortical [5–8], the cerebellum and basal ganglia in particular, there is a debate as to the relative role played by these structures and their interaction with cortical regions.
Gordon Holmes suggested that the disturbance of voluntary movement in patients with lesions of the cerebellum was due to a “delay in cortico-spinal innervation” [4]; in other words, the cerebellum might regulate motor timing. Theoretical support for such a concept came from the idea that parallel fibers of the cerebellum provide delay lines for converting spatial patterns into temporal signals [9]. Since then, this framework had been developed and modified by many groups, but the exact role of the cerebellum in the timing process is still elusive [10–12]. Based largely on recent neuropsychological and neuroimaging studies, there is evidence that the cerebellum is involved in a wide variety of cognitive and perceptual activities, including temporal processing [10, 11, 13–17]. The other subcortical structures considered to play an important role in timing are the basal ganglia particularly during longer temporal intervals [15, 18] but also during shorter intervals in the milliseconds to seconds range [19–21]. However, there is no strong evidence that unequivocally supports the role of either cerebellum or basal ganglia in the control of timing. In addition, there are many instances of counter-intuitive results. For example, the increase in temporal variability that one expects following damage to a structure involved in the control of timing was not seen during perception and production tasks in patients with cerebellar disease [22]. Furthermore, both the cerebellum [23–25] and the basal ganglia [26] have been associated exclusively with the perception of short temporal intervals.
One potential explanation that might resolve the apparently conflicting evidence concerning the basal ganglia and cerebellum is that there are two functionally distinct timing circuits that can be dissociated [5, 27]: (1) an automatic timing system that works in the millisecond range used in discrete-event (discontinuous) timing and involving the cerebellum, and (2) a continuous-event, cognitively controlled timing system that requires attention and involves the basal ganglia and related cortical structures [12, 17, 28]. Other possibilities are that the control of timing might be dependent on the interaction between these two subcortical structures [25, 29] or may not be localized to specific brain areas but be processed locally in the prefrontal and parietal cortex in a task-dependent way [28, 30].
The goal of the current functional magnetic resonance imaging (fMRI) study was to examine the role of cerebellar dysfunction in a particular type of cognitive process that engages predictive timing behavior. To do so, we examined human subjects with “lesions” of the cerebellum due to spinocerebellar ataxia (SCA) types 6 and 8, a genetically and clinically well-defined with a predominantly cerebellar syndrome [31], and compared both their performance and functional activation to that of normal subjects during a predictive motor timing task that involved interception of a moving target [32, 33].
The behavioral task was specifically designed so that the elemental abnormalities of motor output in subjects with cerebellar disease would not interfere with motor prediction. This task required for successful performance both the accurate perception of target information and a precise predictive motor response. The motor response was a simple finger press, thus avoiding the interpretative difficulties associated with whole limb movements. We expected different activity patterns in control compared to the cerebellar subjects, especially in the area of the cerebellum and in the associated projection regions in basal ganglia and cerebral cortex, which would be the signature of a deficit produced by the motor timing component of the main task.
Materials and Methods
Subjects
Twelve healthy subjects (age-matched controls) with no neurological or other health problems (five females, mean age 51.5 years, SD 12.5 years) and nine subjects (five females, mean age 49.1 years, SD 10.7 years) with spinocerebellar ataxia (SCA) were recruited to participate in the study. The patients (Table 1) were recruited from the Ataxia Outpatient Clinic at the University of Minnesota and were diagnosed as having a genetically defined SCA type 6 (n = 5) or type 8 (n = 4). SCA types 6 and 8 are clinical syndromes with predominant involvement of the cerebellum that are well characterized both clinically and genetically [31]. Prior to testing, the clinical status of the patients was scored on the International Cooperative Ataxia Rating Scale of the World Federation of Neurology (WFN Scale) [34]. All subjects were right-handed [35] and did not have clinically apparent depression on the Montgomery and Asberg Depression Rating Scale [36]. None of the subjects had a history of color blindness or evidence of cognitive decline. All the subjects were remunerated for their participation after giving informed consent. The study was approved by the Institutional Review Board of the University of Minnesota.
Behavioral Task
We used the same behavioral task as reported elsewhere [32, 33]. Our participants performed a motor reaction timing task in which they had to respond by pressing a button to intercept a circular target that moved from left to right on a computer screen. Once the button was pressed, it launched a yellow circular object (“fireball”) from the lower right of the screen that traveled upward with constant speed (20.0 cm/s) to intercept the moving target. The objective of the task was to launch the ball at the optimal time in order to hit the moving target: the interception zone was always in the same position on the screen. If the subject successfully intercepted the target, both the fireball and target balls appeared to explode (the red dots). If the subject failed to intercept the target, no explosion animation occurred. The participants were seated 60 cm in front of a computer monitor. The diameter of the target was 1 cm, and the diameter of the “fireball” was 0.3 cm. The target was launched from the left side of the screen such that it corresponded to a ballistic launch at three different angles of movement relative to the horizontal plane of the screen (0°, 15°, and 30°) and followed a linear trajectory (the dotted yellow lines in Fig. 1a, not visible to the subjects) toward the interception zone. The moving target could have one of three different movement types: constant velocity, deceleration, and acceleration; and three different travel speeds: slow (complete travel time across the screen 3.5 s), medium (complete travel time across the screen 3.0 s), and fast (complete travel time across the screen 2.5 s). The target movement was thus characterized by any combination of the three variables (type, speed, angle) giving a total of 27 separate potential target movement conditions. In that which follows, we will refer to this behavioral task as the “interception task”.

The performance of the SCA and control subjects in both control (CC1) condition and predictive task (interception)
For the actual experiment, blocks of trials were organized on the basis of movement type (constant, acceleration, deceleration) within which the combination of speed and angle was randomized. There were six blocks of trials, yielding two for each movement type, containing 54 trials bounded by 20 s break periods. The duration of the interception task was 18 min and 27 s. Each combination of variables was presented six times during every block, corresponding to 12 of a particular trial type (movement, speed, and angle) during the entire experiment. Before the task, the subjects were given one block to practice the task (PT). This practice block had 54 trials; each combination of a particular trial type was presented twice. The duration of single PT was 3 min and 26 s.
We also included cross-hair (CC1) condition requiring no prediction, where subjects could “hit” the fireball instantaneously. In this case, a cross-hair was presented in the interception zone, in the upper right side of the screen. The target ball passed through this area regardless of the orientation of its trajectory (angle), speed, and type of movement. Subject's task in this condition was to push the fire button at the moment the ball was in the interception area, as close as possible to the center of the cross-hair. Whenever this instantaneous interception was successful, an explosion animation occurred. Two blocks of 54 trials were presented in this condition.
Analysis of Behavioral Data
Given that the dependent variable in each individual trial is binary (Correct vs. Incorrect, Hit vs. Error), we could not use directly the parametric methods to analyze the behavioral results. In addition, the errors could be of two types: “early errors” (when subjects pressed the fire button too early (before the target arrived in the hitting area) and “late errors” (when subjects reacted too late). As a consequence, we assigned the dependent variable in each trial into one of three categories (early errors, hits, or late errors). Nevertheless, in order to be able to employ parametric methods, we first performed the following computations: first, for all the trials in each of the six blocks of the task, we calculated the count for each category, then we computed the percentage of each type of trial in each block (based on speed and movement type) out of the total number of trials per block (54 trials), and we averaged these values for each subject. These new dependent variables are likely to be normally distributed given that they now can take values anywhere in the 0 to 100 interval. However, in order to check the normality of the distributions, we performed Kolmogorov–Smirnov tests. These tests showed that the distribution of values in each of these variables was not significantly different than the normal distribution (all p > 0.05), thus warranting the use of parametric methods for the additional analyses. Then, we employed a mixed general linear model (GLM) with the type of trial (early errors, hits, and late errors) as repeated, within-subject factors and the group (control group vs. SCA group) as a between-subject factor. Post-hoc pairwise comparisons were done using Sidak tests which account for and adjust the p level based on the number of independent comparisons. To further investigate to what extent the response strategy was based on time estimation, we considered the relationship between the temporal window of the interception (the time interval during which the fireball could hit the target in each type of trial; this window was narrower for fast speed trials, for example) and the hit ratio (number of hits divided by the total number of trials of a given type). One would expect to observe a positive correlation between the amount of time during which it was possible to successfully intercept the target and the hit ratio; the greater this window width, the greater the chances for success. In addition, the magnitude or the strength of this correlation should reflect the participants' ability to predict and react within the required time interval. A separate analysis was performed by splitting the healthy subjects group in two equal subgroups based on their median performance (“poor” performers, with a hit ratio less than the median; “good” performers, with a hit ratio greater than the median). Here, we employed the same GLM model as that specified above. The goal of this analysis was to test whether the performance profile of the “poor” but healthy performers differed significantly from that of the SCA group.
Imaging Parameters of the fMRI Experiment
A 3 Tesla Whole Body MR System (MAGNETOM Trio, Siemens Medical Systems, Erlangen, Germany) was used for image acquisition. Before the fMRI run, 144 or 160 (depending on the subject's head width) FLASH structural images were acquired in slices of 1 mm thickness in sagittal plane (256 × 256 mm) yielding a spatial resolution of 1 × 1 × 1mm for the anatomical volume. The imaging parameters of the anatomical sequence were: time to repetition (TR) and time to echo (TE)—13 and 4.92 ms, respectively, with a flip angle (FA) of 25°. Then, whole brain fMRI was performed using an echo-planar imaging sequence measuring blood oxygenation level dependent (BOLD) signal. A total of 30 functional slices per volume were acquired for all subjects in all runs. These slices, which were acquired in transversal plane with a 30° positive tilt around Y-axis (in order to cover the whole brain and the cerebellum), in ascending order and interleaved, had a thickness of 3 mm, an inplane resolution of 3 × 3 mm (matrix size 64 × 64), in a field of view of 192 × 192 mm, with a 1-mm gap between them in order to avoid cross talking. Therefore, the spatial resolution of functional images was 3 × 3 × 3 mm. A complete scan of the whole brain was acquired in 2,000 ms (TR); the flip angle was 75°, TE = 30 ms. A total number of 556 volumes were acquired during the functional run.
Preprocessing of fMRI Data
Brain Voyager QX (Brain Innovation B.V., Maastricht, the Netherlands) software was used for fMRI data preprocessing and analysis. The functional bi-dimensional images of every subject were preprocessed to correct for the difference in time slice acquisition (slice scan time correction). In addition to linear detrending, a high-pass filter of three cycles per time course (frequency domain) was applied to the corrected 2D slices. Then, the functional series was preprocessed to correct for possible motion artifacts in any plane of the tridimensional space and to ensure that the movements in any plane did not exceed 3 mm. Later, these functional images were then used to reconstruct the 3D functional volume for every subject and every run, which was aligned with the corresponding 3D anatomical volume, and both were normalized to standard Talairach space [37]. Spatial smoothing using a Gaussian kernel at 7 mm full width at half maximum was applied to the 3D functional data.
Analysis of fMRI Data
We used a rapid event-related block design for our experiment. Each behavioral event in both control and predictive tasks (2.5, 3.0, or 3.5 s long corresponding to the complete travel time of the moving target across the screen) was classified according to the behavioral outcome in that particular trial (hit, early, and late error). These predictors were entered as fixed factors in single subject GLM; then, the parameter estimates of this GLM model were subsequently entered into a second level of analysis corresponding to a random-effect GLM model that was used for group analysis [38]. The statistical parameters of this latter model were estimated voxel-wise for the entire brain, and activation maps were computed for various contrasts between the predictors. For each condition, separately, we used two main contrasts of interest: (1) the contrast between hits and errors, common for all subjects (no differentiation between the two groups) and (2) the difference between control group and SCA group regarding the contrast between hits and errors. When displaying the activation maps, we used the false discovery rate (FDR) as a criterion for the minimum statistical value (t test) in each voxel and a minimum cluster size of 150 adjacent significant voxels (1 × 1 × 1 mm). In the second stage of the analysis, we analyzed the BOLD signal in cerebellar and striatal regions of interest (ROIs) obtained as a result of these contrasts. Here, similar to the behavioral analysis, we split the group of control subjects in two equal subgroups based on their median general performance into “poor performers” and “good performers”. In this way, we believe that we were be able to determine whether the differences observed in an ROI are determined solely by the classification of subjects in the two main groups (control group vs. SCA group) or whether they arise from a combination of the group taxonomy with performance. This detailed ROI analysis was done using a one-way analysis of variance (ANOVA) with group as independent factors and the BOLD signal expressing the contrast of interest averaged over all voxels in the ROI as dependent measure. To this end, we employed the SPSS (Statistical Package for Social Sciences, SPSS Inc., Chicago, USA) software.
Results
Behavioral Results
The performance of the SCA subjects in both the control condition and predictive task (percentage of hits) was worse than that of the controls, and this was confirmed by GLM analysis [F 1,19 = 26.06, p < 0.001, for control condition and F 1,19 = 37.49, p < 0.001 for predictive task] (Fig. 1). When comparing the two groups on their performance in the main experimental task as a function of trial type (early errors, hits, late errors), the GLM revealed a significant effect of the type of trial (F 2,38 = 5.46, p < 0.001) and a significant interaction between the type of trial and the group (F 2,38 = 22.54, p < 0.001) (Fig. 2a). Pair-wise comparisons revealed that the interaction effect arose from different performance patterns observed within each group as a function of trial type (early error, hit, late error): in the control group, the percentage of hits was greater than that of either the early or late errors (p < 0.001), whereas in the SCA group, the hit percentage was smaller than that of the early error (p < 0.01). It has to be noted that while the difference in percentage of hits and early errors was significant in both groups, the direction of these differences was opposite: healthy controls had more hits than early errors, with the reverse pattern seen among SCA patients.

a Mean percentage of early errors, hits, and late errors out of all trials for both groups during interception task. Error bars reflect the standard error of the mean (SEM). b The correlation between temporal window width (time interval to launch the cannon ball in order to successfully hit the target) and the hit ratio for both groups. For controls, the correlation coefficient was significant r = 0.408, p < 0.001, (N = 108—9 points per subject, corresponding to different temporal window widths). For the SCA group, the correlation was not significant, r = 0.123, p = ns, (N = 81); suggesting again that for these subjects the temporal estimation was impaired
Even within the healthy controls, there was a broad range of performance. As stated in the “Materials and Methods” section, we split the subjects in the control group into “poor” and “good” performers based on whether the hit ratio for the entire session (all hits divided by total number of trials) of a given participant was below or above, respectively, the median hit ratio for the entire group. When repeating the same analysis, but this time for patients and the two subgroups of healthy controls (“poor” and “good” performers), we observed a significant difference among the three groups regarding the percentage of hits (F 2,18 = 55.73, p < 0.001) and also a significant interaction effect between the group and type of trial (F 4,36 = 21.02, p < 0.001). Pair-wise analyses performed using Sidak tests revealed that actually the difference between the two subgroups of healthy controls originated from differences in the level of performance (which is expected given that they were separated based on the percentage of hits) and not from a different distribution of early and late errors (p > 0.05). The SCA subjects, however, were significantly different (p < 0.05) from both subgroups regarding their early errors and only from the “good” performers regarding the late errors. Again, regardless of the division of healthy controls based on their performance, these individuals could be differentiated from the SCA subjects in terms of the distribution of hits and early errors.
Figure 2b shows the correlation between the temporal window width needed for a successful trial and the hit ratio in the interception task and for both groups. For controls, the correlation coefficient was r = 0.408, p < 0.001, (N = 108). For the SCA group, the correlation was not significant, r = 0.123, p = ns, (N = 81), which suggests that these subjects were not able to adjust their performance to optimize performance under the task conditions, therefore, their estimation of time was impaired. Taken together, these results suggest that the two groups differ in terms of their anticipatory strategy. As a consequence, we decided to use only the contrast between hits and early errors when analyzing the imaging results for two reasons. First, the hits/early error contrast was the behavioral measure for which the groups showed the greatest difference. Second, both of these types of trials (hits and early errors) involve prediction and anticipation, the difference being that in one case, the process was successful and in another not, whereas for the late errors, it is hard to determine what led to the error (e.g., lack of attention, bad prediction, no response etc.).
Imaging Results: Commonalities Between the SCA Group and Control Group
We performed the contrast HITS>EARLY ERRORS for all subjects, control, and SCA groups together. In the control condition, we did not find any cerebellar or striatal area that was significantly activated by this contrast. In the predictive task however, the same contrast revealed a set of regions including a network of cortical areas, the thalamus, and several foci with the cerebellum (Table 2); yet the basal ganglia were not activated. Because our main focus was on the cerebellum, we therefore defined three regions of interest based on this contrast: right dentate nucleus, left uvula (lobule V), and lobule VI for further detailed BOLD signal analysis with respect to the different subject groups (Fig. 3). In each of the ROIs, there was more activity during hits compared to early errors (p < 0.05; the red stars in the graphs of Fig. 3) in each of the groups with the exception of the poor performers group in the dentate nucleus.

Cerebellar regions activated by the contrast [Hits>Early Errors] in all subjects, regardless of their group (images in the left column) and the corresponding change in the average BOLD signal in each group (the bar graphs to the right of each region). The statistical threshold for displaying the activation map was: a cluster size of minimum 100 adjacent significant voxels and a minimum t (20) value of 4.54 (p < 0.0002; FDR corrected). The red stars in the bar graphs indicate that the difference between Hits and Early errors was significantly greater than zero (baseline) for a given group (one star, p < 0.05; two stars, p < 0.01); the black star indicates a significant difference (p < 0.05) for this contrast between groups
A one-way ANOVA analysis performed in each ROI revealed that the three groups were significantly different from one another for the contrast HITS>EARLY ERRORS only in left cerebellar lobule V [F 2,18 = 5.09, p < 0.05]. In the remaining two ROIs, there was no significant difference among the groups [F 2,18 = 2.79, p = 0.08—dentate nucleus; F 2,18 = 2.27, p = 0.13—culmen]. Several conclusions can be drawn based on these results: (1) in all ROIs, the difference in BOLD signal between hits and early errors trials was significant for both SCA patients and the good performers and (2) when comparing only the good performers subgroup with the SCA patients we observed significantly higher difference between hits and early errors among the healthy controls than among the patients (significance for Sidak tests, in culmen—p = 0.056; in all other ROIs—p < 0.05].
Imaging Results: Differences Between the SCA and Control Group
We next proceeded to test the neural basis of the interaction effect between group and performance. This analysis uncovered a large network of areas that were more active in the hits versus early errors contrast in the control than in the SCA subjects (Table 3). These regions comprised an extensive network (Table 3) involving the cortex, thalamus (ventrolateral nucleus), putamen (lentiform nucleus), and cerebellum (right dentate nucleus and culmen—lobule IV). Again, we focused on the cerebellum and basal ganglia because our primary goal was to determine the parts of the cerebellum that were essential for correct performance in the task. We selected three ROIs from this network for further detailed analysis (Fig. 4): the putamen and the two cerebellar regions. A one-way analysis of variance revealed that in each of these ROIs, there was a significant overall difference among the three groups regarding the contrast HITS>EARLY ERRORS (all p < 0.05). Pair-wise comparisons (Sidak test, p < 0.05) among the three groups revealed that in all ROIs, the overall difference between groups was in fact explained by a significant difference between the good performers subgroup and the SCA group (black stars in Fig. 4).

Cerebellar and striatal regions activated by the contrast [Hits>Early Errors] significantly more in healthy than in cerebellar subjects (images in the left column) and the average BOLD signal change in these ROIs for healthy control subjects (good and poor performers) and all patients. In the bar graphs, the black stars indicate significant differences (one star, p < 0.05; two stars, p < 0.01) between various subgroups
Discussion
The behavioral task we used focused on prediction and tested the ability of subjects to integrate a prediction about the perception of target movement with a precise predictive motor response and in that sense was similar to naturalistic everyday behaviors that require the integration of sensory and motor prediction such as in catching, shooting, playing tennis, and in many other sports. The concept that the cerebellum may be involved in prediction is not new [39]. The question remains, however, as to what type of prediction the cerebellum may facilitate and under what circumstances [40]. Based on our results, with respect to our recently published behavioral study [33], we can draw the following points: (1) cerebellum is essential for the task, (2) SCA 6 and 8 have quantitative not qualitative effects on temporal processing, (3) there is no evidence of compensatory reorganization. The involvement of the cerebellum in predicting the sensory consequences of motor commands [11, 39–43] makes it the ideal structure to learn or store internal models of motor behavior [44, 45]. The cerebellum also seems to be engaged in the forward-modeling or prediction of purely perceptual events [29]. However, the prediction of perceptual events is rarely an end in itself and is often part of a greater goal that involves motor behavior.
Correct timing is the essence of our behavioral task, and the cerebellum is thought to be important in a variety of time-based behaviors extending from the sensory to the motor domain including the discrimination of temporal intervals [13, 14, 46, 47], phoneme discrimination [48], timing during conditioning tasks [49, 50], anticipatory adjustments of the limb segments [51], and rhythmic tapping [52]. Recently, a distinction has been made between the role of the cerebellum in rhythmic time-based motor behaviors that are continuous and those that are discontinuous or “event-based” [17]. The idea is that the cerebellum is engaged when one has to time the interval between successive events in motor behavior that have a distinct beginning and end but not during continuous drawing, for example.
Besides the cerebellum, thalamic activation was seen in our results. Although common activation for both groups was in mediodorsal thalamus, the higher activation with regards to the good performance of the task was localized in the ventrolateral thalamus. This part of the thalamus was earlier associated with explicit timing [53], whereas the medial thalamus is considered important for recognition memory [54].
Basal ganglia (namely putamen) were active only when we looked at differences between the groups, but not when we looked at commonalities. Although the cerebellum may have been the pivotal component in the network of areas responsible for correct performance in the interception task, our analysis suggests that the basal ganglia also needed to be engaged. The role of the cerebellum and basal ganglia in timing has often been presented as dichotomous with each being tuned for different time scales [5, 27]. Other studies have stressed the importance of the distinction between the cerebellum as the neural basis for timing in the motor domain and the fronto-striatal network responsible for timing during cognitive behavior [12, 55, 56]. Our results indicate that even within the motor domain, both the basal ganglia are essential for performance. In a similar vein, the time scale of the intervals in our behavioral task would seem to straddle those typically regarded as the exclusive province of either the cerebellum or basal ganglia.
One important conclusion is that we did not find areas where the activation was higher in the SCA than in controls. This suggests that, unlike the cerebral plasticity or reorganization following a traumatic event (e.g., stroke, lesion) [57], the SCA (which is an atrophy) does not lead to a qualitative reorganization of the brain activity, where the patients will use a given area significantly more than control subjects, to compensate for the functional impairment. Our results showed that the difference we observed were quantitative (i.e., smaller activation for patients, in the same regions) and not qualitative (different regions for the two groups). This implies that atrophy, in contrast to a lesion, is less likely to lead to a qualitative reorganization of the cerebral activity.
There are several potential limitations of our study. One might argue that brain structures and systems outside the cerebellum may also be affected in SCA [31] and thus confound the interpretation of our results. While it is impossible to completely discount this objection, the phenotypes in the subjects we studied (SCA 6 and 8) are generally regarded as having a rather pure cerebellar syndrome [31]. There are some alternative interpretations of our results which may not be directly connected with sensorimotor integration and time prediction. The first is that a disruption of eye movement control in the SCA group accounted for poor task performance. Although eye movements may be disrupted in subjects with damage to the cerebellum, we have previously shown that abnormalities in gaze shifting cannot explain the timing and nature of interception deficits reported here because there was no correlation between the oculomotor component of ICARS score and the performance of the SCA subjects [32]. These findings are reinforced by data from other studies in subjects with cerebellar disease in which examining smooth pursuit tasks in subjects with cerebellar disease, in which the eye-movement abnormalities were not sufficient to account for the other motor, perceptual, or attentional deficits [58, 59]. The second possibility is that deficits in movement coordination known to be present in subjects with disease of the cerebellum affected performance. Again, we think this unlikely, because the motor output in the behavior task was minimal, a single button press across a single joint.
Cognitive and executive impairment are prominent in spinocerebellar patients with extracerebellar pathology (spinocerebellar ataxia 1, 2, and 3); however, mild cognitive and executive impairments were observed in both spinocerebellar ataxia 6 and 8—our sample—[60–62]. What is interesting is that more than other categories, these patients have trouble in theory of mind tasks, such as recognition and attribution of social and emotional responses [63]. In our experiment, we found that these individuals have troubles in predicting target's trajectory, resulting in an increased number of early errors. Taken together, these findings suggest that impaired prediction processes requiring precise motor output may represent a diagnosis signature of these types of patients. Once this pattern is confirmed by future studies, using motor prediction tasks may become part of the differential diagnosis procedure aimed to differentiate between various cerebellar ataxia types.
In conclusion, our data showed that the differences between control group and cerebellar group we observed were quantitative; smaller activation for cerebellar patients and in the same regions; and not qualitative—different regions for the two studied groups. This implies that atrophy itself, in contrast to a lesion, is less likely to lead to a qualitative reorganization of the cerebral activity, probably because the atrophied region likely still plays a functional role [64]. Our conception of cerebellar function is very much in keep with the suggestion of Holmes [4] that the cerebellum does not act alone but rather “primes” other brain areas in regulating the appropriate timing of muscular contraction. This conception is enhanced by our observations where the automatic timing system used in discrete-event (discontinuous) timing and involving the cerebellum, and the continuous-event, cognitively controlled timing system that requires attention and involves the basal ganglia are dependent on the interaction between these two subcortical structures [12, 65].
References
Hore J, Watts S. Timing finger opening in over arm throwing based on a spatial representation of hand path. J Neurophysiol. 2005;93:3189–99.
Iacoboni M. Playing tennis with cerebellum. Nat Neurosci. 2001;4:555–6.
Harrington DL, Haaland KY. Neural underpinnings of temporal processing: a review of focal lesion, pharmacological, and functional imaging research. Rev Neurosci. 1999;10(2):91–116.
Holmes G. The cerebellum of man. Brain. 1939;62:1–30.
Gibbon J, Malapani C, Dale CL, Gallistel C. Toward the neurobiology of temporal cognition: advances and challenges. Curr Opin Neurobiol. 1997;7:170–84.
Matell MS, Meck WH. Cortico-striatal circuits and interval timing: coincidence detection of oscillatory processes. Brain Res Cogn Brain Res. 2004;21:139–70.
Mauk MD, Buonomano DV. The neural basis for temporal processing. Annu Rev Neurosci. 2004;27:307–40.
Ivry RB, Spencer RMC. The neural representation of time. Curr Opin Neurobiol. 2004;14:225–32.
Braitenberg V. Is the cerebellar cortex a biological clock in the millisecond range? Prog Brain Res. 1967;25:334–46.
Apps R, Garwicz M. Anatomical and physiological foundations of cerebellar information processing. Nat Neurosci. 2005;6:297–311.
Blakemore SJ, Sirigu A. Action prediction in the cerebellum and in the parietal lobe. Exp Brain Res. 2003;153:239–45.
Buhusi CV, Meck WH. What makes us tick? Functional and neural mechanisms of interval timing. Nat Rev Neurosci. 2005;6:755–65.
Ivry RB, Keele SW. Timing functions of the cerebellum. J Cogn Neurosci. 1989;1:136–52.
Jueptner M, Rijntjes M, Weiller C, Faiss JH, Timmann D, Mueller SP, et al. Localization of a cerebellar timing process using PET. Neurology. 1995;45:1540–5.
Meck WH. Neuropsychology of timing and time perception. Brain Cogn. 2005;58:1–8.
Pastor MA, Day BL, Macaluso E, Friston KJ, Frackowiak RSJ. The functional neuroanatomy of temporal discrimination. J Neurosci. 2004;24:2585–91.
Spencer RMC, Zelaznik HN, Diedrichsen J, Ivry RB. Disrupted timing of discontinuous but not continuous movements by cerebellar lesions. Science. 2003;300:1437–9.
Meck WH, Benson AM. Dissecting the brain's internal clock: how frontal–striatal circuitry keeps time and shifts attention. Brain Cogn. 2002;48(1):195–211.
Harrington DL, Haaland KY, Hermanowitz M. Temporal processing in the basal ganglia. Neuropsychology. 1998;12:3–12.
Malapani C, Rakitin B, Levy R, Meck WH, Deweer B, Dubois B, et al. Coupled temporal memories in Parkinson's disease: a dopamine-related dysfunction. J Cogn Neurosci. 1998;10:316–31.
O’Boyle DJ, Freeman JS, Cody FW. The accuracy and precision of timing of self-paced, repetitive movements in subjects with Parkinson's disease. Brain. 1996;119:51–70.
Harrington DL, Lee RR, Boyd LA, Rapcsak SZ, Knight RT. Does the representation of time depend on the cerebellum? Effect of cerebellar stroke. Brain. 2004;127:561–74.
Ferrandez AM, Huqueville L, Lehericy S, Poline JB, Marsault C, Pouthas V. Basal ganglia and supplementary motor area subtend duration perception: an fMRI study. Neuroimage. 2003;19(4):1532–44.
Livesey AC, Wall MB, Smith AT. Time perception: manipulation of task difficulty dissociates clock functions from other cognitive demands. Neuropsychologia. 2007;45:321–31.
Nenadic I, Gaser C, Volz HP, Rammsayer T, Häger F, Sauer H. Processing of temporal information and the basal ganglia: new evidence from fMRI. Exp Brain Res. 2003;148:238–46.
Jahanshahi M, Jones C, Dirnberger G, Frith C. The substantia nigra pars compacta and temporal processing. J Neurosci. 2006;26(47):12266–73.
Ivry RB. The representation of temporal information in perception and motor control. Cur Opin Neurobiol. 1996;6:851–7.
Lewis PA, Miall RC. A right hemispheric prefrontal system for cognitive time measurement. Behav Processes. 2006;71:226–34.
O’Reilly JX, Mesulam MM, Nobre AC. The cerebellum predicts the timing of perceptual events. J Neurosci. 2008;28(9):2252–60.
Leon MI, Shadlen MN. Representation of time by neurons in the posterior parietal cortex of the macaque. Neuron. 2003;38:8432–44.
Maschke M, Oehlert G, Xie TD, Perlman S, Subramony SH, Kumar N, et al. Clinical feature profile of spinocerebellar ataxia type 1–8 predicts genetically defined subtypes. Mov Disord. 2005;20:1405–12.
Bares M, Lungu O, Liu T, Waechter T, Gomez CM, Ashe J. Impaired predictive motor timing in patients with cerebellar disorders. Exp Brain Res. 2007;180(2):356–65.
Bares M, Lungu OV, Husarova I, Gescheidt T. Predictive motor timing performance dissociates between early diseases of the cerebellum and Parkinson's disease. Cerebellum. 2010;9(1):124–35.
Trouillas P, Takayanagi T, Hallett M, Currier RD, Subramony SH, Wessel K, et al. International cooperative ataxia rating scale for pharmacological assessment of the cerebellar syndrome. J Neurol Sci. 1997;145:205–11.
Oldfield RC. The assessment and analysis of handeness: the Edinburgh inventory. Neuropsychologia. 1971;9:97–113.
Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatr. 1979;134:382–9.
Talairach J, Tournoux P. Co-planar stereotactic atlas of the human brain. Stuttgart: Georg Thieme Verlag; 1988.
Penny W, Holmes A. Random-effects analysis. In: Frackowiak RSJ, Friston KJ, Frith CD, Dolan RJ, Friston KJ, Price CJ, Zeki S, Ashburner J, Penny W, editors. Human brain function, chap 42. 2nd ed. London: Academic; 2003. p. 843–50.
Miall RC, Weir DJ, Wolpert DM, Stein JF. Is the cerebellum a smith predictor? J Mot Behav. 1993;25:203–16.
Bastian AJ. Learning to predict future: the cerebellum adapts feed-forward movement control. Curr Opin Neurobiol. 2006;16:645–9.
Nixon PD. Predicting sensory events. The role of the cerebellum in motor learning. Exp Brain Res. 2001;138:251–7.
Nowak DA, Topka H, Timmann D, Boecker H, Hermsdörfer J. The role of the cerebellum for predictive control of grasping. Cerebellum. 2007;6:7–17.
Nowak DA, Hufnagel A, Ameli M, Timmann D, Hermsdörfer J. Interhemispheric transfer of predictive force control during grasping in cerebellar disorders. Cerebellum. 2009;8(2):108–15.
Bo J, Block HJ, Clark JE, Bastian AJ. A cerebellar deficit in sensorimotor prediction explains movement timing variability. J Neurophysiol. 2008;100(5):2825–32.
Wolpert DM, Miall RC, Kawato M. Internal models in the cerebellum. Trends Cogn Sci. 1998;2:338–47.
Lewis PA, Miall RC. Brain activation patterns during measurement of sub- and supra-second intervals. Neuropsychologia. 2003;41(12):1583–92.
Xu D, Liu T, Ashe J, Bushara KO. Role of the olivo-cerebellar system in timing. J Neurosci. 2006;26:5990–5.
Mathiak K, Hertrich I, Grodd W, Ackermann H. Cerebellum and speech perception: a functional magnetic resonance imaging study. J Cogn Neurosci. 2002;14(6):902–12.
Perrett SP, Ruiz BP, Mauk MD. Cerebellar cortex lesions disrupt learning-dependent timing of conditioned eyelid responses. J Neurosci. 1993;13:1708–18.
Gerwig M, Hajjar K, Dimitrova A, Maschke M, Kolb FP, Frings M, et al. Timing of conditioned eyeblink responses is impaired in cerebellar patients. J Neurosci. 2005;25:3919–31.
Timmann D, Watts S, Hore J. Failure of cerebellar patients to time finger opening precisely causes ball high–low inaccuracy in overarm throws. J Neurophysiol. 1999;82(1):103–14.
Ullen F, Forssberg H, Erhsson HH. Neural networks for the coordination of the hands in time. J Neurophysiol. 2003;89(2):1126–35.
Rao SM, Harrington DL, Haaland KY, Bobholz JA, Cox RW, Binder JR. Distributed neural systems underlying the timing of movements. J Neurosci. 1997;17(14):5528–35.
Edelstyn NM, Ellis SJ, Jenkinson P, Sawyer A. Contribution of the left dorsomedial thalamus to recognition memory: a neuropsychological case study. Neurocase. 2002;8(6):442–52.
Lewis PA, Miall RC. Distinct systems for automatic and cognitively controlled time measurement: evidence from neuroimaging. Curr Opin Neurobiol. 2003;13:250–5.
Manto MU. On the cerebello-cerebral interactions. Cerebellum. 2007;5(4):286–8.
Daly JJ, Wolpaw JR. Brain–computer interfaces in neurological rehabilitation. Lancet Neurol. 2008;7(11):1032–43.
Grant MP, Leigh RJ, Seidman SH, Riley DE, Hanna JP. Comparison of predictable smooth ocular and combined eye-head tracking behaviour in patients with lesions affecting the brainstem and cerebellum. Brain. 1992;115:1323–42.
Townsend J, Courchesne E, Covington J, Westerfield M, Harris NS, Lyden P, et al. Spatial attention deficits in patients with acquired or developmental cerebellar abnormality. J Neurosci. 1999;19:5632–43.
Lilja A, Hamalainen P, Kaitaranta E, Rinne R. Cognitive impairment in spinocerebellar ataxia type 8. J Neurol Sci. 2005;237(1–2):31–8.
Kawai Y, Suenaga M, Watanabe H, Ito M, Kato K, Kato T, et al. Prefrontal hypoperfusion and cognitive dysfunction correlates in spinocerebellar ataxia type 6. J Neurol Sci. 2008;271(1–2):68–74.
Suenaga M, Kawai Y, Watanabe H, Atsuta N, Ito M, Tanaka F, et al. Cognitive impairment in spinocerebellar ataxia type 6. J Neurol Neurosurg Psychiatry. 2008;79(5):496–9.
Garrard P, Martin NH, Giunti P, Cipolotti L. Cognitive and social cognitive functioning in spinocerebellar ataxia—a preliminary characterization. J Neurol. 2008;255(3):398–405.
Werner S, Bock O, et al. The effect of cerebellar cortical degeneration on adaptive plasticity and movement control. Exp Brain Res. 2009;193(2):189–96.
Huang C. Implications on cerebellar function from information coding. Cerebellum. 2008;7(3):314–31.
Acknowledgements
Supported by NIH grant NS40106, MH065598, the Department of Veterans Affairs, the Brain Sciences Chair, Proshek-Fulbright grant, Academia Medica Pragensis Foundation, and by MSM0021622404.
Conflict of Interest
There are no potential conflicts of interest in the submission and no financial and personal relationship that might bias our work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bares, M., Lungu, O.V., Liu, T. et al. The Neural Substrate of Predictive Motor Timing in Spinocerebellar Ataxia. Cerebellum 10, 233–244 (2011). https://doi.org/10.1007/s12311-010-0237-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12311-010-0237-y