
Abstract
The aim of this study is to evaluate the oxidative stress in predialysis, hemodialysis (HD) and peritoneal dialysis patients and to test the effects of antihypertensive drugs and volume control on oxidative stress parameters. The study was composed of five groups as follows: control group (n = 30), predialysis group (n = 30), peritoneal dialysis group (n = 30), hemodialysis group, (normotensive with strict volume control, n = 30), hemodialysis group (normotensive with medication, n = 30). Plasma malondialdehyde (MDA), erythrocyte superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GSHPx) and routine biochemical parameters were studied in all patients. Hemodialysis patients with strict volume control (HDvc) had lower levels of MDA than other patient groups (p < 0.001), and CAT, SOD values had highest level other patient groups (p < 0.001). The treatment of hypertension with strict volume control in chronic renal failure patients causes less damage to the antioxidant capacity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The balance between pro-oxidant and anti-oxidant capacities in chronic renal failure (CRF) is shifted towards a state of increased oxidative stress. In CRF, not only the usual cardiovascular risk factor but also those unique to uremia increases oxidative stress [1–7]. In the presence of oxidative stress, free oxygen radicals attacks the functional molecules, such as proteins, lipids and DNA, either denaturing them or altering their structure. The attack by free radicals on the polyunsaturated fatty acids on the surface of the cell membrane results in the production of lipid peroxidation like malondialdehyde. High level of this products is a marker of systemic oxidation. Healthy people are protected themselves against free radicals by several defense mechanisms. Major intracellular scavenger of free radicals is reduced glutathione (GSH). Decreased GSH levels and increased oxidized form glutathione (GSSG) levels may indicate depletion of the anti-oxidant reserves [2, 5, 8–10].
The progressive increase in oxidative stress in patients with CRF from the onset of chronic renal disease, is caused by a number of factors, among which are deficiency of vitamin C resulting from the reduced consumption of fresh vegetables and fruits in order to avoid hypercalcemia, loss of vitamins during dialysis, nutritional deficiencies such as intra-cellular vitamin E, reduction in selenium concentration as well as advanced age, presence of diabetes, accumulation of uremic toxins, chronic inflammation, hypervolemia, hypertension and renal replacement therapy itself [2, 5, 9]. In addition, some defects have been detected in different components of prophylactic anti-oxidant mechanism in patients with CRF. These are reduction in the activities of antioxidant enzymes which include SOD, CAT and GSHPx, antioxidant enzymes [2, 5, 9, 10].
Tepel [3] have shown that oxidative stress plays a role in the pathogenesis of hypertension. Hypertension occurs very frequently in patients with CRF and is the most important factor to contribute to the development of cardio-vascular diseases [11]. It has been suggested that the hypertension that occurs in CRF might be ascribed to volume overload and rennin activity. It is claimed that excessive volume accounts for more than 90, 95 % of the cases, and that rennin would have a secondary role. Excessive volume increases first cardiac output and then systemic vascular resistance, resulting in blood pressure to rise. With strict volume control and sufficient dialysis, the rate of hypertension prevalence is lowered by 20–25 % at the end of the first year of dialysis. [12].
Objectives
The aim of this study is to evaluate the oxidative stress in different groups of CRF patients including predialysis, HD and PD patients and to test the effects of antihypertensive drugs and volume control on oxidative stress parameters in HD patients.
Material and Method
This is a cross-sectional study. The study was conducted on 120 patients studied at Nephrology Department of the Fırat University Medical Faculty Hospital in Elazığ. The study was composed of five groups as follows:
-
1. Control group was comprised of 30 healthy and voluntary individuals with no systematic disease. Their routine biochemical findings were within normal ranges. The control group composed of 15 women and 15 men.
-
2. Predialysis group: patients with renal disease who had not yet reached the stage of dialysis and normotensive had been obtained with medication for at least for 6 months (n = 30). Predialysis group composed of 17 women and 13 men.
-
3. Peritoneal dialysis (PD) group whose normotensive had been obtained with strict volume control for at least for 6 months (n = 30). The PD group composed of 10 women and 20 men.
-
4. HDdrug group whose normotensive had been obtained with medication for at least 6 months. There were 30 patients in this group undergoing hemodialysis 4–5 h/session three times a week for more than 6 months. The HDdrug group composed of 9 women and 21 men.
-
5. HDvc group whose normotensive had been obtained with strict volume control for at least 6 months (n = 30). There were 30 patients in this group undergoing hemodialysis 4–5 h/session three times a week for more than 6 months. The HDvc group composed of 9 women and 21 men.
Patients with diabetes mellitus, chronic pulmonary disease and hepatic insufficiency were not included in any of the groups. Parameters of biochemistry and oxidative stress were measured both in patients groups and control. The participants with mean systolic (SBP) ≥ 140 mmHg and diastolic blood pressures (DBP) ≥ 90 mmHg and above were considered hypertensive.
Patients whose normotensive had been obtained with medication were using various antihypertensive drugs. Forty-two percent of the patients were using angiotensin-converting-enzyme (ACE) inhibitors, 26.3 % ACE inhibitor + diuretics, and 10.5 % calcium antagonists, 11 % β-bloker and 10 % α-bloker.
Ethical approval for the study was obtained from the Health Sciences Research Ethics Committee of the Firat University and all patients gave informed consent.
Samples
After a 5-minute resting period, blood pressure was measured and then blood sample were collected subsequent to an approximately 12-hour fasting period and before dialysis therapy in patients on HD.
Fasting venous 5 ml blood sample were collected without anticoagulant for separation of serum sample which was used for determination of glucose, albumin, sodium, potassium, calcium, phosphorus, urea and creatinine levels. Serum was separeted immediately by centrifuged for 10 min at 3,000 rpm and general biochemical tests measurements were performed without delay by the autoanalyzer, Olympus AU 600, (Olympus co Ltd Japan) was used with Olympus kits, and methods suited to their content. Four milliliter venous blood were drawn into tubes containing K3-EDTA. The samples were centrifuged at 3,000 × g for 10 min, and plasma was removed. Plasma was used to determination of MDA. The erythrocytes were subsequently washed four times with for 0.9 % NaCl. Then they were hemolyzed with cold distilled water in the proportion 1:5. This hemolysates was used to determine SOD, GSHPx and CAT. Plasma sample and erythrocyte package were collected in Eppendorf tubes and stored in −80°C to examine parameters of oxidatif stress.
Four millilitre blood were drawn into tubes containing anticoagulant for determination of blood count. Complete blood count were determined by Beckman coulter Gen S Hematology Analyzer (Beckman Coulter Inc. U.S.A) together with appropriate kits.
Plasma MDA levels were measured by a modification of the methods of Satoh [13] and Yagi [14]. Samples were read spectrophotometrically at 532 nm. Plasma MDA results were expressed as nmol/ml.
Erythrocyte CAT activity was estimated by the method of Aebi [15]. Hydrogen peroxide yields maximum absorbance at 240 nm. Absorbance levels diminishing as a function of time in the catalase peroxide reaction have been measured at intervals of 30 s for 3 min at 240 nm. The reduction in the absorbance is directly proportional to catalase activity. Findings have been expressed in u/g hemoglobin (Hb).
Erythrocyte SOD activity was determined by the method devised by Sun [16], and according to the modification by Durak [17]. In this method SOD activity is based upon the principle of reduction of nitroblue tetrazolium by superoxide produced with the system of xanthine/xanthine oxidase. This complex yields maximum absorbance at 560 nm. Findings have been expressed in U/g Hb.
The glutathione peroxidase activity was measured by the method of Paglia and Valentine [18]. The activity of P-GSH-Px was expressed as U/g Hb.
Statistical Analyses
All statistical analysis were performed using the SPSS version 11.0 packet program. The results were shown as mean ± standard deviation (SD). χ2 test was used for the evaluation of age in the groups. In the evaluation of biochemistry parameters among the groups, one-way analysis of variance (ANOVA) tests were used. Tukey B and Scheffe tests were used for comparison between two groups. A p value <0.05 was accepted as statistically significant.
Results
The clinical and biochemical findings of the groups have been presented in Table 1. PD group were younger than other groups (p < 0.01). There were no significant difference between patients groups in length of dialysis (p > 0.05).
The SBP and DBP of the HDvc and PD groups were very similar to those of the subjects in the control group. However, it is noteworthy that predialysis group have noticeably higher SBP and DBP than the patients in the other groups. HDdrug group’ SBP has been found higher than in the other groups (Table 1).
Interdialytic weight gain was significantly higher in the HDdrug compared to this in the HDvc.
Urea (p < 0.001), creatinine (p < 0.001) and hematocrit levels (p < 0.001) were significantly higher in the patients groups compared to those in the controls. While there are differences in creatinine levels between patient groups, HDdrug HDvc were not different in this respect (p = 0.991). Sodium (p < 0.001) and albumin (p < 0.001) levels were decreased in the PD group compared to the control group. Potassium (p < 0.05) and phosphorus levels (p < 0.001) were higher in HDdrug group than control group. The albumin levels of the predialysis and PD groups were lower than control group (p < 0.05, p < 0.001 respectively). As for the patient groups there were differences between PD, HDvc and HDdrug (p < 0.01, p < 0.05 respectively).
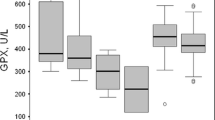
The oxidant and antioxidant parameters of the groups have been presented in Table 2. Compared to the controls, markedly lower SOD level (p < 0.001) was seen in patients groups. CAT levels have been found statistically different neither in comparisons of patient groups with the control group nor in intra-group comparisons.
GSHPx level was significantly higher in control group compared to the HDdrug (p < 0.001) and HDvc group (p < 0.001). GSHPx level was significantly decreased in the HDdrug group compared to the predialysis and PD groups (p < 0.05).
The level of MDA was higher in the patient groups compared to the control group. The difference between the control and HDvc groups has not reached statistical difference, (p = 0.066). The MDA level of the HDdrug was significantly higher than the HDvc group (p < 0.05).
Discussion
The presence of oxidative stress in patients with CRF is based on the elevation of the plasma concentration of MDA reduction of the antioxidant capacity, and the impairment of antioxidant enzymes [19].
Low level of antioxidant enzyme activities and high level of MDA were observed in the patient groups as compared with control group in this study. The major finding of our study, HDvc has the best antioxidant capacity, and the lowest MDA level among patients groups.
Annuk et al. [5] has demonstrated the presence of a correlation between the extent of renal failure and the level of lipid peroxidation in predialysis patients. In a multitude of studies, it has been found that in CRF, while MDA rises [20–23], antioxidant levels fall compared to the control group [24–26]. Several studies have shown that while the same findings may be observed in PD patients as well, antioxidant levels are more favorable in HD group [26, 27]. It has been showed that antioxidant levels of predialysis group, on the other hand, are lower than in the control group, but higher than in HD or PD group [5, 27].
It has been demonstrated that elevated oxidative stress, particularly hydroxyl radicals, contributes to development of hypertension [3]. Barton et al. [28] have found that oxidative stress plays an important part in the pathogenesis of genetic and acquired forms of hypertension, and that it resulted in hypertension in normotensive animals, especially in the absence of GSH. Demirci et al. [29] have shown that MDA level of PD patients was higher in hypertensive subgroup compared to control, and antioxidant capacity (CAT and GSHPx) was tended to be reduced in hypertensive PD patients.
While MDA, the indicator of oxidant system in our study, was the highest in HDdrug group, it was the lowest in HDvc group. We have assessed oxidant system by studying SOD, CAT, and GSHPx levels. In this study, antioxidant capacity was tended to be reduced in patient groups. As is seen in Table 2, those of the patient groups with most favorable antioxidant capacity are HDvc, predialysis, and PD patients in descending order. When patient groups are compared among themselves, the most favorable SOD and CAT levels are HDvc group. As for GSHPx levels, it has been observed that HDdrug group has lower levels than all the other groups. We divided patients into two groups according to their antihypertensive therapy. We wanted to know which treatment is effective in oxidative stress. Compared with HDdrug patients, HDvc patients constitute the group with less oxidative stress and most favorable oxidant capacity. When the blood pressure levels of both groups of HD patients are studied, a statistically significant difference is observed. It is know that hypertension is related to oxidative stress [11, 12]. We are of the opinion that in the HDdrug group, even if blood pressure is reduced, hypervolemia the most important cause of hypertension persist. Increase of volume occurs in HD patients, which, in turn, is responsible for the development of hypertension. Hypervolemia by causing high speed of the intra-arterial blood flow can have impacted the endothelium negatively and thus intensified the production of free oxygen radicals. In addition, hypervolemia leads to inflammation, which runs with elevated C-reactive protein and interleukin-6 and reduced albumin [30]. Subsequently high levels of C-reactive protein and interleukin-6 stimulate polymorph nuclear leukocytes, causing them to produce free oxygen radicals [31]. If treatment is desired, without lowering volume, it should be in the form of reducing blood pressure by providing relaxation of arteries muscles with meditation per se. However there will constantly occur mechanical damage to the surface of the artery since the volume passing through it has not been reduced.
Serum albumin level is an indirect indicator of this inflammation. Albumin is a natural anti-oxidant cytokines that arise, notably interleukin-6 prevents direct synthesis of albumin in the liver [32, 33]. Furthermore, it is argued that leukocytes could be activated, increasing the production of free oxygen radicals, as a result of not only the blood being in contact with dialysis membrane, which is used during dialysis and is not biocompatible, but also of endotoxins’ capability of being transmitted to patients from the system during the process of dialysis [31]. However, the MDA levels in the predialysis and PD groups in our study have been higher than HDvc group, whose leukocytes have not been in contact with a foreign membrane. PD fluids contain high glucose concentrations. The long term exposure of the peritoneum to these solution are responsible for the accumulation of advanced glycation and products and glucose degradation product. We think that this is highly effective in improving the oxidative stress. However, it seems that PD group has a lower oxidant level and higher antioxidant levels compare to HDdrug group.
In this study, predialysis group is the second best group according to the level of MDA, CAT and SOD. Also, the best group according to the level of GSHPx. It is reported that renal proximal tubule cells may be necessary for the activity of plasma GSHPx. As a result of renal failure, renal synthesis of GSHPx is reduced [24]. This condition is compatible with our results. In the predialysis group the level of MDA and blood pressure were increased, CAT and SOD levels were decreased compared to the HDvc group. We suggests that hypervolemia plays a more important role in the development of oxidative stress.
This study showed that oxidative stress was increased and antioxidant capacity was decreased in HDdrug group compared to the HDvc group. Also, strict volume control in hypertensive patients is a method more effective on the oxidant system.
Conclusion
The treatment of hypertension with strict volume control in dialysis patients can improve the survival rates by causing less destruction in anti-oxidant capacity and reducing the rate of atherosclerosis development.
Limitations
The negative side of this study could be done prospectively.
References
Locatelli F, Canaud B, Eckardt KU, Stenvinkel P, Wanner C, Zoccali C. Oxidative stress in end-stage renal disease: an emerging threat to patient outcome. Nephrol Dial Transplant. 2003;18(7):1272–80.
Annuk M, Zilmer M, Fellsröm B. Endothelium-dependent vasodilation and oxidative stress in chronic renal failure: impact on cardiovascular disease. Kidney Int Suppl. 2003;84:50–3.
Tepel M. Oxidative stress: does it play role in genesis of essential hypertension of uraemia? Nephrol Dial Transplant. 2003;18(8):1439–42.
Erdoğan C, Ünlüçerçi Y, Türkmen A, Kuru A, Çetin Ö, Bekpınar S. The evaluation of oxidative stress in patients with chronic renal failure. Clin Chim Acta. 2002;322(1–2):157–61.
Annuk M, Zilmer M, Lind L, Linde T, Fellström B. Oxidative stress and endothelial function in chronic renal failure. J Am Soc Nephrol. 2001;12:2747–52.
Rutkowski P, Slominska EM, Szolkiewicz M, Aleksandrowicz E, Smoleński RT, Wołyniec W, et al. Relationship between uremic toxins and oxidative stress in patients with chronic renal failure. Scand J Urol Nephrol. 2007;41(3):243–8.
Moreno M, Delbosc S, Dupuy AM, Canaud B, Cristol JP. Overproduction of reactive oxygen species in end-stage renal disease patients: a potential component of hemodialysis-associated inflammation. Hemodial Int. 2005;9(1):37–46.
Ferretti G, Bachetti T, Masciangelo S, Pallotta G. Lipid peroxidation in hemodialysis patients: effect of vitamin C supplementation. Clin Biochem. 2008;41(6):381–6.
da Silva AC, Rocha JBT, Morsch ALB, Zanina RF, Kaizera R, Maldonadoa PA, et al. Oxidative stress and δ-ALA-D activity in chronic renal failure patients. Biomed Pharmacother. 2007;61(2–3):180–5.
Himmelfarb J. Uremic toxicity, oxidative stress, and hemodialysis as renal replacement therapy. Semin Dial. 2009;22(6):636–43.
Mailloux LU, Levey AS. Hypertension in patients with chronic renal disease. Am J Kid Disease. 1998;32(5 suppl 3):120–41.
Mailloux LU, Haley WE. Hypertension in the ESRD patient: pathophysiology, therapy, outcomes, and future directions. Am J Kid Disease. 1998;32(5):705–19.
Satoh K. Serum lipid peroxide in cerebrovascular disorders determined by a new colorimetric method. Clin Chim Acta. 1978;90(1):37–43.
Yagi K. Assay of blood plasma or serum for lipid peroxide level and its clinical significance. Methods Enzym. 1984;105:224–41.
Aebi H. Catalase in vitro. Methods Enzym. 1984;105:121–6.
Sun Y, Oberley LW, Li Y. A simple method for clinical assay of superoxide dismutase. Clin Chem. 1988;34(3):497–500.
Durak İ. Letter to the editor. A methodological approach to superoxide dismutase activity assay based on inhibition of nitroblue tetrazolium reduction. Clin Chem Acta. 1993;214:103–4.
Paglia DE, Valentine WN. Studies on the quantitative characterization of erythrocyte glutathione peroxidase. J Lab Clin Med. 1967;70(1):158–69.
Vaziri ND. Effect of chronic renal failure on nitric oxide metabolism. Am J Kidney Dis. 2001;38(4 Suppl 1):74–9.
Miyazaki H, Matsuoka H, Itabe H, Usui M, Ueda S, Okuda S, Imaizumi T. Hemodialysis impairs endothelial function via oxidative stress: effects of vitamin E-coated diayzer. Circulation. 2000;101(9):1002–6.
Göçmen AY, Şahin E, Koçak H, Tuncer M, Gümüşlü S. Levels of asymmetric dimethylarginine, nitric oxide and lipid peroxidation markers in patients with end-stage renal disease having peritoneal dialysis treatment. Clin Biochem. 2008;41(10–11):836–40.
Kadkhodaee M, Hemmati M, Zahmatkesh M, Ghaznavi R, Mirershadi F, Mahdavi-Mazde M, Seifi B. Assessment of plasma antioxidant status in hemodialysis patients. Ther Aphe Dial. 2008;12(2):147–51.
Derici Ü, Ebinç FA, Yılmaz M, Kulaksızoğlu S, Arınsoy T, Sindel Ş. Lipid peroxidation and the antioxidant capacity of dialysis patients: the effects of a single hemodialysis session with different dialysis membranes. Gazi Med J. 2008;19(2):53–5.
Çeliker H, Elkiran B, İlhan N, Günal Aİ, Doğukan A. The effects of hemodialysis and peritoneal dialysis on oxidative stress parameters. Turk Neph Dial Transpl. 2001;10(2):88–92.
Dursun B, Dursun E, Çapraz I, Tomris O, Apaydın A, Süleymanlar G. Are uremia, diabetes, and atherosclerosis linked with impaired antioxidant mechanisms? J Investig Med. 2008;56(2):545–52.
Kayabasi H, Sit D, Atay AE, Yılmaz Z, Kadiroğlu AK, Yılmaz ME. Parameters of oxidative stress and echocardiographic indexes in patients on dialysis therapy. Ren Fail. 2010;32(3):328–34.
Bibi G, Green Y, Nagler RM. Compositional and oxidative analysis in the saliva and serum of predialysis chronic kidney disease patients and end-stage renal failure patients on peritoneal dialysis. Ther Apher Dial. 2008;12(2):164–70.
Barton CH, Ni Z, Vaziri N. Enhanced nitric oxide inactivation in aortic coarctation-induced hypertension. Kidney Int. 2001;60(3):1083–7.
Demirci Ş, Şekeroğlu MR, Noyan T, Köçeroğlu R, Soyoral YU, Dülger H, et al. The importance of oxidative stress in patients with chronic renal failure whose hypertension is treated with peritoneal dialysis. Cell Biochem Funct. 2011;29:249–54.
Ortega O, Gallar P, Munoz M, Carreño A, Ortiz M, Molina A, et al. Association between C-reactive protein levels and N-terminal pro-B-type natriuretic peptide in pre-dialysis patients. The Link between ventricular dysfunction, hypervolemia and inflammation? Nephron Clin Pract. 2004;97(4):125–30.
Toborek M, Wasik T, Drozdz M, Klina M, Magner-Wróbela K, Kopieczna-Grzebieniaka E. Effect of hemodialysis on lipid peroxidation and antioxidant system in patients with chronic renal failure. Metabolism. 1992;41(11):1229–32.
Wanner C, Zimmermann J, Schwedler S, Metzger T. İnflammation and cardiovascular risk in dialysis patients. Kidney Int Suppl. 2002;80:99–102.
Yeun JA, Kaysen GA. Factors influencing serum albumin in dialysis patients. Am J Kidney Dis. 1998;32(6 Suppl 4):118–25.
Conflict of Interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Günal, S.Y., Üstündağ, B. & Günal, A.İ. The Assessment of Oxidative Stress on Patients with Chronic Renal Failure at Different Stages and on Dialysis Patients Receiving Different Hypertensive Treatment. Ind J Clin Biochem 28, 390–395 (2013). https://doi.org/10.1007/s12291-013-0316-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12291-013-0316-1