
Abstract
Lectin-like oxidized low-density lipoprotein receptor-1 (SR-E1, LOX-1, OLR1) was first discovered as a vascular receptor for modified lipoprotein particles nearly 20 years ago. Since then, in vitro and in vivo studies have demonstrated an association between LOX-1, a soluble form (sLOX-1) and a number of diseases including atherosclerosis, arthritis, hypertension and pre-eclampsia. However, converting such discoveries into tools and drugs for routine clinical use is dependent on translational preclinical and clinical studies but such studies have only begun to emerge in the past decade. In this review, we identify the key clinical applications and corresponding criteria that need to be addressed for the effective use of LOX-1-related probes and molecules for patient benefit in different disease states.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lectin-like oxidized low-density lipoprotein receptor-1 (SR-E1, LOX-1, OLR1) is a class E scavenger receptor (SR) found on macrophages and chondrocytes, as well as endothelial and smooth muscle cells [1–3]. This is a 273-residue, type 2 membrane protein encoded in humans by a gene locus on chromosome 12. Its discovery and presumed function revolved around its binding affinity for oxidized low-density lipoprotein (oxLDL) particles in the formation of ‘pre-atherosclerotic’ fatty streaks [4] (Fig. 1). Much of the early work assessing the biological function of LOX-1 has focused on this aspect of disease. However, LOX-1 can recognize other ligands including bacteria, apoptotic cells and C-reactive protein (CRP) [5–7].

Role of LOX-1 in atherosclerosis. Low-density lipoproteins (LDL) pass into the subendothelial layer and undergo oxidation (oxLDL). OxLDL binds to LOX-1 on the endothelial cell surface triggering activation of an inflammatory reaction: adhesion proteins encourage monocyte recruitment and subendothelial layer translocation. OxLDL bound to macrophage LOX-1 is internalized and accumulates in the cell cytoplasm leading to the transformation of macrophages into foam cells. Further inflammation and LOX-1 oxLDL binding on smooth muscle cells and platelets leads to smooth muscle cell invasion into the intima and platelet aggregation with luminal narrowing
Cell surface LOX-1 expression can be elevated by multiple stimuli including reactive oxygen species (ROS) [8], inflammatory cytokines (TNF-α, TGF-β) [9] as well as oxLDL particles. Activated LOX-1 is implicated in multiple signal transduction pathways which influence atherosclerosis plaque initiation and progression. Firstly, activated LOX-1 signalling to the Bax/Bcl-2 pathway is implicated in programmed cell death (apoptosis) in smooth muscle and endothelial cells [10]. Furthermore, LOX-1 activation is also implicated in downregulation of inhibitory apoptotic protein-1 (cIAP-1) and upregulation of caspase-3 and caspase-9 activity, which also serve to bring about apoptosis [11]. LOX-1 can activate protein kinase C (PKC) activity [12] which in turn enhances mitogen-activated protein kinase (MAPK) and nuclear factor κB (NF-κB) activity. NF-κB promotes smooth muscle cell proliferation [13] and expression of cell adhesion molecules and chemokines [14]. Such signal transduction promotes endothelial-monocyte cell-cell adhesion and platelet aggregation. Other pathophysiological functions of LOX-1 include the activation of arginase II (ARG2) enzyme, leading to suppression of nitric oxide levels and increased vascular tone [15]. Finally, LOX-1 is also implicated in decreased atherosclerotic plaque stability through increased activation of metalloproteases [12] (Fig. 2). A full discussion of the biological functions of LOX-1 is beyond the scope of this review; however, this has been explored recently elsewhere [16, 17].

LOX-1-dependent signal transduction. LOX-1 expression is stimulated by nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), angiotensin II (AngII), advanced glycation end products (AGEs), oxidized low-density lipoprotein (oxLDL), glucose and tumour necrosis factor-alpha (TNF-α) amongst others. At the cell membrane, it binds oxLDL as well as C-reactive protein (CRP) and other ligands. OxLDL/LOX-1 is trafficked into the cell where it activates a protein kinase C (PKC) leading to an inflammatory cascade involving mitogen-activated kinase proteins (p38/p42); further downstream, vascular and intercellular adhesion molecules (VCAM, ICAM) lead to platelet and monocyte adhesion and further inflammation. Matrix metalloproteases are also upregulated leading to atherosclerotic plaque instability. Lastly, a number of apoptosis pathways are triggered including upregulation of the Bcl-2 family, downregulation of inhibitory apoptotic protein-1 (ICAP-1) and upregulation of caspases
In vitro studies of LOX-1 have assessed cellular responses found in arthritis, pre-eclampsia, renal disease and cancer [18–21]. The study of transgenic mice carrying LOX-1 knockouts or overexpression [22] has been a catalyst to a growing body of further research [23–25]. However, the translation of such work has been limited; to date, no effective LOX-1 suppressing treatment has been tested on humans. Furthermore, antibody therapy has been safely used as a treatment regime for diseases such as cancer, inflammatory bowel disease and arthritis for decades [26–28]. The use of targeted antibody therapy for the management of cardiovascular disease may be a rich area of research to be explored.
Soluble LOX-1 and Cardiovascular Risk Factors
The extracellular domain of LOX-1 is cleaved at the cell surface to generate a soluble molecule (sLOX-1) [29]. Although the exact mechanism for the cleavage of LOX-1 remains elusive, recent evidence suggests that it likely takes place by the action of the ADAM10 metalloprotease by cleaving of the neck domain of LOX-1 [30, 31]. It is speculated that circulating sLOX-1 levels are proportional or linked to membrane LOX-1 levels [32], though this has not been proven. An increasingly important use of sLOX-1 as a biomarker is in its link to cardiovascular disease risk factors (i.e. diabetes, hypertension, smoking and hyperlipidaemia). However, such studies face a major challenge since these conditions tend to co-exist, necessitating large numbers of patients to adequately power research studies in this area. Tan and colleagues demonstrated an association between sLOX-1 and type 2 diabetes mellitus (T2DM) [33]. Exclusion of patients with co-existing risk factors for cardiovascular disease leads to a preserved association; however, this subgroup analysis was not backed by regression testing. A recently published study has also identified an independent association between sLOX-1 levels and hypertension by multivariate analysis [34]. Smoking intensity and expired carbon monoxide levels have been correlated with elevated sLOX-1 levels in a single study; however, this study lacked non-smoking controls [35]. Whilst these studies are useful for outlining the relationship between LOX-1 and cardiovascular disease risk factors, the diagnosis of diabetes, hypertension and smoking is necessarily based on the measurement of blood sugar, blood pressure and the patient’s smoking history. sLOX-1 measurement would be of greater use if it could be used to diagnose a disease which is otherwise categorized based on associated factors: indeed, there is an association between sLOX-1 levels and metabolic syndrome. However, a diagnostic cut-off with high sensitivity or specificity has not been identified [36]. The above findings suggest that sLOX-1 is likely to be a marker of endothelial damage, and its elevation may be due to multifactorial causative events.
sLOX-1 in the Diagnosis of Acute and Chronic Disease
In their keynote study, Hayashida et al. [37] demonstrated that in a large cohort of patients, soluble LOX-1 levels correlated with a diagnosis of acute coronary syndrome (ACS) earlier in clinical presentation than troponin T levels. This has led to much work investigating serum sLOX-1 levels as a marker of cardiovascular health in acute and chronic disease states. One such study has demonstrated that sLOX-1 rises faster and is more reliable than cardiac troponins in the diagnosis of ACS [38]. However, notable methodological flaws affected this study, such as mixed patient groups (emergent and elective coronary intervention), unequal recruitment into study groups and the absence of prospective powering. Misaka and colleagues [39] have described the use of a LOX-1 assay to distinguish ACS from exertional angina pectoris at presentation. Patients who were later diagnosed with ACS displayed significantly higher sLOX-1 serum levels at primary coronary intervention [39]. However, this study could not identify a correlation between sLOX-1 and other markers of cardiac ischaemia (i.e. troponin, creatine kinase and high sensitivity CRP.
When examining non-acute manifestations of coronary artery disease, one study [40] showed that sLOX-1 can be used for prognostic evaluation of ischemic heart disease and stroke risk. The LOX-1 index score ([apolipoprotein B-bound LOX-1] × [total circulating sLOX-1]) had a positive correlation with the risk of both ACS and stroke at 11-year follow-up. Whilst no direct correlation could be made between sLOX-1 levels and cardiovascular risk, the low overall incidence of such events (2.79% of IHD and 3.73% of stroke) may mean the study was underpowered despite analysing samples from over 2000 patients [40]. Given the low prevalence of cardiovascular disease in the study cohort of Japanese men and women [41], a more significant association may be found in other ethnic groups and/or regions. sLOX-1 has also been shown to correlate with the presence of plaque rupture in cases of thin-cap fibroatheroma [42]. There is a significant association between plaque rupture and sLOX-1 levels and a significant difference in sLOX-1 levels between stable angina patients and those who experience ACS [43]. Lastly, sLOX-1 levels are elevated threefold in the presence of coronary artery disease in patients with metabolic syndrome [44].
Outside of cardiovascular disease, Ishikawa et al. [45] found that serum and synovial sLOX-1 levels are elevated in rheumatoid arthritis. Further, LOX-1 is thought to be an important biomarker of disease activity and treatment efficacy; however, this is complicated by evidence that other disease states also elevate sLOX-1 levels [33, 36]. Thus, LOX-1 is not simply a sensor and vehicle for oxLDL but also a gauge of chronic disease status. Whilst trials have recognized that LOX-1 could be of use for future-targeted therapy, this has not come to fruition. Future research could yield new and diverse clinical applications based on LOX-1-specific probes: animal work has begun to elucidate how this might work.
Manipulation of LOX-1 Function in Disease
LOX-1 has been investigated predominantly as a biomarker and contributory factor to atherosclerotic disease. Much of the preclinical therapeutic evaluations of antibodies directed against LOX-1 have also focused on this pathology. Mehta and colleagues [46, 47] investigated the use of a blocking antibody directed against LOX-1 in a rat myocardial ischaemia-reperfusion injury model. Animals treated with vehicle or antibody were subjected to ligation of the left anterior descending coronary artery for 60 min before resumption of blood flow. In the control group, there was increased myocardial metalloprotease expression and leucocyte recruitment. LOX-1 antibody administration attenuated such effects; in addition, the myocardial infarct area was significantly smaller compared to controls. Lin et al. [48] found that the incidence of cardiac hypertrophy in ApoE-null transgenic mice on a fat and cholesterol-rich diet was nullified by anti-LOX-1 antibody treatment. Nakano and colleagues [49] demonstrated that anti-LOX-1 antibody treatment caused reduction in lipid deposits in the mesenteric arteries of stroke-prone spontaneous hypertensive rats. Finally, Lund and colleagues [50] suggest that anti-LOX-1 treatment can modulate the pro-atherogenic effects of air pollutants.
Hinagata et al. [51] demonstrated that following iatrogenic balloon injury of carotid arteries, the administration of repeated doses of anti-LOX-1 antibody caused a 29 % decrease in intimal hyperplasia of the carotid artery in rat models. Additionally, there were reduced levels of myeloperoxidase and reactive oxygen species (ROS) in the endothelial cells lining the injured arteries [51]. A role for LOX-1 has also been implicated in renal vascular disease: Dominguez and colleagues [52] injected obese diabetic hypertensive (OM) rats with either anti-LOX-1 antibody or control-matched immunoglobulin and evaluated effects on kidney pathology. The OM phenotype was associated with a significant decrease in renal vascular density and lower levels of glomerular vascular endothelial growth factor A (VEGF-A). These effects were attenuated in OM rats subjected to anti-LOX-1 antibody treatment. Histological analysis also suggested that this mode of treatment conferred protection against renal fibrosis.
The link between LOX-1 and rheumatoid arthritis is further supported by evidence that intra-articular administration of oxLDL to a rat model led to significant joint swelling, mediated via synovial hyperplasia [45]. However, such effects are attenuated by the co-administration of anti-LOX-1 antibody [53]. Earlier work by Nakagawa et al. [54] had also demonstrated that anti-LOX-1 antibody administration reduced the incidence of zymosan-induced arthritis in rat models.
The LOX-1 gene (OLR1) is localized with the natural killer gene complex on the short arm of human chromosome 12, suggesting a functional role in innate immunity [55]. However, anti-LOX-1 administration reduces leucopenia and improves survival upon exposure to bacterial endotoxin [55]. Landsberger et al. [56] found that administration of E. coli lipopolysaccharides led to significant changes in the intestinal microcirculation including increased leucocyte adhesion to blood vessel walls and increased release of TNF-α. However, anti-LOX-1 administration reduced these effects. Zhang et al. [57] examined the effect of LOX-1 blockade on acute lung injury and concluded that there was markedly reduced myeloperoxidase activity, sequestration of leucocytes into the lung interstitium and capillary permeability. In addition, markers for cell apoptosis were also markedly reduced by such treatment. Thus, LOX-1 may have a role in modulating the systemic inflammatory response syndrome. Vincent and colleagues [58] also explored the effects of anti-LOX-1 administration on the pro-inflammatory axis involving NF-κB and diabetes. Anti-LOX-1 administration blocked NF-κB activation and reduced incidence of nerve dysfunction. Thus, perturbation of LOX-1 function may also modulate peripheral neuropathy.
Akamatsu et al. [59] have suggested a role for LOX-1 in neonatal hypoxic-ischaemic encephalopathy (HIE). In their study, LOX-1 (OLR1) gene expression was found to be elevated in neural tissues of a rat HIE model [59]. Furthermore, daily administration of intravenous anti-LOX-1 antibody reduced brain oedema and total volume apoptosis associated with this model.
There is increasing realization that LOX-1 could prove to be valuable for molecular imaging applications. Ishino et al. [60] were the first to describe the use of a Technetium-99-labelled anti-LOX-1 antibody for atherosclerosis detection. Watanabe heritable hyperlipidemic rabbits injected with this probe revealed labelling of atherosclerotic regions in major arterial beds. Further, there was a strong correlation between in vivo imaging and post-mortem pathological analyses. Li et al. [61] tested the use of magnetic resonance imaging and single-positron emission computed tomography on ApoE-null and LOX-1-null transgenic mice. Using liposomes bound to anti-LOX-1 and relevant imaging markers, arterial areas dense in LOX-1 expression could be mapped, particularly at rupture-prone sites within atherosclerotic plaques. De Vos et al. [62] used protein nanobodies directed at LOX-1 using similar models, but binding affinity was poor and results inconclusive.
Translational Applications
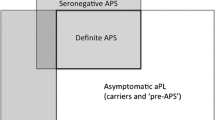
Taken together, such studies provide evidence to support the feasibility LOX-1 as a biomarker of human disease and target for therapeutic strategies. However, a few points must be borne in mind: Firstly, one must consider the significant differences in the primary sequence and structure of LOX-1 when compared between humans, mice and rats (Fig. 3); rat and murine LOX-1 proteins contain more than 90 additional residues in the extracellular domains that may have unique properties not associated with human LOX-1. Careful comparison of effects across different animal species is needed before clinical application. Secondly, the endpoints in many of these studies are scientifically convenient but clinically irrelevant. Parameters such as joint diameter and myeloperoxidase expression levels are unsuitable for quantifying human diseases that are best measured in quality of life effects and functional impairment. Thus, reconciling experimental parameters with clinical end points is of paramount importance. Thirdly, outcomes in diseases such as cardiovascular disease, HIE and rheumatoid arthritis are measured over years [63–67] and short-term results in the animal experiments described may not correlate with longer-term effects.

Comparison of amino acid sequence of human, rabbit, bovine, murine and rat LOX-1. Line diagrams depicting relationship between LOX-1 proteins from different species. Blue: human protein sequence; green: matching animal amino acids; red: non-matching animal amino acids. Note the presence of a much longer neck domain in murine and rat LOX-1 of unknown function
One must also consider the heterogeneity of the studies reviewed (Table 1). The delivery route of antibodies varies substantially between different LOX-1-related animal studies. Further, antibodies have been delivered to human targets by subcutaneous [68], intramuscular [69] and intrathecal [70] routes; such routes remain untested in LOX-1 studies. The dose and scheduling adopted also shows great variability. Clearly, like other monoclonal antibody-based therapies [71], the pharmacokinetics of anti-LOX-1 antibodies need to be explored further.
Assuming that the above criticisms are appropriately addressed, there are two further considerations which will face future translational research. Whilst guidance on safety profiling for antibody therapy now exists [72], side effects associated with such therapies are significant [73]. Whilst this is not a new consideration, the absence of side effect reporting in preclinical studies is notable. Moreover, cost may prove to be the greatest barrier to the adoption of immunological therapies to LOX-1. Alemtuzumab, as an example, was marketed at US$60,000 per patient per year [74]. Given the pandemic proportion of cardiovascular disease, and the fact that conventional, cheaper treatments for cardiovascular disease have not been proven to be cost-effective for widespread primary prevention [75], treating patients at a preclinical stage of disease will likely be prohibitively expensive.
Conclusions and Future Research
There are significant hurdles to overcome in order to translate preclinical findings into clinically valid and cost-effective endpoints: The side effects of targeting LOX-1 remains a worrying and valid concern; The therapeutic route for targeting LOX-1 is problematical: oral administration of proteins is not yet practical despite advances in formulation vehicles, enzyme inhibitors, absorption enhancers and mucoadhesive polymers [76]. Nonetheless, anti-LOX-1 probes show great potential in risk stratification of cardiovascular disease. Such agents may also have a wider role in the management of other chronic and acute disease.
Abbreviations
- (ox)LDL:
-
(Oxidized) low-density lipoprotein
- LOX-1, OLR1:
-
Lectin-like oxidized low-density lipoprotein receptor-1
- TNF-α:
-
Tumour necrosis factor-alpha
- TGFβ:
-
Transforming growth factor beta
- ACS:
-
Acute coronary syndrome
- ApoE:
-
Apolipoprotein E
- NF-κB:
-
Nuclear factor kappa-light-chain-enhancer of activated B cells
- MCP1:
-
Monocyte chemotactic protein 1
- HIE:
-
Hypoxic ischemic encephalopathy
References
Chiba, Y., Ogita, T., Ando, K., & Fujita, T. (2001). PPARgamma ligands inhibit TNF-alpha-induced LOX-1 expression in cultured endothelial cells. Biochemical and Biophysical Research Communications, 286(3), 541–546.
Simopolou, T., Malizos, K. N., & Tsezou, A. (2007). Lectin-like oxidized low density lipoprotein receptor 1 (LOX-1) expression in human articular chondrocytes. Clinical and Experimental Rheumatology, 25(4), 605–612.
Yoshida, H., Kondratenko, N., Green, S., Steinberg, D., & Quehenberger, O. (1998). Identification of the lectin-like receptor for oxidized low-density lipoprotein in human macrophages and its potential role as a scavenger receptor. Biochemical Journal, 334, 9–13.
Sawamura, T., Kume, N., Aoyama, T., Moriwaki, H., Hoshikawa, H., Aiba, Y., et al. (1997). An endothelial receptor for oxidized low-density lipoprotein. Nature, 386(6620), 73–77.
Shimaoka, T., Kume, N., Minami, M., Hayashida, K., Sawamura, T., Kita, T., et al. (2001). LOX-1 supports adhesion of gram-positive and gram-negative bacteria. The Journal of Immunology, 166(8), 5108–5114.
Murphy, J. E., Tacon, D., Tedbury, P. R., Hadden, J. M., Knowling, S., Sawamura, T., et al. (2006). LOX-1 scavenger receptor mediates calcium-dependent recognition of phosphatidylserine and apoptotic cells. Biochemical Journal, 393(1), 107–115.
Shih, H. H., Zhang, S., Cao, W., Hahn, A., Wang, J., Paulsen, J. E., et al. (2009). CRP is a novel ligand for the oxidized LDL receptor LOX-1. American Journal Physiology: Heart and Circulatory Physiology, 296(5), H1643–H1650.
Wang, X., Philips, M. I., & Mehta, J. L. (2011). LOX-1 and angiotensin receptors, and their interplay. Cardiovascular Drugs and Therapeutics, 25, 401–417.
Minami, M., Kume, N., Kataoka, H., Morimoto, M., Hayashida, K., Sawamura, T., et al. (2000). Transforming growth factor-B(1) increases the expression of lectin-like oxidized low-density lipoprotein receptor-1. Biochemical and Biophysical Research Communications, 272, 357–361.
Kataoka, H., Kume, N., Miyamoto, S., Minami, M., Morimoto, M., Hayashida, K., et al. (2001). Oxidized LDL modulates Bax/Bcl-2 through the lectin-like Ox-LDL receptor-1 in vascular smooth muscle cells. Arteriosclerosis, Thrombosis, and Vascular Biology, 21, 955–960.
Chen, J., Mehta, J. L., Zhang, X., Singh, B. K., & Li, D. (2004). Role of LOX-1 in expression of apoptotic proteins and activation of caspase pathways in human coronary artery endothelial cells. Circulation Research, 94, 370–376.
Li, D., Liu, L., Chen, H., Sawamura, T., Ranganathan, S., & Mehta, J. L. (2003). LOX-1 mediates oxidized low-density lipoprotein-induced expression of matrix metalloproteinases in human coronary artery endothelial cells. Circulation, 107(4), 612–617.
Eto, H., Miyata, M., Kume, N., Minami, M., Itabe, H., Orihara, K., et al. (2006). Expression of lectin-like oxidized LDL receptor-1 in smooth muscle cells after vascular injury. Biochemical and Biophysical Research Communications, 341(2), 591–598.
Jiang, R., Teng, Y., Huang, Y., Gu, J., & Li, M. (2010). Protein kinase C-alpha activation induces NF-kB-dependent VCAM-1 expression in cultured human umbilical vein endothelial cells treated with sera from preeclamptic patients. Gynecologic and Obstetric Investigation, 69(2), 101–108.
Ryoo, S., Bhunia, A., Chang, F., Shoukas, A., Berkowitz, D. E., & Romer, L. H. (2011). OxLDL-dependent activation of arginase II is dependent on the LOX-1 receptor and downstream RhoA signaling. Atherosclerosis, 214(2), 279–287.
Xu, S., Ogura, S., Chen, J., Little, P. J., Moss, J., & Liu, P. (2013). LOX-1 in atherosclerosis: biological functions and pharmacological modifiers. Cellular and Molecular Life Sciences, 70, 2859–2872.
Taye, A., & El-Sheikh, A. A. K. (2013). Lectin-like oxidized low-density lipoprotein receptor 1 pathways. European Journal of Clinical Investigation, 743, 740–745.
Kakinuma, T., Yasuda, T., Nakagawa, T., Hiramitsu, T., Akiyoshi, M., Akagi, M., et al. (2004). Lectin-like oxidized low-density lipoprotein receptor 1 mediates matrix metalloproteinase 3 synthesis enhanced by oxidized low-density lipoprotein in rheumatoid arthritis cartilage. Arthritis & Rheumatology, 50(11), 3495–3503.
Lee, H., Park, H., Kim, Y. J., Kim, H. J., Ahn, Y. M., Park, B., et al. (2005). Expression of lectin-like oxidized low-density lipoprotein receptor-1 (LOX-1) in human preeclamptic placenta: possible implications in the process of trophoblast apoptosis. Placenta, 26(2), 226–233.
Wang, R., Ding, G., Liang, W., Chen, C., & Yang, H. (2010). Role of LOX-1 and ROS in oxidized low-density lipoprotein induced epithelial-mesenchymal transition of NRK52E. Lipids in Health and Disease, 19(9), 120.
Liang, M., Zhang, P., & Fu, J. (2007). Up-regulation of LOX-1 expression by TNF-alpha promotes trans-endothelial migration of MDA-MB-231 breast cancer cells. Cancer Letters, 258(1), 31–37.
Mehta, J. L., Sanada, N., Hu, C. P., Chen, J., Dandapat, A., Sugawara, F., et al. (2007). Deletion of LOX-1 reduces atherogenesis in LDLR knockout mice fed high cholesterol diet. Circulation Research, 100, 1634–1642.
Hsieh, C. C., Yen, M. H., Yen, C. H., & Lau, Y. T. (2001). Oxidized lowdensity lipoprotein induces apoptosis via generation of reactive oxygen species in vascular smooth muscle cells. Cardiovascular Research, 49(1), 135–145.
Hu, C., Dandapat, A., Sun, L., Chen, J., Marwall, M. R., Romeo, F., et al. (2008). LOX-1 deletion decreases collagen accumulation in atherosclerotic plaque in low-density lipoprotein receptor knockout mice fed a high-cholesterol diet. Cardiovascular Research, 79(2), 287–293.
Hu, C., Bum-Yong, K., Megyesi, J., Kaushal, G. P., Safirstein, R., & Mehta, J. L. (2009). Deletion of LOX-1 attenuates renal injury following angiotensin II infusion. Kidney International, 76, 521–527.
Presta, L. G., Chen, H., O’Connor, S. J., Chisholm, V., Meng, G., Krummen, L., et al. (1997). Humanization of an anti-vascular endothelial growth factor monoclonal antibody for the therapy of solid tumors and other disorders. Cancer Research, 57(20), 4593–4595.
van Duleman, H. M., van Deveneter, S. J., Hommes, D. W., Bill, H. A., Jansen, J., Tytgat, G. N., et al. (1997). Treatment of Crohn’s disease with anti-tumor necrosis factor chimeric monoclonal antibody (cA2). Gastroenterology, 109(1), 129–135.
Elliott, M. J., Mini, R. N., Feldman, M., Kalden, J. R., Antoni, C., Smolen, J. S., et al. (1994). Randomised double-blind comparison of chimeric monoclonal antibody to tumour necrosis factor α (cA2) versus placebo in rheumatoid arthritis. Lancet, 344(8930), 1105–1110.
Murase, T., Kume, N., Kataoka, H., Minami, M., Sawamura, T., Masaki, T., et al. (2000). Identification of soluble forms of lectin-like oxidised receptor-1. Arteriosis Sclerosis and Vascular Biology, 20(3), 715–720.
Mitsuoka, H., Kume, N., Hayashida, K., Inui-Hayashida, A., Aramaki, Y., Toyohara, M., et al. (2009). Interleukin 18 stimulates release of soluble lectin-like oxidized LDL receptor-1 (sLOX-1). Atherosclerosis, 202(1), 176–182.
Biocca, S., Arcangeli, T., Tabliaferri, E., Testa, B., Vindigni, G., Oteri, F., et al. (2013). Simulative and experimental investigation on the cleavage site that generates the soluble human LOX-1. Archives of Biochemistry and Biophysics, 540(1–2), 9–18.
Brinkley, T. E., Kume, N., Mitsuoka, H., Phares, D. A., & Hagberg, J. M. (2008). Elevated soluble lectin-like oxidized LDL receptor 1 (LOX-1) levels in obese postmenopausal women. Obesity, 16(6), 1454–1456.
Tan, K. C., Shiu, S. W., Wong, Y., Leng, L., & Bucala, R. (2007). Soluble lectin-like oxidized low density lipoprotein receptor-1 in type 2 diabetes mellitus. The Journal of Lipid Research, 49(7), 1438–1444.
Yavuzer, S., Yavuzer, H., Cengiz, M., Erman, H., Altiparmak, M. R., Korkmazer, B., et al. (2015). Endothelial damage in white coat hypertension: role of lectin-like oxidized low-density lipoprotein-1. Journal of Human Hypertension, 29(2), 92–98.
Takanabe-Mori, R., Ono, K., Wada, H., Takaya, T., Ura, S., Yamakage, H., et al. (2013). Lectin-like oxidized low-density lipoprotein receptor-1 plays an important role in vascular inflammation in current smokers. Journal of Atherosclerosis and Thrombosis, 20(6), 585–590.
Civelek, S., Kutnu, M., Uzun, H., Erdenen, F., Altunoglu, E., Andican, G., et al. (2014). Soluble lectin-like oxidized LDL receptor 1 as a possible mediator of endothelial dysfunction in patients with metabolic syndrome. Journal of Clinical Laboratory Analysis, 29(3), 184–190.
Hayashida, K., Kume, N., Murase, T., Minami, M., Nakagawa, D., Inada, T., et al. (2005). Serum soluble lectin-like oxidized low-density lipoprotein receptor-1 levels are elevated in acute coronary syndrome: a novel marker for early diagnosis. Circulation, 112(6), 812–818.
Kume, N., Mitsuoka, H., Hayashida, K., Tanaka, M., Kominami, G., & Kita, T. (2010). Soluble lectin-like oxidized LDL receptor-1 (sLOX-1) as a sensitive and specific biomarker for acute coronary syndrome—comparison with other biomarker. Journal of Cardiology, 56(2), 159–165.
Misaka, T., Suzuki, S., Sakamoto, N., Yamaki, T., Sugimoto, K., Kunii, H., et al. (2014). Significance of soluble lectin-like oxidized LDL receptor-1 levels in systemic and coronary circulation in acute coronary syndrome. BioMed Research International. doi:10.1155/2014/649185.
Inoue, N., Tomonori, O., Yoshihiro, K., Fujita, Y., Sato, Y., Mamoru, N., et al. (2010). LOX index, a novel predictive biochemical marker for coronary heart disease and stroke. Clinical Chemistry, 56(4), 550–558.
Iso, H. (2011). Lifestyle and cardiovascular disease in Japan. Journal of Atherosclerosis and Thrombosis, 18(2), 83–88.
Virmani, R., Burke, A. P., Kolodgie, F. D., & Farb, A. (2003). Pathology of the thin-cap fibroatheroma: a type of vulnerable plaque. Journal of Interventional Cardiology, 16(3), 267–272.
Kobayashi, N., Takano, M., Hata, N., Kume, N., Yamamoto, M., Yokoyama, S., et al. (2013). Soluble lectin-like oxidized LDL receptor-1 (sLOX-1) as a valuable diagnostic marker for rupture of thin-cap fibroatheroma: verification by optical coherence tomography. International Journal of Cardiology, 168(4), 3217–3223.
Li, B., Zhang, L., Yang, X., Liu, X., & Ren, Y. (2010). Serum sLOX-1 levels are associated with the presence and severity of angiographic coronary artery disease in patients with metabolic syndrome. Clinical & Investigative Medicine, 33(6), E398–E404.
Ishikawa, M., Ito, H., Akyoshi, M., Kume, N., Yoshitomi, H., Mitsuoka, H., et al. (2012). Lectin-like oxidized low-density lipoprotein receptor 1 signal is a potent biomarker and therapeutic target for human rheumatoid arthritis. Arthritis and Rheumatology, 64(4), 1024–1034.
Li, D., Williams, V., Liu, L., Chen, H., Sawamura, T., Antakli, T., et al. (2002). LOX-1 inhibition in myocardial ischemia-reperfusion injury: modulation of MMP-1 and inflammation. American Journal Physiology: Heart and Circulatory Physiology, 283(5), H1795–H1801.
Li, D., Williams, V., Liu, L., Chen, H., Sawamura, T., Romeo, F., et al. (2003). Expression of lectin-like oxidized low-density lipoprotein receptors during ischemia-reperfusion and its role in determination of apoptosis and left ventricular dysfunction. Journal of the American College of Cardiology, 41(6), 1048–1055.
Lin, L., Gong, H., Zhou, N., Jiang, G., Wu, J., Li, L., et al. (2010). Oxidized low-density lipoprotein-induced cardiac hypertrophy is partly mediated by lectin-like oxidized low-density lipoprotein receptor-1 activating angiotensin II type 1 receptor independent of angiotensin II. Beijing, China: World Congress of Cardiology Scientific Sessions.
Nakano, A., Inoue, N., Sato, Y., Nishimichi, N., Takikawa, K., Fujita, Y., et al. (2010). LOX-1 mediates vascular lipid retention under hypertensive state. Journal of Hypertension, 28(6), 1273–1280.
Lund, A. K., Lucero, J., Harman, M., Madden, M. C., McDonald, J. D., Seagrave, J. C., et al. (2011). The oxidized low-density lipoprotein receptor mediates vascular effects of inhaled vehicle emissions. American Journal of Respiratory and Critical Care Medicine, 184(1), 82–91.
Hinagata, J. I., Kakutani, M., Fuji, T., Naruko, T., Inoue, N., Fujita, Y., et al. (2006). Oxidized LDL receptor LOX-1 is involved in neointimal hyperplasia after balloon arterial injury in a rat model. Cardiovascular Research, 69(1), 263–271.
Dominguez, J. H., Mehta, J. L., Li, D., Wu, P., Kelly, K. J., Packer, C. S., et al. (2008). Anti-LOX-1 therapy in rats with diabetes and dyslipidemia: ablation of renal vascular and epithelial manifestations. American Journal of Physiology, 894(1), F110–F119.
Ishikawa, M., Ito, H., Furu, M., Murata, K., Shibuya, H., Yoshitomi, H., et al. (2013). A crucial role for lectin-like oxidized LDL receptor-1 on joint inflammation in RA. Madrid, Spain: Annual European Congress of Rheumatology of the European League Against Rheumatism.
Nakagawa, T., Akagi, M., Hoshikawa, H., Chen, M., Yasuda, T., Mukai, S., et al. (2002). Lectin-like oxidized low-density lipoprotein receptor 1 mediates leukocyte infiltration and articular cartilage destruction in rat zymosan-induced arthritis. Arthritis and Rheumatology, 46(9), 2486–2494.
Honjo, M., Nakamura, K., Yamashiro, K., Kiryu, J., Tanihara, H., McEvoy, L. M., et al. (2003). Lectin-like oxidized LDL receptor-1 is a cell-adhesion molecule involved in endotoxin-induced inflammation. Proceedings of the National Academy of Sciences of the United States of America, 100(3), 1274–1279.
Landsberger, M., Zhou, J., Wilk, S., Thaumuller, C., Pavlovic, D., Otto, M., et al. (2010). Inhibition of lectin-like oxidized low-density lipoprotein receptor-1 reduces leukocyte adhesion within the intestinal microcirculation in experimental endotoxemia in rats. Critical Care, 14(6), R223.
Zhang, P., Liu, M. C., Cheng, L., Liang, M., Ji, H. L., & Fu, J. (2009). Blockade of LOX-1 prevents endotoxin-induced acute lung inflammation and injury in mice. Journal of Innate Immunity, 1(4), 358–365.
Vincent, A. M., McLean, L. L., Pande, M., Oh, S. S., & Feldman, E. L. (2012). LOX-1-mediated injury in sensory neurons in type 2 diabetes. International Journal of Diabetes and Metabolism, 20(2), 59–63.
Akamatsu, T., Dai, H., Mizuguchi, M., Goto, Y. I., Oka, A., & Itoh, M. (2014). LOX-1 is a novel therapeutic target in neonatal hypoxic-ischemic encephalopathy. American Journal of Pathology, 184(6), 1843–1852.
Ishino, S., Mukai, T., Kuge, Y., Kume, N., Ogawa, M., Takai, N., et al. (2008). Targeting of lectinlike oxidized low-density lipoprotein receptor 1 (LOX-1) with99mTc-labeled anti-LOX-1 antibody: potential agent for imaging of vulnerable plaque. Journal of Nuclear Medicine, 49(10), 1677–1685.
Li, D., Patel, A. R., Klibanov, A. L., Kramer, C. M., Ruiz, M., Kang, B. Y., et al. (2010). Molecular imaging of atherosclerotic plaques targeted to oxidized LDL receptor LOX-1 by SPECT/CT and magnetic resonance. Circulation: Cardiovascular Imaging, 3(4), 464–472.
De Vos, J., Broisat, A., Totsek, J., Ghezzi, C., Muyldermans, S., Lahouette, T., et al. (2012). Development of LOX-1 nanobodies for imaging of atherosclerosis. Journal of Nuclear Medicine, 53(4), 667.
Shankaran, S., Laptook, A. R., Ehrenkranz, R. A., Tyson, J. E., McDonald, S. A., Donovan, E. F., et al. (2005). Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. New England Journal of Medicine, 353(15), 1574–1584.
Maini, R., St Clair, E. W., Breedveld, F., Furst, D., Kalden, J., Weisman, M., et al. (1999). Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. ATTRACT Study Group. Lancet, 354(9194), 1932–1939.
Huizinga, T. W., Fleischmann, R. M., Jasson, M., Radin, A., van Adelsberg, J., Fiore, S., et al. (2014). Extended report: Sarilumab, a fully human monoclonal antibody against IL-6Rα in patients with rheumatoid arthritis and an inadequate response to methotrexate: efficacy and safety results from the randomised SARIL-RA-MOBILITY Part A trial. Annals of the Rheumatic Diseases, 73(9), 1626–1634.
Pedersen, T. R., Faergeman, O., Kaastelein, J. J., Olsson, A. G., Tikkanen, M. J., Holme, I., et al. (2005). High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA, 294(19), 2437–2445.
The SPS3 Investigators. (2012). Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. New England Journal of Medicine, 367(9), 817–825.
Lundin, J., Kimby, E., Björkholm, M., Broliden, P. A., Celsing, F., Hjalmar, V., et al. (2002). Phase II trial of subcutaneous anti-CD52 monoclonal antibody alemtuzumab (Campath-1H) as first-line treatment for patients with B-cell chronic lymphocytic leukemia (B-CLL). Blood, 100(3), 768–773.
Meissner, H. C., Groothius, J. R., Rodriguez, W. J., Welliver, R. C., Hogg, G., Gray, P. H., et al. (1999). Safety and pharmacokinetics of an intramuscular monoclonal antibody (SB 209763) against respiratory syncytial virus (RSV) in infants and young children at risk for severe RSV disease. Antimicrobial Agents and Chemotherapy, 43(5), 1183–1188.
Brown, M. T., Coleman, R. E., Friedman, A. H., Freidman, H. S., McLendon, R. E., Reiman, R., et al. (1996). Intrathecal 131I-labeled antitenascin monoclonal antibody 81C6 treatment of patients with leptomeningeal neoplasms or primary brain tumor resection cavities with subarachnoid communication: phase I trial results. Clinical Cancer Research, 2(6), 963–972.
Leveque, D., Winiewski, S., & Jehl, F. (2005). Pharmacokinetics of therapeutic monoclonal antibodies used in oncology. Anticancer Research, 25, 2327–2344.
Muller, P. Y., & Brennan, F. R. (2009). Safety assessment and dose selection for first-in-human clinical trials with immunomodulatory monoclonal antibodies. Clinical Pharmacology & Therapeutics, 85(3), 247–258.
Hansel, T., Kroopshofer, H., Singer, T., Mitchell, J. A., & George, A. J. (2010). The safety and side effects of onoclonal antibodies. Nature Reviews Drug Discovery, 9(4), 35–38.
Shaughnessy, A. F. (2012). Monoclonal antibodies: magic bullets with a hefty price tag. British Medical Journal. doi:10.1136/bmj.e8346.
Greving, J. P., Visseren, F. L., de Wit, G. A., & Algra, A. (2011). Statin treatment for primary prevention of vascular disease: whom to treat? Cost-effectiveness analysis. British Medical Journal. doi:10.1136/bmj.d1672.
Park, K., Kwon, I. C., & Park, K. (2011). Oral protein delivery: current status and future prospect. Reactive and Functional Polymers, 71(3), 280–287.
Acknowledgments
This work was supported by the Leeds Teaching Hospitals National Health Service Trust (J.D.S.) and a PhD scholarship from the Brunei government (I.A.Z.).
Compliance with Ethical Standards
No human studies were carried out by the authors for this article. No animal studies were carried out by the authors for this article.
Conflict of Interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Enrique Lara-Pezzi oversaw the review of this article
Rights and permissions
About this article

Cite this article
De Siqueira, J., Abdul Zani, I., Russell, D.A. et al. Clinical and Preclinical Use of LOX-1-Specific Antibodies in Diagnostics and Therapeutics. J. of Cardiovasc. Trans. Res. 8, 458–465 (2015). https://doi.org/10.1007/s12265-015-9655-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12265-015-9655-z