
Abstract
Both Doppler-guided hemorrhoidal artery ligation (DG-HAL) and infrared coagulation (IRC) are well-established techniques in the management of hemorrhoids. The aim of the study is to compare the clinical outcomes of DG-HAL and IRC in the patients with grade 1 and 2 hemorrhoids. A total of 296 patients were registered for the study, but 51 patients were lost in follow-up; hence, finally 245 patients were included in the analysis. Patients were randomized into two groups (mean age, 42 years; range, 19–60 years). Group A (n = 116) was treated with DG-HAL and group B (n = 129) was treated with IRC. Patients were examined at 1 week, 1 month, and 6 months after the procedure. Mean time taken for HAL was 21 min and for IRC, 12 min. The cost of the DG-HAL procedure was 1,440 rupees ($31.53) and that of IRC was 376 rupees ($8). The mean duration of hospital stay after HAL was 6 h and after IRC, 2 h. Control of symptoms with HAL was 96 %, whereas with IRC, 81 %. Postoperative complication rate for HAL was 2 %, whereas for IRC, 13 %. Requirement of repeat procedure with HAL was 9 % and with IRC, 28 %. Both the procedures are minimally invasive, associated with minimal discomfort, and suitable for day care surgery. IRC requires lesser procedure time, lesser postoperative hospital stay, and has lower procedure cost, whereas DG-HAL is more effective in controlling symptoms of hemorrhoids, has lower post operative complication rate, and has lesser requirement of repeat procedure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
“Hemorrhoids are local masses formed by pathologic hypertrophy or migration of the anal cushions, or stasis of the blood stream in the subcutaneous blood vessels around the anus [1].” These are cushions of specialized, highly vascular tissue found within the anal canal in the submucosal space. The term “hemorrhoidal disease” should be reserved for those vascular cushions that are abnormal and cause symptoms in patients. These cushions of thickened submucosa contain blood vessels, elastic tissue, connective tissue, and smooth muscles [2].
Studies have shown that hemorrhoidal bleeding is arterial and not venous because hemorrhage from disrupted hemorrhoids occurs from presinusoidal arterioles that communicate with the sinusoids in this region [2]. This is supported by the bright red appearance and the arterial pH of the blood [3].
Hemorrhoids are very common and affect more than 4 % of the population [4]. The new understanding of the pathogenesis of hemorrhoids based on the role of arterial flow through arteriovenous anastomoses has recently led to the assumption that artery ligation should result in shrinkage of the hemorrhoidal mass. On the basis of this assumption, a new technique for the treatment of hemorrhoids, Doppler-guided hemorrhoidal artery ligation (DG-HAL), was introduced by Morinaga et al. in 1995 [5].
This technique is based on the identification and ligation of the terminal branches of the superior rectal artery through a proctoscope equipped with a Doppler probe. A specially developed anoscope can be used for this purpose that incorporates a side-viewing Doppler head. The submucosal arteries approaching the anal canal from above can be identified using a Doppler transducer connected to an echo sounder. They can be ligated through a window situated just above the Doppler head. The success of the ligation can be judged by the disappearance of the arterial Doppler sound. The arterial inflow to the hemorrhoidal mass suddenly drops after the ligation of the artery. While venous outflow is not compromised, the ratio of the inflow/outflow also drops. The hemorrhoidal mass collapses and both the bleeding and the pain cease. The decreasing tension allows regeneration of the connective tissue within the hemorrhoids, which facilitates the shrinkage of the hemorrhoidal tissue and eventually leads to decrease in the prolapse.
In infrared coagulation (IRC), the tissue is coagulated not by means of an electric current but through infrared light [6]. During the treatment, mechanical pressure and radiation energy are applied simultaneously. There is an obvious risk of electric current passing through the body with the use of electrocoagulation, which may cause painful muscular spasms [7]. IRC has proved to be an effective and safe method of treatment for the early-grade bleeding hemorrhoids [8].
The infrared photocoagulator produces infrared light that penetrates the tissue and converts to heat, promoting coagulation of vessels and fixation of hemorrhoidal tissue. The amount of tissue destruction depends on the intensity and duration of the application. It is recommended that the infrared probe be applied for 1.5 s to the apex of each internal hemorrhoid, and be repeated three times on each hemorrhoid. Infrared coagulation does not cause tissue necrosis because of the small amount of heat delivered, and is therefore only useful in the treatment of grade 1 and 2 hemorrhoids, without significant prolapse.
Material and Methods
This prospective, longitudinal, analytical study was conducted during January 2009 to July 2010 and registered 296 patients initially, but 51 patients were lost in follow-up and were not included in the final analysis. The patients underwent careful history taking, clinical and proctoscopic examination for the diagnosis and staging of the disease. A patient was defined as grade 1 if the hemorrhoidal cushions were found to be enlarged, but without any prolapse and as grade 2 if there was prolapse through the anal orifice during straining, but reduced spontaneously.
Inclusion Criteria
All symptomatic patients with grade 1 and grade 2 hemorrhoids who failed to respond to medical management given in the form of plenty of fluids and 20 g of ispaghula husk every night for 10 days.
Exclusion Criteria
The following patients were excluded from this study:
-
Patients with grade 3 and grade 4 hemorrhoids.
-
Patients with grade 1 and grade 2 hemorrhoids, who responded to medical management.
-
Patients with other concurrent proctological diseases (fistula, fissure, perianal abscess, IBD).
-
Patients with coagulation disorders.
-
Patients under therapy with anticoagulant drugs.
-
Patients with other medical diseases such as portal hypertension and liver cirrhosis.
-
Patients who were lost in follow-up.
Patients were randomized to either group A, undergoing DG-HAL, or group B, undergoing infrared photocoagulation. The patients were informed about the modalities of treating hemorrhoids and about possible complications, and each signed a standard informed consent form.
Operative Procedure
DG-HAL was performed under saddle block (regional anesthesia) given by 0.7 ml of sensoricaine heavy. We used the DG-HAL system from AMI®. There is an opening slightly distally from the transducer through which the ligature can be placed in the tissue. The proctoscope connects to the Doppler device and produces easily recognizable acoustic signals. After an arterial signal is detected, it is ligated. After ligation, the absence of an arterial signal on that spot is confirmed with the Doppler transducer. Three full circles with the proctoscope are performed in the anal canal with the proctoscope and every arterial signal is ligated. The ligations were performed with a 2.0 vicryl suture especially made for this procedure (AMI HAL suture, 2/0 vicryl, tapered needle, 5/8 circle).
During infrared coagulation 5 % Xylocaine jelly was applied as surface anesthesia. A lubricated proctoscope was inserted and the probe was placed at the base of the hemorrhoidal mass and infrared bursts of 1.5 s were applied. A small white spot marked the point of coagulation. Beneath this point, the blood vessels of the hemorrhoids are destroyed, resulting in decreased blood flow to the hemorrhoids and sometimes immediate reduction of bleeding. Over the following week or two, scar tissue would form and the healing process would be completed.
In the postoperative period, we used on-demand analgesics. Patients were discharged on the same day provided that there was no intraoperative or postoperative complication (bleeding, urinary retention, severe pain).
They were advised to use one of the analgesics when needed, oral antibiotic (Tab ciprofloxacin 500 mg BD for 5 days) and stool softener along with dietetic modifications.
Outcome Measures
We examined the patients after 1 week, 1 month, and 6 months after the procedure. Any patient who lost follow-up at the above-mentioned period, was not included in the analysis of outcome.
The assessment of both the groups was done in terms of
-
1.
time taken in the procedure,
-
2.
perioperative pain,
-
3.
cost of treatment,
-
4.
duration of hospital stay,
-
5.
symptomatic relief,
-
6.
postoperative complications,
-
7.
requirement of repeat procedure.
Groups were compared by the χ 2 homogeneity test at 5 % probability. Results showing normal distribution are given as mean with standard deviation. Statistical significance of differences was accepted when the P value was less than 0.05.
Results
Patient Characteristics
Total 245 patients were finally included in the study analysis. There were 69 males and 47 females in group A (DG-HAL), whereas in group B (IRC), there were 76 males and 53 females. There was a predominance of males in both the groups, but without any significant difference. The mean age of the patients in group A was 45 versus 42.2 years in group B. In both the groups, most patients had grade 2 hemorrhoids. The chief complaint of most of the patients in both groups was bleeding. The clinical characteristics of the patients in the two groups were similar regarding the mean age, sex, hemorrhoids degree, and preoperative complaints (P > 0.05), as shown in Table 1.
Perioperative Outcome
The operative time was longer in the DG-HAL group (mean 21 min) than the IRC group (mean 12 min). All the patients were discharged on the same day of the procedure. The mean duration of hospital stay for the DG-HAL group was 6 h, whereas for the IRC group, it was 2 h. The mean cost of the DG-HAL procedure was 1,440 rupees ($31.53), whereas for IRC, the cost was 376 rupees ($8). Postoperative pain was reported in 11 patients from the DG-HAL group and in 21 patients from the IRC group, as summarized in Table 2.
Follow-Up Outcome
After 1 week, pain and bleeding were controlled in 86 % patients in the DG-HAL group and in 61 % patients in the IRC group. Postoperative complications (mainly discharge and bleeding) were seen only in 2 % patients in the DG-HAL group, whereas in 13 % patients in the IRC group, as summarized in Table 3.
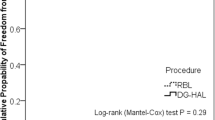
One-month and 6-month follow-up too revealed significant difference in control of symptoms with DG-HAL than IRC. Repeat procedure was required in 9 % patients undergoing DG-HAL and 28 % patients undergoing IRC.
Discussion
There are many treatment modalities presently available for hemorrhoids ranging from dietary modification, lifestyle change, and minimal invasive methods to hemorrhoidectomy. The need for treatment for hemorrhoids is primarily based on the severity of the symptoms. For decades, innovations in the field of hemorrhoidal treatment have centered on modifying the traditional methods to achieve a minimally invasive, less painful procedure, and yet with a more sustainable result.
For grade 1 hemorrhoids, medical management is the mainstay of treatment, whereas grade 2 hemorrhoids are mainly treated surgically. In practice, there are many patients with grade 1 hemorrhoids, who do not respond to medical management and require surgical management. DG-HAL and IRC both are well-established procedures for hemorrhoids. IRC is effective for early grades of hemorrhoids, whereas DG-HAL is effective in all grades of hemorrhoids.
After the successful ligation of the arteries, the inflow to the piles drops, while the venous outflow remains intact, the tension within the anal cushions drops. The piles collapse and both the bleeding and the pain cease. The decreasing tension allows regeneration of the connective tissue within the piles, which facilitates the shrinkage of the hemorrhoid and eventually leads to the definitive decrease in the prolapse. The whole process supports the “hypertensive cushion” theory [9, 10]. During the DG-HAL procedures, there were more arteries than expected on the basis of the traditional anatomical concept [11, 12].
In our study, IRC was performed with surface anesthesia, which has lesser cost of procedure, lesser duration of hospital stay, and lesser procedure time, but has poor control of symptoms, more requirement of repeat procedure, and more post-op complications than DGHAL.
In conclusion, both procedures are minimally invasive, associated with minimal discomfort, and suitable for day care surgery but DG-HAL is more effective than IRC in controlling symptoms of hemorrhoids.
References
Dehong Yu, Yang X, Huang Y (2000) Update and improve hemorrhoids diagnosis and treatment. Chin J Surg 38(12):890–891
Thomson WH (1975) The nature of haemorrhoids. Br J Surg 62(7):542–552
Thulesius O, Gjores JE (1973) Arterio-venous anastomoses in the anal region with reference to the pathogenesis and treatment of haemorrhoids. Acta Chir Scand 139(5):476–478
Bleday R, Pena JP, Rothenberger DA, Goldberg SM, Buls JG (1992) Symptomatic hemorrhoids: current incidence and complications of operative therapy. Dis Colon Rectum 35:477–481
Morinaga K, Hasuda K, Ikeda T (1995) A novel therapy for internal hemorrhoids: ligation of the hemorrhoidal artery with a newly devised instrument (Moricorn) in conjunction with a Doppler flowmeter. Am J Gastroenterol 90:610–613
Pfenninger JL, Surrell (1995) Nonsurgical treatment options for internal hemorrhoids. Am Fam Physician 52(821–834):839–841
Leicester RJ, Nicholls RJ, Mann CV (1981) Infrared coagulation: a new treatment for hemorrhoids. Dis Colon Rectum 24:602–605
O’Holleran TP (1990) Infrared photocoagulation of hemorrhoids. Nebr Med J 75:307–308
Sun WM, Read NW, Shorthouse AJ (1990) Hypertensive anal cushions as a cause of the high anal canal pressures in patients with haemorrhoids. Br J Surg 77:458–462
Sun WM, Peck RJ, Shorthouse AJ, Read NW (1992) Haemorrhoids are associated not with hypertrophy of the internal anal sphincter, but with hypertension of the anal cushions. Br J Surg 79:592–594
Sohn N, Aronoff JS, Cohen FS, Weinstein MA (2001) Transanal hemorrhoidal dearterialisation is an alternative to operative hemorrhoidectomy. Am J Surg 182:515–519
Arnold S, Antonietti E, Rollinger G, Scheyer M (2002) Doppler ultrasound assisted hemorrhoid artery ligation. A new therapy in symptomatic hemorrhoids. Chirurg 73:269–273
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ahmad, A., Kant, R. & Gupta, A. Comparative Analysis of Doppler Guided Hemorrhoidal Artery Ligation (DG-HAL) & Infrared Coagulation (IRC) in Management of Hemorrhoids. Indian J Surg 75, 274–277 (2013). https://doi.org/10.1007/s12262-012-0444-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-012-0444-5