
Abstract
Hemorrhoidal artery ligation (HAL) procedure aims specifically at reducing the arterial flow to the hemorrhoids. The Doppler probe allows an accurate localization of the branches of superior rectal artery which are individually ligated. However, the vessels can also be ligated by digital palpation of vessels without the help of Doppler probe. In this study, we have compared the results of hemorrhoidal artery ligation procedure with and without Doppler guidance in symptomatic grades I–III hemorrhoids. The study was a single-blinded randomized clinical study. Patients were randomly allocated into two groups, the non-Doppler group (HAL group) and the Doppler group (DGHAL group). The outcome was assessed by using HDSS questionnaire as proposed by Nyström et al. Patients were followed at 6 weeks, 6 months, and 1 year following the procedure. In this study, the overall control of bleeding was 86.9% (86.0% in HAL group and 87.9% in DGHAL group) after 1 year of follow-up. The overall recurrence of prolapse in patients with grade II hemorrhoids after 1 year of follow-up was 16.9% (17.9% patients in HAL group and 16.0% in DGHAL group). The overall recurrence of prolapse in patients with grade III hemorrhoid after 1 year follow-up was 58.6% (60% patients in HAL group and 57.1% in DGHAL group). However, there was no significant difference between both groups. No significant difference was found in both groups in the secondary outcome measures (pain, soiling, and itching). Our study indicates that the hemorrhoidal artery ligation procedure can be performed effectively without the use of Doppler transducer. The study also suggests that HAL procedure is more effective in early grade hemorrhoids (grades I and II).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hemorrhoids are one of the most common clinical conditions to affect humans with prevalence of 4.4%. [1,2,3] Hemorrhoids are vascular cushions within the anal canal, usually found in three main locations, left lateral, right anterior, and right posterior position. They lie beneath the epithelial lining of the anal canal and consist of direct arteriovenous communications, mainly between the terminal branches of the superior rectal, middle, and inferior hemorrhoidal arteries. It has been suggested that their presence is essential for continence; they contribute approximately 15 to 20% of the resting anal pressure. The theory of sliding cushions is widely accepted and hemorrhoids become symptomatic when the vascular cushions engorge or descend. [4,5,6,7,8]
Treatment of hemorrhoid ranges from dietary and lifestyle modification to excision of hemorrhoid, depending on degree and severity of symptoms [9, 10]. Medical management includes micronized purified flavonoid fraction (MPFF), consisting of 90% diosmin and 10% hesperidin. [11] Office procedures used in hemorrhoid treatment are sclerotherapy, rubber band ligation, and infrared coagulation (IRC) with variable results. [12,13,14,15,16] Excisional hemorrhoidectomy is the most effective treatment for hemorrhoids with the lowest rate of recurrence compared with other modalities. In clinical practice, the third-degree or fourth-degree internal hemorrhoids are the main indication for hemorrhoidectomy. A major drawback of hemorrhoidectomy is postoperative pain. [17]
A new technique based on Doppler-guided ligation of the terminal branches of the superior hemorrhoidal artery (DGHAL) was introduced in 1995 as an alternative to hemorrhoidectomy. [18] The rationale of this treatment was later supported by the findings from studies which demonstrated that patients with hemorrhoid had increased caliber and arterial blood flow of the terminal branches of the superior rectal arteries. DGHAL technique aims specifically at interrupting the arterial flow to the hemorrhoids, thought to be a main factor in the etiology. The Doppler probe allows an accurate localization of all the branches of superior rectal artery which reduces the inflow. The connective tissue in the collapsed hemorrhoid slowly regenerates with resolution of the prolapse. Postoperative pain is minimal compared with hemorrhoidectomy. None of the severe complications (sepsis, perforation, fistulas) associated with other techniques has been seen. There is no anal wound left to heal. There is no risk of incontinence or strictures. The technique is simple and very easy to master. Patients can be discharged safely on the day of operation, thus reducing hospital costs. [19,20,21] Success rate is well beyond that of other methods of treatment such as rubber band ligation that usually requires multiple banding procedures. In a multicenter, open-label randomized controlled trial comparing hemorrhoidal artery ligation versus rubber band ligation, at 1 year post-procedure, 87 (49%) of 176 patients in the RBL group and 48 (30%) of 161 patients in the HAL group had hemorrhoid recurrence (adjusted odds ratio [aOR] 2·23, 95% CI 1·42–3·51; p = 0·0005). [22]
The three main branches of superior rectal artery are usually consistent in position. The vessels are usually found in the area of visible hemorrhoidal tissue and sometimes the vessels can be identified by digital examination by fingertip. Some recent studies have shown that the Doppler transducer does not contribute to the beneficial effect of HAL procedure and can be omitted during the ligation procedure in the treatment of hemorrhoidal disease. [23] Thus, we hypothesize that the HAL procedure can be performed by finger palpation of hemorrhoidal vessels (FPHAL) or ligation of vessels at the anatomical position at the site of visible pathological hemorrhoidal tissue.
The aim of this study is to compare the outcome of the hemorrhoidal artery ligation (HAL) procedure in grades I–III symptomatic hemorrhoids with and without the use of the Doppler transducer.
Material and Methods
The single-blinded randomized clinical study was conducted at the Department of Surgery, King George’s Medical University, Lucknow, UP, India. Patients with symptomatic grades I–III hemorrhoids who did not respond to medical treatment were included in the study. Patients who are pregnant, with Crohn’s disease, and those with abscesses, colorectal carcinoma, or portal hypertension were excluded from the study. Patients with predominant external hemorrhoids and grade IV hemorrhoids were not included in the study. Patients with concomitant anal fissure were also excluded from the study. A written informed consent was obtained from the patients after describing the procedures involved, perceived benefits, and possible side effects/complications of each of the two treatment modalities and informing the right of patient not to participate and to withdraw from the study at their will without affecting the quality of their care. Ethical approval was obtained from the Institutional Ethics Committee.
Sample size assessment was done keeping in consideration a targeted mean pain score difference of 0.40 and a pooled standard deviation of 0.8 between two groups at 80% power (beta error 20%) and 95% confidence (alpha error 5%). The calculated sample size was 53 for each group. After making contingency provisions, the sample size was kept as 60 in each group. Selection bias was removed through randomization. Randomization was done using computer-generated tables and patients were distributed into two groups, the Doppler group (DGHAL group) and the non-Doppler group (HAL group). Allocation bias/confounder effect was analyzed statistically by matching the two groups demographically and for baseline characteristics. Treatment bias could not be controlled as blinding was not possible. Analytical bias was removed by coding the group names instead of naming them.
All patients were operated in spinal anesthesia in lithotomy position. The ligations were performed with an absorbable, synthetic, braided suture (2/0 Vicryl, 5/8 circumference). Patients in non-Doppler group received the artery ligation procedure without the help of Doppler transducer, and the ligations were placed after digitally palpating the artery about 2–3 cm above the pectinate line. In approximately one-third of cases, the arterial pulsations were not felt and the sutures were placed in the area of visible pathologic hemorrhoidal tissue. In patients of the Doppler group, the standard artery ligations were performed with the help of Doppler transducer using A.M.I. HAL/RAR system. In both groups, a figure of eight ligations was applied with a maximum of 6 ligations. In both groups, no additional procedures were performed. All procedures were performed by surgeons and residents under the supervision of the same surgeon.
Patients were followed at 6 weeks, 6 months, and 1 year after surgery. Symptoms were assessed using frequency of the 5 symptoms including bleeding, prolapse, pain, soiling, itching, as proposed by Nystrom et al. [24] A questionnaire was filled at the outpatient department and also telephonically for patients who did not present themselves at the outpatient department. The symptoms were categorized as mild (once a week), moderate (one to six per week), and severe (every day) based on their frequency.
Categorical variables were presented in number and percentage and continuous variables were presented as mean and SD. Qualitative variables were compared using chi-square test/Fisher’s exact test as appropriate. A p value of <0.05 was considered statistically significant. The data was entered in MS Excel spreadsheet and analysis was done using Statistical Package for Social Sciences (SPSS) version 17.0.
Results
There were 120 patients included in the study. The DGHAL procedure was performed in 60 patients and HAL procedure (without Doppler) was performed in 60 patients. Out of 120 patients, 38 patients had grade I, 53 patients had grade II, and 29 patients had grade III hemorrhoids. The distribution of age, gender, and grade of hemorrhoidal disease was found to be comparable in both groups. At 1 year follow-up, five patients were lost to follow-up. The five different symptoms in both groups were analyzed.
In patients who had undergone HAL procedure, at 1 year follow-up, no bleeding was found in 86% of patients, mild bleeding was found in 12.3% of patients, and moderate bleeding was found in 1.8% of patients. In patients who had undergone DGHAL procedure, at 1 year follow-up, no bleeding was found in 87.9% of patients, and mild bleeding was found in 12.1% of patients. There was no statistically significant difference between the two groups (Table 1).
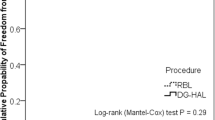
In patients with grade II hemorrhoids who had undergone HAL procedure, at 1 year follow-up, no prolapse was found in 82.1% of patients, and mild prolapse was found in 17.9% patients. For patients who had undergone DGHAL procedure, at 1 year follow-up, no prolapse was found in 84% of patients, and mild prolapse was found in 16% patients. However, the results were comparable and there was no statistically significant difference between the two groups.
In patients with grade III hemorrhoids who had undergone HAL procedure, at 1 year follow-up, no prolapse was found in 40% of patients, mild prolapse was found in 40% patients, moderate prolapsed was found in 13.3%, and severe prolapsed was found in 6.7% of patients. For patients who had undergone DGHAL procedure, at 1 year follow-up, no prolapse was found in 42.9% of patients, mild prolapse was found in 35.7% of patients, and moderate prolapse was found in 21.4% of patients; however, the results were comparable between the two groups (Table 2).
There was no significant difference in the other outcome measures (pain, soiling, and itching) in both groups.
Discussion
In our study, the overall control of bleeding was 86.9% after 1 year of follow-up. The results were comparable in the non-Doppler (86.0%) and Doppler group (87.9%). Mild bleeding was present in 12.3% patients of HAL group and 12.1% patients of DGHAL group. None of the patients in either group reported severe bleeding at 1 year follow-up. In a randomized clinical trial to compare the outcome of hemorrhoidal artery ligation procedure with and without Doppler transducer in grades II–III hemorrhoidal disease, at 6 months follow-up, no bleeding was reported in 87.0% patients, mild bleeding was present in 13.0% patients and none of the patients reported severe bleeding in the non-Doppler group. In Doppler group at 6 months follow-up, no bleeding was present in 62.5% of patients, mild bleeding was seen in 33.3% patients, and severe bleeding was found in 4.2% patients. The result of both groups was comparable and statistically non-significant (p = 0.221). [23]
A prospective study on suture ligation of internal hemorrhoids without Doppler guidance concluded that 82.81% of patients can be satisfactorily managed by HAL procedure without Doppler transducer, at the end of 1 year. [25]
In our study, out of 53 patients with grade II hemorrhoids, 16.98% of patients had persistent prolapse after 1 year. Out of 29 patients with grade III hemorrhoids, 58.62% of patients had persistent prolapse after 1 year. Therefore, correction of prolapse was better in patients with grade II hemorrhoids as compared with grade III hemorrhoids. However, there was no significant difference between the two groups in grade II (p value = 0.857) and grade III hemorrhoids (p value = 0.739).
A systematic review of 5-year follow-up of Doppler-guided hemorrhoidal artery ligation study (17 studies, comprising 1996 patients) reported an overall recurrence rate at 1 year or more of 10.8% for prolapse and 9.7% for bleeding, while the recurrence rate for grade IV hemorrhoids was higher than for grades II and III. In this study, they report a decreasing success rate of the DGHAL procedure during the 5-year postoperative period, with a trend toward a higher recurrence rate for grade III hemorrhoids compared with grade II. [26]
Another systematic review of twenty-eight studies including 2904 patients found that recurrence varied from 3 to 60%, at 6 weeks to 5 years. The pooled total recurrence rate was 17.5% with the highest rates for grade IV hemorrhoids. [27]
In a multicenter trial, a total of 803 patients affected by symptomatic hemorrhoids, who failed a conservative approach, were treated primarily with the Doppler procedure. Recurrence of hemorrhoidal prolapse, bleeding, and both prolapse and bleeding requiring a medical or surgical therapy was seen in 26 (8.7%), 10 (3.4%), and 3 patients (1.0%), respectively. [28]
The other outcome measures (pain, soiling, and itching) were comparable in both groups. None of the patients reported any serious problem in the postoperative period. The study indicates that the results of hemorrhoidal artery ligation procedure are similar with and without the use of the Doppler transducer.
Conclusion
This study indicates that the hemorrhoidal artery ligation procedure can be performed effectively without the use of Doppler transducer. The finger-palpated HAL is a learned procedure and one may get the premonition after having done a score of DGHAL. However, the training of the new surgeons for finger-palpated HAL (FPHAL) can start from the beginning. The study also suggests that HAL procedure is more effective in early grade hemorrhoids (grades I and II) as compared with grade III hemorrhoids.
References
Johanson JF, Sonnenberg A (1990) The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 99:1856–1857
Cintron J, Abacarian H (2007) Benign anorectal: hemorrhoids. In: Wolff B G, Fleshman J W, editors. The ASCRS of colon and rectal surgery. New York, NY: Springer-Verlag. pp. 156–177
Smith LE (2004) Hemorrhoids. In: Fazio V, editor. Current therapy in colon and rectal surgery. St. Louis, MO: Mosby. pp. 11–18
Kluiber RM, Wolff BG (1994) Evaluation of anemia caused by hemorrhoidal bleeding. Dis Colon Rectum 37(10):1006–1007
Aigner F, Gruber H, Conrad F, Eder J, Wedel T, Zelger B, Engelhardt V, Lametschwandtner A, Wienert V, Böhler U, Margreiter R, Fritsch H (2009) Revised morphology and hemodynamics of the anorectal vascular plexus: impact on the course of hemorrhoidal disease. Int J Color Dis 24(1):105–113
Greenspon J, Williams SB, Young HA, Orkin BA (2004) Thrombosed external hemorrhoids: outcome after conservative or surgical management. Dis Colon Rectum 47(9):1493–1498
Johanson JF, Rimm A (1992) Optimal nonsurgical treatment of hemorrhoids: a comparative analysis of infrared coagulation, rubber band ligation, and injection sclerotherapy. Am J Gastroenterol 87(11):1600–1606
Bat L, Melzer E, Koler M, Dreznick Z, Shemesh E (1993) Complications of rubber band ligation of symptomatic internal hemorrhoids. Dis Colon Rectum 36(3):287–290
Acheson AG, Scholefield JH (2008) Management of hemorrhoid. BMJ. 336:380–383
Kaidar-Person O, Person B, Wexner SD (2007) Hemorrhoidal disease: a comprehensive review. J Am Coll Surg 204:102–117
Lyseng-Williamson KA, Perry CM (2003) Micronised purified flavonoid fraction: a review of its use in chronic venous insufficiency, venous ulcers and hemorrhoid. Drugs. 63(1):71–100
Labrid C (1995) A lymphatic function of Daflon 500 mg. Int Angiol 14:36–38
Struckmann JR, Nicolaides AN (1994) Flavonoids. A review of the pharmacology and therapeutic efficacy of Daflon 500 mg in patients with chronic venous insufficiency and related disorders. Angiology. 45:419–428
Chong PS, Bartolo DC (2008) Hemorrhoids and fissure in ano. Gastroenterol Clin N Am 37:627–644 ix
Hain JM (2011) Medical treatment of hemorrhoids using flavonoids. Pract Gastroenterol:1–5
Shanmugam V, Thaha MA, Rabindranath KS, Campbell KL, Steele RJ, Loudon MA (2005) Systematic review of randomized trials comparing rubber band ligation with excisional haemorrhoidectomy. Br J Surg 92:1481–1487
Sim AJ, Murie JA, Mackenzie I (1983) Three year follow-up study on the treatment of first and second degree hemorrhoids by sclerosant injection or rubber band ligation. Surg Gynecol Obstet 157(6):534–536
Morinaga K, Hasuda K, Ikeda T (1995) A novel therapy for internal hemorrhoids: ligation of the hemorrhoidal artery with a newly devised instrument (Moricorn) in conjunction with a Doppler flowmeter. Am J Gastroenterol 90:610–613
Felice G, Privitera A, Ellul E, Klaumann M (2005 Nov) Doppler-guided hemorrhoidal artery ligation: an alternative to hemorrhoidectomy. Dis Colon Rectum 48(11):2090–2093
Sohn N, Aronoff JS, Cohen FS, Weinstein MA (2001) Transanal hemorrhoidal dearterialization is an alternative to operative hemorrhoidectomy. Am J Surg 182:515–519
Ramirez JM, Aguilella V, Elia M, Gracia JA, Martinez M (2005) Doppler-guided hemorrhoidal artery ligation in the management of symptomatic hemorrhoids. Rev Esp Enferm Dig 97:97–103
Hemorrhoidal artery ligation versus rubber band ligation for the management of symptomatic second degree and third degree hemorrhoids (HubBle): a multicentre, one-label, randomized controlled trial. The Lancet Vol 388, issue 10042, P 356–364, July 23, 2016
Schuurman JP, Borel Rinkes IH, Go PM (2012) Hemorrhoidal artery ligation procedure with or without Doppler transducer in grade II and III hemorrhoidal disease: a blinded randomized clinical trial. Ann Surg 255(5):840–845
Nyström PO, Qvist N, Raahave D, Lindsey I, Mortensen N (2010) Stapled or open pile procedure (STOPP) trial study group. Randomized clinical trial of symptom control after stapled anopexy or diathermy excision for haemorrhoid prolapse. Br J Surg 97:167–176
Saxena P, Bhakuni YS (2017) A prospective study on suture ligation of internal hemorrhoids without Doppler guidance for the treatment of symptomatic hemorrhoid disease. Int Surg J 4:671–676
Avital S, Inbar R, Karin E, Greenberg R (2012) Five-year follow-up of Doppler-guided hemorrhoidal artery ligation. Tech Coloproctol 16:61–65
Pucher PH, Sodergren MH, Lord AC, Darzi A, Ziprin P (2013) Clinical outcome following Doppler-guided haemorrhoidal artery ligation: a systematic review. Color Dis 15(6):e284–e294
Ratto C, Parello A, Veronese E, Cudazzo E, D’Agostino E, Pagano C, Cavazzoni E, Brugnano L, Litta F (2015) Doppler-guided transanal haemorrhoidal dearterialization for hemorrhoid: results from a multicentre trial. Color Dis 17(1):O10–O19
Author information
Authors and Affiliations
Contributions
All authors contributed in the study.
Corresponding author
Ethics declarations
Ethical approval was obtained from the Institutional Ethics Committee.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ahmad, A., Kalimuddin, M., Sonkar, A.A. et al. A Randomized Clinical Study to Compare the Outcome of Hemorrhoidal Artery Ligation (HAL) Procedure with and without Doppler Guidance in Grades I–III Hemorrhoidal Disease. Indian J Surg 83, 1153–1157 (2021). https://doi.org/10.1007/s12262-020-02606-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-020-02606-z