
Abstract
Altered CD24, c-myc and phospholipase 2a expression was reported in different cancers. Our aim was to measure the expression of these genes in prostate cancer tissues, and compare it to non-cancerous samples. Prostate tissue samples were collected by needle biopsy from 20 prostate cancer (PCA) and 11 benign prostate hyperplasic (BPH) patients. RNA was isolated; cDNA synthetized, CD24, c-myc and phospholipase 2A (PL2A) expressions were determined by quantitative real-time PCR method. The expression of β-globin gene was measured for normalization of the gene expression results. Serum prostate specific antigen (PSA) levels were determined by microparticle enzyme immunoassay (MEIA) method. PSA levels were significantly different between the PCA and BPH groups, 252.37 ± 308.33 ng/ml vs. 3.5 ± 2.14 ng/ml (p = 0.001), respectively. CD24 expression was 988.86 ± 3041 ng/μl in prostate tumor and 4.00 ± 4.25 ng/μl in the BPH group (p = 0.035). The c-myc expression was 88.32 ± 11.93 ng/μl in the prostate tumor and 17.08 ± 21.75 ng/μl in the BPH group (p = 0.02), and the PL2A 31.36 ± 67.02 ng/μl was in PCA and 5.56 ± 14.08 ng/μl in BPH (p = 0.025). Gleason’s scores showed correlation with c-myc (p = 0.019) and PSA (p = 0.033) levels. Overexpression of PL2A, CD24 and c-myc was observed in prostate cancer samples using quantitative real-time PCR method.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer (PCA) is the second most common cancer in men. PCA develops slowly, this helps to use successful screening protocols to reduce mortality and morbidity [1]. Digital rectal examinations and serum prostate specific antigen (PSA) determinations are the most commonly used screening methods worldwide. PSA has an excellent sensitivity with a low specificity. There is a great interest to find more reliable diagnostic and prognostic markers. The molecular mechanisms playing role in the development of prostate cancer is not known yet [2]. Heterogeneity of PCA has been recognized long time ago which varies from asymptomatic to a rapidly fatal systemic malignancy [2–8]. Molecular biological methods are involved to find out similarities and differences, as well as get useful information for effective treatment and prognosis [5, 6].
The widely used biochemical, histopathological, Gleason score and prostate-specific antigen determinations had only limited success and produce significant variability in predictive value [6].
Recently, CD24 expression was described as a novel prognostic marker in different cancers including prostate [9–12]. CD24 is a small, heavily glycosylated mucin like glycosylphosphatidyl-inositol-linked cell surface protein, expressed in B cell lymphomas, renal cell carcinoma, bladder carcinoma, breast cancer and epithelial ovarian cancer. CD24 is an alternative ligand of P-selectin and an adhesion receptor on activated endothelial cells and platelets, it enhances the metastatic potential of tumor cells [11].
c-myc is an oncogene, member of the myc family. It is expressed during the fetal development with two other gene-family members MYCN and MYCL1, whereas only c-myc is expressed in adult tissues. c-myc is involved in apoptosis, genomic instability, growth, transformation, proliferation, angiogenesis and differentiation. Deregulation of c-myc was observed in many tumors including melanomas, carcinomas of breast, prostate and ovarian cancer. c-myc became as a target in molecular based treatment of cancer [13, 14]. Nupponen et al. observed specific amplification of c-myc in 72% of the androgen-independent prostate cancer samples using FISH method [8].
Phospholipase 2A (PL2A) has an important role in providing arachidonic acid for eicosanoids biosynthesis, these regulates the synthesis of prostaglandins, thromboxans, leukotrienes and lipoxins [15]. The production of arachidonic acid occurs mainly by activation of PL2A in response to different extracellular stimuli. Expression of PL2A was increased in several cancers, and it became as target for anticancer drugs [16].
We decided to establish a suitable model to determine the expression of PL2A, CD24 and c-myc in prostate tissue samples using quantitative real-time PCR method, and verify the PCR method with MEIA.
Patients and Methods
Patients
Prostate tissue samples were obtained by transrectal ultrasound guided needle biopsy from non-treated 20 prostate cancer (PCA) and 11 benign prostate hyperplasic (BPH) patients from October of 2005 to March of 2006. The number of the biopsy samples was determined by Vienna nomogramm, a program which consider the age of the patient and the volume of the prostate (min. four samples/patients). In the case of the PCA patients the ratio of the tumor cells were 80–100% in the prostates based on the histopathological examinations.
The selection of patients was based on digital rectal examinations and on serum PSA levels, it was confirmed by histological examination later. Gleason’s grades were assigned. The average age of the patients was 72.0 ± 8.8 years for PCA and 64.3 ± 12.1 years for BPH. The Ethical Committee of the Semmelweis University has approved the study and all patients agreed to be involved in the study and informed consent was signed.
Prostate tissue samples were transferred to a 1.5 ml Eppendorf tubes containing 0.5 ml of DNA/RNA Stabilization Reagent (Roche, Mannheim, Germany) and kept at −85°C until the RNA isolation.
PSA Determination
Pre-biopsy PSA levels were determined by using microparticle enzyme immunoassay (MEIA) method on Abbott IMx using PSA kit (Abbott Park, IL, USA).
RNA Isolation
During the RNA isolation tissue samples were moved to a lysing matrix tubes containing 0.3 ml RNA lysis puffer and were treated with FastPrep Bio101 tissue destroyer centrifuge (Thermo Savant, Holbrook, NY, USA). Perfect RNA Eukaryotic kit was used (Eppendorf, Hamburg, Germany) for RNA isolation from the samples according to the instructions of the manufacturer.
cDNA Synthesis
Complementary cDNA was synthetized using DNase-I-treated total RNA with First Stand cDNA synthesis kit for RT-PCR (Roche Diagnostic Corp., Indianapolis, IN, USA) according to the manufacturer’s instructions.
Quantitative Real-time PCR
We used two kind of gene expression determination, SYBRGreen I (for β-globin, PL2A and c-myc) and primer-probe system (CD24) [17–19]. CD24 expression was determined according to a previously described method [17]. c-myc and PL2A gene specific primers were designed and synthesized by TIB MOLBIOL (Berlin, Germany) [18, 20]. The house-keeping gene β-globin expression was measured and used for normalization of the gene expression results. β-globin (DNA Control kit, Roche) DNA was used in each PCR run in 15 ng/μl, 1.5 ng/μl, 0.15 ng/μl and 0.015 ng/μl concentration according to the manufacturer’s instructions.
Quantitative polymerase chain reaction was performed using LightCycler (Roche) for determination of β-globin, PL2A and c-myc expressions, each PCR-mix consisted of 1 μl of DNA Master SYBR Green I mix (LC FastStart DNA Master SYBR Green I kit, Roche), in the case of CD24 expression measurements, 1 μl of FastSart DNA Master mix (LC FastStart DNA Master HybProbe, Roche), 1.2 mM MgCl2, and 0.25 pmol of primers and probes [14, 17–19]. The amplification program included an initial denaturation at 95°C with 10 min hold, followed by 40 cycles with denaturation at 95°C with 10 s hold, annealing at 56°C and 65°C with 5 s hold and extension at 72°C with 10 s hold. Amplifications were followed by melting curve analysis. Each sample was run in duplicates and a negative control (d. water) was used for in each run.
Statistical Analysis
Student T-test was used for the statistical evaluation of the data (with paired comparisons), the level of significance was determined as p ≤ 0.05 (SPSS, Chicago, IL, USA).
Results
We determined the PL2A, CD24 and the c-myc expression in prostate tissue of 20 prostate cancer (PCA) and 11 benign prostate hyperplasic (BPH) patients using quantitative real-time PCR method. The level of prostate specific antigen was measured by microparticle enzyme immunoassay (MEIA) in all patients.
The level of PSA was 252.37 ± 308.33 ng/ml in the PCA and 3.50 ± 2.14 ng/ml in the BPH group (p = 0.001).
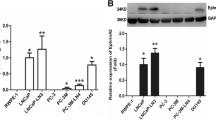
CD24 expression was 988.86 ± 3041 ng/μl in the PCA and 4.00 ± 4.25 ng/μl in the BPH group (p = 0.035), while the c-myc expression was 88.32 ± 11.93 ng/μl and 17.08 ± 21.75 ng/μl (p = 0.02). The expression of PL2A was 31.36 ± 67.02 ng/μl and 5.56 ± 14.08 ng/μl (p = 0.025).
The mean Gleason’s grade was 7.60 ± 1.31, 11 patients had higher than 7. Gleason’s grades showed correlation with c-myc (p = 0.019) and PSA (p = 0.033) levels. We used Student t-test for the comparison of the data. Table 1 shows the summarized gene expression results.
Discussion
Prostate cancer is the second leading cause of death in the US and in Europe. PCA is a heterogeneous disease and the outcome is hardly predictable [2]. Digital rectal examination and serum PSA level measurements are the main tools in the diagnostic protocols.
Recently, molecular biological methods including comparative genomic hybridization, immunohistochemistry, microarray and quantitative real-time PCR determinations were involved in the searching process to find out the molecular mechanism of the development of prostate cancer, and to find new diagnostic and prognostic markers [6, 18, 21].
From these studies one promising molecule was found recently, the CD24 [17]. This molecule has been studied in hematological malignancies mostly before, and lately in different kind of tumors [22–26]. Kristiansen et al. [12] and Schostak et al. [19] made significant work to find out the role of CD24 in prostate cancer. Our results are in concordance with their findings.
We used two types of gene expression measurements for the determination of the gene expressions, SYBRGreen I was used in the case of PL2A and c-myc, while the primer-probe system for the CD24. As the comparisons were made in the two patients groups using same method, it does not have effect on the results.
The expression of the PL2A was significantly higher in the PCA group. Several studies demonstrated increased expression of PL2A in several human cancers including prostate. Dong et al. found 22 times higher levels. sPL2A (IIA) was increased in seminal fluid and for use as diagnostic marker was recommended [33]. PL2A mediates carcinogenesis by the release of arachidonic acid which induces cancer cell growth and proliferation [35]. Hughes-Fulford et al. found that arachidonic acid induces cPLA2 in prostate carcinoma cells and it depends on downstream synthesis of PGE2. They recommended PL2A as pharmaceutical target for treatment of cancer [32, 34].
We found significant overexpression of CD24 in 21 prostate cancer samples. The levels showed association with serum PSA levels and Gleason’s grades. We measured the c-myc expressions and we found similar association. We suppose the measurement of the expression of these could give valuable information for the clinicians. We realize also that studies using higher number of patients are necessary to get final conclusion on the clinical importance on PL2A, c-myc and CD24 expression.
Overexpression of c-myc was described in different tumors including PCA, whereas during our literature search we did not find any quantitative real-time PCR determination. Jenkins et al. used fluorescence in situ hybridization for the detection of c-myc amplification in prostate carcinoma [27]. Devi et al. studied the effect of β-hCG on prostate cells and they found that antisense phosphorodiamidate morpholino oligomers caused specific decrease of the target [14]. Bernard et al. showed that overexpression of c-myc is sufficient to induce androgen-independent growth. It does not have effect through androgen-receptors, as c-myc did not increase PSA expression and did not increase PSMA expression [28]. Another very interesting finding, is that c-myc could immortalize human prostate epithelial cells. They suppose that c-myc has role in the early stages of PCA. The oncogenic myc potentiate apoptosis, whereas Bcl-2 activation inhibits it [28].
c-myc became a target in gene therapy recently. There are very promising experiments in cancer cells, where blocking myc results in tumor regression [29, 30]. Data of these experiments supports the idea that targeting myc in tumors represents a valid therapeutic approach.
Lately, Liu et al. published an article about the protein expression of CD24 molecule. They found that CD24 is highly expressed in most of primary tumors, including prostate, and the two types of prostate tumors, the glandular and the non-glandular tumors are not different related to the CD24 expression [31].
In this study we determined the CD24, the c-myc and PL2A expressions. We found overexpression of c-myc and PSA, they showed correlation with Gleason’s grades. We need higher number of patients and longer time to collect useful data on survival. These markers could be involved in the diagnostic tools.
References
Müller H, Brenner H (2006) Urine markers as possible tools for prostate cancer screening: review of performance characteristics and practicality. Clin Chem 52:562–573
Kopper L, Timár J (2005) Genomics of prostate cancer: is there anything to “translate”. Pathol Oncol Res 11:197–203
Maitland NJ, Collins A (2005) A tumour stem cell hypothesis for the origins of prostate cancer. BJU Int 96:1219–1223
Hughes C, Murphy A, Martin C et al (2005) Molecular pathology of prostate cancer. J Clin Pathol 58:673–684
Quinn DI, Henshall SM, Sutherland LR (2005) Molecular markers of prostate cancer outcome. Eur J Cancer 41:858–887
Glinsky VG, Glinskii BA, Stephenson JA et al (2004) Gene expression profiling predicts clinical outcome of prostate cancer. J Clin Invest 113:913–923
Prowatke I, Devens F, Benner A et al (2006) Expression analysis of imbalanced genes in prostate carcinoma using tissue microarrays. Br J Cancer 96:82–88
Nupponen NN, Kakkola L, Koivisto P et al (1998) Genetic alterations in hormone refractory recurrent prostate carcinomas. Am J Pathol 153:141–148
Kristiansen G, Denkert C, Schlüns K et al (2002) CD24 is expressed in ovarian cancer and is a new independent prognostic marker of patients survival. Am J Pathol 161:1215–1221
Kristiansen G, Schlüns K, Yongwei Y et al (2003) CD24 is an independent prognostic marker of survival in non-small cell lung cancer patients. Br J Cancer 88:231–236
Kristiansen G, Winzer KJ, Mayordomo E et al (2003) CD24 expression is a new prognostic marker in breast cancer. Clin Cancer Res 9:4906–4913
Kristiansen G, Pilarsky C, Pervan J et al (2004) CD24 expression is a significant predictor of PSA relapse and poor prognosis in low grade or organ confined prostate cancer. Prostate 58:183–192
Ponzielli R, Katz S, Barsyte-Lovejoy D et al (2005) Cancer therapeutics: targeting the dark side of Myc. Eur J Cancer 41:2485–2501
Devi RG, Oldenkamp RJ, London AC et al (2002) Inhibition of human chorionic gonadotropin β-subunit modulates the mitogenic effect of c-myc in human prostate cancer cells. Prostate 53:200–210
Hirabayashi T, Shimuzu T (2000) Localization and regulation of cytosolic phospholipase A2. Biochim Biophys Acta 1488:124–138
Dong Q, Patel M, Scott KF et al (2006) Oncogenic action of phospholipase A2 in prostate cancer. Cancer Letters 240:9–16
Wikmam H, Seppanen JK, Sarhadi VK et al (2004) Caveolins as tumor markers in lung cancer detected by combined use of cDNA and tissue microarrays. J Pathol 203:584–593
Kettunen E, Nicholson AG, Nagy B et al (2005) L1CAM, INP10, P-cadherin, tPA and ITGB4 overexpression in malignant pleural mesothelioma primary tumors revealed by combined use of cDNA and tissue microarray. Carcinogenesis 26:17–25
Schostak M, Krause H, Miller K et al (2006) Quantitative real-time RT-PCR of CD24 mRNA in the detection of prostate cancer. BMC Urol 119:1396–1402
Nagy B, Lundan T, Larramendy ML et al (2003) Abnormal expression of apoptosis-related genes in haematological malignancies: overexpression of MYC is poor prognostic sign in mantle cell lymphoma. Br J Haematol 120:434–441
Ohl F, Jung M, Xu C et al (2005) Gene expression studies in prostate cancer tissue: with reference gene should be selected for normalization? J Mol Med 83:1014–1024
Calvo A, Gonzalez-Moreno O et al (2005) Prostate cancer and the genomic revolution: advances using microarray analyses. Mut Res 576:66–79
Raife TJ, Lager DJ, Kemp JD et al (1994) Expression of CD24 (BA-1) predicts monocytic lineage in acute myeloid leukemia. Am J Clin Pathol 101:296–299
Jackson D, Waibel R, Weber E et al (1992) CD24, a signal-transducing molecule expressed on human B cells, is a major surface antigen on small cell lung carcinomas. Cancer Res 52:5264–5270
Huang LR, Hsu HC (1995) Cloning and expression of CD24 gene in human hepatocellular carcinoma: a potential early tumor marker gene correlates with p53 mutation and tumor differentiation. Cancer Res 55:4717–4721
Pirrucello SJ, Lang MS (1990) Differential expression of CD24-related epitopes in mycosis fungiodes/Sezary syndrome: a potential marker for circulating Sezary cells. Blood 76:895–905
Jenkins RB, Qian J, Lieber MM et al (1997) Detection of c-myc oncogene amplification and chromosomal anomalies in metastatic prostatic carcinoma by fluorescence in situ hybridization. Cancer Res 57:524–531
Bernard D, Pourtuer-Manzanedo A, Gil J et al (2003) Myc confers androgen-independent prostate cancer cell growth. J Clin Invest 112:1724–1731
Shachaf CM, Kopelman AM, Arvanitis C et al (2004) MYC inactivation uncovers pluripotent differentiation and tumour dormancy in hepatocellular cancer. Nature 431:1112–1117
Arnold I, Watt FM (2001) c-Myc activation in transgenic mouse epidermis results in mobilization of stem cells and differentiation of their progeny. Curr Biol 11:558–568
Liu YA, Roudier PM, True DL (2004) Heterogeneity in primary and metastatic prostate cancer as defined by cell surface CD profile. Am J Pathol 165:1543–1556
Hughes-Fulford M, Tjandrawinata RR, Li C-F et al (2005) Arachidonic acid, an omega-6 fatty acid, induces cytoplasmic phospholipase A2 in prostate carcinoma cells. Carcinogenesis 26:1520–1526
Kallajoki M, Alanen KA, Nevalainen M et al (1998) Group II phospholipase A2 in human male reproductive organs and genital tumors. Prostate 35:263–272
Shimuzu M, Matsumoto Y, Kurosawa T et al (2008) Release of arachidonic acid induced by tumor necrosis factor-α in the presence of caspase inhibition: evidence for cytosolic phospholipase A2α-independent pathway. Biochem Pharmacol doi:10.1016/j.bcp.2007.11.020
Cummings BS (2007) Phospholipase A2 as targets for anticancer drugs. Biochem Pharmacol 74:949–959
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nagy, B., Szendroi, A. & Romics, I. Overexpression of CD24, c-myc and Phospholipase 2A in Prostate Cancer Tissue Samples Obtained by Needle Biopsy. Pathol. Oncol. Res. 15, 279–283 (2009). https://doi.org/10.1007/s12253-008-9077-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12253-008-9077-1