
Abstract
Background
Prior studies found that pain fear avoidance and pain acceptance are significantly associated with adjustment to chronic pain.
Purpose
The purpose of this study is to compare the influence of pain fear avoidance and pain acceptance on adjustment to chronic pain across three samples: patients with chronic back pain treated at primary care centres, patients with heterogeneous pain conditions treated at a pain clinic and patients with pain associated with inflammatory bowel disease.
Methods
Structural equation modelling was used to test for differences between groups in the linear relationships between variables.
Results
The model had the best fit for the group of patients with back pain. Three significant relationships were equal across the groups: experiential avoidance on pain fear avoidance, pain intensity on pain fear avoidance, and pain fear avoidance on negative mood.
Conclusions
The associations between both pain fear avoidance and pain acceptance and adjustment to chronic pain vary depending on the pain condition and the type of health care centres where the patients are treated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since 1983, when the fear-avoidance model of pain was first proposed [1], decades of intense research has demonstrated the influence of persistent avoidance behaviours motivated by fear on the development of disability [2–5]. Although the model was developed to explain chronicity of low back pain, it has been suggested that the model may be equally applicable to other chronic pain conditions [4]. Anxiety sensitivity was included by Norton and Asmundson [6] in the fear-avoidance model as a vulnerability variable, which could explain individual differences in fear of pain. Several studies have investigated the role of other vulnerability variables such as neuroticism and experiential avoidance [7, 8]. Both anxiety sensitivity and experiential avoidance are dispositional variables associated with negatively experiencing internal events [9]; however, whereas experiential avoidance involves negative private experiences in general, anxiety sensitivity specifically involves arousal-related body sensations. A recent study in a sample of patients with chronic back pain found that experiential avoidance and anxiety sensitivity independently contributed to pain fear avoidance [8].
Apart from the process that leads to disability, the original fear-avoidance model of pain identified another “positive” pathway, which leads to recovery: noncatastrophising patients do not develop pain-related fear and quickly resume their daily activities. Despite its importance, this response pattern has been little studied [3]. In recent years, numerous studies have shown that acceptance of chronic pain is associated with less disability and distress and decreased use of healthcare resources [10–12]. Acceptance of pain might represent an adaptive form of “confrontation” in contrast to avoidance since pain acceptance includes responding to pain-related experiences without attempts at control or avoidance and engaging in valued activities and reaching personal goals regardless of these experiences [13].
The role of dispositional variables which could be associated with individual differences in pain acceptance has also been investigated. Resilience, conceptualised as a relatively stable personal trait characterised by the ability to adapt to adversity [14], could explain individual differences in pain acceptance. A pioneering study [15] established the characteristics that constitute resilience: having a balanced perspective on life, perseverance, self-reliance, attributing a meaning to life, and existential aloneness. Several authors have suggested that the concepts of resilience and acceptance are interconnected [16, 17]; it has even been proposed that some measures of psychological resilience contain measures of psychological acceptance [16]. Thus, resilient people with a relatively stable tendency to display an accepting attitude in life will probably develop accepting behaviour when faced with chronic pain. Some studies have concluded that resilience is relevant in predicting pain, physical functioning and emotional well being in patients with chronic pain [18–24]. Specifically, two studies on patients with chronic back pain found that resilience was highly associated with pain acceptance [25, 26].
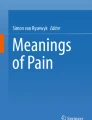
In line with the aforementioned research, a hypothetical model was proposed in which anxiety sensitivity and experiential avoidance were included as dispositional variables, which would be associated with individual differences in pain fear avoidance. In addition, resilience was postulated as a dispositional variable associated with individual differences in pain acceptance. Pain intensity is postulated to be associated with pain fear avoidance. At the same time, pain fear avoidance and pain acceptance would be associated with daily functioning and negative mood (Fig. 1). Although two studies have investigated the validity of this model in patients with chronic back pain treated in primary care centres [8, 25], no research has been conducted on other groups of patients; this raises the question of whether the model can be generalised to patients with other pain conditions treated by other health services. Thus, the aim of this cross-sectional study was to test for differences across three groups of patients in the linear relationships between the variables included in this hypothetical model: patients with chronic back pain treated at primary care centres, patients with heterogeneous pain conditions treated at a pain clinic and patients with pain associated with inflammatory bowel disease (IBD). Patients with back pain treated at primary care centres were compared to patients treated at a pain clinic because patients who have been referred to this type of specialised health service are characterised by being highly impaired [27]. Patients with IBD were also of interest because, unlike chronic back pain, pain is a prevalent symptom that is associated with this specific illness and is one symptom among many others [28]. According to previous studies, since the fear-avoidance model [1, 2] was developed to account for chronicity of low back pain where avoidance of activity plays a central role in the explanation of disability, it was predicted that the present model would better represent the sample of patients with chronic back pain treated at primary care centres.

Hypothetical model. ASI1 Physical Concerns Subscale, Anxiety Sensitivity Index; ASI2 Cognitive Concerns Subscale, Anxiety Sensitivity Index; ASI3 Social Concerns Subscale, Anxiety Sensitivity Index; AAQ Acceptance and Action Questionnaire; INDEX Composed Pain Intensity Index; SF-36 PAIN Bodily Pain Subscale, SF-36; RS1 Personal Competence Subscale, Resilience Scale; RS2 Acceptance of Self and Life Subscale, Resilience Scale; PCS Pain Catastrophising Scale; PVAQ Pain Vigilance and Awareness Questionnaire; PASS Pain Anxiety Symptoms Scale; CPAQ1 Activity Engagement Subscale, Chronic Pain Acceptance Questionnaire; CPAQ2 Pain Willingness Subscale, Chronic Pain Acceptance Questionnaire; HADS-ANX Anxiety Subscale, Hospital Anxiety and Depression Scale; HADS-DEP Depression subscale, Hospital Anxiety and Depression Scale; IFI-FUNC Functioning Subscale, Impairment and Functioning Inventory; IFI-IMP Impairment subscale, Impairment and Functioning Inventory. Latent variables are represented by circles and observed variables by squares
Methods
Participants
The participants consisted of a consecutive sample of 419 patients with chronic pain divided into three groups. The recruitment process lasted from October 2010 to October 2011. Individuals were considered eligible for inclusion if, at the moment of their participation in the study, they were experiencing pain and had been experiencing pain for at least the last 3 months; were not being treated for a malignancy, terminal illness or psychiatric disorder; and were able to understand the Spanish language. The doctors who participated in the study reviewed the patients’ clinical history and if the patients fulfilled the inclusion criteria, their participation was requested. No one refused participation. Thirteen participants provided incomplete data and were excluded from the analyses. Thus, the final sample included 406 participants: 128 patients with IBD who were treated at a gastro-intestinal and internal medicine unit, 141 patients with back pain who were treated at four primary care centres and 137 with various pain conditions who were treated at a pain management unit.
Patients with pain related to inflammatory bowel disease
The IBD group consisted of 58 men and 70 women: 51 % were currently married or living together and 44 % were single. The average age was 37.91 years (SD = 12.39). Thirty-eight per cent had received primary education alone, and 32 % were university graduates. Forty-five per cent were employed, 19 % were unemployed, 17 % were homemakers and 11 % were retired. All the members of this group had been diagnosed with IBD, met the Rome II criteria for IBD [29] and had an endoscopically and histologically confirmed diagnosis of Crohn’s disease or ulcerative colitis. According to the inclusion criteria, at the moment of their participation in the study, all of them were experiencing pain and had been experiencing pain for at least the last 3 months. The mean duration of pain was 63.88 months (SD = 58.33). The mean number of days in pain per week was 3.97 (SD = 2.27). The average number of pain-free periods since pain onset was 4.14 (SD = 5.03) with a mean duration of 5.56 months (SD = 5.49). Fourteen patients had undergone one surgical intervention related to IBD, and eight patients had undergone between two and four surgical interventions related to IBD. The mean number of pain medications prescribed was .24 (SD = 0.53; range, 0–3).
Patients with back pain treated at primary care centres
The back pain group consisted of 64 men and 77 women: 69 % were currently married or living together. The average age was 45.75 years (SD = 12.44). Thirty-seven per cent had received primary education alone, and 37 % had completed high school. Fifty-four per cent were employed, 15 % were unemployed, 16 % were homemakers and 12 % were retired. All the members of this group had back pain in the following regions: cervical, 21.28 %; thoracic, 2.84 %; lumbar, sacral and coccygeal, 63.12 %; and generalised spinal pain, 12.76 %. The mean duration of pain was 53.05 months (SD = 70.01). The mean number of days in pain per week was 6.25 (SD = 0.75). The average number of pain-free periods since pain onset was 1.52 (SD = 4.10) with a mean duration of 1.19 months (SD = 7.62). Six patients had undergone one pain-related surgical intervention, and the mean number of pain-related medications prescribed was 1.31 (SD = 1.10; range, 0–5).
Patients with different pain conditions treated at a pain clinic
The specialty pain clinic group consisted of 60 men and 77 women: 76 % were currently married or living together. The average age was 53.20 years (SD = 13.21). Thirty-eight per cent had received primary education alone, and 25 % had completed high school. Fifty-three per cent were retired, 24 % were homemakers and 17 % were employed. In total, 48.18 % had relatively generalised pain syndromes (i.e. peripheral neuropathy, complex regional pain syndromes, polymyalgia rheumatica, fibromyalgia, rheumatoid arthritis or osteoarthritis) according to the classification of the International Association for the Study of Pain [30]; 7.30 % had relatively localised syndromes of the head and the neck; 14.60 % had cervical spinal pain syndromes; 1.45 % had thoracic spinal pain; 22.63 % had lumbar, sacral and coccygeal spinal pain; 5.11 % had local syndromes of the lower limbs; and 0.73 % had genital pain.
The mean duration of pain was 107.16 months (SD = 97.34). The mean number of days in pain per week was 6.64 (SD = 0.36). The average number of pain-free periods since pain onset was 0.28 (SD = 0.08) with a mean duration of 1.46 months (SD = 10.85). Twenty-five patients had undergone one pain-related surgical intervention; nine patients, two interventions; and 14 between three and eight interventions. The mean number of pain medications prescribed was 2.21 (SD = 1.15; range, 1–5).
Procedure
This research project was approved by the Carlos Haya Hospital Ethics Committee. To guarantee the standardisation of the recruitment process across the three centers, and prior to data collection, the researchers held a meeting with the participating doctors in which the eligibility criteria were explained and the procedures were decided on.
At the end of their visit to their doctor, each patient who fulfilled the eligibility criteria was informed of the study aims and their participation was requested. Some patients were interviewed after their visit, whereas others left their telephone number to make an appointment on another day. Informed consent was obtained prior to data collection. The participants were aware that the information collected was confidential and that this information would be linked to a number alone and not to their name. Each participant had a semi-structured interview with a psychologist to obtain demographic, social or medical history data. A battery of questionnaires was also completed by each participant. Patients with back pain were interviewed in their usual primary care centre, patients with IBD were interviewed in the gastro-intestinal and internal medicine unit and patients with heterogeneous pain conditions were interviewed in the pain clinic.
Measures
Anxiety Sensitivity Index
This is a 16-item questionnaire where respondents indicate the degree to which they fear the negative consequences of anxiety symptoms on a 5-point Likert-type scale [31]. It has three subscales: Physical, Cognitive, and Social Concerns. The Spanish version of the Anxiety Sensitivity Index (ASI) is fully equivalent to the original. The results of validation studies provide cross-cultural evidence for construct validity and the concurrent validity of the Spanish ASI [32].
Acceptance and Action Questionnaire
This questionnaire assesses experiential avoidance [33]. The Spanish version of the Acceptance and Action Questionnaire (AAQ) [34] was used in this study. It consists of nine items in which participants are asked to rate each statement on a 7-point scale. Higher scores indicate higher levels of avoidance and immobility. The Spanish AAQ is a stable, internally consistent and valid scale.
The Resilience Scale
This scale consists of 25 items arranged in two subscales: personal competence (17 items) and acceptance of self and life (eight items) [35]. The construct validity of the Resilience Scale (RS) was supported by correlations with measures of self-esteem and perceived stress. The RS has been adapted to the Spanish-speaking population [36]. The RS has been adapted into Spanish for patients with chronic musculoskeletal pain [37]. This version showed good internal consistency and test–retest reliability. Furthermore, the scale shows good concurrent validity with measures of adjustment to chronic pain.
Pain Catastrophising Scale
This scale is a 13-item measure in which respondents indicate on a 5-point scale the degree to which they experience various thoughts and feelings while in pain [38]. It consists of three subscales assessing rumination, magnification and helplessness, and also provides a total score on catastrophising. The total score alone was used in this study. The Spanish Version of the scale shows good reliability and validity and its internal consistency is high [39].
Pain Vigilance and Awareness Questionnaire
This instrument assesses awareness, vigilance, preoccupation and observation of pain [40]. The original Pain Vigilance and Awareness Questionnaire (PVAQ) consists of 16 items and has been validated for use in chronic pain samples and nonclinical samples. The Spanish version consists of two related subscales, corresponding to two factors: active vigilance and passive awareness. The total scale and the subscales show good internal consistency. Both subscales and the total score are positively and significantly correlated with other fear-related constructs: fear-avoidance beliefs, pain anxiety, and pain catastrophising [41].
Pain Anxiety Symptoms Scale
This is a 40-item measure of anxiety and fear responses associated with chronic pain [40]. It consists of four subscales, which measure (a) cognitive anxiety responses, (b) escape and avoidance, (c) fearful thinking and (d) physiological anxiety responses. The psychometric properties of the Pain Anxiety Symptoms Scale (PASS) subscales and total score are highly reliable [42]. The total score alone was used in this study. The Spanish version of the questionnaire [43] shows high internal consistency.
Chronic Pain Acceptance Questionnaire (CPAQ)
We applied the Spanish version of the questionnaire Chronic Pain Acceptance Questionnaire (CPAQ-SV) [44, 45]. This instrument consists of 20 items. Similar to the original questionnaire, the CPAQ-SV yields a total score and two subscale scores for pain willingness and activity engagement. The subscales of the CPAQ-SV show good internal consistency [45]. Two studies on the CPAQ-SV [45, 46] have supported the validity of a 20-item version with two subscales corresponding to two independent factors. In addition, the CPAQ-SV demonstrates good criterion validity [45].
Hospital Anxiety and Depression Scale
This is a self-reporting scale that contains two seven-item scales, one for anxiety and one for depression [47]. The Spanish version of the scale shows appropriate reliability and validity. The internal consistency of both scales is high [48].
Impairment and Functioning Inventory
This consists of 30 items each referring to an activity related to one of the following areas: household, autonomous behaviour, leisure, and social relationships [49]. First, the patients are asked whether they performed an activity during the previous week. If they have, they are asked about frequency, but if they have not, they are asked whether they practiced this activity before suffering chronic pain. This approach differentiates between present functioning and impairment and is useful in assessing patients with a long history of pain where the degree of deterioration is at least as informative as the current level of functioning. The Impairment and Functioning Inventory has been specifically developed for patients with chronic pain and takes into account the distinguishing features of Spanish culture. The instrument provides an index of functioning, an index of impairment and scores for each of these areas. The subscales and global scales are very reliable.
Pain Intensity Index
Patients were asked to rate their mildest, average and worst pain during the past 2 weeks, as well as their current pain, on a scale ranging from 0 to 10, with a “0” indicating “no pain” and “10” indicating pain as “intense as you could imagine”. A composite pain intensity score was calculated for each subject by calculating the average of the mildest, average, worst and current pain. Composites of the 0–10 ratings are very reliable measures of pain intensity in chronic pain patients [50].
Bodily Pain Scale (SF-36)
This scale is taken from the Spanish Version of the SF-36 Health Survey and is composed of two items [51, 52]. Patients indicate on a 6- and 5-point scale, respectively, pain intensity and pain interference on daily life during the past 4 weeks. The score of the scale was calculated following the algorithms for the original version and ranges from 0 to 100. The scale has high internal consistency (α = .84).
Statistical Analysis
First, the three groups were compared in relation to the following variables: sex, age, marital status, duration of pain in months and educational level. When there were significant differences between the groups in one variable, this variable was correlated with the variables included in the model to determine whether it represented a possible confounder between groups; if the correlation was significant, this variable was included as a covariate in the rest of the analysis. An analysis of covariance was used to determine mean differences between the three groups in relation to the variables included in the hypothetical model. Multi-sample analyses were then performed to test the statistical significance of the parameter differences between the three groups by structural equation modelling using LISREL 8.30 software [53]. LISREL 8.30 can simultaneously analyse data from multiple samples and compare differences in model fit when some or all parameters are considered equal between groups. Finding a statistically significant improvement in fit when freeing a parameter between multiple groups indicates that the parameter value is different between the groups tested.
The data were checked prior to the analyses and we found that some variables were not normally distributed. Thus, the estimation method used was maximum likelihood because this method is effective for any distribution of the data if the analyses are performed on covariance matrices and the matrix of fourth-order moments is provided [54]. The covariance matrices used in this study are available in the Electronic Supplementary Material (ESM). In a multi-sample analysis, χ 2 is a measure of overall fit of all models in all groups and cannot be decomposed into a χ 2 for each group separately [53]. In multi-sample analyses, it is first assumed that all the parameters are the same in all groups; this forms the baseline model. Next, successive models are estimated in which each parameter, one by one, is allowed to vary for each group. The relative fit across the groups is compared in relation to the changes in χ 2. If, compared to the baseline model, the change in χ 2 is significant—that is, the model shows a better fit—it can be concluded that the parameters are significantly different across the groups.
Eleven latent variables—anxiety sensitivity, experiential avoidance, pain intensity, resilience, pain fear avoidance, pain acceptance, negative mood, daily functioning, educational level, age and time in pain—were associated in a hypothetical structural equation model (Fig. 1). Pain fear avoidance and pain acceptance were allowed to covariate. Seventeen observable variables or indicators of the latent variables were used. Anxiety sensitivity was specified by the three subscales of the Anxiety Sensitivity Index: physical concerns, cognitive concerns, and social concerns. Resilience was specified by the two subscales of the Resilience Scale: personal competence and acceptance of self and life. Pain intensity was specified by the Composite Pain Intensity Index and the Bodily Pain scale of the SF-36. Pain fear avoidance as a latent construct was specified by pain catastrophising (PCS), hypervigilance (PVAQ) and pain anxiety (PASS). As in a previous study [8], these three observable variables were combined in a latent variable because they were highly correlated; some authors have suggested that they seem to share some potential overlap [4]. Pain acceptance was specified by the two subscales of the Pain Acceptance Questionnaire: activity engagement and pain willingness. Negative mood was specified by the two subscales of the Hospital Anxiety and Depression Scale: anxiety and depression. Daily functioning was specified by the two subscales of the Impairment and Functioning Inventory: functioning and impairment. One loading for each latent variable was fixed at 1.0 for setting the metric of the latent construct.
Experiential avoidance, educational level, age, and time in pain were measured by one variable; thus, the error variance was fixed at 0 and the loading value at 1. To avoid clutter, the covariates educational level, age, and time in pain have not been included in Fig. 1.
Results
Covariates
One-way analyses of variance between groups indicated significant differences in age [M IBD = 37.91, SDIBD = 12.39; M back pain = 45.75, SDback pain = 12.44; M pain unit = 53.20, SDpain unit = 14.01; F(2, 403) = 47.99, P < .000], duration of pain in months [M IBD = 63.88, SDIBD = 58.33; M back pain = 53.05, SDback pain = 70.01; M pain unit = 107.16; SDpain unit = 97.34; F(2, 403) = 18.87, P < .000] and educational level [M IBD = 12.13, SDIBD = 3.50; M back pain = 6.76, SDback pain = 1.95; M pain unit = 6.01, SDpain unit = 2.34; F(2, 401) = 14.97, P < .000]. Therefore, these variables were used as covariates in the model for the variables with which they were significantly correlated.
Univariate comparisons between groups
Table 1 shows the estimated marginal means and standard errors for anxiety sensitivity, experiential avoidance, resilience, pain catastrophising, pain hypervigilance, pain anxiety, pain acceptance, pain intensity (index and SF-36 bodily pain), anxiety, depression, functioning and functional impairment, the F value for the main effect of group in the analyses of covariance and the results of the post hoc comparisons using the Scheffé test. The results of analyses of covariance indicated that there were significant mean differences between the groups in all the variables, except for anxiety. Post hoc comparisons indicated that the patients with IBD had lower anxiety sensitivity than the other two groups and that the patients with back pain showed lower experiential avoidance than the other two groups. In relation to pain catastrophising, pain anxiety, bodily pain, pain intensity and functional impairment, the means of the three samples were significantly different: Patients with IBD had the lowest means, followed by patients with back pain and the patients treated at the pain clinic had the highest means. The three samples were also significantly different regarding depression: In this case, the patients with back pain had the highest mean, followed by the patients treated at the pain clinic and the patients with IBD had the lowest mean. Regarding pain hypervigilance, the patients from the pain clinic had a significantly higher mean than the other two groups. In relation to pain acceptance, the patients from the pain clinic had a significantly lower mean than the means of the other two groups. Patients with back pain showed better functioning than the other two groups, which did not significantly differ. Finally, regarding resilience, patients with IBD showed a significantly higher mean than the mean of the patients treated at the pain clinic.
Measurement Model
The invariance of the measurement model between groups has to be examined before multi-group hypotheses are submitted to further testing [55]. The complete measurement invariance assumption was tested first, and the results indicated that this model had a poor fit between the three groups [χ 2 (546) = 2,765.26, P = .000]; when LISREL 8.30 was used to calculate the factor loadings for each group, significant changes in χ 2 were found [χ 2 (438) = 2610.86; Δχ 2 (8) = 154.40, P = .000]. Thus, the multi-sample confirmatory analysis indicated that complete invariance between factor loadings between the three groups could not be justified for one of the latent constructs: pain fear avoidance. In a situation when not all the measures operate in the same way between groups, some researchers [56] have demonstrated that it is possible to proceed under the condition of “partial measurement invariance”, which refers to a situation when there is invariance for only some of the measures between groups. Thus, the baseline model for the three groups was obtained under the condition of partial measurement invariance, which constrained all the parameter estimates to be equal for the three groups except for the factor loadings of “pain hypervigilance” and “pain anxiety” on the latent variable “pain fear avoidance”. These factor loadings were freely estimated between the three groups (see Fig. 2).

Empirical model. ASI1 Physical Concerns Subscale, Anxiety Sensitivity Index; ASI2 Cognitive Concerns Subscale, Anxiety Sensitivity Index; ASI3 Social Concerns Subscale, Anxiety Sensitivity Index; AAQ Acceptance and Action Questionnaire; INDEX Composed Pain intensity index; SF-36 PAIN Bodily Pain Subscale, SF-36; RS1 Personal Competence Subscale, Resilience Scale; RS2 Acceptance of Self and Life Subscale, Resilience Scale; PCS Pain Catastrophising Scale; PVAQ Pain Vigilance and Awareness Questionnaire; PASS Pain Anxiety Symptoms Scale; CPAQ1 Activity Engagement Subscale, Chronic Pain Acceptance Questionnaire; CPAQ2 Pain Willingness Subscale, Chronic Pain Acceptance Questionnaire; HADS-ANX Anxiety subscale, Hospital Anxiety and Depression Scale; HADS-DEP Depression subscale, Hospital Anxiety and Depression Scale; IFI-FUNC Functioning Subscale, Impairment and Functioning Inventory; IFI-IMP Impairment subscale, Impairment and Functioning Inventory. Latent variables are represented by circles and observed variables by squares. B Back pain, I IBD, P pain clinic. *p < .05
Baseline model
Following the establishment of the measurement model, structural equation modelling was performed specifying that all structural path coefficients were equal across the three groups. Path coefficients should not be interpreted as correlation coefficients. A path coefficient (e.g., .80) connecting two variables (A and B) means that if A increases by one standard deviation from its mean, B would be expected to increase its own standard deviations from its own mean by .80 while holding all other relevant connections constant. With a path coefficient of −0.16, when A increases by 1 standard deviation from its mean, B would be expected to decrease its own standard deviations from its own mean by 0.16 while holding all other relevant connections constant.
Age, duration of pain, and educational level were used as control variables. No constraints were placed on the path from age, duration of pain and educational level variables to the other latent variables, allowing them to act independently across the groups as control variables. Table 2 shows the path of the covariates across the three groups. The covariance between the latent variables pain acceptance and pain fear avoidance was −14.97 (P < .05).
Table 3 shows the path coefficients for this baseline model. The value of χ 2 indicated that this model had a bad fit between the three groups [χ 2 (184) = 1,627.51, P = .000].
Linear differences between groups
The next step in the analysis was to remove the constraint that the path coefficients between the latent variables were equal between the groups, taking into account one path at a time. Compared to the baseline model in which all the paths in the three groups are constrained to be equal, this analysis tests—similar to analysis of variance—whether there is a difference between groups for a particular path coefficient. Table 3 shows the path coefficients between the latent variables across the groups that were successively estimated; the differences in the chi-square values compared to the baseline model and the significance of these differences are also displayed. A significant difference in chi-square values would represent a significant improvement in model fit indicating that there is a difference between these path coefficients. As can be seen, experiential avoidance and pain intensity both had a positive significant association with pain fear avoidance and were equal across the three groups: the higher the experiential avoidance and pain intensity, the higher the pain fear avoidance. Pain fear avoidance also showed a significant positive association with negative mood of an equal magnitude among the three groups; thus, the higher the pain fear avoidance, the higher the negative mood in the three groups of patients. Anxiety sensitivity was significantly associated with pain fear avoidance alone in the sample of patients with back pain. Resilience was positive and significantly related to pain acceptance for the samples of patients with back pain and IBD, but not for the patients treated at the pain clinic. Pain fear avoidance showed negative significant associations with daily functioning for the samples of patients with back pain and those treated at the pain clinic. Finally, pain acceptance was significantly and positively related to daily functioning alone in the sample of patients with back pain. Regarding negative mood, pain acceptance showed negative and significant relationships in the groups with back pain and IBD.
Discussion
This study compared three samples of patients: patients with chronic back pain treated at primary care centres, patients with heterogeneous pain conditions treated at a pain clinic and patients with pain associated with inflammatory bowel disease (Table 1). With the exception of anxiety, there were significant differences between the groups in all the variables. In general, the patients with IBD showed better adjustment to pain and had lower means in anxiety sensitivity, pain catastrophising, pain anxiety, pain intensity, bodily pain, functional impairment and depression. Several studies have shown that in patients with IBD, pain is associated with diminished quality of life [57–60] and higher pain anxiety and catastrophising [61]. These differences could be due to the fact that patients with IBD had the lowest pain intensity; in addition, in contrast to the two other groups of patients in whom pain is the central symptom, they do not have their attention exclusively centred on pain, since this is just one symptom among many others. Furthermore, IBD has an organically identifiable source of pain, whereas the organic source of many of the pain conditions in the other groups may not have been identified.
On the other hand, the patients treated at the pain clinic showed the worst adjustment to pain and had higher means than the other two groups in pain catastrophising, pain anxiety, pain intensity, bodily pain, functional impairment, and pain hypervigilance and had the lowest mean in pain acceptance. It must be borne in mind that this group, which was treated in a specialised medical service focused on the management of pain, had the longest history of pain; they had undergone more surgical interventions related to pain and consumed the highest amount of pain medications. The patients with back pain had the lowest levels of experiential avoidance and the highest levels of depression. Regarding the remaining variables, this group, which was treated at primary care centres, showed worse adjustment than the IBD group but better adjustment than the group treated at the pain clinic.
There were also differences in the linear associations between the variables included in the hypothetical model (Table 3). In summary, and as predicted, the model had the best fit for the group of patients with back pain treated at primary care centres. These results are in line with two previous studies that investigated the validity of this model in patients with chronic back pain treated in primary care centers [8, 25]. In addition, it should be borne in mind that the fear-avoidance model of pain was proposed to explain adjustment in patients with chronic musculoskeletal pain [1, 2], where the avoidance of activity plays a central role. As shown in Table 3, all the path coefficients in this group were significant: higher experiential avoidance, anxiety sensitivity, and pain intensity were associated with higher pain fear avoidance, which, in turn, was associated with worse daily functioning and higher negative mood. In addition, higher resilience was associated with higher pain acceptance, which was related to better daily functioning and decreased negative mood.
It should be emphasised that three relationships were significant and equal across the three groups: Higher experiential avoidance was associated with higher pain fear avoidance; higher pain intensity was associated with higher pain fear avoidance; and higher pain fear avoidance was associated with higher negative mood. Thus, experiential avoidance, that is, the unwillingness to endure upsetting emotions, thoughts, memories, and other private experiences, which lead to maladaptive efforts to resist, escape, and avoid such experiences [62], was associated with pain fear avoidance in the three groups. This is in line with the results of previous studies suggesting that individuals reporting higher levels of experiential avoidance have lower pain tolerance and higher pain catastrophising [63, 64]. Anxiety sensitivity, that is, the fear of bodily anxiety-related sensations [65], was only related to pain fear avoidance in the group of patients with chronic back pain treated at primary care centres. Again, this is in line with the amended fear-avoidance model [6], which asserts that anxiety sensitivity promotes catastrophic cognitions about pain since both constructs share a common cognitive dimension—namely, a general tendency to catastrophise the meaning of unpleasant physical sensations [66]. Thus, anxiety sensitivity seems to be useful in the early identification of people at risk of becoming disabled by pain only in patients with chronic back pain.
Higher pain intensity was associated with higher pain fear avoidance across the three groups. This is in line with the results of a recent longitudinal study in two samples of workers with back pain [67]. This study found, as previously suggested [68], that fear of pain may be better conceived as a consequence of pain severity rather than an antecedent. Finally, higher pain fear avoidance was associated with higher negative mood across the three groups. Regarding this result, it should be borne in mind that, in this study, the latent variable was specified as a latent construct by pain catastrophising (PCS), hypervigilance (PVAQ) and pain anxiety (PASS). The PASS includes fearful interpretations, avoidance and escape, physiological responses and symptoms of cognitive interference [69]. In this study, this measure was considered more appropriate to assess all the groups than other questionnaires on fear of pain that include items specifically related to fear of movement and beliefs about how work or physical activity affect pain [70, 71]; these are less appropriate for patients who do not suffer musculoskeletal pain for whom movement is a less pressing issue.
Apart from the paths that were significant and equal across the three groups, anxiety sensitivity was not significantly associated with pain fear avoidance in the group of patients with IBD, neither were pain fear avoidance or pain acceptance significantly associated with daily functioning. Thus, none of the variables included in this model explained daily functioning in this group of patients, which, as previously indicated, had less functional impairment than the other two groups. In contrast, both pain fear avoidance and pain acceptance significantly contributed to negative mood.
Finally, the patients treated at the pain clinic were the only group in which resilience was not significantly associated with pain acceptance. Resilience and pain acceptance were found to be highly associated in two studies conducted with patients suffering from chronic back pain [25, 26]. Since the relationship between resilience and pain acceptance has been little studied, future longitudinal research should investigate whether resilient people develop an acceptance response when faced with chronic pain. Pain acceptance was not significantly associated with daily functioning or negative mood in the patients treated at the pain clinic; pain fear avoidance alone significantly contributed to negative mood, as in the other groups, and to daily functioning. It appears that in the patients treated at the pain clinic—the group that showed the poorest adjustment to pain—a significant positive pathway represented by resilience and pain acceptance was not present. These results partially contradict the results of a previous study [10], which was also conducted with patients treated at a pain clinic, since pain acceptance was significantly associated with Functional Impairment. On the other hand, our results are in line with this study since pain acceptance was not associated with depression.
The role of the covariates included in the model deserves special attention (Table 2). First, educational level acted as a protective agent since it was positively associated with resilience and pain acceptance (except for the patients from the pain clinic) and negatively with experiential avoidance, pain intensity and depression. Second, age was associated with lower daily functioning especially in the patients who were treated at the pain clinic; on the other hand, without reaching statistical significance, in all three groups the higher the age the higher the negative mood. These results highlight the importance of taking into account the influence of demographic and clinical variables in future studies.
This study is not without limitations. First, since the data were cross-sectional, it is impossible to determine the exact nature of the associations between the variables of interest or to form conclusions on cause and effect relationships. Prospective, longitudinal studies are needed to determine the precise nature of the relationships explored in this study. Second, self-reporting was the only method followed, and shared method variance may have contributed to the magnitude of some correlations. Future research should replicate the present study and include different assessment methods as well as experimental designs.
Despite these limitations, the current findings extend our understanding of the relationships among resilience, anxiety sensitivity, experiential avoidance, pain fear avoidance, pain acceptance, and adjustment to pain, by integrating concepts from different research traditions within the same framework. It is important to understand the relationships between the large number of variables currently being investigated to determine if some of them can be integrated into a smaller number of dimensions. In addition, this is the first study to simultaneously investigate these associations across three groups of patients with different pain conditions; these patients were treated at different health services, thus contributing to generalisable knowledge of the relationships tested.
Overall, the results of this study showed that pain fear avoidance was associated with different but meaningful outcomes in the three samples. However, the differences between the groups of patients with different pain conditions and attending different health care centres should not be ignored and future research should determine the source of these differences. Furthermore, although there were also differences between groups, pain acceptance seems to represent a course of action that leads to recovery by patients engaging in goals unrelated to pain relief [11], thus improving their well being.
The results of this study have several clinical implications. Since anxiety sensitivity was only associated with pain fear avoidance in patients with chronic back pain, treatments based on exposure to arousal-related body sensations [72] seem to be appropriate only for these patients. On the other hand, since daily functioning was significantly associated with pain fear avoidance in the patients treated at the pain clinic, it may be the case that patients with complex, long-standing pain conditions could receive more benefit from therapeutic approaches mainly oriented to exposure to feared activities and behavioral activation. Finally, since negative mood was strongly associated with pain fear avoidance and pain acceptance in patients with IBD and back pain, they may benefit more from therapeutic approaches centered on exposure to distressing emotions and their acceptance [73].
References
Lethem J, Slade PD, Troup JDG, Bentley G. Outline of a fear-avoidance model of exaggerated pain perceptions. Behav Res Ther. 1983;21:401-408.
Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain. 2000;85:317-332.
Crombez G, Eccleston C, Van Damme S, Vlaeyen JWS, Karoly P. Fear avoidance model of chronic pain. The next generation. Clin J Pain. 2012;28:475–83
Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS. The fear avoidance model of musculoskeletal pain: Current state of scientific evidence. Behav Med. 2007;30:77-94.
Vlaeyen JWS, Linton SJ. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain. 2012;153:1144-1147.
Norton PJ, Asmundson GJG. Amending the fear-avoidance model of chronic pain: What is the role of physiological arousal? Behav Ther. 2003;34:17-30.
Goubert L, Combez G, Van Damme S. The role of neuroticism, pain catastrophizing and pain-related fear in vigilance to pain: A structural equations approach. Pain. 2004;104:234-241.
Esteve R, Ramírez-Maestre C, López-Martínez AE. Experiential avoidance and anxiety sensitivity as dispositional variables and their relationship to the adjustment to chronic pain. Eur J Pain. 2012;16:718-726.
Berman NC, Wheaton MG, McGrath P, Abramowitz JS. Predicting anxiety: The role of experiential avoidance and anxiety sensitivity. J Anx Disord. 2012;24:109-113.
Esteve R, Ramírez-Maestre C, López-Martínez AE. Adjustment to chronic pain: the role of pain acceptance, coping strategies and pain-related cognition. Ann Behav Med. 2007;33:179-188.
McCracken LM, Velleman SC. Psychological flexibility in adults with chronic pain: A study of acceptance, minfulness, and values-based action in primary care. Pain. 2012;148:141-147.
Vowles KE, McCracken LM, Eccleston C. Patient functioning and catastrophizing in chronic pain: The mediation effect of acceptance. Health Psychol. 2008;27:S136-S143.
McCracken LM, Eccleston C. A prospective study of acceptance and patient functioning with chronic pain. Pain. 2005;118:164-169.
Davydov DM, Steward R, Ritchie K, Chaudieu I. Resilience and mental health. Clin Psychol Rev. 2010;30:479-495.
Wagnild G, Young HM. Resilience among older women. J Nur Scholarship. 1990;22:252-255.
Biglan A, Hayes SC, Pistorello J. Acceptance and commitment: Implications for prevention science. Prev Sci. 2008;9:139-152.
Thompson RW, Arnkoff DB, Glass CR. Conceptualizing mindfulness and acceptance as components of psychological resilience to trauma. Trauma Violence Abuse. 2011;12:220-235.
Karoly P, Ruehlman LS. Psychological resilience and its correlates in chronic pain: Finding from a national community sample. Pain. 2006;123:90-97.
Ong AD, Zautra AJ, Reid MC. Psychological resilience predicts decreases in pain catastrophizing through positive emotions. Psychol Aging. 2010;25:516-523.
Smith BW, Zautra AJ. Vulnerability and resilience in women with arthritis: Test of a two-factor model. J Consult Clin Psychol. 2008;76:799-810.
Strand EB, Zautra AJ, Thoresen M, Odegard S, Uhlig T, Finset A. Positive affect as a factor of resilience in the pain-negative affect relationship in patients with rheumatoid arthritis. J Psychosom Res. 2006;60:477-484.
Vinaccia S, Contreras F, Palacio C, Marín A, Tobon S, Moreno-San PE. Disposiciones fortalecedoras: personalidad resistente y autoeficacia en pacientes con diagnóstico de artritis reumatoide. Ter Psicol. 2005;23:15-24.
Wright LJ, Zautra AJ, Going S. Adaptation to early knee osteoarthritis: The role of risk, resilience, and disease severity on pain and physical functioning. Ann Behav Med. 2008;36:70-80.
Zautra AJ, Johnson LM, Davis MC. Positive affect as a source of resilience for women in chronic pain. J Consul Clin Psychol. 2005;73:212-220.
Ramírez-Maestre C, Esteve R, López A. The path to capacity: Resilience and spinal chronic pain. Spine. 2012;4:1-8.
Ríos-Velasco L. Vulnerabilidad y resiliencia: diferencias interculturales en la experiencia de dolor crónico. Doctoral Thesis, University of Málaga, 2011.
Casals M, Samper D. Epidemiology, prevalence and quality of life of non-malignant chronic pain. ITACA study. Rev Soc Esp Dolor. 2004;11:260-269.
Bielefeldt K, Davis B, Binion DG. Pain and inflammatory bowel disease. Inflamm Bowel Dis. 2009;15:778-788.
Drossman DA. ROME II: The Functional Gastrointestinal Disorders. 2nd ed. McLean: Degnan Associates; 2000.
Merskey H, Bogduk N. Classification of Chronic Pain. Seattle: IASP Press; 1994.
Peterson RA, Reiss S. Anxiety Sensitivity Index Mannual. 2nd ed. Worthington: International Diagnostic Systems; 1992.
Sandín B, Chorot P, McNally RJ. Validation of the Spanish version of the Anxiety Sensitivity Index in a clinical sample. Behav Res Ther. 1996;34:283-290.
Hayes SC, Stronsahl K, Wilson KG, et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol Rec. 2004;54:553-578.
Barraca J. Spanish adaptation of the acceptance and action questionnaire. Int J Psych Psychol Ther. 2004;4:505-515.
Wagnild GM, Young HM. Development and psychometric evaluation of the Resilience Scale. J Nurs Meas. 1993;1:165-178.
Heileman MV, Lee K, Kury FS. Psychometric properties of the Spanish version of the Resilience Scale. J Nurs Meas. 2003;11:61-75.
Ruíz-Párraga G. Adaptación española de la Escala de Resiliencia para su uso en pacientes con dolor crónico de origen músculoesqueletal. Degree Thesis, University of Málaga, 2011.
Sullivan MJL, Bishop SC, Pivik J. The Pain Catastrophizing Scale: Development and validation. Psychol Assess. 1995;7:524-532.
Muñoz M, Esteve R. Reports of memory functioning by chronic pain patients. Clin J Pain. 2005;21:287-291.
McCracken LM. Attention to pain in persons with chronic pain: A behavioral approach. Behav Ther. 1997;28:271-284.
Esteve R, Ramírez-Maestre C, López-Martínez AE. Empirical evidence of the validity of the Spanish version of the Pain Vigilance Awareness Questionnaire. Int J Behav Med. 2013;20:59–68.
Roelofs J, McCracken L, Peters ML, Crombez G, van Breukelen G, Vlaeyen JWS. Psychometric evaluation of the Pain Anxiety Symptoms Scale (PASS) in chronic pain patients. J Behav Med. 2004;27:167-183.
Esteve R, Muñoz M. Fear of Pain and Anxiety Sensitivity: Related or redundant constructs? In: Columbus P, ed. Fear of Pain. New York: Nova Publishers; 2010:25-42.
McCracken LM, Vowles KE, Eccleston C. Acceptance of chronic pain: Component analysis and a revised assessment method. Pain. 2004;107:159-166.
Bendayan R, Esteve R, Blanca MJ. Empirical evidence of the validity of the Spanish version of the chronic pain acceptance questionnaire: The differential influence of activity engagement and pain willingness on adjustment to chronic pain. Br J Health Psychol. 2012;17:314-326.
Rodero B, García-Campayo J, Casanueva B, Lopez Y, Serrano-Blanco A, Luciano JV. Validation of the Spanish versión of the Chronic Pain Acceptance Questionnaire (CPAQ) for the assessment of acceptance in fibromyalgia. Health Qual Life Outcomes. 2010;8:37.
Zigmong AS, Snaith RP. The Hospital Anxiety and Depression Scale. Act Psych Scan. 1983;67:361-70.
Quintana JM, Padierna A, Esteban C, Arostegui I, Bilbao A, Ruiz I. Evaluation of the psychometric characteristics of the Spanish Version of the Hospital Anxiety and depression Scale. Act Psych Scan. 2003;107:216-221.
Ramírez-Maestre C, Valdivia Y. Evaluación del funcionamiento diario en pacientes con dolor crónico. Psicología Conductual. 2003;11:283-291.
Jensen MP, Turner P, Romano JM, Fischer LD. Comparative reliability and validity of chronic pain intensity measures. Pain. 1999;83:157-162.
Alonso J, Prieto L, Antó JM. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): Un instrumento para la medida de los resultados clínicos. Med Clin. 1995;104:771-776.
Alonso J, Prieto L, Ferrer G, et al. Testing the measurement properties of the Spanish Version of the SF-36 health survey among male patients with chronic obstructive pulmonary disease. J Clin Epid. 1998;11:1087-1094.
Jöreskog KG, Sörbom D. Lisrel 8: Structural Equation Modeling with the SIMPLIS Command Language. Hillsdale: Scientific Software International; 1993.
Batista JM, Coenders G. Modelos de Ecuaciones Estructurales. Madrid: La Murralla; 2000.
Byrne BM. Structural Equation Modeling with EQS and EQS/Windows: Basic Concepts, Applications and Programming. Thousand Oaks: Sage; 1994.
Byrne BM, Shavelson RJ, Muthén B. Testing for the equivalence of factor covariance and mean structures: The issue of partial measurement invariance. Psychol Bull. 1989;105:456-466.
Bernkleva T, Jahnsenc J, Schulzd T, et al. Course of disease, drug treatment and health-related quality of life in patients with inflammatory bowel disease 5 years after initial diagnosis. Eur J Gastroenterol Hepatol. 2005;17:1037-1045.
Mussell M, Böcker U, Nagel N, Singer MV. Predictors of disease-related concerns and other aspects of health-related quality of life in outpatients with inflammatory bowel disease. Eur J Gastroenterol Hepatol. 2004;16:1273-1280.
Schirbel A, Reichert A, Roll S, et al. Impact of pain on health-related quality of life in patients with inflammatory bowel disease. World J Gastroenterol. 2010;16:3168-3177.
Smith GD, Watson R, Roger D, et al. Impact of a nurse-led counselling service on quality of life in patients with inflammatory bowel disease. J Adv Nur. 2002;38:152-160.
Lix LM, Graff LA, Walker JR, et al. Longitudinal study of quality of life and psychological functioning for active, fluctuating, and inactive disease patterns in inflammatory bowel disease. Inflamm Bowel Dis. 2008;14:1575-1584.
Hayes SC, Wilson KG, Gifford E, Follette VM, Strosahl KD. Emotional avoidance and behavior disorders: A functional dimensional approach to diagnosis and treatment. J Consult Clin Psychol. 1996;64:1152-1168.
Feldner MT, Hekmat H, Zvolensky MJ, Vowles KE, Secrist Z, Leen-Feldner EW. The role of experiential avoidance in acute pain tolerance: A laboratory test. J Behav Ther Exp Psychiat. 2006;37:146-158.
Zettle RD, Hocker TR, Mick KA, et al. Differential strategies in coping with pain as a function of level of experiential avoidance. Psychological Rec. 2005;55:511-524.
Reiss S, McNally RJ. Expectancy model of fear. In: Reiss S, Bootzin RR, eds. Theoretical Issues in Behaviour Therapy. San Diego: Academic; 1985:107-121.
Drahovzal DN, Stewart S, Sullivan MJL. Tendency to catastrophize somatic sensations: Pain catastrophizing and anxiety in predicting headache. Cogn Behav Ther. 2006;35:226-235.
Gheldof ELM, Crombez G, Van den Bussche E, et al. Pain-related fear predicts disability, but not pain severity: A path analytic approach of the fear-avoidance model. Eur J Pain. 2010;14(870):e1-870.e9.
Pincus T, Vogel S, Burton AK, Santos R, Field AP. Fear avoidance and prognosis in back pain: A systematic review and synthesis of current evidence. Arth Rheum. 2006;54:3999-4010.
McCracken LM, Zayfert C, Gross RT. The pain anxiety symptoms scale: Development and validation of a scale to measure fear of pain. Pain. 1992;50:67-73.
Kori SH, Miller RP, Todd DD. Kinesiophobia: a new view of chronic pain behavior. Pain Manage. 1990;3:35–43.
Waddell G, Newton M, Henderson J, Somerville D, Main CJ. A Fear-avoidance Beliefes Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52:157-168.
Watt MC, Stewart SH, Lefaivre MJ, Uman LS. A brief cognitive–behavioral approach to reducing anxiety sensitivity decreases pain-related anxiety. Cogn Behav Ther. 2006;35:248-256.
Wicksell RK, Olsson GL, Hayes SC. Psychological flexibility as a mediator of improvement in acceptance and commitment therapy for patients with chronic pain following whiplash. Eur J Pain. 2011;14:1059-1067.
Disclosures
This study was supported by grants from the Spanish Ministry of Science and Innovation (PSI2008-01803/PSIC) and the Regional Government of Andalusia (HUM-566; P07-SEJ-3067).
Conflict of Interest Statement
The authors have no conflict of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 169 kb)
About this article
Cite this article
Esteve, R., Ramírez-Maestre, C. Pain Fear Avoidance and Pain Acceptance: A Cross-Sectional Study Comparing Their Influence on Adjustment to Chronic Pain Across Three Samples of Patients. ann. behav. med. 46, 169–180 (2013). https://doi.org/10.1007/s12160-013-9499-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-013-9499-1