
Abstract
Background
African American men who have sex with men (MSM) are disproportionately affected by HIV and constitute more than half of all HIV-infected MSM in the USA.
Purpose
Data from the New York City location of a multi-site study were used to evaluate the effectiveness of three HIV testing strategies for detecting previously undiagnosed, 18 to 64-year-old African American MSM. Effectiveness was defined as the identification of seropositive individuals.
Methods
Using a quasi-experimental design (N = 558), we examined HIV-positive test results for men tested via alternative venue testing, the social networks strategy, and partner counseling and referral services, as well as behavioral risk factors for 509 men tested through alternative venue testing and the social networks strategy.
Results
Detection rates of HIV-positives were: alternative venue testing—6.3%, the social networks strategy—19.3%, and partner services—14.3%. The odds for detection of HIV-positive MSM were 3.6 times greater for the social networks strategy and 2.5 times greater for partner services than alternative venue testing. Men tested through alternative venue testing were younger and more likely to be gay-identified than men tested through the social networks strategy. Men who tested through the social networks strategy reported more sexual risk behaviors than men tested through alternative venue testing.
Conclusions
Findings suggest differential effectiveness of testing strategies. Given differences in the individuals accessing testing across strategies, a multi-strategic testing approach may be needed to most fully identify undiagnosed HIV-positive African American MSM.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Centers for Disease Control and Prevention (CDC) estimates that approximately 1.2 million people were living with HIV in the USA in 2008 [1]. In the same year, men who have sex with men (MSM) accounted for more than 50% of the new HIV cases, and in terms of race, African Americans accounted for 74% of new infections [1]. Overall, among African Americans, approximately half of new infections were among MSM. Moreover, in 2008 in New York City, African American MSM accounted for 38% of the new HIV diagnoses; of these new diagnoses, 36% had a concurrent AIDS diagnosis [2].
Despite African Americans in general and African American MSM reporting higher rates of lifetime testing for HIV [3–5], epidemiological patterns demonstrate disparate levels of HIV-positive diagnoses and lower levels of perceived awareness of HIV status prior to testing than their non-black or heterosexual peers [6]. Numerous explanations for not being tested have been proposed and include the belief that one is not at risk for HIV [7], a general fear of testing results [8, 9], fear of stigmatization [10–12], misunderstanding about test result reporting [8, 13], lack of HIV/AIDS-related knowledge [9], distrust in the accuracy of testing [9], mistrust of the medical system [14], and lack of culturally appropriate testing strategies [9, 10, 14]. As a result, a variety of strategies have been developed to identify previously undiagnosed African American MSM.
Partner counseling and referral services (now known as partner services), has been the traditional method for engaging at-risk individuals into testing. Partner services is a public health strategy that involves identifying, locating, and interviewing HIV-infected persons (index patients) to elicit names and contact information of their sex and needle-sharing partners, notifying partners of their exposure to HIV, and providing HIV counseling, testing, and referral services to those partners [15]. Research suggests that partner services is effective for recruiting partners into testing services and identifying previously undiagnosed HIV-positive individuals [16–19].
Since the advent of HIV rapid testing, counseling and testing initiatives within alternative venues (e.g., bars, churches, mobile units) have been the focal point of identifying, engaging, and recruiting high-risk persons who do not normally seek to be tested for HIV in traditional clinical settings [20, 21]. Alternative venue testing allows agencies to test large numbers of people by engaging in street outreach and attending events where high-risk populations may be reached.
A third strategy for accessing high-risk populations utilizes social networks of HIV positive or high-risk negative persons to identify individuals at risk for HIV and link them to counseling and testing services. The literature suggests that the social networks strategy may be an effective method for identifying persons with undiagnosed sexually transmitted infections, including HIV [22–25]. In the social networks strategy, HIV testers and agency staff engage either HIV-positive individuals or those at high risk of seroconversion to become “recruiters.” Through active enlistment and coaching processes, staff build relationships and help recruiters engage people in their social circles (i.e., network associates) into HIV testing.
In the ensuing analyses, we report results from the New York City site of a 3-year, multi-site, CDC-funded study to evaluate the relative effectiveness of alternative venue testing, the social networks strategy, and partner services for reaching and motivating previously undiagnosed 18 to 64-year-old African American MSM to be tested for HIV and linked to medical care. The number and proportion of seropositive test results detected via each of the methods assessed the differential effectiveness of testing methodologies. The objectives of the study were to: (1) compare rates of HIV-positive diagnoses via the three strategies (alternative venue testing, the social networks strategy, partner services); (2) examine demographic and sexual risk behavior differences across testing groups (alternative venue testing, the social networks strategy); and: (3) examine the extent to which sociodemographic factors, sexual behavior patterns, and testing strategy in combination explain the likelihood of differentiating individuals with seropositive and seronegative HIV antibody testing results.
Methods
Study Site and Population
The study was conducted by Harlem United Community AIDS Center in collaboration with New York University. Harlem United is a community-based organization that provides health care, housing, and prevention services for individuals at risk for and living with HIV and AIDS. The community-based organization has offices in Upper Manhattan and the Bronx and provides services for clients from East Harlem to the Bronx. The study protocol was reviewed and approved by human subjects review boards for New York University and CDC.
Study Population
The study was conducted between April 2008 and August 2009. Men were eligible to participate if they: (1) were 18–64 years old, (2) were biologically male, (3) self-reported race as being black (of African descents, excluding immigrants), (4) had the ability to communicate in English, (5) self-reported anal sex with a man in the past year, and (6) provided informed consent.
Measures
Data were collected via a cross-sectional survey composed of both demographic and behavioral questions. The survey was incorporated into the day-to-day documentation used by HIV testing teams at Harlem United to ensure normal testing processes were not disrupted by the research. Core questions focused on HIV-testing strategy (alternative venue testing or the social networks strategy only), sociodemographic information, and sexual and drug-use behavior.
Sociodemographics
The following data were collected: age, gender, race, ethnicity (i.e., Hispanic versus non-Hispanic), sexual orientation, and educational attainment.
HIV Testing History (Self-Reported)
Participants were asked if they had ever been tested for HIV. Those who responded positively were asked the date and results of their last test. Men who reported their last test result to be positive were not eligible for the study.
Sexual Behavior
To assess HIV risk behaviors, participants were asked how many men, women, and/or transgender persons they had vaginal and/or anal sex with in the last 6 months and with how many of these partners they had unprotected receptive anal, insertive anal, and/or vaginal intercourse. A sample question is as follows:
How many men have you had anal sex with in the last 6 months? ….In the last 6 months, with how many of these men did you put your penis in his butt without a condom?… In the last 6 months, how many of these men put their penis in your butt without a condom?
HIV Status
The OraQuick rapid HIV antibody test was used to determine the HIV status of participants. Results were coded as preliminary positive or HIV-negative.
Testing Strategies
Alternative Venue Testing
Alternative venue testing activities were conducted with use of a mobile van. The van was placed in locations throughout New York City known to have large African American MSM populations. New venues were researched on the Internet and ethnographic observations were conducted prior to outreach efforts to ensure venues yielded African American MSM. A typical alternative venue testing recruitment event occurred at least once per week and lasted approximately 4 h per event. Outreach events occurred in three of the five New York City boroughs and included locations near or at: (1) gay neighborhoods, bars, and clubs; (2) community events; and (3) churches. For example, recruitment occurred in neighborhoods such as Chelsea, Greenwich Village at weekly outreach events and special events such as the Gay Pride Parade. Those participants recruited via this testing strategy provided informed consent, were tested for HIV and completed the study instrument on the mobile van. While the alternative venue testing process did not exclude individuals, efforts were made to target African American MSM. In the first 10 months of the study, participation in the alternative venue testing arm of the study was not incentivized, which created difficulties with recruiting men to be in the study due to other local and national programs who were simultaneously conducting HIV testing in New York City and providing incentives. After we received human subjects approval to provide a $30 incentive for the alternative venue testing component of the study, recruitment improved dramatically.
The Social Networks Strategy
The social networks strategy participants were recruited through intra-agency referrals by Harlem United staff, who engaged HIV-positive and high-risk, HIV-negative African American MSM (i.e., men who have sex with men and share needles). African American MSM perceived to be influential by staff or who self-reported having a network of African American MSM were encouraged to participate. Eligible men participating as recruiters provided informed consent and identified men (provided a first name or nickname only) in their social and/or sexual network(s), known as network associates, to engage for HIV testing. Staff assisted recruiters with developing a plan for and coached them on how to engage network associates into HIV testing. Men recruited for testing via this strategy came to the Harlem United offices where they completed all aspects of the protocol. In this approach, recruiters received a $10 incentive for each referral. Originally, those referred did not receive an incentive; however, as with alternative venue testing, the protocol was modified at the same time point in the study such that they received a $20 incentive for testing. We employed 70 recruiters. On average, the recruiters named 2.59 men (SD = 3.84, range = 0, 30), and of these, an average of 1.47 men were tested (SD = 3.40, range = 0, 26).
Recruiters from our study were all men, except one person identified as transgender. Ten percent of the recruiters were Hispanic, and all of the men were African American. Regarding the sexual orientation of the recruiters, 98.6% were either gay or bisexually identified. Sixty-one percent of the recruiters had a high school diploma, GED, or less, while the remaining had an associate degree or higher.
Partner Services
Because Harlem United does not have an on-site partner services program, partner services data were provided by the New York City Department of Health and Mental Hygiene. Harlem United received monthly reports of aggregate-confirmed HIV testing data without identifiers for African American MSM engaged in partner services during the study period (April 2008–August 2009). The report provided the following data: (1) total number of African American/black MSM tested for HIV, and (2) total number of African American/black MSM tested who were HIV-positive (i.e., previously undiagnosed HIV-positive). No other data were provided.
Analytic Plan
For purposes of analyses, responses to the sexual orientation question were dichotomized into two categories—non-gay (bisexual, heterosexual, and other) and gay. Descriptive and bivariate analyses were used to examine the demographic characteristics of participants tested through alternative venue testing and the social networks strategy. The overarching goal of our analysis was to assess the differential effectiveness of recruitment strategies to detect seropositive individuals. Chi-square tests of independence and odd ratios were calculated to determine differences in the detection of newly diagnosed HIV-positive men across all three testing strategies (alternative venue testing, the social networks strategy, partner services). We considered the sexual behaviors of men tested via alternative venue testing and the social networks strategy only because these data were not available for those tested via partner services. Differences in sexual risk behaviors (number of partners and unprotected acts) by testing strategy and differences in risk behaviors by test results were examined using non-parametric Kruskal–Wallis tests, given the large frequency of zeros and non-normal distributions of the variables. Finally, based on the bivariate analyses, we tested a multivariate logistic regression model to determine variables that best explained the likelihood of a preliminary HIV-positive test result. In the model, demographic variables were entered in the first block, sex risk behaviors in the second block, and testing strategy in the third block.
Results
Sample Characteristics
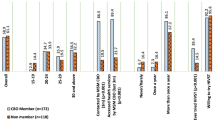
In total, 509 men were recruited and tested via alternative venue testing or the social networks strategy. Table 1 summarizes the sociodemographic characteristics of the participants. All of the men identified as black; 9.6% (n = 49) also reported Hispanic ethnicity. Approximately 98% (n = 497) identified as male. The average age was 26.4 years (MD = 22, range 18–61 years). Sixty-five percent (n = 331) of the men reported having a high school degree/GED education or less, while 35% (n = 178) reported some college, associate’s, bachelor’s degrees or higher. Sixty-six percent of the sample (n = 337) was gay identified.
Bivariate tests were performed to examine relationships between the sociodemographic characteristics and testing strategy. Statistically significant differences were found for educational attainment (p < 0.01) and age (p < 0.001). Men tested via alternative venue testing were younger (25 years old (SD = 8.87) vs. 30 years old (SD = 10.83)) and had lower educational attainment than men tested via the social networks strategy.
HIV Test Results by Testing Strategy
Forty-six (9.0%) of the 509 men tested via alternative venue testing and the social networks strategy demonstrated preliminary HIV-positive antibody test results. Of these 46 men, all identified as black, not mixed race, 95.0% (n = 44) identified as non-Hispanic, and 73.9% (n = 34) stated they were gay. In terms of educational attainment, the majority (63.0%, n = 29) had a high school degree or less.
Statistically significant differences in HIV test result were found across the three testing strategies (χ 2(2) = 18.31, p < 0.001). As shown in Table 2, the positivity rate for men tested via alternative venue testing was 6.3% (n = 25) compared to 19.3% (n = 21) for men tested via the social networks strategy and 14.3% (n = 7) for men tested via partner services. There was no statistically significant difference in HIV test results for men tested via the social networks strategy and partner services (OR = 1.43, 95% CI = 0.56, 3.64). There was, however, a statistically significant difference in test results for men tested via alternative venue testing and those tested via partner services [χ 2(1) = 4.26], p < 0.05; OR = 0.40, 95% CI = 0.16, 0.98). Finally, significance was achieved in comparing alternative venue testing to the social networks strategy [χ 2(1) = 17.65], p < 0.01; OR = 0.28, 95% CI = 0.15, 0.52). Results indicate a 3.6 times greater odds for the social networks strategy to detect HIV-positive men than alternative venues testing, and a 2.5 times greater odds for the partner services to detect HIV-positive MSM than the alternative venue testing.
HIV Risk Behaviors by Testing Strategy (Alternative Venue Testing and Social Networks Strategy)
No significant differences were found by testing strategy for total number of male partners in the last 6 months. However, men tested through the social networks strategy reported more female [χ 2(1) = 10.32, p < 0.001] and transgender [χ 2(1) = 8.74, p < 0.01] partners than men tested through alternative venue testing. These results are shown in Table 3.
Statistically significant differences were found by testing strategy with regard to unprotected insertive and receptive anal intercourse with male, female, and transgender partners. Men tested through the social networks strategy had significantly more unprotected insertive anal intercourse with female partners [χ 2(1) = 7.94, p < 0.01], male partners [χ 2(1) = 9.24, p < 0.01], and transgendered partners [χ 2(1) = 4.44, p < 0.05] than men tested through alternative venue testing. Furthermore, men tested through the social networks strategy reported more unprotected receptive anal intercourse [χ 2(1) = 5.82, p < 0.05] with male partners than men tested through alternative venue testing. With regard to vaginal sex, men tested through alternative venue testing reported less unprotected vaginal intercourse than those tested through the social networks strategy [χ 2(1) = 5.18, p < 0.05].
HIV Risk Behaviors by Test Result (Alternative Venue Testing and Social Networks Strategy)
We then compared the sociodemographic characteristics and risk behaviors of men who tested positive to those who tested negative. Men with preliminary HIV-positive test results were slightly older than those with HIV-negative results [t (52) = 2.29, p < 0.05]. Additionally, men who tested positive reported more male sex partners than men who tested negative [χ 2(1) = 5.44, p < 0.05]. Finally, men who tested positive also reported more episodes of unprotected insertive anal intercourse with men [χ 2(1) = 9.45, p < 0.01] and more episodes of unprotected receptive anal intercourse with men [χ 2(1) = 8.31, p < 0.01] than those who tested negative.
Multivariate Modeling
Based on the bivariate analyses, we tested a multivariate logistic regression model with three block hierarchical entry to determine variables that best explained the likelihood of a preliminary HIV-positive test result. In the model, demographic variables were entered in the first block, sex risk behaviors with male partners in the second block, and testing strategy in the third block. The three-block model provided the best fit (χ 2(5) = 21.20, p = 0.001; Nagelkerke R 2 = 9.2%). Moreover, the addition of the third block (testing strategy) improved fit over the second block (χ 2(1) = 13.08, p < 0.001). Fit indices for variables are shown in Table 4 and suggest that testing strategy is the only significant variable (p < 0.001). The odds ratio for testing methods is 0.29 (95% CI, 0.15, 55) and suggests that alternative venue testing is associated with 72% lower odds of detecting a positive result compared to the social networks strategy.
Discussion
Behavioral studies assessing HIV testing strategy effectiveness for identifying and testing undiagnosed HIV-positive people are few in number and limited in scope. While previous research has examined the effectiveness of alternative venue testing, [20, 26] the social networks strategy, [22–25] and partner services [16, 27] strategies alone, and in comparison to in-house testing, none have effectively compared all the methods nor considered these strategies in relation to participants’ risk profiles. The current investigation is the first to compare positivity rates across three testing strategies (i.e., alternative venue testing, the social networks strategy, and partner services) and analyze sexual risk behaviors by HIV testing strategy for African American MSM. Detection of HIV-positive test results was the metric for comparison of the three methodologies.
In studies that compared effectiveness of in-house and mobile van testing, positivity rates found in the mobile testing component ranged from 0.7% to 5.6% [20, 26, 28]. These rates were less than the alternative venue testing rate in the current study (6.3%). With regard to the social networks strategy, the detected HIV-positivity rate in this study (19%) was higher than rates (ranging from 4.4% to 9.8%) cited in previous work [22–25]. We hypothesize that the higher rates detected in our work may be due to higher prevalence of HIV in New York City, especially among the high-risk group of African American MSM, and potentially due to the use of monetary incentives. The use of incentives may inflate positivity rates due to the inclusion of previously diagnosed positive participants [29]. Because we had no previous records of those tested via alternative venue testing and the social networks strategy, and previous HIV testing history was self-reported by participants, our rates could be potentially inflated due to the inclusion of known seropositive men.
Results from published studies comparing the detection of HIV by testing strategies indicate differential levels of effectiveness. DiFranceisco [20] found that those tested through alternative venue testing were 23% more likely to test positive than those tested at a clinic. However, Shrestha [26] found that those tested in-house had a 2.2% positivity rate, while those tested by alternative venue testing had positivity rates of 0.7% and 1.5%. We found that alternative venue testing (6.3%) detected the largest number of, but a smaller proportion of undiagnosed HIV-positive African American MSM than either the social networks strategy (19.3%) or partner services (14.3%). Additionally, rates of detection were equivalent for the social networks strategy and partner services.
Regarding the sexual risk behaviors, to our knowledge, there are no comparable studies that analyzed number of partners by HIV testing strategy. Our study findings revealed that those tested through alternative venue testing were younger, more likely to identify as gay, had fewer female and transgender sexual partners and fewer unprotected sex partners than those tested through the social networks strategy. While men tested through alternative venue testing and the social networks strategy reported similar numbers of male sex partners, men tested through the social networks strategy reported having more unprotected receptive and insertive anal sex partners in the last 6 months. Taken together, these findings suggest that these two strategies captured different segments of African American MSM. Given the high prevalence of HIV in adolescent and young adult African American MSM in New York City [30] and other urban areas, [31–33] alternative venue testing should be considered a viable strategy to detect HIV in this population.
The findings of our investigation are embedded within the larger framework of an ecosocial model [34], which suggests that individual, community, and societal factors together help us to delineate the causal paths of disease. With regard to our study and based on both the bivariate and multivariate models, we find that individual-level behaviors and the environmental factors of HIV testing recruitment strategy are critical in identifying HIV disease in African American MSM. Moreover, the different demographic characteristics of African American MSM identified in each testing method may be indicative of the social navigation of at-risk African American MSM of varying ages and sexual orientations. HIV prevention efforts must not view African American MSM as a monolith but rather as a diverse group of individuals, where differences in developmental stage and sexual identity are crucial factors in understanding both the risk behaviors of these men and also the environments and venues in which they may socialize. This perspective aligns with an ecosocial understanding of disease and further indicates the need to address both micro (individual level) and macro (structural and social level) determinants of HIV transmission. This understanding informs a multi-level approach to HIV prevention in African American MSM, specifically and MSM more broadly.
Limitations
The study had several limitations. First, the sample included only African American MSM living in New York City. Further research is needed to fully assess the effectiveness of these testing strategies with African American MSM populations that reside outside of urban areas. In addition, the lack of socioeconomic information of study participants limits our ability to comment on the economic means of the study sample, an issue of critical importance given the high level of association between socioeconomic status and HIV prevalence [35]. Regarding results for partner services, the aggregate data from the partner services component of this study revealed a positivity rate of 14.3%, which falls within the range of 12.5–62% reported in previous studies [16, 17, 27]. Although these results are aligned with the literature on partner services, they should be interpreted with caution, given the sample size of this component. Finally, the inability to perform partner services on-site limited our ability to analyze the risk behaviors and other demographic information across the three strategies, thus limiting these analyses to alternative venue testing and the social networks strategy.
Conclusions
The findings of the current investigation suggest the differential effects of three different strategies for engaging previously undiagnosed African American men into HIV testing, an issue of critical importance given the higher prevalence of HIV infection in this segment of the population. In the era of antiretroviral therapy, targeting, testing, and treating high-risk individuals provides an effective means for curtailing the epidemic. Our findings suggest that while more previously undiagnosed, HIV-positive men were identified via the social networks strategy and partner services, a more diverse group of men, including younger and more gay-identified, were recruited and tested via alternative venue testing. Thus, we suggest consideration of all three strategies for improving HIV testing among African American MSM. Finally, operational research utilizing a rigorous experimental study design is needed to identify the most effective HIV testing strategies for high-risk and hard-to-reach populations including African American MSM.
References
Centers for Disease Control and Prevention. HIV surveillance report, 2008; vol. 20. http://www.cdc.gov/hiv/surveillance/resources/reports/2008report. 2010. Accessed November 28, 2010.
New York City Department of Health and Mental Hygiene. HIV/AIDS among men who have sex with men. http://www.nyc.gov/html/doh/html/dires/hivepi.shtml 2010. Accessed November 30, 2010.
Centers for Disease Control & Prevention. Human immunodeficiency virus (HIV) risk, prevention, and testing behaviors United States, national HIV behavioral surveillance system: Men who have sex with men, November 2003–April 2005. Morb Mortal Wkly Rep. 2006;55(SS-6), 1–16.
Centers for Disease Control & Prevention. QuickStats: Percentage of adults aged >18 years who reported ever being tested for human immunodeficiency virus (HIV), by sex and race/ethnicity – national health interview survey, United States, 2006. Morb Mortal Wkly Rep. 2007;56(31),796
Centers for Disease Control & Prevention. Persons tested for HIV-United States, 2006 . Morb Mortal Wkly Rep. 2008;57(31),845-849.
Millett GA, Peterson JL, Wolitski RJ, Stall R. Greater risk for HIV infection of black men who have sex with men: A critical literature review. Am J Public Health. 2006;96(6):1007–1019.
MacKellar DA. Unrecognized HIV infection, risk behaviors, and perceptions of risk among young men who have sex with men: Opportunities for advancing HIV prevention in the third decade of HIV/AIDS. J Acquir Immune Defic Syndr. 2005;38(5):603–614.
Awad GH, Sagrestano LM, Kittleson MJ, Sarvela PD. Development of a measure of barriers to HIV testing among individuals at high risk. AIDS Educ Prev. 2004;16(2):115–125.
Hutchinson AB, Corbie-Smith G, Thomas SB, Mohanan S, del Rio C. Understanding the patient’s perspective on rapid and routine HIV testing in an inner-city urgent care center. AIDS Educ Prev. 2004;16(2):101–114.
Brooks RA, Etzel MA, Hinojos E, Henry CL, Perez M. Preventing HIV among Latino and African American gay and bisexual men in a context of HIV-related stigma, discrimination, and homophobia: Perspectives of providers. AIDS Patient Care ST. 2005;19(11):737–744.
Fortenberry JD, McFarlane M, Bleakley A, et al. Relationships of stigma and shame to gonorrhea and HIV screening. Am J Public Health. 2002;92(3):378–381.
Fullilove MT, Fullilove RE. Stigma as an obstacle to AIDS action. Am Behav Sci. 1999;42(7):1117–1129.
Grusky O, Roberts KJ, Swanson AN, et al. Anonymous versus confidential HIV testing: Client and provider decision making under uncertainty. AIDS Patient Care & STDs. 2005;19(3):157–166.
Wheeler DP. Working with positive men: HIV prevention with black men who have sex with men. AIDS Educ Prev. 2005;17(Supplement A):102–115.
Carballo-Dieguez A, Remien RH, Benson DA, Dolezal C, Decena CU, Blank S. Intention to notify sexual partners about potential HIV exposure among New York city STD clinics’ clients. Sex Transm Dis. 2002;29(8):465–471.
Bocour A, Udeagu CCN, Renaud TC, Hadler JL, Begier EM. Comparing HIV partner notification effectiveness between blacks and Hispanics in New York City. Sex Transm Dis. 2010;37(12):784–788.
Hogben M, McNally T, McPheeters M, Hutchinson AB. The effectiveness of HIV partner counseling and referral services in increasing identification of HIV-positive individuals: A systematic review. Am J Prev Med. 2007;33(2):S89-S100.
Malave MC, Shah D, Sackoff JE, Rubin S, Begier EM. Human immunodeficiency virus partner elicitation and notification in New York City: Public health does it better. Sex Transm Dis. 2008;35(10):869–876.
Passin WF, Kim AS, Hutchinson AB, Crepaz N, Herbst JH, Lyles CM. A systematic review of HIV partner counseling and referral services: Client and provider attitudes, preferences, practices, and experiences. Sex Transm Dis. 2006;33(5):320–328.
DiFranceisco W, Holtgrave DR, Hoxie N, et al. HIV seropositivity rates in outreach-based counseling and testing services: Program evaluation. JAIDS J Acquired Immune Defic Syndromes. 1998;19(3):282–288.
Hutchinson AB, Branson BM, Kim A, Farnham PG. A meta-analysis of the effectiveness of alternative HIV counseling and testing methods to increase knowledge of HIV status. AIDS. 2006;20(12):1597–1604.
Golden MR, Gift TL, Brewer DD, et al. Peer referral for HIV case-finding among men who have sex with men. AIDS. 2006;20(15):1961–1968.
Kimbrough LW, Fisher HE, Jones KT, Johnson W, Thadiparthi S, Dooley S. Accessing social networks with high rates of undiagnosed HIV infection: The social networks demonstration project. Am J Public Health. 2009;99(6):1093–1099.
Rothenberg R, Kimbrough L, Lewis-Hardy R, et al. Social network methods for endemic foci of syphilis: A pilot project. Sex Transm Dis. 2000;27(1):12–18.
Shrestha RK, Sansom SL, Kimbrough L, et al. Cost-effectiveness of using social networks to identify undiagnosed HIV infection among minority populations. Journal of Public Health Management and Practice. 2010;16(5):457–464.
Shrestha RK, Clark HA, Sansom SL, et al. Cost-effectiveness of finding new HIV diagnoses using rapid HIV testing in community-based organizations. Public Health Rep. 2008;123 (Suppl 3):94–100.
Jordan WC, Tolbert L, Smith R. Partner notification and focused intervention as a means of identifying HIV-positive patients. J Natl Med Assoc. 1998;90(9):542–546.
Ellen JM. Comparison of clients of a mobile health van and a traditional STD clinic. J Acquir Immune Defic Syndr. 2003;32(4):388–393.
Renaud TC, Woog V, Ramaswamy CK, et al. Overtating social networks’ ability to diagnose new cases of HIV. Am J Public Health. 2010;100(S1):S5-S6.
New York City Department of Health and Mental Hygiene. New HIV diagnoses rising in New York City among men who have sex with men [DOH Press Release No. 079–07]. 2007. http://www.nyc.gov/html/doh/html/pr2007/pr079-07.shtml. Accessed April 30, 2010.
Centers for Disease Control and Prevention. Fact sheet: HIV/AIDS and young men who have sex with men. http://www.cdc.gov/HealthyYouth/sexualbehaviors/pdf/hiv_factsheet_ymsm.pdf 2009. http://www.cdc.gov/HealthyYouth/sexualbehaviors/pdf/hiv_factsheet_ymsm.pdf27. Accessed March 1, 2010.
Mustanski B, Garofalo R, Herrick A, Donenberg G. Psychosocial health problems increase risk for HIV among urban young men who have sex with men: Preliminary evidence of a syndemic in need of attention. Ann Behav Med. 2007;34(1):37–45.
Valleroy LA, MacKellar DA, Karon JM, et al. HIV prevalence and associated risks in young men who have sex with men. JAMA. 2000;284(2):198–204.
Krieger, N. Epidemiology and the web of causation: Has anyone seen the spider? Soc Sci Med. 1994;39(7):887–893.
American Psychological Association. Fact Sheet: HIV/AIDS & Socioeconomic Status. 2010. http://www.apa.org/pi/ses/resources/publications/factsheet-hiv-aids.aspx. Accessed November 23, 2010.
Acknowledgments
This work was funded by a Cooperative Agreement from the U.S. Centers for Disease Control and Prevention Contract # 1UR6 PS000369. The contents of this article are solely the responsibility of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Conflict of interest
The authors have no conflict of interest to disclose
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Halkitis, P.N., Kupprat, S.A., McCree, D.H. et al. Evaluation of the Relative Effectiveness of Three HIV Testing Strategies Targeting African American Men Who Have Sex with Men (MSM) in New York City. ann. behav. med. 42, 361–369 (2011). https://doi.org/10.1007/s12160-011-9299-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-011-9299-4