
Abstract
To systematically review published data on the role of positron emission tomography (PET) or PET/computed tomography (PET/CT) using either Carbon-11 (11C) or Fluorine-18 (18F) choline tracer in tumors other than prostatic cancer. A comprehensive literature search of studies published in PubMed/MEDLINE and Embase databases through January 2012 and regarding 11C-choline or 18F-choline PET or PET/CT in patients with tumors other than prostatic cancer was carried out. Fifty-two studies comprising 1800 patients were included and discussed. Brain tumors were evaluated in 15 articles, head and neck tumors in 6, thoracic tumors (including lung and mediastinal neoplasms) in 14, liver tumors (including hepatocellular carcinoma) in 5, gynecologic malignancies (including breast tumors) in 5, bladder and upper urinary tract tumors in 5, and musculoskeletal tumors in 7. Radiolabeled choline PET or PET/CT is useful to differentiate high-grade from low-grade gliomas and malignant from benign brain lesions, to early detect brain tumor recurrences and to guide the stereotactic biopsy sampling. The diagnostic accuracy of radiolabeled choline PET is superior compared to Fluorine-18 fluorodeoxyglucose (18F-FDG) PET in this setting. Radiolabeled choline PET or PET/CT seems to be accurate in differential diagnosis between malignant and benign thoracic lesions and in staging lung tumors; nevertheless, a superiority of radiolabeled choline compared to 18F-FDG has not been demonstrated in this setting, except for the detection of brain metastases. Few but significant studies on radiolabeled choline PET and PET/CT in patients with hepatocellular carcinoma (HCC) and musculoskeletal tumors are reported in the literature. The combination of radiolabeled choline and 18F-FDG PET increases the detection rate of HCC. The diagnostic accuracy of radiolabeled choline PET or PET/CT seems to be superior compared to 18F-FDG PET or PET/CT and conventional imaging methods in patients with bone and soft tissue tumors. Limited experience exists about the role of radiolabeled choline PET and PET/CT in patients with head and neck tumors, bladder cancer and gynecologic malignancies including breast cancer.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Positron emission tomography (PET) and PET/computed tomography (PET/CT) using Carbon-11 (11C) or Fluorine-18 (18F) radiolabeled choline are diagnostic tools that are increasingly used in clinical oncology [1–6]. Abnormal choline metabolism is emerging as a metabolic hallmark that is associated with oncogenesis and tumor progression. Following transformation, the modulation of enzymes that control anabolic and catabolic pathways causes increased levels of choline-containing precursors and breakdown products of membrane phospholipids [7]. As tumor cells present a high metabolic rate, choline uptake increases in tumor tissue to keep up with the demands of the synthesis of phospholipids in cellular membranes [8]. The increased levels of choline-containing compounds are associated with proliferation, and recent studies emphasize the complex reciprocal interactions between oncogenic signalling and choline metabolism [9].
Choline can be radiolabeled using 11C or 18F for PET imaging. 11C-choline is biochemically indistinguishable from natural choline, thus, it can be considered as a true tracer of cancer cell metabolism. However, the 11C relatively short half-life (20 min) requires an on-site cyclotron and image acquisition has to be performed early after injection. Practical issues led to the development of fluorinated compounds as 18F-fluoroethyl-choline (FEC) or 18F-fluoromethyl-choline (FCH). FEC and FCH have shown some differences in their biokinetics. In fact, FCH revealed phosphorylation by choline-kinase similarly to choline while the rates of FEC phosphorylation were 30 % lower. The phosphorylation step is thought to be crucial for PET imaging because of metabolic retention of the tracer within the tumor. Both compounds participate further in the synthesis of membrane phospholipids, although the rate of their incorporation into phospholipids may be slower than that of choline. The cancer cells uptake of FEC was one-fifth of that of FCH [10]. However, despite these differences in molecular behavior, no significant differences were observed in the clinical setting. Thus, the PET results can be considered as equal for both 18F-choline tracers.
11C- and 18F-labelled choline is rapidly cleared up after injection; both tracers’ uptake is most pronounced in kidneys and liver. However, only 2 % of injected dose of 11C-choline is excreted in the urine during 1.5 h after injection, compared to the high urinary bladder activity of 18F-choline. Thus, 11C-choline seems to be more advantageous in pelvis evaluation compared to 18F-choline.
Nevertheless, at the moment it is not established which choline derivative is most advantageous in the clinical setting because of the lack of direct comparative studies on individual compounds.
The role of radiolabeled choline PET or PET/CT is mainly recognized in the evaluation of prostate cancer patients, particularly when a biochemical relapse occurs [2, 3, 5, 6]. However, PET and PET/CT with radiolabeled choline have been largely tested also for the non-invasive assessment of a variety of malignancies other than prostate cancer [3, 4].
To date, a systematic review article about the usefulness of radiolabeled choline PET and PET/CT in prostatic cancer already exists [6]. Conversely, a systematic review article about the usefulness of radiolabeled choline PET or PET/CT in tumors other than prostatic cancer is still lacking in the literature. The aim of this study is to update and to analyze the current evidence for the use of radiolabeled choline PET and PET/CT in the management of patients with malignancies other than prostate cancer.
Methods
A comprehensive computer literature search of the PubMed/MEDLINE and Embase databases was carried out to find relevant peer reviewed articles on the use of 11C- or 18F-choline PET or PET/CT in patients with either histologically proven or suspected tumors other than prostatic cancer.
A search algorithm based on a combination of the terms: (a) ‘‘PET’’ or “positron emission tomography” and (b) “choline” was used. No beginning date limit was used and the search was updated until January 20th, 2012. To expand our search, references of the retrieved articles were also screened for additional studies. No language restriction was used.
All studies or subsets in studies investigating the role of 11C- or 18F-choline PET or PET/CT in patients with suspected tumors other than prostatic cancer were eligible for inclusion.
The exclusion criteria were: (a) articles not within the field of interest of this review; (b) review articles, editorials or letters, comments, conference proceedings; and (c) case reports or small case series (less than five patients included).
Two researchers (GT and EG) independently reviewed the titles and the abstracts of the retrieved articles, applying the inclusion and exclusion criteria mentioned above. The same two researchers then independently reviewed the full-text version of the articles to confirm their eligibility for inclusion. Disagreements were resolved in a consensus meeting.
For each included study, information was collected concerning basic study (author names, journal, year of publication, country of origin), patient characteristics (number of patients and type of tumors evaluated), and PET tracers used.
Results
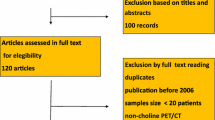
The comprehensive computer literature search from the PubMed/MEDLINE and Embase databases revealed 576 articles. Reviewing titles and abstracts, 524 articles were excluded applying the criteria mentioned above. Fifty-two articles, including 1800 patients referred to PET or PET/CT with radiolabeled choline, were selected and retrieved in full-text version (Fig. 1). No additional study was found screening the references of these articles [11–62]. The characteristics of the included studies are presented in Table 1.

Flow chart of the search for eligible studies on the role of radiolabeled choline PET or PET/CT tumors other than prostate cancer
Brain tumors were evaluated in 15 articles, head and neck tumors in 6, thoracic tumors (including lung and mediastinal neoplasms) in 14, liver neoplasms (including hepatocellular carcinoma) in 5, gynecologic malignancies (including breast tumors) in 5, bladder and upper urinary tract tumors in 5, and musculoskeletal tumors in 7.
Radiolabeled choline PET in brain tumors
The first report on the use of PET and radiolabelled choline was in 1997, by Hara et al. [11]. They evaluated the feasibility of brain tumor imaging using 11C-choline PET in patients with suspected gliomas, demonstrating that this functional imaging method could provide clear images of brain tumors. The uptake in normal brain tissue is, in fact, very low. Conversely, the uptake in venous sinuses, lateral ventricles and pituitary is high. A high uptake of 11C-choline PET was reported in malignant brain tumor in all cases (n = 24) and in pituitary adenoma in two cases; particularly relevant was the very low uptake of surrounded background. 11C-choline uptake was independent of the blood flow rate in the tumor, as assessed using 15O-water PET [11].
Ohtani et al. [12] compared 11C-choline PET, contrast-enhanced magnetic resonance (MR) imaging and Fluorine-18 fluorodeoxyglucose (18F-FDG) PET findings in 22 patients with suspected brain tumors. 11C-choline PET could differentiate between low-grade gliomas and high-grade gliomas, characterized by a higher choline uptake than low-grade gliomas, but could not differentiate between low-grade gliomas and non-neoplastic lesions. The authors suggested that a combination of 11C-choline PET and MR imaging may be useful to identify high-grade gliomas [12].
Conversely, Utriainen et al. [13] found that 11C-choline uptake did not differ between low- and high-grade gliomas. These authors, comparing MR spectroscopy and 11C-choline PET in 12 patients with suspected brain tumors, demonstrated that both the imaging methods could be helpful in differential diagnosis between lymphomas, non-neoplastic lesions and gliomas, being histopathologic methods superior in the estimation of tumor grade [13].
In 2003, Hara et al. [14] tested both 18F- and 11C-choline PET to visualize gliomas prior to stereotactic biopsy procedures. Stereotactic biopsy sampling was performed in 12 patients, in those areas presenting an increased radiolabeled choline uptake on PET images. The radiolabeled choline uptake in high-grade gliomas resulted higher than that of low-grade tumors. Only in one case of oligodendroglioma, the tumor showed no uptake of 18F- and 11C-choline. With this exception, radiolabeled choline PET could be useful to guide the stereotactic biopsy sampling [14].
In two studies, Tian et al. [15, 16] compared the usefulness of 11C-choline and 18F-FDG PET for the differentiating between benign and malignant brain lesions. 11C-choline uptake in malignant lesions was significantly higher than that in benign lesions and it was correlated with 18F-FDG uptake. Accuracy in differentiating between benign and malignant brain lesions was 79 % for 11C-choline PET and 58 % for 18F-FDG PET. The authors suggested that 11C-choline PET is a useful method for differentiating between malignant and benign brain lesions. However, a high uptake of 11C-choline was also reported in some benign tumors and tumor-like lesions [15, 16].
Evaluating with 18F-choline PET 30 solitary brain lesions enhancing at MR, Kwee et al. [17] demonstrated that high-grade gliomas, metastases, and benign lesions can be distinguished on the basis of 18F-choline uptake. The tracer uptake was, in fact, significantly higher in metastases compared to gliomas and benign lesions, and in gliomas compared to benign lesions. In particular, increased peritumoral 18F-choline uptake is a distinguishing characteristic of high-grade gliomas [17].
In 2008, Huang et al. [18], evaluating 94 patients with suspected brain tumors by comparatively using 11C-choline PET and 18F-FDG PET, reported an accuracy in the diagnosis of brain tumors of 84 and 71 % for 11C-choline PET and 18F-FDG PET, respectively. These authors also reported five false positive cases (one abscess, one tuberculosis, one benign gliocyte proliferation, one inflammatory granuloma and one demyelination) and four false negative cases (two metastases from lung cancer, one lymphoma, one grade II glioma) using 11C-choline PET. The authors underlined that 11C-choline PET seems to be superior compared to 18F-FDG PET for the detection of brain tumors. Nevertheless, false positive and false negative results should be kept in mind when interpreting 11C-choline PET findings [18].
In the same year, Kato et al. [19] compared 11C-choline, 11C-methionine (a tracer which evaluate amino acid metabolism) and 18F-FDG PET in 95 patients with gliomas and correlated PET findings with histopathological features. Significant differences were evident between the different grade of gliomas and PET tracers uptake. Tumor type influenced only 11C-methionine uptake. In all cases, significant correlations among 11C-choline, 11C-methionine and 18F-FDG uptake were shown. The authors reported that, in terms of visual evaluation of tumor localization, 11C-methionine PET is superior to 11C-choline and 18F-FDG PET in gliomas, due to its straightforward detection of “hot lesions” [19].
Increased 11C-choline uptake was also reported in benign brain tumors, as reported by Giovacchini et al. [20] in a study comparing 11C-choline and 18F-FDG PET uptake in 7 patients with meningiomas. All cases of meningiomas showed an increased 11C-choline uptake (the uptake was higher in patients with grade II than in grade I meningiomas), whereas 18F-FDG uptake was increased only in one of the 7 meningiomas evaluated. The authors concluded that 11C-choline PET may detect meningiomas better than 18F-FDG PET [20].
Recently Tatenaka et al. [21], comparing 11C-choline, 11C-methionine and 18F-FDG PET in differential diagnosis between gliomas and monofocal acute inflammatory demyelination (MAID), found that 11C-methionine was superior compared to 11C-choline and 18F-FDG in discriminating between MAID and gliomas [21].
Conversely, in the direct comparison to 11C-methionine PET, 11C-choline seems to be promising for the imaging of brain metastases (in particular in patients previously treated with radiation therapy), as demonstrated in a preliminary study of Rottenburger et al. [22], presenting a higher lesion to normal brain uptake ratio in tumor tissue compared with 11C-methionine, without evidence for a lower specificity of 11C-choline PET than that of 11C-methionine PET [22].
Recently Tan et al. [23] compared MR imaging, 18F-FDG and 11C-choline PET/CT in differentiating brain tumor recurrence from necrosis after radiotherapy in 55 patients. The authors reported sensitivity in tumor recurrence diagnosis for MR imaging, 18F-FDG and 11C-choline PET/CT of 87, 77, and 92 %, respectively. The specificity of MR imaging, 18F-FDG and 11C-choline PET/CT was 81, 62.5, and 87.5 %, respectively. These results suggest that 11C-choline PET/CT is superior in distinguishing recurrent brain tumor from radionecrosis compared with both 18F-FDG PET/CT and MR imaging [23].
In a preliminary report, Roelcke et al. [24] showed that 18F-fluoroethyltyrosine (18F-FET, a tracer which evaluate amino acid metabolism) and 18F-choline uptake is similar in low-grade gliomas. These authors stated that, for clinical purposes, 18F-choline PET is not superior to PET using radiolabeled amino acid, such as 18F-FET [24].
Lastly, Li et al. [25] explored the usefulness of 11C-choline PET in optimization of target volume delineation and treatment regimens in postoperative radiotherapy for brain gliomas [25]. These authors found that the tumor target volume was well contrasted using 11C-choline PET (11C-choline uptake correlated with the grade of gliomas), and the boundaries between lesions and surrounding normal brain tissues could be better defined compared with MR imaging and 18F-FDG PET. Furthermore, as differences between 11C-choline PET and MR imaging could be found in the definition of residual tumor in patients with brain gliomas, the authors underlined that for an accurate definition of tumor target volume 11C-choline PET is to be used in combination with MR imaging [25].
Radiolabeled choline PET in head and neck tumors
In 2004, Tian et al. [15] demonstrated that 11C-choline PET is feasible for differentiating between malignant and benign lesions in the head and neck. Furthermore, head and neck lesions showed higher contrast with 11C-choline PET than with 18F-FDG PET [15].
Ninomiya et al. [26] also evaluated the usefulness of 11C-choline PET in the diagnosis of head and neck tumors. These authors studied 22 patients with suspected malignant tumors in the nasal cavity and paranasal sinuses, using both 11C-choline and 18F-FDG PET. These functional imaging methods could depict squamous cell carcinoma showing an increased tracer uptake, significantly higher than that of normal tissue and benign lesions. 11C-choline uptake in squamous cell carcinoma was lower than 18F-FDG uptake but more homogeneous [26].
Khan et al. [27] confirmed the clinical value of 11C-choline PET in differentiating between malignant and benign head and neck lesions. These authors, evaluating 45 patients with suspected head and neck lesions, reported an accuracy of 11C-choline and 18F-FDG PET in this setting of 84 and 80 %, respectively. Malignant tumors presented a significantly higher tracer uptake than that of benign lesions both with 11C-choline and with 18F-FDG PET. 11C-choline PET seemed to detect malignant head and neck tumors as effectively as 18F-FDG PET, with the advantages of a shorter examination period and a low uptake in the muscles. However, both methods have some limitations in the evaluation of salivary gland lesions [27].
Ito et al. [28] assessed the usefulness of 11C-choline and 18F-FDG PET/CT for detecting recurrences of advanced head and neck squamous cell carcinoma after combined chemotherapy and radiotherapy in 53 patients. 11C-choline PET/CT was not superior to 18F-FDG PET/CT for the detection of recurrent head and neck cancer (sensitivity and specificity were 83 and 80 % for 11C-choline PET/CT and 89 and 91 % for 18F-FDG PET/CT, respectively) [28].
The same authors reported that the abilities of 11C-choline and 18F-FDG PET/CT for detecting recurrences of non-squamous cell head and neck malignancies after chemotherapy and radiotherapy were comparable [29].
11C-choline PET/CT has a superior potential for imaging skull base and intracranial lesions compared to 18F-FDG PET/CT because the normal brain is not choline avid [30]. For this reason, 11C-choline PET/CT improves tumor staging in patients with nasopharyngeal carcinoma, as recently demonstrated by Wu et al. [30].
Radiolabeled choline PET in thoracic neoplasms
Esophageal carcinoma
In 1999, Kobori et al. [31] demonstrated that the combination of 11C-choline and 18F-FDG PET was very effective in preoperatively lymph nodal staging in patients with esophageal carcinoma. 11C-choline PET was more effective than 18F-FDG PET and CT in detecting very small metastases localized in the mediastinum. It was ineffective, however, in detecting metastases localized in the upper abdomen, because of the physiological uptake of 11C-choline in the liver [31].
Also Jager et al. [32] compared 11C-choline and 18F-FDG PET for staging esophageal cancer in 18 patients. These authors demonstrated that 11C-choline PET is able to visualize esophageal carcinoma and its metastases, but appears to be more limited with respect to 18F-FDG PET in terms of diagnostic accuracy. Presumably, this is due to a lower tumoral uptake of 11C-choline compared to 18F-FDG and to a considerable non-specific uptake of 11C-choline in liver, stomach wall, pancreas and small intestine [32].
Mediastinal lesions
In 2006, Liu et al. [33] assessed the role of 11C-choline PET/CT in the evaluation of mediastinal masses in 32 patients. 11C-choline PET/CT proved to be a valuable diagnostic tool for differential diagnosis of benign versus malignant lesions with an accuracy of 75 %. 11C-choline uptake in malignant lesions appeared to be higher than that of benign lesions. Nevertheless, 11C-choline PET/CT may provide misdiagnosis in a substantial proportion of patients with mediastinal masses compared to videomediastinoscopy [33].
The same group reported that dual time point 11C-choline PET/CT may improve the accuracy. In particular, they used an imaging protocol including a first PET scanning 5–10 min after the radiopharmaceutical injection and a second PET scanning after 25–30 min. However, videomediastinoscopy remains the gold standard in differentiation of malignant and benign mediastinal lesions [34].
Lung cancer
In 2000, Hara et al. [35] compared the diagnostic accuracy of 11C-choline and 18F-FDG PET in detecting mediastinal lymph node metastases originating from non-small cell lung cancer (NSCLC). The authors found that 11C-choline PET was very effective in detecting lymph node metastases in the mediastinum originating from NSCLC, with a detection rate of 100 % [35].
Pieterman et al. [36] reported that 11C-choline PET can be used for staging thoracic cancers. In the 17 patients evaluated, primary tumors were visualized both with 11C-choline and 18F-FDG PET, although the accuracy in the detection of lymph node metastases with 11C-choline PET was inferior compared to that of 18F-FDG PET. Nevertheless, 11C-choline PET provided a better accuracy in the detection of brain metastases compared to that of 18F-FDG PET [36].
Khan et al. [37] also compared the diagnostic value of 11C-choline and 18F-FDG PET in the detection of primary lung cancer and mediastinal lymph node metastases. The authors demonstrated that both techniques present a clinical value for the non-invasive detection of primary lung cancer equal or larger than 2 cm in size. However, 18F-FDG PET is superior to 11C-choline PET in the detection of lung cancer smaller than 2 cm in diameter and of mediastinal lymph node metastases [37].
In 2003, Hara et al. [38] evaluated the combined role of 11C-choline and 18F-FDG PET to differentiate between lung cancer and mycobacteriosis. In lung cancer patients, the uptake of both 18F-FDG and 11C-choline was high. In patients with tuberculosis, the uptake of 18F-FDG was high, but the uptake of 11C-choline was low. In patients with atypical mycobacterial infection, the uptake of both 18F-FDG and 11C-choline was low [38].
In 2004, Tian et al. [15, 16] showed that 11C-choline PET is similar to 18F-FDG PET in differentiation between malignant and benign pulmonary lesions. In fact, both 11C-choline and 18F-FDG uptake in malignant tumors was significantly higher than that of benign lesions [15, 16].
In 2006, Wang et al. [39] performed 11C-choline PET in 39 patients with suspected lung cancer and reported that sensitivity, specificity and diagnostic accuracy of 11C-choline PET in the diagnosis of malignant lung nodules was 89, 60 and 77 %, respectively. Moreover, the authors found that 11C-choline PET can effectively evaluate lymph nodal staging and accurately depict brain metastases in patients with lung cancer [39].
In 2010, the same authors [40] demonstrated that 11C-choline PET is a valuable tool in the diagnosis of lung cancer but also lead to false positive and false negative results. The authors found that the sensitivity, specificity and accuracy of 11C-choline PET were 84, 58 and 75 %, respectively [40].
Recently, Balogova et al. [41] compared 18F-choline and 18F-FDG PET/CT in the diagnosis of well-differentiated lung adenocarcinoma and in the evaluation of patients with ground-glass opacities, demonstrating that both imaging methods had similar diagnostic performance [41].
Lastly, Peng et al. [42] compared the diagnostic abilities of 11C-choline PET/CT and contrast-enhanced CT in 108 patients with pulmonary lesions or loco-regional lymph nodal metastases from lung cancer. The accuracy, sensitivity, and specificity of 11C-choline PET/CT for diagnosing lung cancer were 82, 85, and 73 %, respectively, compared with 73, 77, and 61.5 %, respectively, of CT. The accuracy, sensitivity and specificity of 11C-choline PET/CT for lymph nodal metastatic disease were 84, 82 and 84 %, respectively, compared with 69, 64, and 71 %, respectively, of CT. Differences between 11C-choline PET/CT and CT were statistically different for lymph nodal detection but not for pulmonary lesions characterization [42].
Radiolabeled choline PET in liver neoplasms
In 2006, Talbot el al. [43] compared 18F-choline with 18F-FDG PET/CT in patients with hepatocellular carcinoma (HCC). 18F-choline provided a high detection rate for HCC (12/12 patients evaluated were correctly detected using 18F-choline PET/CT), making it potentially useful in the initial evaluation of HCC or in the detection of recurrent disease compared to 18F-FDG PET/CT (of the 9 patients who underwent both methods, all 9 were positive with 18F-choline whereas only 5 were positive with 18F-FDG) [43].
Yamamoto et al. [44] demonstrated that 11C-choline is a promising PET tracer to complement 18F-FDG in detection of HCC lesions. These authors found that 11C-choline PET showed a slightly higher detection rate than that of 18F-FDG PET for the detection of HCC (63 vs. 50 %, respectively). 11C-choline PET presented a better detection rate than that of 18F-FDG PET for moderately differentiated HCC lesions, but not for poorly differentiated HCC lesions (75 vs. 25 %, respectively). 18F-FDG PET produced the opposite results (42 vs. 75 %, respectively) [44].
In 2010, Talbot et al. [45] suggested that performing PET/CT using both 18F-choline and 18F-FDG represents the best option for detection and surveillance of HCC. Per patient- and per lesion-based sensitivity of 18F-choline PET/CT (88 and 84 %, respectively) was superior to that of 18F-FDG PET/CT (68 and 67 %, respectively), and 18F-choline PET/CT is superior compared to 18F-FDG PET/CT in patients with well-differentiated HCC. In contrast, 18F-FDG PET/CT appeared more sensitive in detecting other liver malignancies and more specific than 18F-choline PET/CT (for example 18F-FDG PET/CT was negative in patients with focal nodular hyperplasia in contrast to 18F-choline PET/CT) [45].
In this regard, a recent pilot study of Esschert et al. [46] showed that 18F-choline PET/CT can differentiate hepatocellular adenoma (HCA) from focal nodular hyperplasia (FNH) because the radiopharmaceutical uptake was superior in HCA compared to FNH [46].
Wu et al. [47] recently reported that the combination of 18F-FDG in conjunction with 11C-choline PET/CT could increase the detection rate of HCC, from 63 % using 18F-FDG PET/CT alone to 89 % using both PET tracers. Furthermore, compared with 18F-FDG PET/CT, 11C-choline PET/CT showed an improved detection of well-differentiated HCC (66.7 vs. 35.7 %). For the detection of moderately differentiated HCC, the sensitivity of 11C-choline and 18F-FDG PET/CT was similar [47].
Radiolabeled choline PET in tumors of the urinary tract
In 2002, Jong et al. [48] demonstrated that 11C-choline uptake in bladder cancer was avid, yielding the tumor visualization in the virtual absence of urinary radioactivity. Nevertheless, no increased uptake of 11C-choline could be detected either in pre-malignant lesions or in small non-invasive tumors [48].
Four years later, Picchio et al. [49] compared the diagnostic accuracy of contrast-enhanced CT and 11C-choline PET for the staging of bladder cancer in 27 patients. The resulted data suggested that 11C-choline PET is comparable to CT for detecting residual bladder cancer after transurethral resection, but appears to be superior to CT for the evaluation of potential additional lymph nodal metastases [49].
Gofrit et al. [50] evaluated the contribution of 11C-choline PET/CT in the staging of 18 patients with advanced transitional cell carcinoma. 11C-choline PET/CT was highly sensitive for primary and metastatic transitional cell carcinoma. Moreover, carcinoma in situ, lymph node metastases and early bone metastases could be detected [50].
Recently Maurer et al. [51] also assessed the diagnostic accuracy of 11C-choline PET/CT compared with CT in lymph nodal staging of patients with bladder cancer. On patient-based analysis, sensitivity, specificity, and accuracy for 11C-choline PET/CT were 58, 66, and 64 %, respectively; for CT, the results were 75, 56, and 61 %, respectively. The authors concluded that preoperative lymph node staging with 11C-choline PET/CT was not able to improve diagnostic efficacy compared with conventional CT alone [51].
Lastly, Golan et al. [52] compared 11C-choline with 18F-FDG PET/CT for staging bladder cancer in 20 patients. 11C-choline PET/CT did not show any significant diagnostic advantage compared to 18F-FDG PET/CT in the detection of metastatic bladder cancer [52].
Radiolabeled choline PET in gynecologic malignancies including breast cancer
In 2003, Torizuka et al. [53] demonstrated the feasibility of 11C-choline PET for imaging of gynecologic tumors in 21 patients. The main advantage of this tracer compared to 18F-FDG was the lower urinary radioactivity. However, intestinal background activity may interfere with the interpretation of 11C-choline PET [53].
In 2009, Sofue et al. [54] evaluated the role of 11C-choline PET/CT in the staging of uterine carcinoma in 22 patients. Based on PET/CT findings, the reviewers correctly classified T stage in 8 patients (47 %), N stage in 21 patients (96 %), M stage in 20 patients (91 %). The authors found that the combination of 11C-choline PET/CT and MR imaging could increase the accuracy of staging in patients with uterine carcinoma [54].
In 2009, Contractor et al. [55] examined the ability of 11C-choline PET to detect clinically aggressive phenotype in patients with estrogen receptor (ER)-positive breast cancer. Breast tumors were well visualized in 30 of 32 patients and 11C-choline uptake correlated with tumor grade [55].
The same authors demonstrated that 11C-choline uptake can be reproducibly assessed in patients with breast cancer [56] and that choline metabolism and proliferation (assessed by 18F-fluorothymidine PET) were correlated in ER-positive breast cancer [57].
Radiolabeled choline PET in musculoskeletal tumors
In 2003, Zhang et al. [58] compared 11C-choline PET with 18F-FDG PET for the differentiation between benign and malignant bone and soft tissue tumors in 43 patients. The study showed that 11C-choline PET was superior to 18F-FDG PET in differentiation between malignant and benign lesion in bone and soft tissue tumors. In fact, 11C-choline uptake in malignant lesions was significantly higher than that in benign lesions and correlated with 18F-FDG uptake. The sensitivity, specificity and accuracy of 11C-choline PET were 100, 64 and 76 %, respectively. The sensitivity, specificity and accuracy of 18F-FDG PET were 86, 42 and 56 %, respectively [58]. These findings were further confirmed by other papers of the same group [15, 16, 59].
Yanagawa et al. [60] also compared 11C-choline PET with 18F-FDG PET in the evaluation of musculoskeletal tumors in 33 patients. The authors found a significant correlation between 11C-choline and 18F-FDG uptake for all lesions. 11C-choline and 18F-FDG uptake in malignant lesions was significantly higher than that of benign lesions. The sensitivity, specificity and accuracy of 11C-choline PET were 92, 90 and 91 %, respectively. The sensitivity, specificity and accuracy of 18F-FDG PET were 85, 80 and 82 %, respectively. The authors demonstrated that 11C-choline PET is not inferior to 18F-FDG PET for differentiating malignant from benign musculoskeletal tumors. The advantages of 11C-choline PET were the shorter examination time and the negligible retention in the bladder. Therefore, this modality may thus be useful for preoperative planning for musculoskeletal tumors, especially for lesions in the region of hip joints [60].
In 2006, Tateishi et al. [61] compared the diagnostic accuracy of 11C-choline PET/CT and conventional imaging for the staging of bone and soft tissue sarcomas in 16 patients. The overall TNM staging and N staging accuracy of 11C-choline PET/CT was significantly higher than that of conventional imaging. The authors concluded that 11C-choline PET/CT is more accurate than conventional imaging regarding clinical staging of patients with bone and soft tissue sarcomas [61].
As multiple myeloma (MM) bone lesions may present low 18F-FDG uptake, Nanni et al. [62] assessed the possible added value of 11C-choline PET/CT in 10 patients with MM. Overall, 11C-choline PET/CT scans detected 37 bone lesions and 18F-FDG PET/CT scans detected 22 bone lesions but the difference was not significant. 11C-choline PET/CT appeared to be more sensitive than 18F-FDG PET/CT for the detection of MM bone lesions [62].
Conclusion and general remarks
Radiolabeled choline PET or PET/CT has been widely used to evaluate brain tumors, in particular gliomas. These techniques seem to be useful to differentiate high-grade from low-grade gliomas, and malignant from benign brain lesions, to early detect brain tumor recurrences and to guide the stereotactic biopsy sampling. The diagnostic accuracy of radiolabeled choline PET is superior compared to 18F-FDG PET. However, false positive and false negative results should be kept in mind when interpreting radiolabeled choline PET findings. Further studies comparing radiolabeled choline to amino acid, PET tracers in brain tumors are needed.
Limited experience exists about the role of radiolabeled choline PET and PET/CT in patients with head and neck tumors. These techniques seem to differentiate between malignant and benign tumors but a superiority in terms of diagnostic accuracy compared to 18F-FDG PET has not been clearly demonstrated. Promising results of radiolabeled choline PET in the detection of skull base and intracranial lesions have been reported.
As for thoracic tumors, the diagnostic accuracy of radiolabeled choline PET is not proven to be superior to that of 18F-FDG PET in staging esophageal cancer. Radiolabeled choline PET is able to differentiate between malignant and benign mediastinal lesions but its diagnostic accuracy is inferior compared to that of videomediastinoscopy. Several studies evaluated patients with lung cancer using radiolabeled choline PET or PET/CT. These methods seem to be accurate in differential diagnosis between malignant and benign lung lesions and in staging lung tumors; nevertheless, a superiority of radiolabeled choline compared to 18F-FDG has not been demonstrated in this setting, except for the detection of brain metastases.
Few but significant studies on radiolabeled choline PET and PET/CT in patients with HCC are reported in the literature. The combination of radiolabeled choline and 18F-FDG PET increases the detection rate of HCC. Radiolabeled choline PET is more sensitive for well-differentiated HCC compared to 18F-FDG PET. Conversely, 18F-FDG PET is more sensitive in poorly differentiated HCC compared to radiolabeled choline PET.
Limited studies evaluated the usefulness of radiolabeled choline PET or PET/CT in bladder cancer staging; the diagnostic accuracy of these methods does not seem to be superior compared to 18F-FDG PET/CT; furthermore, the superiority of radiolabeled choline PET compared to CT is not yet clearly evident in the literature.
Some authors evaluated the feasibility of radiolabeled choline PET in gynecologic tumors and breast cancer, but further studies are needed.
Few but significant studies reported a high accuracy of radiolabeled choline PET or PET/CT in the detection of bone and soft tissue tumors. These methods seem to be superior compared to 18F-FDG PET or PET/CT and conventional imaging method, but further studies are warranted. The encouraging preliminary data obtained with radiolabeled choline PET in patients with MM should be confirmed in a larger series of patients.
References
Chen K, Chen X. Positron emission tomography imaging of cancer biology: current status and future prospects. Semin Oncol. 2011;38:70–86.
Chiti A, Picchio M. The rising PET: the increasing use of choline PET/CT in prostate cancer. Eur J Nucl Med Mol Imagin. 2011;38:53–4.
Mertens K, Slaets D, Lambert B, Acou M, De Vos F, Goethals I. PET with (18)F-labelled choline-based tracers for tumour imaging: a review of the literature. Eur J Nucl Med Mol Imaging. 2010;37:2188–93.
Nanni C, Rubello D, Fanti S. Could choline PET play a role in malignancies other than prostate cancer? Eur J Nucl Med Mol Imaging. 2008;35:216–8.
Picchio M, Giovannini E, Messa C. The role of PET/computed tomography scan in the management of prostate cancer. Curr Opin Urol. 2011;21:230–6.
Bauman G, Belhocine T, Kovacs M, Ward A, Beheshti M, Rachinsky I. (18)F-fluorocholine for prostate cancer imaging: a systematic review of the literature. Prostate Cancer Prostatic Dis. 2012;15:45–55.
Zeisel SH, Blusztajn JK. Choline and human nutrition. Annu Rev Nutr. 1994;14:269–96.
Podo F. Tumour phospholipid metabolism. NMR Biomed. 1999;12:413–39.
Glunde K, Bhujwalla ZM, Ronen SM. Choline metabolism in malignant transformation. Nat Rev Cancer. 2011;11:835–48.
DeGrado TR, Baldwin SW, Wang S, Orr MD, Liao RP, Friedman HS, et al. Synthesis and evaluation of (18)F-labeled choline analogs as oncologic PET tracers. J Nucl Med. 2001;42(12):1805–14.
Hara T, Kosaka N, Shinoura N, Kondo T. PET imaging of brain tumor with [methyl-11C]choline. J Nucl Med. 1997;38:842–7.
Ohtani T, Kurihara H, Ishiuchi S, Saito N, Oriuchi N, Inoue T, et al. Brain tumour imaging with carbon-11 choline: comparison with FDG PET and gadolinium-enhanced MR imaging. Eur J Nucl Med. 2001;28:1664–70.
Utriainen M, Komu M, Vuorinen V, Lehikoinen P, Sonninen P, Kurki T, et al. Evaluation of brain tumor metabolism with [11C]choline PET and 1H-MRS. J Neurooncol. 2003;62:329–38.
Hara T, Kondo T, Hara T, Kosaka N. Use of 18F-choline and 11C-choline as contrast agents in positron emission tomography imaging-guided stereotactic biopsy sampling of gliomas. J Neurosurg. 2003;99:474–9.
Tian M, Zhang H, Oriuchi N, Higuchi T, Endo K. Comparison of 11C-choline PET and FDG PET for the differential diagnosis of malignant tumors. Eur J Nucl Med Mol Imaging. 2004;31:1064–72.
Tian M, Zhang H, Higuchi T, Oriuchi N, Endo K. Oncological diagnosis using (11)C-choline-positron emission tomography in comparison with 2-deoxy-2-[(18)F] fluoro-d-glucose-positron emission tomography. Mol Imaging Biol. 2004;6:172–9.
Kwee SA, Ko JP, Jiang CS, Watters MR, Coel MN. Solitary brain lesions enhancing at MR imaging: evaluation with fluorine 18 fluorocholine PET. Radiology. 2007;244:557–65.
Huang Z, Zuo C, Guan Y, Zhang Z, Liu P, Xue F, et al. Misdiagnoses of 11C-choline combined with 18F-FDG PET imaging in brain tumours. Nucl Med Commun. 2008;29:354–8.
Kato T, Shinoda J, Nakayama N, Miwa K, Okumura A, Yano H, et al. Metabolic assessment of gliomas using 11C-methionine, [18F] fluorodeoxyglucose, and 11C-choline positron-emission tomography. AJNR Am J Neuroradiol. 2008;29:1176–82.
Giovacchini G, Fallanca F, Landoni C, Gianolli L, Picozzi P, Attuati L, et al. C-11 choline versus F-18 fluorodeoxyglucose for imaging meningiomas: an initial experience. Clin Nucl Med. 2009;34:7–10.
Takenaka S, Shinoda J, Asano Y, Aki T, Miwa K, Ito T, et al. Metabolic assessment of monofocal acute inflammatory demyelination using MR spectroscopy and (11)C-methionine-, (11)C-choline-, and (18)F-fluorodeoxyglucose-PET. B. Brain Tumor Pathol. 2011;28:229–38.
Rottenburger C, Hentschel M, Kelly T, Trippel M, Brink I, Reithmeier T, et al. Comparison of C-11 methionine and C-11 choline for PET imaging of brain metastases: a prospective pilot study. Clin Nucl Med. 2011;36:639–42.
Tan H, Chen L, Guan Y, Lin X. Comparison of MRI, F-18 FDG, and 11C-choline PET/CT for their potentials in differentiating brain tumor recurrence from brain tumor necrosis following radiotherapy. Clin Nucl Med. 2011;36:978–81.
Roelcke U, Bruehlmeier M, Hefti M, Hundsberger T, Nitzsche EU. F-18 choline PET does not detect increased metabolism in F-18 fluoroethyltyrosine-negative low-grade gliomas. Clin Nucl Med. 2012;37:e1–3.
Li FM, Nie Q, Wang RM, Chang SM, Zhao WR, Zhu Q, et al. (11)C-CHO PET in optimization of target volume delineation and treatment regimens in postoperative radiotherapy for brain gliomas. Nucl Med Biol 2012;39:437–42.
Ninomiya H, Oriuchi N, Kahn N, Higuchi T, Endo K, Takahashi K, et al. Diagnosis of tumor in the nasal cavity and paranasal sinuses with [11C]choline PET: comparative study with 2-[18F]fluoro-2-deoxy-d-glucose (FDG) PET. Ann Nucl Med. 2004;18:29–34.
Khan N, Oriuchi N, Ninomiya H, Higuchi T, Kamada H, Endo K. Positron emission tomographic imaging with 11C-choline in differential diagnosis of head and neck tumors: comparison with 18F-FDG PET. Ann Nucl Med. 2004;18:409–17.
Ito K, Yokoyama J, Kubota K, Morooka M, Shiibashi M, Matsuda H. 18F-FDG versus 11C-choline PET/CT for the imaging of advanced head and neck cancer after combined intra-arterial chemotherapy and radiotherapy: the time period during which PET/CT can reliably detect non-recurrence. Eur J Nucl Med Mol Imaging. 2010;37:1318–27.
Ito K, Yokoyama J, Kubota K, Morooka M. Comparison of 18F-FDG and 11C-choline PET/CT for detecting recurrences in patients with nonsquamous cell head and neck malignancies. Nucl Med Commun. 2010;31:931–7.
Wu HB, Wang QS, Wang MF, Zhen X, Zhou WL, Li HS. Preliminary study of 11C-choline PET/CT for T staging of locally advanced nasopharyngeal carcinoma: comparison with 18F-FDG PET/CT. J Nucl Med. 2011;52:341–6.
Kobori O, Kirihara Y, Kosaka N, Hara T. Positron emission tomography of esophageal carcinoma using (11)C-choline and (18)F-fluorodeoxyglucose: a novel method of preoperative lymph node staging. Cancer. 1999;86:1638–48.
Jager PL, Que TH, Vaalburg W, Pruim J, Elsinga P, Plukker JT. Carbon-11 choline or FDG-PET for staging of oesophageal cancer? Eur J Nucl Med. 2001;28:1845–9.
Liu Q, Peng ZM, Liu QW, Yao SZ, Zhang L, Meng L, et al. The role of 11C-choline positron emission tomography-computed tomography and videomediastinoscopy in the evaluation of diseases of middle mediastinum. Chin Med J. 2006;119:634–9.
Peng ZM, Liu Q, Liu QW, Yao SZ, Meng L, Liu Q, et al. The value of dual time point 11C-choline PET-CT in differentiating malignant from benign lesion of mediastinum. Zhonghua Yi Xue Za Zhi. 2007;87:3317–20.
Hara T, Inagaki K, Kosaka N, Morita T. Sensitive detection of mediastinal lymph node metastasis of lung cancer with 11C-choline PET. J Nucl Med. 2000;41:1507–13.
Pieterman RM, Que TH, Elsinga PH, Pruim J, van Putten JW, Willemsen AT, et al. Comparison of (11)C-choline and (18)F-FDG PET in primary diagnosis and staging of patients with thoracic cancer. J Nucl Med. 2002;43:167–72.
Khan N, Oriuchi N, Zhang H, Higuchi T, Tian M, Inoue T, et al. A comparative study of 11C-choline PET and [18F]fluorodeoxyglucose PET in the evaluation of lung cancer. Nucl Med Commun. 2003;24:359–66.
Hara T, Kosaka N, Suzuki T, Kudo K, Niino H. Uptake rates of 18F-fluorodeoxyglucose and 11C-choline in lung cancer and pulmonary tuberculosis: a positron emission tomography study. Chest. 2003;124:893–901.
Wang T, Sun YE, Yao SL, Yu CH, Yin DY, Tian JH. Value of carbon-11 choline positron emission tomography in patients with pulmonary abnormalities. Zhonghua Wai Ke Za Zhi. 2006;44:405–8.
Wang T, Sun YE, Chu XY, Yao SL, Yang B, Tian JH, et al. Positron emission tomography with special tracers in pulmonary abnormalities. Zhonghua Wai Ke Za Zhi. 2010;48:99–102.
Balogova S, Huchet V, Kerrou K, Nataf V, Gutman F, Antoine M, et al. Detection of bronchioloalveolar cancer by means of PET/CT and 18F-fluorocholine, and comparison with 18F-fluorodeoxyglucose. Nucl Med Commun. 2010;31:389–97.
Peng Z, Liu Q, Li M, Han M, Yao S, Liu Q. Comparison of (11)C-choline PET/CT and enhanced CT in the evaluation of patients with pulmonary abnormalities and locoregional lymph node involvement in lung cancer. Clin Lung Cancer. 2011. doi:10.1016/j.cllc.2011.09.005.
Talbot JN, Gutman F, Fartoux L, Grange JD, Ganne N, Kerrou K, et al. PET/CT in patients with hepatocellular carcinoma using [(18)F]fluorocholine: preliminary comparison with [(18)F]FDG PET/CT. Eur J Nucl Med Mol Imaging. 2006;33(11):1285–9.
Yamamoto Y, Nishiyama Y, Kameyama R, Okano K, Kashiwagi H, Deguchi A, et al. Detection of hepatocellular carcinoma using 11C-choline PET: comparison with 18F-FDG PET. J Nucl Med. 2008;49:1245–8.
Talbot JN, Fartoux L, Balogova S, Nataf V, Kerrou K, Gutman F, et al. Detection of hepatocellular carcinoma with PET/CT: a prospective comparison of 18F-fluorocholine and 18F-FDG in patients with cirrhosis or chronic liver disease. J Nucl Med. 2010;51:1699–706.
van den Esschert JW, Bieze M, Beuers UH, van Gulik TM, Bennink RJ. Differentiation of hepatocellular adenoma and focal nodular hyperplasia using 18F-fluorocholine PET/CT. Eur J Nucl Med Mol Imaging. 2011;38:436–40.
Wu HB, Wang QS, Li BY, Li HS, Zhou WL, Wang QY. F-18 FDG in conjunction with 11C-choline PET/CT in the diagnosis of hepatocellular carcinoma. Clin Nucl Med. 2011;36:1092–7.
de Jong IJ, Pruim J, Elsinga PH, Jongen MM, Mensink HJ, Vaalburg W. Visualisation of bladder cancer using (11)C-choline PET: first clinical experience. Eur J Nucl Med Mol Imaging. 2002;29:1283–8.
Picchio M, Treiber U, Beer AJ, Metz S, Bössner P, van Randenborgh H, et al. Value of 11C-choline PET and contrast-enhanced CT for staging of bladder cancer: correlation with histopathologic findings. J Nucl Med. 2006;47:938–44.
Gofrit ON, Mishani E, Orevi M, Klein M, Freedman N, Pode D, et al. Contribution of 11C-choline positron emission tomography/computerized tomography to preoperative staging of advanced transitional cell carcinoma. J Urol. 2006;176:940–4.
Maurer T, Souvatzoglou M, Kübler H, Opercan K, Schmidt S, Herrmann K, et al. Diagnostic efficacy of [11C]choline positron emission tomography/computed tomography compared with conventional computed tomography in lymph node staging of patients with bladder cancer prior to radical cystectomy. Eur Urol. 2012;61:1031–38.
Golan S, Sopov V, Baniel J, Groshar D. Comparison of 11C-choline with 18F-FDG in positron emission tomography/computerized tomography for staging urothelial carcinoma: a prospective study. J Urol. 2011;186:436–41.
Torizuka T, Kanno T, Futatsubashi M, Okada H, Yoshikawa E, Nakamura F, et al. Imaging of gynecologic tumors: comparison of (11)C-choline PET with (18)F-FDG PET. J Nucl Med. 2003;44:1051–6.
Sofue K, Tateishi U, Sawada M, Maeda T, Terauchi T, Kano D, et al. Role of carbon-11 choline PET/CT in the management of uterine carcinoma: initial experience. Ann Nucl Med. 2009;23:235–43.
Contractor KB, Kenny LM, Stebbing J, Al-Nahhas A, Palmieri C, Sinnett D, et al. [11C]choline positron emission tomography in estrogen receptor-positive breast cancer. Clin Cancer Res. 2009;15:5503–10.
Kenny LM, Contractor KB, Hinz R, Stebbing J, Palmieri C, Jiang J, et al. Reproducibility of [11C]choline-positron emission tomography and effect of trastuzumab. Clin Cancer Res. 2010;16:4236–45.
Contractor KB, Kenny LM, Stebbing J, Challapalli A, Al-Nahhas A, Palmieri C, et al. Biological basis of [¹¹C]choline-positron emission tomography in patients with breast cancer: comparison with [18F]fluorothymidine positron emission tomography. Nucl Med Commun. 2011;32:997–1004.
Zhang H, Tian M, Oriuchi N, Higuchi T, Watanabe H, Aoki J, et al. 11C-choline PET for the detection of bone and soft tissue tumours in comparison with FDG PET. Nucl Med Commun. 2003;24:273–9.
Tian M, Zhang H, Endo K. Comparison of cell proliferation, protein, and glucose metabolism in musculoskeletal tumors in a PET study. J Biomed Biotechnol. 2011;2011:807929.
Yanagawa T, Watanabe H, Inoue T, Ahmed AR, Tomiyoshi K, Shinozaki T, et al. Carbon-11 choline positron emission tomography in musculoskeletal tumors: comparison with fluorine-18 fluorodeoxyglucose positron emission tomography. J Comput Assist Tomogr. 2003;27:175–82.
Tateishi U, Yamaguchi U, Maeda T, Seki K, Terauchi T, Kawai A, et al. Staging performance of carbon-11 choline positron emission tomography/computed tomography in patients with bone and soft tissue sarcoma: comparison with conventional imaging. Cancer Sci. 2006;97:1125–8.
Nanni C, Zamagni E, Cavo M, Rubello D, Tacchetti P, Pettinato C, et al. 11C-choline vs. 18F-FDG PET/CT in assessing bone involvement in patients with multiple myeloma. World J Surg Oncol. 2007;5:68.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Treglia, G., Giovannini, E., Di Franco, D. et al. The role of positron emission tomography using carbon-11 and fluorine-18 choline in tumors other than prostate cancer: a systematic review. Ann Nucl Med 26, 451–461 (2012). https://doi.org/10.1007/s12149-012-0602-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-012-0602-7