
Abstract
Objective
Lung clearance rates of inhaled 99mTc-DTPA aerosols constitute a sensitive index to evaluate the permeability changes characteristic of airway epithelial damage. It was thought that edema of the airway wall which is reported in asthma could be relieved with a diuretic like furosemide, helping to relieve the symptoms. We intended to study the effect of inhaled furosemide on lung epithelial permeability in asthmatics and smokers with the help of 99mTc-DTPA lung clearance test (LCT).
Methods
The study included three groups (n = 15), viz. normal healthy controls, asymptomatic chronic smokers, and chronic persistent asthmatics. Each subject underwent the LCT twice, baseline and post-furosemide (Lasix) study, within a week’s interval. The post-furosemide study was carried out 15 min after inhalation of 10 mg of lasix. Lung epithelial permeability was determined in terms of clearance half-life (T 1/2).
Results
The baseline mean T 1/2 values for controls, smokers, and asthmatics were 50.95 ± 16.58, 20.81 ± 5.47, 24.06 ± 6.19 min, respectively. Post-lasix T 1/2 values were 50.83 ± 15.84, 20.70 ± 5.65, 41.27 ± 15.07 min, respectively. There was a significant difference (P < 0.001) in baseline and post-lasix clearance values in asthmatics only.
Conclusion
Baseline lung epithelial permeability was altered in smokers and asthmatics compared to the controls. Furosemide was effective only in asthmatics in reverting the permeability almost back to the normal range. Inhaled furosemide was effective even in moderate and severe asthmatics. Furosemide has multiple mechanisms of action. It possibly acts at bronchial level in view of the pathology in asthmatics lying in the airways.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Asthma affects approximately 5% of the population, causes major morbidity with days lost from work or school, and leads to heavy use of health care resources [1]. It is the predominant chronic disease in industrialized nations, and there is every indication that its prevalence is increasing throughout the world. Efficacy of the currently available drugs is limited by adverse reactions and frequent dosing with short intervals, which often impedes patient compliance. There is a need for newer and cheaper modalities of treatment.
It is not new in medicine for existing drugs to reveal unexpected properties that make them suitable for newer applications. Furosemide is one of them. In the past there has been an increasing interest in the possibility that furosemide, which has been in clinical use for more than two decades as a diuretic, may be useful in the treatment of asthma. Furosemide acts as a diuretic by reducing salt re-absorption in the thick ascending limb of loop of Henle via inhibition of Na+ K+—ATPase responsible for Na+/K+/2Cl− cotransport across the tubular epithelium [2]. It is well recognized that a change in osmolarity of the periciliary fluid in airways is a potent stimulus to airway narrowing, and may be a common cause for provoking an attack of asthma. It is thought that a change in osmolarity of the airways causes the release of inflammatory mediators, which then act to narrow the airways [3]. Furosemide, known to interfere with Na+/K+/2Cl− cotransport, may prove helpful to prevent or antagonise the osmolarity changes in airways, and may thus be useful in asthmatics.
The interest in solute exchange across the pulmonary epithelium has grown rapidly over the years. It has become increasingly evident that many pulmonary disorders must involve inopportune movement of liquids, electrolytes, and cellular elements from one to another lung compartment. Alterations in the permeability of the membranes separating these compartments may be present in a variety of both acute and chronic diseases of the lung [4]. A simple, effective and reliable method to quantitate the permeability of this epithelial membrane and its integrity would be very useful in studying the pathogenesis of lung disorders.
One of the favorite solutes to be studied is Di-ethylene tri-amine penta-acetic acid (DTPA). 99mTc-DTPA lung clearance test (LCT) is considered to be a very good tool to study lung epithelial permeability. Lung clearance rates of inhaled 99mTc-DTPA aerosols constitute a sensitive index to evaluate the permeability changes characteristic of the airway epithelium [4–6]. Lung epithelial permeability is a reflection of epithelial damage. The epithelial permeability is one of the first things to change in inflammation, infection, or injury. 99mTc-DTPA lung clearance test is one of the early indicators that can determine this change non-invasively, sensitively and non-fastidiously even before the development of clinical signs and symptoms.
Lung epithelial permeability is changed in different respiratory conditions [7–13]. It is now well accepted that there is an inflammatory process present in the airways of patients with asthma [14]. This underlying ongoing inflammation is known to be the pathological basis of different manifestations of asthma. Epithelial damage is one of the histological changes in asthma [15]. So, taking into consideration these underlying pathophysiological changes, one can expect to find an increased lung epithelial permeability in asthmatics.
Hence, combining these two aspects, viz. usefulness of furosemide in asthma and 99mTc-DTPA Lung Clearance Test, an index of epithelial permeability of lung, we planned (1) to study lung epithelial permeability in normal healthy controls, smokers, and asthmatics with the help of LCT; and (2) to study the effect of furosemide on lung epithelial permeability in these 3 groups.
Materials and methods
Study subjects
The study included 3 groups, viz. controls, smokers, and asthmatics. Each group had 15 subjects. The study was approved by the ethics committee of our institute, and informed consent was obtained from the subjects.
Group 1 included 15 non-smoking healthy volunteers (11 males and 4 females) between the ages of 18 and 54 years (mean age 29.60 ± 9.66 years).
Group 2 was made up of 15 asymptomatic chronic smokers without evidence of pulmonary diseases, between the ages of 24 and 58 years (mean age 43.07 ± 10.95 years). All the 15 smokers were males. They were smoking at least 5 cigarettes a day for at least 5 years. A unit of ‘pack-years’ was used to determine their smoking history [16]. While calculating this, a pack of 20 cigarettes was taken into consideration.
Group 3 consisted of 15 cases (7 males and 8 females) diagnosed with chronic persistent asthma between the ages of 8 and 70 years (mean age 47.93 ± 20.33 years). They were clinically categorized as mild, moderate, or severe persistent asthmatic as per established criteria [1]. They were taking β2 agonists and steroids. All asthmatics were non-smokers so as to avoid the confounding effect of smoking on airway permeability. They had been free of respiratory tract infections for at least 2 weeks and had no medication for at least 12 h before the test. All asthmatics were clinically stable at the time of the study. The consecutive patients who met the above criteria were included in the study.
Study design
Lung epithelial permeability was studied with the help of 99mTechnetium-DTPA lung clearance test. All subjects underwent LCT twice, first a baseline study and second, a post-furosemide (Lasix, Sanofi-Aventis Pharma, France) study. Post-lasix study, which followed within 1 week after the baseline study, was done 15 min after inhalation of 10 mg of lasix. Lasix was nebulized with the help of an aerosol generator, the same used for 99mTc-DTPA aerosol nebulization as described below.
All subjects underwent pulmonary function tests (PFTs) on the day of the baseline study. The parameters taken into consideration were peak expiratory flow rate (PEFR), forced expiratory volume in one-second (FEV1), and maximum mid expiratory flow rate (MMEFR).
Methods
99mTc DTPA lung clearance test [4, 5, 17]
A quantity of 15–20 mCi of 99mTechnetium-DTPA was nebulized using a dry aerosol generator manufactured by B.A.R.C. (Bhabha Atomic Research Center, Mumbai, India). It consists of a big metal box (aerosol chamber) with attached small box type instrument consisting of detachable glass tubing containing desired solution to produce aerosols with the help of inflow pipe of oxygen to produce air pressure and an outflow pipe for delivery of aerosols to face mask for inhalation. Face mask has additional outflow pipe attached further to a big plastic bag to collect exhaled air. The basis of the method to determine lung epithelial permeability is to deliver the tracer 99mTc-DTPA (mol. wt. 492 daltons) into the lungs as an aerosol, and then measure the disappearance rate from the lungs with the help of a gamma camera. The activity median aerodynamic diameter (AMAD) of the generated aerosols was 0.84 μm with an associated geometric standard deviation of 2.08. The aerosol generator consisted of an aerosol chamber that allowed settling of bigger droplets.
All subjects inhaled the 99mTc-DTPA aerosol at normal tidal volume through a mask lying in the supine position on a gamma camera table for 5 min. The camera was started along with inhalation of aerosols. Posterior views of the lungs were obtained with the help of the gamma camera (ADAC Genesys, California, USA) fitted with a low-energy, all purpose, parallel hole collimator and interfaced to a computer. Inhalation of aerosols was continued for the first 5 min to get adequate counts. Counts were acquired continuously into 128 × 128 × 16 matrix for a minimum period of 20 min at the rate of 30 s per frame. At the end of the fifth minute inhalation of aerosols was stopped and the subject continued to lie down in supine position until the end of the study. The subject was instructed not to move throughout the study.
The data were processed with the help of ADAC Pegasys computer interfaced to the gamma camera. The region of interest (ROI) was drawn over each lung, excluding hilar areas. Hot spots, if any, were not included in the ROI. There was good peripheral deposition of the aerosol radioactivity as seen by the well-outlined lung images, though separate penetration indices were not calculated. Time activity curves (Fig. 1) were derived from the counts per frame computed in an ROI drawn over each lung field. Time–activity curves were plotted with time (in seconds) on X-axis and counts on the Y-axis. Counts at peak and 7 min after the peak were taken for calculation. The reason behind the restriction to 7 min after reaching the peak was to minimize the influence of background radioactivity [18]. A least-square fit was carried out for regression analysis. Decay correction was applied to the curves. The T 1/2 value (time required for clearance of 50% of the activity from lung fields) was calculated with the help of the established formula [19]:
where N 1 = counts at peak, N 2 = counts at 7 min after peak, t 1 = time at N 1, and t 2 = time at N 2
The mean value (±2 SD) of the clearance half-life (T 1/2) of the right and left lung fields was used for data analysis. Lung epithelial permeability of 99mTc-DTPA aerosols was determined from half-life (T 1/2). The T 1/2 was calculated in minutes. Decreased T 1/2 denotes faster clearance, i.e., increased permeability, which indicates damage to the epithelial membrane.

Time–activity curves generated from dynamic data. Example of prototype baseline (on left side) and post-lasix (on right side) curves are shown for normal healthy control, smoker, and asthmatic. No change is seen in baseline and post-lasix curves for control and smoker, but in asthmatic there is a change in the curve pattern and in mean T 1/2. Post-lasix lung clearance mean T 1/2 has increased significantly only in asthmatic
Statistical analysis
Paired t test was used for comparison of baseline and post-lasix clearance half-life values in each group. Unpaired t test was used to compare T 1/2 values between the groups. Method of Karl-Pearson coefficient of correlation (r) was used to correlate T 1/2 with parameters such as pack-years, severity of asthma, and PFT parameters. P < 0.05 was considered statistically significant.
Results
Controls
The baseline mean T 1/2 for normal healthy subjects was 50.95 ± 16.58 min. The post-lasix mean T 1/2 just fractionally dropped down to 50.83 ± 15.84 min. Thus, there was no statistically significant difference between baseline and post-lasix lung clearance (P > 0.1, not significant) indicating no effect of furosemide on lung epithelial permeability in normal healthy controls (Figs. 1, 2, 3). There was no correlation between age and lung clearance (T 1/2) indicating that age was not an influencing factor for lung epithelial permeability (P > 0.1). Also, lung epithelial permeability was not influenced by the sex of the subject. All the three parameters of PFT for all controls were above the minimum normal predicted levels.

Comparison of 99mTc-DTPA lung clearance (T 1/2) in controls, smokers, and asthmatics. No change between baseline and post-lasix mean T 1/2 values for controls and smokers but statistically significant change in case of asthmatics (P < 0.001)

Baseline and post-lasix distribution of lung clearance T 1/2 values is shown for controls, smokers, and asthmatics. No change between baseline and post-lasix values in controls and smokers but significant change in asthmatics
Smokers
The baseline mean T 1/2 value was 20.81 ± 5.47 min. This was significantly less than the baseline mean T 1/2 value for the controls (P < 0.001) indicating the lung epithelial damage in smokers. The post-lasix mean T 1/2 just fractionally dropped down to 20.70 ± 5.65 min. Thus, there was no statistically significant difference between baseline and post-lasix lung clearance (P > 0.1) indicating no effect of furosemide on lung epithelial permeability in smokers (Figs. 1, 2, 3).
When 99mTc-DTPA lung clearance (T 1/2) was correlated with pack-years in smokers, a statistically significant negative correlation was found indicating decrease in T 1/2 value with increasing number of pack-years (P < 0.05). This meant that as the number of cigarettes and the duration of smoking increased, the lung permeability also increased indicating more damage. In PFTs, the two parameters PEFR and FEV1 were above the minimum normal predicted levels. In 10 of 15 smokers, the MMEFR was just marginally lower than minimum normal predicted levels indicating very mild small airway obstruction. There was no statistically significant correlation between lung clearance T 1/2 values and MMEFR (P > 0.1).
Asthmatics
The baseline mean T 1/2 for asthmatics was 24.06 ± 6.19 min (Table 1). This was significantly less than the corresponding value for the controls indicating the lung epithelial damage occurring in chronic persistent asthma (P < 0.001). The post-lasix mean T 1/2 was 41.27 ± 15.07 min (Table 1). This was significantly different than the baseline value (P < 0.001). This statistically significant difference in the lung clearance after furosemide inhalation indicates the effectiveness of furosemide on lung epithelial permeability in asthmatics (Figs. 1, 2, 3). There was no statistically significant difference between the baseline mean T 1/2 for the normal healthy controls and the post-lasix mean T 1/2 for the asthmatics (P > 0.1) indicating permeability approaching the normal range after furosemide inhalation.
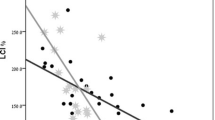
The pulmonary function tests in these asthmatic subjects were deranged depending on their severity of asthma. There was a statistically significant negative correlation between lung clearance T 1/2 values and severity of asthma indicating increase in lung epithelial permeability with increasing severity of asthma (Fig. 4a) (P < 0.05). Also, there was a statistically significant positive correlation between lung clearance T 1/2 values and the three PFT parameters, viz. PEFR, FEV1, MMEFR (Fig. 4b, c, d, respectively) (P < 0.05) indicating decrease in T 1/2 values with decrease in PFT values; in other words, increased permeability with increased severity of asthma.

Correlation between 99mTc-DTPA lung clearance (T 1/2) and severity of asthma, PEFR, FEV1, MMEFR in asthmatics
No adverse effect of inhaled lasix was seen in the form of diuresis or anything else in any of the groups.
Discussion
Interest in furosemide having effects on the airways has been sparked by the observation that inhaled furosemide can inhibit a variety of bronchoconstrictor challenges in asthma. It was thought that edema of the airway wall which is reported in asthma could be relieved with a diuretic like furosemide, helping to relieve the symptoms.
A quantity of 10 mg of lasix was taken instead of 5 mg in the study of Inoue et al. [20], to compensate for the loss in dead space of the BARC aerosol generator. Also, the asthmatic patients selected by Inoue et al. had normal PFT parameters, whereas the asthmatic patients in the present study had deranged PFTs. This group included mild, moderate, and severe chronic persistent asthmatics. Inoue et al. [20] showed the effectiveness of inhaled lasix in mild asthmatics. The present study has shown such additional benefit even in moderate and severe chronic persistent asthmatics.
There was hardly any difference between baseline and post lasix T 1/2 values for controls (Fig. 3). Thus, furosemide given by inhalation does not have any effect on normal, healthy, intact lung epithelium. No diuresis was observed in any of the subjects. Neither age nor sex of the subject influenced the lung epithelial permeability. Thus, in normal, healthy persons the epithelium would still be intact with advancing age, irrespective of sex.
The baseline lung clearance half-life in smokers was significantly lower than that of controls (Fig. 2). This significantly increased lung epithelial permeability in smokers which indicates damage to the lung epithelium. Damage does occur to the epithelium in smokers that may not be clinically perceptible, or even PFTs may not shed more light on it in early stages.
The different histological changes seen in smokers include basal cell hyperplasia, loss of cilia in some areas, occurrence of cells with atypical nuclei, and loss of alveolar attachments [21, 22]. Using an electron microscope Simani et al. [23] have shown the damage occurring in the alveolar and bronchial epithelium of animals exposed to cigarette smoke. The effect of cigarette smoke on the alveolar epithelium may be due to the chronic effects of carbon monoxide (CO) exposure [24]. Other possible mechanisms include the action of nicotine, catecholamines, NO, NO2, and other constituents of cigarette smoke. The damage also occurs due to the inflammatory mediators released by effector or structural cells exposed to the cigarette smoke [25]. Alveolar macrophages may also play a part in it.
The possibility of cigarette smoke causing damage to the alveolar-capillary barrier is of considerable importance in understanding the pathogenesis of disorders related to cigarette smoking. 99mTc-DTPA lung clearance test provides us with a sensitive, simple, and non-invasive procedure to study the integrity of the pulmonary epithelium and alveolar-capillary barrier. This picks up the earliest changes that would not be shown by other tests, like PFT, so easily. Stopping smoking might allow the epithelium to repair so that the disrupted barrier would have a chance to recover.
Furosemide inhalation in smokers did not affect the lung epithelial permeability as post-lasix mean T 1/2 did not change significantly. Thus, even though in smokers the lung epithelial permeability is increased compared to controls, the furosemide inhalation does not have any effect on it.
The baseline lung epithelial permeability was significantly increased in asthmatics compared to controls. The subjects in this study group were chronic persistent asthmatics. They were having frequent attacks of asthma for which they needed regular therapy. Asthma is considered to be an inflammatory, desquamative condition [14]. Keeping this and other histologic changes seen in asthma [15] in mind, the lung epithelium in chronic persistent asthmatics is not expected to be normal and intact. And that is why there is faster clearance of solutes across the lung epithelium indicating the damage to the epithelium.
Lemarchand et al. [26] have observed similarly increased DTPA bronchial clearance in asthmatics during acute attacks of asthma. They further observed that clearance values decreased within 4 weeks after treatment of acute attacks, but remained increased compared to the values in a control group. Thus, the permeability remains increased for sometime even after treatment of acute attacks. Hence, chronic persistent asthmatics would also show increased permeability, as seen in our study, as they have repeated attacks of asthma. This increased airway permeability in asthmatics may lead to increased hyperresponsiveness because of increased access of the allergens and may further aggravate the problem [15].
In our study, a statistically significant negative correlation was found between lung clearance T 1/2 values and severity of asthma (Fig. 4a). That means as the severity of asthma increased, the T 1/2 value decreased. Or in other words, in terms of permeability we can say that as the severity of asthma increased, the lung epithelial permeability increased indicating more epithelial damage.
Also, a statistically significant positive correlation was found between lung clearance T 1/2 values and the three PFT parameters, viz. PEFR, FEV1, MMEFR when they were correlated individually (Fig. 4b, c, d, respectively) in asthmatics. This suggests that in chronic persistent asthmatics lung epithelial permeability as well as PFTs are affected. PFTs and LCT indicate two different pathologies, viz. bronchoconstriction and epithelial damage, respectively. Presence of a statistically significant positive correlation between these two suggests simultaneous existence of the above two pathologies in asthma in proportion to the severity of damage.
The clearance rate of 99mTc-DTPA includes three components: alveolar permeability, bronchial mucosal permeability, and mucociliary transport [20]. We have taken care to exclude the third component of mucociliary transport by excluding the hilar regions while drawing regions of interest. With the submicronic particle size of aerosols, like what we have used, the particles (99mTc-DTPA) are supposed to reach the alveoli. But in view of the presence of small airway obstruction in asthma (more so in moderate and severe asthmatics), less particles of 99mTc-DTPA are likely to reach alveoli and are more likely to be deposited in smaller airways, and the information we obtain is mainly about the airway permeability, i.e., mucosal permeability, which one should be interested in while studying asthmatics because it is the airways where the pathology lies in asthma and not the alveoli [1, 14, 15]. Thus, the technique is suitable to study chronic persistent asthmatics with small airway obstruction as we can get the information about mucosal permeability and not just the alveolar permeability. Our result showing increased permeability in chronic persistent asthmatics is more likely to be due to the changes in bronchial mucosa.
However, some studies have shown the presence of alveolar tissue inflammation in asthma, especially so in nocturnal asthma [27]. It was seen that inflammation extended well beyond the airway smooth muscle and was significant even around the pulmonary arteries. If this is substantiated then it can further corroborate the finding of increased permeability in asthmatics, at least in mild asthmatics wherein radiotracer particles can reach the alveoli. In the absence of small airway obstruction we would expect the particles to reach alveoli and the information derived would be mainly about alveoli. So, in smokers the decreased clearance T 1/2 values indicate the presence of pathology mainly in alveoli. The available literature supports this contention [16, 23–25].
After inhalation of lasix (furosemide), the mean clearance T 1/2 value increased considerably toward the normal range in asthmatics. This proves the effectiveness of furosemide on lung epithelial permeability in chronic persistent asthmatics which otherwise is increased. This predicts the usefulness of furosemide in asthmatics. Thus, using this novel concept of lung epithelial permeability we have tried to show that furosemide can be useful in asthmatics.
The affair with furosemide began in 1988 when Bianco et al. [28] for the first time showed that inhaled furosemide prevented exercise-induced bronchoconstriction in asthmatic patients. The protective profile of furosemide shows that it is inactive against bronchoconstrictors that act directly on airway smooth muscle, such as histamine, methacholine and PGF2α, but is active against bronchoconstrictor mechanisms that act through “indirect mechanisms” [29, 30].
How does furosemide produce these effects? The drug inhibits the inward movement of chloride via the electrically neutral Na+/K+/2Cl− cotransporter in the basolateral membrane of epithelial cells, and so reduces chloride and sodium secretion into the airway lumen. This altogether results in the reduction of hypersecretion of bronchial mucosa in asthmatics [31]. Alteration of the osmotic or ionic composition of epithelial lining fluid might inhibit release of mediators from luminal mast cells after inhalation of antigen or as a consequence of hyperosmolarity induced by exercise and hyperventilation, or it might reduce sensory nerve input from the lumen. Another possibility is that inhibition of Na+/K+/2Cl− cotransporter may affect the resting membrane potential making the threshold voltage for depolarization more difficult to reach [32].
Inhibition of Na+/K+/2Cl− cotransport in vitro is seen only when furosemide is added to the mucosal surface of epithelial cells. So, it is perhaps surprising that nebulized furosemide, delivered to the luminal surface of the airways, is effective unless the increased permeability of the epithelial barrier in asthma allows the drug access to the basolateral membrane of the epithelial cell.
One possible action of furosemide in the airways may be to stimulate the production of PGE2, particularly from the airway epithelium which may be an important source of PGE2 [30]. Furosemide inhibits airway microvascular leakage induced by sodium metabisulphite aerosol in guinea pigs [30]. Rodwell et al. [33] felt that furosemide may block the release of neurotransmitters from excitatory non-adrenergic, non-cholinergic nervous system such as substance P. Also, furosemide might stimulate the release of bronchodilating mediators such as vasoactive intestinal peptides (VIP) and nitric oxide (NO) from airway epithelium.
The transepithelial clearance rate of 99mTc-DTPA follows the equation [6]:
where C is the concentration at time t, C 0 is the initial concentration of inhaled aerosol, P is the permeability of the membrane, S is the surface area of the membrane and V is the epithelial lining fluid volume. Inhaled furosemide may decrease the permeability (P) or surface-to-volume ratio (S/V) on which aerosol is deposited by inhibition of ion and water transport.
Though the lung epithelial permeability was increased in both smokers and asthmatics, it was only in asthmatics that furosemide was effective. The inhaled furosemide seemed to mainly affect the mucosal permeability in view of the known pathophysiology of asthma. Furosemide may be acting on Na+ Cl− cotransporter in the epithelial cells at the mucosal level and not at the alveolar level. In smokers, the initial damage is mainly at the alveolar level [16, 23, 24, 34]. Different pathophysiological backgrounds underlying the increase in the pulmonary clearance rate of 99mTc-DTPA in smokers and asthmatics may explain the different responses to the inhaled furosemide.
It was observed that in some asthmatics lung epithelial permeability did not change to the extent to it did in others after lasix administration. Possibly furosemide treatment would not be that effective in these particular cases, and they may not respond to furosemide inhalation therapy. 99mTc-DTPA lung clearance test gives us an easy way to find out whether the patient would respond to furosemide inhalation therapy or not. Accordingly, we can decide our management strategy. This aspect needs to be studied further to incorporate this utility into practice.
Thus, our data support the presence of a furosemide sensitive mechanism in asthmatics. Furosemide inhalation was effective not only in mild asthmatics but also in moderate and severe asthmatics in restoring the deranged epithelial permeability. This implies better prospects for the use of furosemide in the treatment of asthma. A beneficial effect of inhaled furosemide can be expected in patients with bronchial hyperreactivity in the form of reduced access of allergens and, thereby, prevention of bronchoconstriction. This needs to be confirmed with more studies.
Lung isotope studies have the potential to be thoroughly explored and applied for the management of asthma and development of new drugs. They reveal early changes, like in smokers, and underlying subclinical alterations, like in chronic persistent asthmatics, which otherwise would go unnoticed until the patient presents with the problem. They provide us with the evidence for the need of continued treatment even in the absence of attacks of asthma. Also, they may help us in deciding the treatment, choosing the drug, and continuing the drug. Another possible use of this methodology of radionuclide lung scan can be to evaluate inhaled drug distribution in lungs. For e.g., drug solution and 99mTc-DTPA solution can be mixed and nebulized together with this aerosol generator and the distribution of drug can be studied under a gamma camera.
Conclusion
The results of our study showed that lung epithelial permeability was significantly increased in smokers and asthmatics. But, furosemide was effective only in asthmatics in reverting the permeability almost back to normal range. This lends further support to the idea of the presence of a furosemide sensitive mechanism in asthmatics. Inhaled furosemide was effective even in moderate and severe asthmatics. Furosemide seems to possess multiple mechanisms of action. It possibly acts at a bronchial level in view of the pathology in asthmatics lying in the airways. 99mTc-DTPA lung clearance test can detect early and subclinical changes which otherwise would go unnoticed until the appearance of symptoms in various lung conditions.
References
Mcfadden ER. Asthma. In: Fauci ASKD, Longo DL, Braunwald E, Hauser SL, Jameson JL, editors. Harrison’s principles of internal medicine. 16th ed. New York: McGraw-Hill; 2005. p. 1508–16.
Suki WN, Eknoyan G, Martinez-Maldonado M. Tubular sites and mechanisms of diuretic action. Annu Rev Pharmacol. 1973;13:91–106.
Anderson SD, Smith CM. Osmotic challenges in the assessment of bronchial hyperresponsiveness. Am Rev Respir Dis. 1991;143(3 Pt 2):S43–6.
Effros RM, Mason GR. Measurements of pulmonary epithelial permeability in vivo. Am Rev Respir Dis. 1983;127(5 Pt 2):S59–65.
Staub NC, Hyde RW, Crandall E. NHLBI workshop summary. Workshop on techniques to evaluate lung alveolar-microvascular injury. Am Rev Respir Dis. 1990;141(4 Pt 1):1071–7.
Susskind H. Technetium-99m-DTPA aerosol to measure alveolar-capillary membrane permeability. J Nucl Med. 1994;35(2):207–9.
Gumuser FG, Pirildar T, Batok D, Sakar A, Ruksen E, Sayit E. Assessment of alveolar epithelial permeability in Behcet’s disease with 99mTc-DTPA aerosol scintigraphy. Ann Nucl Med. 2008;22(5):349–55.
Kaya E, Fidan F, Unlu M, Sezer M, Tetik L, Acar M. Evaluation of alveolar clearance by Tc-99m DTPA radioaerosol inhalation scintigraphy in welders. Ann Nucl Med. 2006;20(8):503–10.
Aydin A, Kiter G, Durak H, Ucan ES, Kaya GC, Ceylan E. Water-pipe smoking effects on pulmonary permeability using technetium-99m DTPA inhalation scintigraphy. Ann Nucl Med. 2004;18(4):285–9.
Kula M, Gulmez I, Tutus A, Coskun A, Gursoy S, Oymak S. Impaired lung epithelial permeability in hepatitis C virus antibody positive patients detected by 99mTc-DTPA aerosol scintigraphy. Nucl Med Commun. 2002;23(5):441–6.
Yuksel H, Yuksel D, Demir E, Tanac R. Influence of inhaled steroids on pulmonary epithelial permeability to Tc99m-dTPA in atopic asthmatic children. J Investig Allergol Clin Immunol. 2001;11(3):188–92.
Uh S, Lee SM, Kim HT, Chung Y, Kim YH, Park CS. The clearance rate of alveolar epithelium using 99mTc-DTPA in patients with diffuse infiltrative lung diseases. Chest. 1994;106(1):161–5.
Caner B, Ugur O, Bayraktar M, Ulutuncel N, Mentes T, Telatar F, et al. Impaired lung epithelial permeability in diabetics detected by technetium-99m-DTPA aerosol scintigraphy. J Nucl Med. 1994;35(2):204–6.
Hogg JC, James AL, Pare PD. Evidence for inflammation in asthma. Am Rev Respir Dis. 1991;143(3 Pt 2):S39–42.
Laitinen LA, Heino M, Laitinen A, Kava T, Haahtela T. Damage of the airway epithelium and bronchial reactivity in patients with asthma. Am Rev Respir Dis. 1985;131(4):599–606.
Tashkin DP, Kleerup EC, Hoh CK, Kim KJ, Webber MM, Gil E. Effects of ‘crack’ cocaine on pulmonary alveolar permeability. Chest. 1997;112(2):327–35.
Oberdorster G, Utell MJ, Morrow PE, Hyde RW, Weber DA. Bronchial and alveolar absorption of inhaled 99mTc-DTPA. Am Rev Respir Dis. 1986;134(5):944–50.
Morrison D, Skwarski K, Millar AM, Adams W, MacNee W. A comparison of three methods of measuring 99mTc-DTPA lung clearance and their repeatability. Eur Respir J. 1998;11(5):1141–6.
Levin S. Statistical methods. In: Harbert JRA, editor. Textbook of Nuclear Medicine. 2nd ed. Philadelphia: Lea & Febiger; 1984. p. 70–91.
Inoue T, Shigeta M, Mochizuki H, Shimizu T, Morikawa A, Suzuki H, et al. Effect of inhaled furosemide on lung clearance of technetium-99m-DTPA. J Nucl Med. 1995;36(1):73–7.
Auerbach O, Hammond EC, Garfinkel L. Changes in bronchial epithelium in relation to cigarette smoking, 1955–1960 vs. 1970–1977. N Engl J Med. 1979;300(8):381–5.
Saetta M, Finkelstein R, Cosio MG. Morphological and cellular basis for airflow limitation in smokers. Eur Respir J. 1994;7(8):1505–15.
Simani AS, Inoue S, Hogg JC. Penetration of the respiratory epithelium of guinea pigs following exposure to cigarette smoke. Lab Invest. 1974;31(1):75–81.
Jones JG, Minty BD, Lawler P, Hulands G, Crawley JC, Veall N. Increased alveolar epithelial permeability in cigarette smokers. Lancet. 1980;1(8159):66–8.
Susskind H, Weber DA, Volkow ND, Hitzemann R. Increased lung permeability following long-term use of free-base cocaine (crack). Chest. 1991;100(4):903–9.
Lemarchand P, Chinet T, Collignon MA, Urzua G, Barritault L, Huchon GJ. Bronchial clearance of DTPA is increased in acute asthma but not in chronic asthma. Am Rev Respir Dis. 1992;145(1):147–52.
Kraft M, Djukanovic R, Wilson S, Holgate ST, Martin RJ. Alveolar tissue inflammation in asthma. Am J Respir Crit Care Med. 1996;154(5):1505–10.
Bianco S, Vaghi A, Robuschi M, Pasargiklian M. Prevention of exercise-induced bronchoconstriction by inhaled frusemide. Lancet. 1988;2(8605):252–5.
Bianco S, Pieroni MG, Refini RM, Robuschi M, Vaghi A, Sestini P. Inhaled loop diuretics as potential new anti-asthmatic drugs. Eur Respir J. 1993;6(1):130–4.
Chung KF. Furosemide and other diuretics in asthma. J Asthma. 1994;31(2):85–92.
Widdicombe JH, Nathanson IT, Highland E. Effects of “loop” diuretics on ion transport by dog tracheal epithelium. Am J Physiol. 1983;245(5 Pt 1):C388–96.
Elwood W, Lotvall JO, Barnes PJ, Chung KF. Loop diuretics inhibit cholinergic and noncholinergic nerves in guinea pig airways. Am Rev Respir Dis. 1991;143(6):1340–4.
Rodwell LT, Anderson SD, Spring J, Mohamed S, Seale JP. Effect of inhaled frusemide and oral indomethacin on the airway response to hypertonic saline challenge in asthmatic subjects. Thorax. 1997;52(1):59–66.
Niden AH. The effects of low levels of carbon monoxide on the fine structure of terminal airways. Am Rev Respir Dis. 1971;103:898.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bhure, U.N., Bhure, S.U., Bhatt, B.M. et al. Lung epithelial permeability and inhaled furosemide: added dimensions in asthmatics. Ann Nucl Med 23, 549–557 (2009). https://doi.org/10.1007/s12149-009-0275-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-009-0275-z