
Abstract
Purpose
To predict the burden of cancer in Catalonia by 2020 assessing changes in demography and cancer risk during 2010–2020.
Methods/patients
Data were obtained from Tarragona and Girona cancer registries and Catalan mortality registry. Population age distribution was obtained from the Catalan Institute of Statistics. Predicted cases in Catalonia were estimated through autoregressive Bayesian age-period-cohort models.
Results
There will be diagnosed 26,455 incident cases among men and 18,345 among women during 2020, which means an increase of 22.5 and 24.5 % comparing with the cancer incidence figures of 2010. In men, the increase of cases (22.5 %) can be partitioned in three components: 12 % due to ageing, 8 % due to increase in population size and 2 % due to cancer risk. In women, the role of each component was 9, 8 and 8 %, respectively. The increased risk is mainly expected to be observed in tobacco-related tumours among women and in colorectal and liver cancers among men. During 2010–2020 a mortality decline is expected in both sexes.
Conclusion
The expected increase of cancer incidence, mainly due to tobacco-related tumours in women and colorectal in men, reinforces the need to strengthen smoking prevention and the expansion of early detection of colorectal cancer in Catalonia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Predicting the number of new cancer cases in a given population is essential for health services planning. This is defined in terms of diagnosis, treatment and required support to guarantee quality care to cancer patients [1]. Predicting the behaviour of a disease is largely dependent on the changes in the most recent cancer trends, since the last period of available data is the most influential one. The estimated future population and the choice of the statistical method used are also clue factors in the prediction. In this context it should be noted that the burden can be quantified in two ways: (1) describing the age-adjusted rates, which take into account changes in the ageing and in the population size and (2) quantifying the number of patients for health planning purposes, which is considered to be more helpful.
This article aims to predict the number of cases and the rates of cancer incidence and mortality in Catalonia during the period 2010–2020, making use of the observed cancer data during 1993–2007 according to sex, age and tumour site.
Materials and methods
Incidence data were supplied by the Tarragona and Girona cancer registries and mortality data by the Catalan mortality registry. Catalan population and their age distribution were provided by the Catalan Institute of Statistics. Cancer data were available for the period 1993–2007 and were stratified by sex, age-groups and tumour site [1]. Data were arranged in three 5-year periods (1993–1997, 1998–2002, 2003–2007) and eighteen 5-year age-groups (0–4 years to ≥85 years). The future population and age distribution for the periods 2008–2012, 2013–2017 and 2018–2022 were used in the incidence and mortality projections.
Bayesian modelling methods were used to estimate cancer rates in Catalonia for 1993–2007 [1]. Making use of these estimates, Bayesian autoregressive age-period, age-cohort and age-period-cohort models [2] were fitted to data from period 1993–2007 and these models were used to predict incidence/mortality for the period 2008–2020 assuming Poisson distribution for the number of cases. Since cancer incidence in Catalonia was estimated on the basis of data from two cancer registries which cover 20 % of the Catalan territory [1], geographic variability cannot be assessed as a whole. In this line, we could uniquely assume homogeneous rates in Catalonia based on data from the Cancer registries. Details of the models used are described in the Supplementary material file. Making use of the predicted number of cancer cases/deaths, tables present results which were generated through the web-application REGSTATTOOLS [3], showing crude, age-adjusted rates and the number of cases according to age-groups. Specific modelling was used for prostate cancer incidence which showed a dramatic rise during 1993–2007 [3]. Since it seems unlikely to expect a similar rise during 2010–2020, we have assumed that incidence remained constant during 2003–2007 [4].
The percentage change in incident cases between 2010 and 2020 was calculated through the web-application RiskDiff [5] that makes use of the Bashir and Estève method [6]. This method allows decomposing the net difference in the number of cases between these 2 years into demographic and cancer risk changes as: difference (%) = demography (%) + cancer risk (%) = age distribution (%) + population size (%) + cancer risk (%).
Results
Incidence
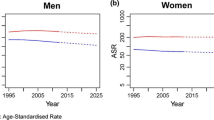
Considering overall age-standardized cancer incidence, excluding skin non-melanoma, by 2020 a levelling off is expected among men (2010: 343.4 per 105; 2020: 345.3 per 105) and an increase among women (2010: 211.4 per 105; 2020: 227.0 per 105). Taking into consideration the number of cases, these will increase by 23 % among men and 24 % among women. During 2010, there were 21,592 new cases in men and 14,741 in women, whereas in 2020, 26,455 and 18,345 cases will be diagnosed respectively. In men, the rise in the cases will be more important in the population older than 65 years than in the youngest (27 and 9 %, respectively), whereas in women, this difference will be smaller (30 and 20 %) (Table 1; Fig. 1).



Observed and projected incidence and mortality age-adjusted rates for the period 1993–2007 and 2008–2020 in Catalonia. When the values of mortality rates are less than 1 per 105 in men or women, they are not shown in the figure
In men, the tumours showing higher increase among the oldest population are colorectal (≥65 years: 56 %; 35–64 years: 30 %), pancreas (44 %; 28 %, respectively), lung (23 %; −11 %) and bladder (18 %; −18 %). Tumours that will mainly increase among the youngest ones are liver (≥65 years: 41 %; 35–64 years: 122 %), gallbladder (40 %; 87 %), melanoma (18 %; 31 %) and kidney (52 %; 66 %). In both age-groups, similar growth pattern will be expected for prostate (29 %; 26 %) and haematologic neoplasms (36 %; 32 %) and, a decline pattern, for oral cavity/pharynx (−8 %; −24 %), oesophagus (−24 %; −29 %), stomach (−11 %; −27 %) and larynx (−9 %; −16 %) (data not shown, calculated from the ratio between cases of the same age-group in the year 2020 and those in the 2010) (Table 1).
In older women an important increase will be expected for lung (≥65 years: 233 %; 35–64 years: 149 %), kidney (88 %; 20 %) and oral cavity/pharynx (51 %; 41 %) tumours; a intermediate increase on breast (23 %; 10 %), colorectal (20 %; 13 %) and pancreas (20 %; −29 %). In younger ones, increase is expected for liver (3 %; 12 %) and haematological malignancies (38 %; 79 %). Tumours showing decrease in both age-groups are those of stomach (−7 %; −21 %), gallbladder (−33 %; 0 %), endometrium (0 %; −3 %) and ovary (−3 %; −10 %) (Table 1).
The role of the demography and of the cancer risk on the difference in incident cases between 2010 and 2020 is showed in Tables 2, 3 and in Fig. 2. In young men, the largest increase of incident cases is predicted for liver cancer, being cancer risk the leading factor. In the older, the predicted large increase of colorectal cancer is attributable of the growing population and the rise of cancer risk. A decline on the number of tobacco-related tumours is expected among the youngest (larynx, oral cavity/pharynx, bladder and lung), whereas in the elderly, an increase of lung and bladder tumours is still expected attributable to growing population (Table 2; Fig. 2).

Net difference between the number of incident cases in 2020 and in 2010 according to sex, tumour site and age-groups. The vertical segment indicates the total variation from incident cases between the years 2010 and 2020. Red is the variation explained by the risk of cancer, navy blue indicates the variation attributable to ageing and light blue to the population growth
In women, regardless of age, it is expected a substantial rise in incidence of lung and larynx cancer being attributable mainly to increased cancer risk. On the contrary, it is expected a decline of gynaecological tumours mainly due to the decrease in the risk. Breast cancer will increase due to increase of population size, but in younger women, breast cancer risk will decrease (Table 3; Fig. 2).
For both sexes, mainly among elderly, we expect an increase in kidney, pancreas and haematologic tumours due to changes in population size and cancer risk. Likewise, a fall of gastric cancer is also predicted due to the decline of cancer risk (Tables 2, 3; Fig. 2).
Mortality
We predict a decline of adjusted mortality rates from all cancers in men (2010: 127, 2 per 105; 2020: 91.0 per 105) and a levelling off in women (2010: 57.6 per 105; 2020: 56.6 per 105) (Table 1; Fig. 1). Considering the number of deaths, it is expected a slight decrease in men (2010: 10,164; 2020: 9,855) and an increase in women (6,479; 6,991, respectively). The decrease in deaths among men lies mainly in the younger group (>65 years: −0.3 %; 35–64 years: −21 %) whereas the rise in deaths among women falls mostly on the older (>65 years: 8 %; 35–64 years: 6 %) (Table 4).
According to the tumour site, a greater increase of deaths among older men compared to the younger in pancreas (≥65 years: 61 %; 35–64 years: 40 %) and melanoma (22 %; 13 %, respectively) is expected. By contrast, in younger men our predictions showed higher mortality in liver cancer (26 %; 92 %) and lower mortality in oral cavity/pharynx (−9 %; −47 %), oesophagus (−7 %; −42 %), colorectal (−36 %; −61 %), lung (1 %; −41 %), prostate (−0.2 %; −6 %), bladder (−9 %; −14 %) and haematologic neoplasms (0.3 %; −15 %) (Table 4).
In women, a greater increase of deaths among older ones compared to the younger ones in tumours of lung (≥65 years: 114 %; 35–64 years: 23 %, respectively), pancreas (33 %; 12 %), cervix (31 %; 0 %), melanoma (22 %; 6 %) and haematologic neoplasms (3 %; −13 %) is expected. By contrast, among the younger it is predicted the highest increase in mortality of liver (−8 %; 35 %) and bladder (11 %; 100 %). In both age groups, mortality due to breast (−15 %; −11 %) and colorectal (−3 %; −4 %) cancers will decline.
Discussion
For the next decade, cancer projections in Catalan men predict a levelling off in their incidence rates and a decline in the mortality ones. In women, a slight rise of incidence and a stabilization of mortality will be expected. This pattern is similar to other previously published European studies [7, 8]. In order to assess the impact of cancer in a country, predicting the number of incident patients instead of only predicting age-adjusted rates might be more useful since these last do not show the demographic changes of the population [6].
The expected number of incident cases in 2020 will have a significant impact in Catalonia. The number of new diagnoses will increase by 23 % in men and 24 % in women compared to 2010. In men, 12 % of the increase might be attributable to changes in age structure (ageing), 8.3 % due to increase of population size and 2.4 % due to increase of cancer risk. In women, the expected rise in incident cases due to ageing, population size and risk are 8.6, 8.4 and 7.5 %, respectively. Since ageing and population size are not avoidable, there are no mechanisms for reducing their impact. This is a key point, especially in men, because the predicted increase on the overall incident cases is largely explained by the demographic changes. By contrast, in women, one-third of the expected rise in incidence depends on the cancer risk changes. The detailed tumour-site analysis according to demography and cancer risk could be useful to identify those tumours that could be initially controlled by implementing specific primary prevention programs.
In Catalonia, the increased incidence of colorectal, kidney, liver, pancreas and the haematological tumours is mainly associated to cancer risk rise. In younger men, tumours associated to cancer risk rise are those of liver, kidney, melanoma and the haematological. In women, regardless of the age, a cancer risk rise is expected for tobacco-related tumours such as lung and oral cavity/pharynx and also haematologic malignancies.
In 2004, the International Agency for Research on Cancer judged that there was sufficient evidence in humans that tobacco smoking causes cancers of the lung, larynx, oral cavity/pharynx, paranasal sinuses, oesophagus, stomach, pancreas, liver, kidney, ureter, bladder, cervix and myeloid leukaemia [9]. The predicted variations in tobacco-related tumours time trends by sex largely reflect differences in the stage and degree of the tobacco epidemic [10]. Smoking initiation and cessation rates in Catalan population according to gender are important markers to explain the current and future trends in these tumors [11]. While tobacco-related tumours trends in men are declining in Catalonia, these increased in women several years after they did in men because of adherence to smoking among women started several decades later than in men. A recent study conducted in UK on mortality data, estimated that in women, 84 % of lung cancer were due to smoking [9]. The predicted increase on cancer risk for these tumours in Catalan women in all age-groups suggests that cancer burden, mainly lung cancer, will continue to increase for several decades unless anti-tobacco interventions are intensified and smoking prevalence will decrease more significantly [11].
Colorectal cancer incidence projections describe an increasing trend in men and a levelling off in women. Increase of colorectal incidence in both sexes has been described in other developed countries [7, 8, 12] and it has been related to a combination of risk factors including changes in dietary patterns, obesity and the less physical activity. In Catalonia, there has not been found a great difference on the prevalence of these risk factors according to gender in order to explain this divergence [13]. The recent implementation of limited screening programs in some Catalan regions will not have an immediate impact on incidence due to the limited coverage and adherence. Even so, preliminary results not yet published of screening, show that although women participate more than men, these last are diagnosed most frequently of pre-malignant and malignant lesions than women. The predicted decline of mortality trends in both sexes is due to largely of improvement of treatments [14], awareness increasing and early detection by means the opportunistic detection [15].
Liver cancer, globally, is two-fold higher in men than in women. Incidence and mortality are increasing in many developed parts of the world, possibly due to the obesity epidemic and the rise in HCV infection through continued transmission by injection drug users 30 years ago [16]. For younger Catalan men the significant increase in the incidence and mortality is mainly explained by an increased cancer risk. This prediction is consistent with the high prevalence of HCV/HBV infections described among the young cohorts of intravenous drug users and the implementation of the highly active antiretroviral therapies for HIV in the 1990s [17]. Surely, the low number of cases in women in the cancer registries did not allow making a more precise analysis to draw conclusions in this gender.
The increase in breast cancer incidence in Catalonia since the 1980s likely results from changes in reproductive factors, the increased use of postmenopausal hormone therapy as well as an increased screening intensity [18]. For 2020, it is anticipated in Catalonia a slight decrease in incidence, as already described in the US, UK, France and Australia [19–21]. Nevertheless, we expect an increase in incident cases among older women largely explained from ageing. The increased of incident cases in the younger women could be entirely attributable to demographic changes because it is expected a risk reduction due to screening saturation as described above in Spain [22]. In contrast, breast cancer deaths will continue to decline related to nationwide screening programme and the treatment improvement [2, 18].
Although we previously forecast an increase in melanoma incidence in Catalonia [23], our predictions based with recent data show a slight decrease in women and stabilization in men. The decrease in women is expected due to the fall of the risk and, the increase in men because demographic shifts and the permanence of cancer risk. These results are in agreement with those from Australia, New Zealand, the US, Canada and Norway where has been described that melanoma incidence have increased steadily over the generations born in the late 1940s, and a stabilization or decrease in cohorts born more recently [24].
Changing classifications of haematologic malignancies complicate the interpretation of their incidence/mortality trends. Our analysis of all grouped morphologic subtypes predicts a slight increase in incidence and a decrease in the mortality in both sexes. Detailed analysis according morphology predicts NHL incidence stabilization and a slight increase of leukaemia, similar to those published in the US and Spain, where NHL incidence has shown a plateau over the past 5–10 years, regardless of HIV infection [25]. A decrease in mortality from haematologic malignancies, mostly among the youngest population, has been predicted like in other European countries [26].
Pancreas, except lung cancer in women, is the only tumour site where the incidence and mortality will increase simultaneously in the years to come for both genders, especially in the elderly. Although diagnostic improvements may explain part of the increase since the 1980s, the rise in recent years is difficult to interpret. Some risk factors have been associated with this tumour, such as smoking, but the decline in the incidence of lung cancer in men does not seem to support strongly this hypothesis [27]. It is necessary to carry out further studies to determine the role of obesity, diabetes and HBV/HCV infections.
In the same line, we expect an increase in kidney cancer incidence in both genders, similarly with the observed in the US where the age-period-cohort analysis revealed a strong influence from cohort effect because the younger cohorts showed highest incidence than the oldest ones [28]. Some risk factors such as obesity, diabetes and less physical activity have been considered as possible risk factors, but we cannot rule out the diagnostic improvements implemented over the past years that might explain part of this increase.
In Catalonia, incidence and mortality of stomach cancer will continue to decline in two sexes. Moreover, in women, will follow decreasing incidence from cervical and ovary cancers, in the first, mainly related to detection of precancerous lesions and early stage cases [29] and, the second one, to the marked reduction in menopausal hormonal therapy use [30]. It is also expected a decreased incidence of endometrial cancer, while other countries have described a recent rise probably related to obesity [29]. Finally, the increase of prostate cancer incidence predicted is similar that the reported in the highest resource countries and the rising trends are largely attributable to increased detection of latent disease following the widespread availability of PSA test in the late-1980s. However, decreasing mortality (observed and predicted) is mainly attributed to the introduction of curative treatment and, it is still widely discussed, to the early detection by PSA [8].
Some limitations must be noted. The method is based on projecting the most recent trends into the future. Several factors could influence future trends and cannot be easily incorporated into predictive models. However, our assumption is supported by the similar patterns that have been predicted in other countries for the main tumours. Projections also depend on the future population estimates, which affect the future age distribution of the Catalan population. Another limitation might be related to changes in the future population because of migration. Barring a large shift in migration, this should not substantially affect the results of the oldest people, where are diagnosed much of the cases, and counts in this age-group is usually not greatly affected by immigration.
In summary, knowledge of the future number of cancer patients in a country helps to plan the proper development of health services such as diagnostic, therapeutic and palliative procedures. The increase in incident cases of cancer in 2020, primarily tobacco-related tumours (92.6 %) in women and colorectal in men (38.5 %), reinforces the need to strengthen the prevention of smoking and the expansion of the early detection of colorectal cancer across the country despite the devastating economic crisis.
References
Clèries R, Esteban L, Borràs J, Marcos-Gagera R, Freitas A, Carulla M, et al. Time trends of cancer incidence and mortality in Catalonia during 1993–2007. Clin Transl Oncol. 2013. doi:10.1007/s12094-013-1060-y.
Clèries R, Martinez JM, Moreno V, Yasui Y, Ribes J, Borras JM. Predicting the change in breast cancer deaths in Spain by 2019: a Bayesian approach. Epidemiology. 2013;24(3):454–60.
Esteban L, Clèries R, Gálvez J, Pareja L, Escriba JM, Sanz X, et al. REGSTATTOOLS: freeware statistical tools for the analysis of disease population databases used in health and social studies. BMC Public Health. 2013;13(1):201.
Møller H, Fairley L, Coupland V, Okello C, Green M, Forman D, et al. The future burden of cancer in England: incidence and numbers of new patients in 2020. Br J Cancer. 2007;96(9):1484–8.
Valls J, Clèries R, Galvez J, Moreno V, Gispert R, Borràs JM, et al. RiskDiff: a web tool for the analysis of the difference due to risk and demographic factors for incidence or mortality data. BMC Publ Health. 2009;9:473.
Bashir SA, Estève J. Analysing the difference due to risk and demographic factors for incidence or mortality. Int J Epidemiol. 2000;29:878–84.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90.
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49(6):1374–403.
Parkin DM. Tobacco-attributable cancer burden in the UK in 2010. Br J Cancer. 2011;105(Suppl 2):S6–13.
Bray FI, Weiderpass E. Lung cancer mortality trends in 36 European countries: secular trends and birth cohort patterns by sex and region 1970–2007. Int J Cancer. 2010;126:1454–66.
Schiaffino A, Fernandez E, Borrell C, Salto E, Garcia M, Borras JM. Gender and educational differences in smoking initiation rates in Spain from 1948 to 1992. Eur J Public Health. 2003;13(1):56–60.
López-Abente G, Ardanaz E, Torrella-Ramos A, Mateos A, Delgado-Sanz C, Chirlaque MD, et al. Changes in colorectal cancer incidence and mortality trends in Spain. Ann Oncol. 2010;21(Suppl 3):iii76–82.
Serra-Majem L, Ribas-Barba L, Salvador G, Jover L, Raidó B, Ngo J, et al. Trends in energy and nutrient intake and risk of inadequate intakes in Catalonia, Spain (1992–2003). Public Health Nutr. 2007;10(11A):1354–67.
Manchon-Walsh P, Borras JM, Espinas JA, Aliste L. Assessing the effectiveness of a guideline recommendation for pre-operative radiochemotherapy in rectal cancer. Radiother Oncol. 2011;99(2):142–7.
Mitry E, Bouvier AM, Esteve J, Faivre J. Improvement in colorectal cancer survival: a population-based study. Eur J Cancer. 2005;41(15):2297–303.
Bosch FX, Ribes J, Díaz M, Cleries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127(5 Suppl 1):S5–16.
Ribes J, Clèries R, Rubió A, Hernández JM, Mazzara R, Madoz P, et al. Cofactors associated with liver disease mortality in an HBsAg-positive Mediterranean cohort: 20 years of follow-up. Int J Cancer. 2006;119(3):687–94.
Althuis MD, Dozier JD, Anderson WF, Devesa SS, Brinton LA. Global trends in breast cancer incidence and mortality 1973–1997. Int J Epidemiol. 2005;34:405–12.
Parkin DM. Is the recent fall in incidence of post-menopausal breast cancer in UK related to changes in use of hormone replacement therapy? Eur J Cancer. 2009;45:1649–53.
Ravdin PM, Cronin KA, Howlader N, Berg CD, Chlebowski RT, Feuer EJ, et al. The decrease in breast-cancer incidence in 2003 in the United States. N Engl J Med. 2007;356:1670–4.
Canfell K, Banks E, Moa AM, Beral V. Decrease in breast cancer incidence following a rapid fall in use of hormone replacement therapy in Australia. Med J Aust. 2008;188(11):641–44.
Pollán M, Pastor-Barriuso R, Ardanaz E, Argüelles M, Martos C, Galcerán J, et al. Recent changes in breast cancer incidence in Spain, 1980–2004. J Natl Cancer Inst. 2009;101(22):1584–91.
Marcos-Gragera R, Vilar-Coromina N, Galceran J, Borràs J, Clèries R, Ribes J, et al. Rising trends in incidence of cutaneous malignant melanoma and their future projections in Catalonia, Spain: increasing impact or future epidemic? J Eur Acad Dermatol Venereol. 2010;24(9):1083–8.
Erdmann F, Lortet-Tieulent J, Schüz J, Zeeb H, Greinert R, Breitbart EW, et al. International trends in the incidence of malignant melanoma 1953–2008—are recent generations at higher or lower risk? Int J Cancer. 2013;132(2):385–400.
Marcos-Gragera R, Pollan M, Chirlaque MD, Guma J, Sanchez MJ, Garau I, et al. Attenuation of the epidemic increase in non-Hodgkin’s lymphomas in Spain. Ann Oncol. 2010;21(Suppl 3):iii90–6.
Bertuccio P, Bosetti C, Malvezzi M, Levi F, Chatenoud L, Negri E, et al. Trends in mortality from leukemia in Europe: an update to 2009 and a projection to 2012. Int J Cancer. 2013;132(2):427–36.
Boseti C, Bertuccio P, Negri E, La Vecchia C, Zeegers MP, Boffeta P. Pancreatic cancer: overview of descriptive epidemiology. Mol Carcinog. 2012;51:3–13.
Tyson MD, Humphreys MR, Parkers AS, Thiel DD, Joseph RW, Andrews PE, et al. Age-period-cohort analysis of renal cell carcinoma in United States adults. Urology. 2013;82(1):43–7.
Klint A, Tryggvadóttir L, Bray F, Gislum M, Hakulinen T, Storm HH, et al. Trends in the survival of patients diagnosed with cancer in female genital organs in the Nordic countries 1964–2003 followed up to the end of 2006. Actal Oncol. 2010;49(5):632–43.
Yang HP, Anderson WF, Rosenberg PS, Trabert B, Gierach GL, Wentzensen N, et al. Ovarian cancer incidence trends in relation to changing patterns of menopausal hormone therapy use in the United States. J Clin Oncol. 2013;31(17):2146–51.
Acknowledgments
This study was conducted within the framework of the Spanish Cancer Research Network (RTICC) of the Carlos III Health Institute. Grants with reference number RD12/0036/0056; RD06/0020/0095; RD06/020/0089. This study was also conducted within the Research Group-Catalan Cancer Registry (SGR 2009–2013) from the Agència d’Ajuts Universitaris i de Recerca-AGAUR of the Catalan Government.
Conflict of interest
The authors declare that they have no conflict of interest related to the publication of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Ribes, J., Esteban, L., Clèries, R. et al. Cancer incidence and mortality projections up to 2020 in Catalonia by means of Bayesian models. Clin Transl Oncol 16, 714–724 (2014). https://doi.org/10.1007/s12094-013-1140-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-013-1140-z