
Abstract
Background
Developing effective cancer control programmes requires information on the future cancer burden in an ageing population. In our study we predicted the burden of cancer in Catalonia from 2015 to 2025.
Methods
Bayesian age–period–cohort models were used to predict the burden of cancer from 2015 to 2025 using incidence data from the Girona and Tarragona cancer registries and cancer mortality data from the Catalan mortality registry. Using the Bashir–Estève method, we divided the net change in the number of cases between 2015 and 2025 into changes due to population size (S), cancer risk (R) and age (A) distribution.
Results
By 2025, there will be 21,743 new cancer cases in men (40% aged > 74 years) and 17,268 in women (37% aged > 74 years). More than 40% of the new cases will be diagnosed among population aged 74 and older in prostate, colorectal, lung, bladder, pancreatic and stomach cancers in men, and in colorectal, pancreatic and bladder cancers and leukaemia in women. During 2015–2025, the number of new diagnoses will increase by 5.5% in men (A + R + S = 18.1% − 13.3% + 0.7% = 5.5%) and 11.9% in women (A + R + S = 12.4% − 1.1% + 0.6% = 11.9%). Overall cancer mortality rates will continue to decrease during 2015–2025. Lung cancer will be the most lethal cancer among men (N = 2705) and women (N = 1174).
Conclusions
The increase in the number of cancer cases in Catalonia from 2015 to 2025 will mostly affect the elderly, prompting the need for increased collaboration between geriatricians and oncologists.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Predicting the future burden of cancer in a given population is of interest to the institutions responsible for cancer control, as this information is required for planning future services and allocating resources [1].
Changes in exposure to cancer risks and protective factors help determine the future burden of cancer in a population [1], as do changes in population demography. As life expectancy increases, so too does the lifetime risk of developing cancer [2]. Since a large proportion of cancers in Catalonia are diagnosed in older adults [3, 4], population ageing leads to an increase in the absolute number of cancer cases [5]. By 2050, 40% of Spain’s population is set to be aged 60 years or older (Population Ageing and Development 2009: http://www.unpopulation.org), so it is crucial to take into account the effect of ageing when assessing the cancer burden [6]. At the same time, treating elderly patients is challenging due to age-related metabolic changes and comorbidities as well as the lack of guidelines, posing a huge problem for policy makers [7, 8]. These factors increase the demand for healthcare resources, particularly for controlling chronic diseases such as cancer.
This paper quantifies the changes in Catalonia’s cancer burden between 2015 and 2025, with particular focus on the changes associated with population ageing.
Materials and methods
We aggregated cancer incidence data from the Tarragona and Girona population-based cancer registries for the period between 1994 and 2012 and used them to estimate cancer incidence in Catalonia. We obtained cancer mortality data for the period between 1994 and 2013 from the Catalan mortality registry. These cancer incidence and mortality data were stratified by sex and cancer type according to the IXth and Xth edition of the International classification of diseases depending on the period of mortality data (See Classification of cancer cases/deaths section and supplementary Table S1 included in the supplementary material). Incidence and mortality data were arranged in annual intervals in 18 5-year age groups, from 0–4 years to 85 and older.
The Catalan Institute of Statistics (http://www.idescat.cat) provided data on the Catalan population and its age distribution in both sexes for the study period. We used the predicted Catalan population for 2015 and 2025 by 5-year age groups in order to project cancer incidence and mortality by age groups.
Modelling projections
We derived cancer incidence in Catalonia from 1994 to 2012 by applying the age-specific cancer rates in Girona and Tarragona, accounting for 20% of the Catalan population [3], as a whole to the age-specific population counts in Catalonia. We assumed homogeneous rates for the whole autonomous community.
Based on these estimates, Bayesian autoregressive age–period–cohort models [9] were fitted to data from the period between 1994 and 2012, and these models were used to predict incidence and mortality for 2015–2025, assuming Poisson distribution for the number of cases [10]. We describe extensive details of the prior distributions, models used and the model choice in the Supplementary material file. Tables 1, 2, 3, 4 present crude and age-standardised (world population) incidence (ASIR) and mortality rates (ASMR), the number of new cancer cases and deaths in the 35–64 and ≥ 65 age groups and the proportion of cases diagnosed in people aged over 74 years for the years 2015 and 2025.
To assess the percentage change in incident cases between 2015 and 2025, we used the Bashir–Estève method through the web tool RiskDiff [11], which enabled us to split the net change (NC) in the number of cases into changes in demography and changes in cancer risk (R). Since demographic changes can be divided into changes in population size (S) and population structure (ageing: A), the NC can be partitioned into three additive quantities NC = A + R|A + S|A, where changes in risk and population size are conditioned by changes in population structure (R|A and S|A) [6]. Based on this method let \( \frac{{N_{2025} - N_{2015} }}{{N_{2015} }} \times 100 = {\text{NC}}(\% ) \), assuming that the predicted number of cases in 2025, could be partitioned into the number of cases due to changes in risk \( N_{2025}^{R} \) and the number of cases due to changes in population size and age structure, known as changes in demography, \( N_{2025}^{D} \), then \( N_{2025} = N_{2025}^{R} + N_{2025}^{D} \). Note that changes in demography can be obtained through \( N_{2025}^{D} = \sum\nolimits_{i} {\lambda_{i2015} \times P_{i2025} } , \) where λ i2015 is the age-specific incidence rate for a specific cancer that was observed during the period 2015, and P i2025 is the age-specific population at risk predicted for the year 2025. If we let \( P_{2015} = \sum\nolimits_{i} {P_{i2015} } \) and \( P_{2025} = \sum\nolimits_{i} {P_{i2025} } \) as the total population counts in 2015 and 2025, respectively, \( P_{2025} \times \frac{{\sum\nolimits_{i} {N{}_{i2015}} }}{{P_{2015} }} \) is the total expected number of cases in 2025 due to changes in population size. Since \( N{}_{i2015} = \lambda_{i2015} P_{i2015} \) and \( N_{2025}^{R} = N_{2025} - N_{2025}^{D} \) all these quantities are related to changes in population structure, ageing. We carried out a factorial analysis to assess the most likely contribution of risk, ageing and population size to the percentage changes in incidence between periods.
Results
The burden of cancer incidence
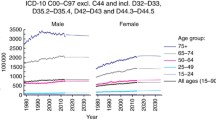
Table 1 presents the projected incidence of the selected cancer types in Catalonia in 2015 and 2025 by age group in both sexes. The total number of new cancer cases in 2015 was predicted to be 36,048 (N = 20,611 in men and N = 15,437 in women). Between 2015 and 2025, we predicted an increase of 5.5% in men (N = 21,743) and 11.9% in women (N = 17,268). Our results show a 4.7% decrease in new diagnoses among men aged between 35 and 64 years over the 10-year study period (N 2015 = 6418; N 2025 = 6129) and a 10.3% increase among those aged 65 and older (N 2015 = 13,755; N 2025 = 15,169). In women, the pattern is slightly different, with an increase predicted in both age groups (35–64 years: 4.9%; > 64 years: 18.1%).
Figure 1 shows the time trend of the overall age-standardised incidence and mortality rates from 1995 to 2025. The age-standardised incidence rate (ASIR) is expected to decrease in men and stabilise in women. When we examine the time trends for each cancer type, we see that there are few exceptions to the general trend (Figures S1 and S2, Supplementary Material). Figure S1 shows a stabilisation of pancreatic cancer and a slight rise in melanoma and testicular cancer in men, while Figure S2 shows an expected rise in lung, kidney and thyroid cancer in women.

Observed and projected rates of cancer incidence (red) and mortality (blue) in Catalonia from1995 to 2025 accounting for all cancer types except non-melanoma skin cancer. ASR age-standardised rate
Table 2 shows the most common cancer types predicted for 2015 and 2025. In men, the three most common types for both years are prostate (N 2015 = 4258; N 2025 = 4652), colorectal (N 2015 = 3508; N 2025 = 4015) and lung (N 2015 = 3150; N 2025 = 2928). Incidence of the latter cancer is expected to decrease by 7% over the 10-year study period. In women, the three most common cancer types in 2015 are breast (N = 4462), colorectal (N = 2493) and corpus uteri (N = 815). In 2025, however, lung cancer (N = 1253) will surpass corpus uteri cancer (N = 840). Our predictions showed that in men, more than 40% of the new cases of prostate, colorectal, lung, bladder, pancreas and stomach cancer will be diagnosed in people aged over 74 years. In women, this age group will account for more than 40% of new cases of colorectal cancer and leukaemia, and more than 50% of new cases of pancreatic and bladder cancer. The change in the burden of these cancers by age group from 1995 to 2025 is depicted in Figure S3 (Supplementary Material). Here, we can see a rising number of new cancer cases among people aged over 64 years, with a large proportion of cases diagnosed in those aged over 74 years. Overall, we predict that between 35 and 40% of new cases diagnosed in 2025 will affect people over 74 years (men: 8681 of 21,743; women: 6330 of 17,268; see Figure S3 d and h).
Comparing cancer incidence between 2015 and 2025: changes in demography and risk in the 35–64 and > 64 age groups
Table 3 shows the percentage difference in the number of cases from 2015 to 2025 due to changes in the risk of developing cancer and changes in population structure (ageing) and size. In men, the 5.5% increase is chiefly attributable to changes in population structure (18.1%) and size (0.7%) since risk of developing cancer is expected to decrease by 13.3%. We observed this pattern for all cancer types except melanoma and testicular cancer, for which an increase in risk is expected (11.1 and 26.1%, respectively). In women, we find a similar pattern, with the decline in gynaecological and breast cancer mainly due to the decrease in risk. In contrast, our results predict a rise in the risk of thyroid (14.2%), kidney (22.2%) and lung cancers (46.6%), with respective net increases in incidence of 16.6, 37.1 and 62.7%, respectively. As with men, population demographics contribute the most (ageing: 12.4%; size: 0.6%) between 2015 and 2025, although to a markedly lesser extent than among men due to the more modest reduction in risk.
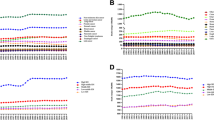
Figure 2 depicts the changes in the number of incident cases from 2015 to 2025 by sex and by age group (35–64 and > 64 years). The supplementary material file presents tables with the corresponding percentage differences in these age groupings (Tables S3–S6). The increase in number of cases in the 35–64 age group is relatively small; the tumour types with the largest increases were prostate cancer in men (49 cases) and breast cancer in women (123 cases) in women. It follows that the overall rise in the number of cases over the 10-year study period is primarily due to the considerable increased number of cases among people aged over 64 years. The increase in population size of this age group (light blue bar) is the main driver of change. Note that changes in population size in a subgroup of older population shows that ageing is a major contributing factor to the burden of the total population. The types of cancer expected to increase by more than 40 cases between 2015 and 2025 are: in men (Fig. 2a, b), colorectal, prostate, bladder, pancreas, lung, non-Hodgkin’s lymphoma, melanoma and kidney; in women (Fig. 2c, d), lung (74% of cases attributable to changes in risk) followed by colorectal, breast, kidney, corpus uteri, pancreas, bladder and thyroid. For these cancer types, the increase is proportional to the change in population size whereas changes in risk may drive the expected increase for kidney and thyroid. To assess these results, a principal components analysis (See Supplementary material) making use of the count variables estimated using these differences has shown that changes in population structure, and, therefore ageing, are the main contributors to the increase in the burden of cancer in Catalonia by 2025 (See supplementary material for details).

Difference from 2015 to 2025 in number of incident cases in Catalonia by cancer type and age group, and proportion of difference due to changes in risk, population structure and population size. Men: a 35–64 years, b ≥ 65 years; Women: c 35–64 years, d ≥ 65 years
Burden of cancer mortality
ASMRs are expected to decrease in men (2015: 129.9 per 105 person-years (py), 2025: 108.2 per 105 py) and level off in women (2015: 64.9 per 105 py, 2025: 61.2 per 105 py) (Table 4; Fig. 1). However, according to our predictions, the number of deaths will increase in men (2015: N = 10,272, 2025: N = 10,691) and in women (2015: N = 6616; 2025: N = 7156) mainly due to the rise in the number of deaths among people aged over 64.
In this age group, the types of cancer for which the greatest increase in number of deaths is expected are lung [Difference (D) = 218 deaths, 11%], pancreas (D = 109 deaths, 28.5%), prostate (D = 95 deaths, 12.4%), kidney (D = 91 deaths, 33%), colorectal (D = 68 deaths, 5.8%) and liver (D = 45, 11.4%) in men, and lung (D = 418; 98.4%), corpus uteri (D = 48; 35%), pancreas (D = 46, 12.7%) and colorectal (D = 44, 5.3%) in women. Our results show a stabilisation followed by a decrease in breast cancer mortality. By 2025, lung cancer is expected to be the leading cause of cancer mortality among women in Catalonia (N = 1174), followed by colorectal cancer (N = 1031) and breast cancer (N = 990).
Discussion
According to the results of our study, from 2015 to 2025, cancer incidence rates in Catalonia will decrease in men and level off in women, mainly due to decreasing incidence rates in the younger population. On the other hand, we predicted a slight increase in the absolute number of new cases between 2015 and 2025, due for the most part to population ageing. Our predictions show that in 2025, 35–40% of new cancer cases will be diagnosed in patients over 74 years of age.
As life expectancy increases, the number of new cancer cases is expected to do the same [2]. However, projections need to focus not only on demographic changes [12], but also on the time lags between changes in risk factors and their effect on the burden of cancer [6] (e.g., smoking prevalence and lung cancer [13]). Our study predicts a significant rise in lung cancer incidence and mortality rates in women in Catalonia, reaching levels similar to those described in the female population of other European countries [14]. Despite this result, the recent stabilisation of the most common cancer types in men (prostate) and women (breast) is the trend with the greatest effect on predicted burden of cancer incidence by 2025.
There are some limitations in the interpretation of our results. The most important limitation is related to the estimation of cancer incidence in Catalonia during the base period. Since cancer incidence data for the whole region are not available, we assumed that the aggregated cancer incidence rates from Girona and Tarragona could be used as an estimate. This assumption may lead to an underestimate of the cancer burden (total number of cases/deaths) for the whole region although it may affect less the time trend effect [10]. Second, the method we used is based on projecting the most recent trends into the future through future population estimates. Changes in the most recent trends as well as in future population counts and age distribution can affect predictions to a considerable degree [1]. Third, we note that the burden of cancer in Catalonia presented here is smaller than that predicted using with the same data in a previous study [4], since the base period was different and the future population counts were 10% higher than currently estimated.
Cancer sites selected
Prostate cancer has been the most widely diagnosed cancer in Spanish men since the mid 1990 s [15] due to the introduction and widespread use of the prostate-specific antigen (PSA) test [3]. Figure S3.1 shows a stable trend in new diagnoses in Catalonia since 2010, while Figure S1 shows a stabilisation followed by a decrease in ASIR. However, we also predicted an increase in the number of cases observed in men aged over 64 years, with 40.7% of new cases expected to be diagnosed in men aged over 74 years by 2025. A similar pattern was previously observed in other countries [16]. Nevertheless, we detected a marked decrease in prostate cancer mortality, possibly as a result of improved treatment and screening [16].
By 2025, colorectal cancer will continue to be the second most common cancer type in both sexes. The predicted increase in crude rates in Catalonia from 2015 to 2025 is mainly due to the ageing of the population (more than 40% of new cases will be diagnosed in people aged over 74 years: 42.4% in men; 49.2% in women). Alcohol and tobacco consumption have been associated with colorectal cancer risk, with studies showing that 70% of new colorectal cancers could be avoided through a healthy lifestyle [17]. The development of screening programmes has also been important for colorectal cancer control. The faecal occult blood test in particular has been shown to reduce cancer incidence and cause-specific mortality by up to 10% through the detection of adenomatous polyps [18]. In 2018, a specific screening programme covering the whole population aged 50–69 years is expected to be fully implemented in Catalonia, and our incidence and mortality predictions may need to be modified depending on the results.
Since 2001, breast cancer incidence in Spain has stabilised [3, 15], with a downturn attributed to routine screening among women aged 45–64 [19]. The slight increase in the number of incident cases from 2015 to 2025 in Catalonia chiefly affects women aged 65 and older. Our mortality predictions show a decrease in the number of breast cancer deaths among women under 65 years, mainly as a result of access to mammography screening and more effective breast cancer management and treatment [6]. As Table 4 shows, lung cancer could soon surpass breast cancer as the most lethal cancer among women in Catalonia.
Lung cancer and other tobacco-related cancers
By 2025, lung cancer will be the third most common cancer in Catalonia and the most lethal cancer in both sexes. The increased burden in women is primarily due to changes in the risk of developing this cancer (46.6%), although the highest increase between 2015 and 2025 is expected to affect women aged 65 years and older (N 2015 = 414; N 2025 = 884; Table 1). The most important risk factor for lung cancer is smoking [20], so the increased prevalence of smoking among Catalan women can explain the rising lung cancer incidence and mortality rates in this population since the late 1990s. This trend stands in contrast to that observed among men in Spain [3, 21, 22], who have increasingly given up the habit since the mid 1980s [21]. It would, therefore, be reasonable to expect a continued rise in lung cancer burden in women [6, 15, 21, 22]. According to our predictions, the male–female ratio of lung cancer incidence and mortality will decrease from fourfold to threefold between 2015 and 2025. This narrowing of the gender gap may also extend to other tobacco-related cancers such as oral cavity, pharyngeal and laryngeal cancer [15]. These types of cancer share common risk factors, such as tobacco and alcohol consumption [20, 23] and, to a lesser extent, human papillomavirus (HPV) infection [24, 25], which is more specifically associated with cancer of the tonsils, base of the tongue and other parts of the oropharynx [24].
A further two types of tobacco-related cancer are urinary bladder (population attributable fraction 50%) [26] and pancreatic cancer (~ 30%) [27]. Our predictions show that in women, more than 55% of new cases in these cancers will be diagnosed in people aged over 74 years.
Other cancer types
Other cancers diagnosed to a large extent in people older than 74 years are stomach cancer (44.2% in men) and leukaemia (44% in women). We also predicted a non-significant difference in the number of cases of corpus uteri, ovary and cervix uteri cancer in women between 2015 and 2025. However, with the parallel introduction of the HPV vaccine and opportunistic screening for HPV in Spain, cervical cancer incidence and mortality are expected to decrease in the coming years [15]. The incidence of non-Hodgkin’s lymphoma has also stabilised and is expected to decrease, possibly due to the decreased incidence of AIDS-related lymphomas among young adults and the efficacy of available treatment in recent years [28].
In Catalonia, skin melanoma incidence may rise slightly among men and level off among women, resulting in similar incidences in both sexes, as observed in other Spanish regions [15]. Our results also show an expected rise in the number of cases of kidney cancer (37.1%) and thyroid cancer (14.2%) in women between 2015 and 2025. Evidence suggests that the increase in kidney cancer may be due to variations in risk factors as well as increased use of imaging techniques, resulting in better detection of small tumours [29], while the stable prevalence of established risk factors for thyroid cancer in the last few decades suggests that rising incidence is associated with improved detection and diagnosis, and largely or totally reflects overdiagnosis of small papillary carcinomas [30]. This could also be the situation in Catalonia.
Conclusion
The increase in the number of new cancer cases from 2015 to 2025 will affect the elderly in particular. These findings can inform planning and resource allocation for future services, having implications for enhancing and expanding existing geriatricians and oncologists’ collaboration [8]. In addition, targeting risk factors such as obesity, physical inactivity and tobacco use may help to reduce cancer risk in younger populations.
References
Bray F, Møller B. Predicting the future burden of cancer. Nat Rev Cancer. 2006;6:63–74. doi:10.1038/nrc1781.
Ahmad AS, Ormiston-Smith N, Sasieni PD. Trends in the lifetime risk of developing cancer in Great Britain: comparison of risk for those born from 1930 to 1960. Br J Cancer. 1930;2015:1–5. doi:10.1038/bjc.2014.606.
Clèries R, Esteban L, Borràs J, Marcos-Gragera R, Freitas A, Carulla M, et al. Time trends of cancer incidence and mortality in Catalonia during 1993–2007. Clin Transl Oncol. 2014;16:18–28. doi:10.1007/s12094-013-1060-y.
Ribes J, Esteban L, Clèries R, Galceran J, Marcos-Gragera R, Gispert R, et al. Cancer incidence and mortality projections up to 2020 in Catalonia by means of Bayesian models. Clin Transl Oncol. 2014;16:714–24. doi:10.1007/s12094-013-1140-z.
Pallis AG, Fortpied C, Wedding U, Van Nes MC, Penninckx B, Ring A, et al. EORTC elderly task force position paper: approach to the older cancer patient. Eur J Cancer. 2010;46:1502–13. doi:10.1016/j.ejca.2010.02.022.
Clèries R, Buxó M, Martínez JM, Espinàs JA, Dyba T, Borràs JM. Contribution of changes in demography and in the risk factors to the predicted pattern of cancer mortality among Spanish women by 2022. Cancer Epidemiol. 2016;40:113–8. doi:10.1016/j.canep.2015.12.002.
Marosi C, Köller M. Challenge of cancer in the elderly. ESMO Open. 2016;. doi:10.1136/esmoopen-2015-000020.
Antonio M, Saldaña J, Carmona-Bayonas A, Navarro V, Tebé C, Nadal M, Formiga F, Salazar R, Borràs JM. Geriatric assessment predicts survival and competing mortality in elderly patients with early colorectal cancer: can it help in adjuvant therapy decision-making? Oncologist. 2017;22(8):934–43. doi:10.1634/theoncologist.2016-0462.
Clèries R, Martínez JM, Moreno V, Yasui Y, Ribes J, Borràs JM. Predicting the change in breast cancer deaths in Spain by 2019: a Bayesian approach. Epidemiology. 2013;24:454–60. doi:10.1097/EDE.0b013e31828b0866.
Clèries R, Ribes J, Buxo M, Ameijide A, Marcos-Gragera R, Galceran J, et al. Bayesian approach to predicting cancer incidence for an area without cancer registration by using cancer incidence data from nearby areas. Stat Med. 2012;31:978–87. doi:10.1002/sim.4463.
Valls J, Clèries R, Gálvez J, Moreno V, Gispert R, Borràs JM, et al. RiskDiff: a web tool for the analysis of the difference due to risk and demographic factors for incidence or mortality data. BMC Public Health. 2009;9:473. doi:10.1186/1471-2458-9-473.
McCormack VA, Boffetta P. Today’s lifestyles, tomorrow’s cancers: trends in lifestyle risk factors for cancer in low- and middle-income countries. Ann Oncol. 2011;22:2349–57. doi:10.1093/annonc/mdq763.
Bilal U, Fernández E, Beltran P, Navas-acien A, Bolumar F, Franco M. Validation of a method for reconstructing historical rates of smoking prevalence. Am J Epidemiol. 2014;179:15–9. doi:10.1093/aje/kwt224.
Malvezzi M, Bertuccio P, Rosso T, Rota M, Levi F, La Vecchia C, et al. European cancer mortality predictions for the year 2015: does lung cancer have the highest death rate in EU women? Ann Oncol. 2015;2015:1–8. doi:10.1093/annonc/mdv001.
Galceran J, Ameijide A, Carulla M, Mateos A, Quirós JR, Rojas D, et al. Cancer incidence in Spain, 2015. Clin Transl Oncol. 2017;. doi:10.1007/s12094-016-1607-9.
Center MM, Jemal A, Lortet-Tieulent J, Ward E, Ferlay J, Brawley O, et al. International variation in prostate cancer incidence and mortality rates. Eur Urol. 2012;61:1079–92. doi:10.1016/j.eururo.2012.02.054.
Binefa G, Rodríguez-Moranta F, Teule A, Medina-Hayas M. Colorectal cancer: from prevention to personalized medicine. World J Gastroenterol. 2014;20:6786–808. doi:10.3748/wjg.v20.i22.6786.
Rossi PG, Vicentini M, Sacchettini C, Di Felice E, Caroli S, Ferrari F, et al. Impact of screening program on incidence of colorectal cancer: a cohort study in Italy. Am J Gastroenterol. 2015;110:1359–66. doi:10.1038/ajg.2015.240.
Pollán M, Pastor-Barriuso R, Ardanaz E, Argüelles M, Martos C, Galcerán J, et al. Recent changes in breast cancer incidence in Spain, 1980–2004. J Natl Cancer Inst. 2009;101:1584–91. doi:10.1093/jnci/djp358.
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JWW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49:1374–403. doi:10.1016/j.ejca.2012.12.027.
Bilal U, Beltran P, Fernández E, Navas-Ancien A, Bolumar F, Franco M. Gender equality and smoking: a theory-driven approach to smoking gender differences in Spain. Tob Control. 2016;25:295–300. doi:10.1136/tobaccocontrol.
López-Campos JL, Ruiz-Ramos M, Fernandez E, Soriano JB. Recent lung cancer mortality trends in Europe. Eur J Cancer Prev. 2017;. doi:10.1097/CEJ.0000000000000354 In Press.
Hashibe M, Brennan P, Chuang S-C, Boccia S, Castellsague X, Chen C, et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol Biomark Prev. 2009;18:541–50. doi:10.1158/1055-9965.EPI-08-0347.
Syrjänen S. The role of human papillomavirus infection in head and neck cancers. Ann Oncol. 2010;21:243–5. doi:10.1093/annonc/mdq454.
Torrente MC, Rodrigo JP, Haigentz MJ, Dikkers FG, Rinaldo A, Takes RP, et al. Human papillomavirus infections in laryngeal cancer. Head Neck. 2011;33:581–6. doi:10.1002/hed.21421.
Murta-nascimento C, Schmitz-Dräger BJ, Zeegers J, Schmitz-dräger MP, Steineck G, Kogevinas M, et al. Epidemiology of urinary bladder cancer: from tumor development to patient’ s death. World J Urol. 2007;25:285–95. doi:10.1007/s00345-007-0168-5.
Bosetti C, Lucenteforte E, Silverman DT, Petersen G, Bracci PM, Ji BT, et al. Cigarette smoking and pancreatic cancer: an analysis from the International Pancreatic Cancer Case–Control Consortium (Panc4). Ann Oncol. 2012;23:1880–8. doi:10.1093/annonc/mdr541.
Marcos-Gragera R, Pollán M, Chirlaque MD, Gumà J, Sanchez MJ, Garau I, et al. Attenuation of the epidemic increase in non-Hodgkin’s lymphomas in Spain. Ann Oncol 2010; 21. doi:10.1093/annonc/mdq088.
Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Rising incidence of small renal masses: a need to reassess treatment effect. J Natl Cancer Inst. 2006;98:1331–4. doi:10.1093/jnci/djj362.
La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer. 2015;136:2187–95. doi:10.1002/ijc.29251.
Acknowledgements
This work was supported by the Agència d’Avaluació d’Universitats i Recerca (2014SGR0635), and partially supported by Instituto de Salud Carlos III through the Project PI14/01041, co-funded by European Regional Development fund/European Social fund: “investing in your future”.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The funders had no role in the design of the study, the collection, analysis, or interpretation of the data, the writing of the manuscript, or the decision to submit the manuscript for publication. The authors state that there are no conflicts of interest concerning this study.
Research involving human participants and/or animals
This article does not contain any studies with human participants or animals performed by any of the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Clèries, R., Ameijide, A., Marcos-Gragera, R. et al. Predicting the cancer burden in Catalonia between 2015 and 2025: the challenge of cancer management in the elderly. Clin Transl Oncol 20, 647–657 (2018). https://doi.org/10.1007/s12094-017-1764-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-017-1764-5