
Abstract
Background
Sarcopenia, the age-related loss of muscle mass and function, is closely associated and frequently concomitant with non-alcoholic fatty liver disease (NAFLD). We aimed to investigate the clinical features of the sarcopenic NAFLD patients from middle-aged and older people.
Methods
A total of 1305 patients with NAFLD from the Shanghai Changfeng Study were included for analysis. Sarcopenia was diagnosed based on the height-adjusted appendicular skeletal muscle mass (ASM/height2). We comprehensively analyzed the metabolic phenotype, carotid artery condition, liver fibrosis score, and serum metabolomic profile of each participant.
Results
Among the middle-aged and older population, 68.1% of patients with sarcopenia and NAFLD were lean. Sarcopenia was independently associated with increased risk of carotid plaque (OR, 2.22; 95%CI 1.23–4.02) and liver fibrosis (OR, 2.07; 95%CI 1.24–3.44), and the sarcopenic lean NAFLD patients were characterized by a higher risk of carotid plaque (p = 0.008) and liver fibrosis (p = 0.001) than the non-sarcopenic lean NAFLD patients, despite their lower BMI and similar prevalence of metabolic syndrome and diabetes. Further serum metabolomic examination indicated that the sarcopenic lean NAFLD patients presented a distinct metabolomic profile prone to carotid plaque and liver fibrosis, with upregulated serum valine, N-acetylneuraminyl-glycoproteins, lactic acid, small LDL triglycerides and VLDL5 components, and reduced components of HDL4. A sarcopenic characterization score based on above metabolites was established and could also predict increased risk of carotid plaque and liver fibrosis.
Conclusion
The presence of sarcopenia identifies a special subgroup of lean NAFLD with increased risk of cardiovascular disease and liver fibrosis clinically.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is currently the most common liver disease worldwide, with a global prevalence of approximately 25% [1]. Usually, NAFLD arises in the context of obesity and its related metabolic diseases [2]. As the prevalence of obesity doubles during the last 30 years in the US, the prevalence of NAFLD also increases from 20 to 32% [3], and is estimated to continuously increase by 18.3% in 2030 [4].
Population aging is another important risk factor driving the rapidly increasing trend of NAFLD. The prevalence of NAFLD is lower than 30% in the Asian adults aged less than 40 years, and higher than 50% in those older than 60 years [5]. According to the National Health and Nutrition Examination Survey III (NHANES III) database, the prevalence of NAFLD doubles in adults aged over 45 years in the United States [6]. Although body weight starts to fall after the age of 50, the proportion of NAFLD with normal weight, also called “lean NAFLD”, is remarkably increased in the older patients (40.9% if ≥ 65 vs. 24.2% if < 65 years) [7]. As the population ages globally, the prevalence of lean NAFLD has also increased from 5.6% before 2000 to 12.6% after 2011 [8]. Usually, lean NAFLD is associated with a more favorable metabolic and histological feature compared with non-lean NAFLD [9]. However, studies also reported that patients with lean NAFLD had a higher all-cause and cardiovascular mortality, most of whom died over the age of 55 [10]. Therefore, NAFLD in the older population, with a high proportion of lean people, may have some special pathophysiological features.
Sarcopenia is a progressive skeletal muscle disorder characterized by the accelerated loss of muscle mass and it is a common feature of human aging. Previous studies from our study population [11] and the Korean and European populations [12,13,14] have found that sarcopenia was associated with NAFLD, non-alcoholic steatohepatitis (NASH) and liver fibrosis, independent of insulin resistance and obesity. Thus, it is highly possible that the presence of sarcopenia may influence the clinical features of NAFLD in the middle-aged and older population.
In the current study, we analyzed the hepatic and metabolic features of the NAFLD patients aged over 45 divided by adiposity and sarcopenia status from Shanghai Changfeng Study. Inspired from our previous study on the outstanding changes in the metabolomic profiles in two genes (PNPLA3 and TM6SF2) associated NAFLD [15], we further investigated the metabolomic characterization of the sarcopenic NAFLD patients and analyzed its correlation with their clinical features.
Patients and methods
Patients selection
A total of 6595 participants aged over 45 years were enrolled from the Shanghai Changfeng Study, a community-based prospective cohort study of multiple chronic diseases in a middle-aged and older Chinese population, from June 2009 to December 2012. The inclusion criteria of participants were (1) aged over 45 years old and (2) lived in the Shanghai Changfeng community for at least 5 years. As shown in the participant flow diagram (Figure S1), 969 participants enrolled from June 2009 to May 2010 had no schedule for liver ultrasound examination and were excluded from analysis. Among the remaining 5626 participants, 2669 participants without fatty liver were excluded and 1652 participants with fatty liver were excluded due to excessive alcohol consumption (N = 653), self-reported or physician-recorded previous history of known liver disease, including hepatitis B (N = 163) and hepatitis C (N = 3), and missing data of liver ultrasound examination (N = 515), body composition measured by dual-energy X-ray absorptiometry (DXA) (N = 275) and serum biochemical or metabolomic data (N = 43). Eventually, a total of 1305 NAFLD patients were included for analysis.
Anthropometric and biochemical measurements
The past history of diseases and medication use of each participant was collected in a face-to-face interview with a trained investigator using a standardized questionnaire. Height and weight were measured without shoes or outer clothing. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of height in meters (kg/m2). Resting systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured using an electronic blood pressure monitor (OMRON Model HEM-752 FUZZY, Omron Co., Dalian, China). Serum biochemical parameters, including serum alanine transaminase (ALT), aspartate transaminase (AST), fasting plasma glucose (FPG), oral glucose tolerance test (OGTT) 2-h post-load plasma glucose (PPG), total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL) cholesterol, were measured after a 12 h overnight fasting using an automated bio-analyzer (HITACHI 7600, Tokyo, Japan). Low-density lipoprotein (LDL) cholesterol was calculated using the Friedewald equation. Fasting insulin was measured using an electrochemiluminescence immunoassay. Homeostasis model assessment for insulin resistance (HOMA-IR) was calculated as FPG (mmol/L) × fasting insulin (mU/L)/22.5.
Liver and carotid artery ultrasonography
The hepatic and carotid artery ultrasound examinations were performed using a GE LOGIQ P5 machine (GE Healthcare, Milwaukee, USA). Liver fat content (LFC) was quantified using an ultrasound quantitative method, and hepatic steatosis was diagnosed by liver ultrasonography [16]. Carotid plaque was defined as the presence of focal wall thickening at least 50% greater than that of the surrounding vessel wall or as a focal region with a carotid intima-media thickness greater than 1.5 mm that protrudes into the lumen that is distinct from the adjacent boundary [17].
DXA measurements of body composition
Lean mass, fat mass and bone mass at the whole body, trunk, and limbs sites, as well as bone mineral density (BMD) (g/cm2) at the lumbar spine (L1–L4) and total hips were measured by a single, trained technician using dual-energy X-ray absorptiometry (Lunar iDXA, GE Healthcare). The appendicular skeletal muscle mass (ASM) in kilograms, calculated as the sum of the lean mass in the bilateral upper and lower limbs, was divided by the square of height in meters and expressed as ASM/height2.
Serum metabolomic measurements by 1H nuclear magnetic resonance spectroscopy (1H-NMR)
The 1H-NMR analysis was conducted on a 600 MHz NMR spectrometer equipped with a BBI probe (Bruker Biospin, Germany) as reported previously [18]. The procedure of metabolomic examination was detailed previously [19]. Among the 178 metabolites initially measured, the metabolites with a missing rate greater than 20% were excluded, and the remaining missing values were filled with half of the minimum value for that metabolite. Ultimately, a total of 158 quantitative parameters were entered into analysis, including 130 lipoprotein parameters, 6 ratio parameters for saturated, unsaturated, monounsaturated, and polyunsaturated fatty acids, 22 small metabolites such as amino acids, ketone bodies, glucose, carboxylic acids and acute-phase N-acetyl-glycoproteins (NAG). The units of the metabolites were mg/dL for the lipoprotein parameters and mmol/L for other metabolomic parameters.
Causes of mortality
The vital status of all participants was determined according to registration data from the Shanghai Center for Disease Control. The causes of death were coded according to the 10th Revision of International Classification of Diseases (ICD-10). The main endpoints during the follow-up included deaths due to cardiovascular diseases (ICD-10 codes I00-I99), liver disease (ICD-10 codes C22.0, C22.2–C22.9, and K70–K76), and other causes, as detailed previously [19].
Definitions
A BMI over 23 kg/m2 and 27 kg/m2 were diagnosed as overweight and obesity according to the optimal cutoff for Asians. Metabolic syndrome was defined if three or more of the following five components are met: (1) waist circumference ≥ 90 cm for male and ≥ 80 cm for female; (2) TG ≥ 1.7 mmol/L or receiving drug treatment for elevated triglycerides; (3) HDL cholesterol levels < 1.03 mmol/L in male or < 1.29 mmol/L in female or receiving drug treatment for reduced HDL cholesterol; (4) SBP/ DBP ≥ 130/85 mmHg or antihypertensive drug treatment in a patient with a history of hypertension; (5) FPG ≥ 5.6 mmol/L, or drug treatment for elevated glucose; according to the updated NCEP ATPIII criteria. Central obesity was defined as waist circumference ≥ 90 cm for male and ≥ 80 cm for female. Diabetes was diagnosed if FPG levels ≥ 7.0 mmol/L or OGTT 2-h PPG levels ≥ 11.1 mmol/L or self-reported history of diabetes or antidiabetic medication use according to the 1999 WHO criteria. Hypertriglyceridemia was diagnosed if serum TG ≥ 1.7 mmol/L, and hypertension was diagnosed as SBP ≥ 140 mmHg or DBP ≥ 90 mmHg or antihypertensive drug treatment. Fatty liver was diagnosed when LFC by ultrasonography exceeded the cut-off value of 9.15% [16]. The fibrosis 4 score (FIB-4) was used to evaluate liver fibrosis grades: FIB-4 = age (years) × AST (U/L)/[platelets (109/L) × √ALT (U/L)]. All the NAFLD patients were stratified as low-risk (FIB-4 < 1.30), intermediate-risk (FIB-4 1.30–2.67) and high-risk (FIB-4 ≥ 2.67) of advanced liver fibrosis, based on the values of FIB-4 [20]. Since the data of young reference group were not available, the sex-specific lower quintiles of ASM/height2 of all participants from the Shanghai Changfeng Study (6.88 kg/m2 in male and 5.67 kg/m2 in female) were used as the cutoff values for diagnosis of sarcopenia according to the consensus of Asian Working Group for Sarcopenia (AWGS) [21]. The cutoff values of 7.0 kg/m2 in male and 5.4 kg/m2 in female, recommended in previous Asian studies [21], were also used to test the stability of the study results under different definitions of sarcopenia.
Statistical analysis
All statistical analyses were performed using the R software version 3.6.2 and SPSS software version 15.0. The continuous parameters with normal distribution are presented as the means ± SD and skewed parameters are presented as the median with the interquartile range (25–75%) given in parentheses. The patients with NAFLD were divided into the following four groups according to their adiposity and sarcopenia status: lean NAFLD (N = 85), sarcopenic lean NAFLD (N = 177), overweight/obese NAFLD (N = 960) and sarcopenic overweight/obese NAFLD (N = 83). All the skewed parameters were log transformed to normality or approximately normality before analysis. The continuous variables were compared using the one-way analysis of variance (ANOVA) and the categorical variables using the chi-square test. The prevalence of metabolic syndrome and its constituent disorders (central obesity, diabetes, hypertriglyceridemia and hypertension), carotid plaque and liver fibrosis were compared using multivariate logistic or ordinal regression models and the all-cause and cause-specific mortalities were compared using Cox regression models among the lean, sarcopenic lean, overweight/obese and sarcopenic overweight/obese NAFLD patients, after adjustment for age and sex. The standardized z-score of each component of their metabolomic profiles was compared using generalized linear models after adjustment for age and sex and false discovery rate (FDR) correction. We also analyzed the association of sarcopenia, overweight/obesity as well as each 1H-NMR-based metabolite with the risk of carotid plaque, liver fibrosis, diabetes, metabolic syndrome and hypertriglyceridemia using logistic or ordinal regression models, with multiple adjustment and false discovery rate (FDR) correction. The interactive effect of adiposity and sarcopenia on liver fibrosis and metabolic diseases was investigated by entering their interactive item into the statistical models.
A sarcopenic characterization score was calculated on the basis of the basic anthropometric parameters and metabolites associated with sarcopenia in all patients using a forward stepwise logistic regression model. The internal cross-validation of the sarcopenic characterization score was tested by a tenfold cross-validation technique and repeated 200 times with the R program. The receiver operating characteristic curve analyses were used to evaluate the diagnostic performance of the sarcopenic characterization score and the diagnostic cutoff of the sarcopenic characterization score was obtained from the maximal Youden index. The risks of carotid plaque and liver fibrosis were further compared among the NAFLD patients divided by the sarcopenic characterization score and adiposity status.
All statistical analyses were two-sided and p < 0.05 was considered statistically significant unless otherwise stated.
Results
Baseline characteristics
Among the 3974 participants aged over 45 years from the Shanghai Changfeng Study, 1305 (32.8%) had NAFLD. Sarcopenia can be diagnosed in 260 NAFLD patients, including 177 (68.1%) sarcopenic lean and 83 (31.9%) sarcopenic overweight/obese patients (Fig. 1A). As shown in Table 1, the sarcopenic NAFLD patients were older and had lower BMI and lean mass, but their fat mass and bone mass were similar to the non-sarcopenic patients, regardless of their adiposity status. The overweight/obese NAFLD patients had higher levels of BMI, waist circumference, fat mass, SBP, DBP, FPG, PPG, HbA1c, HOMA-IR, serum TG and liver enzymes and lower levels of HDL cholesterol than the lean NAFLD patients as expected, but all the common clinical metabolic parameters had no significant difference between the sarcopenic and non-sarcopenic NAFLD patients either in the lean or overweight/obese status.

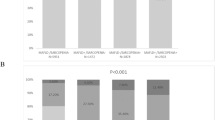
Clinical features of the subgroups of NAFLD patients divided by adiposity and sarcopenia status. a The prevalence of NAFLD and proportion of sarcopenic and non-sarcopenic lean and overweight/obese NAFLD patients. The prevalence of b metabolic syndrome, c carotid plaque, d intermediate- and high-risk advanced liver fibrosis, as well as e all-cause mortality and f cardiovascular mortality were compared among the lean, sarcopenic lean, overweight/obese and sarcopenic overweight/obese NAFLD patients. Level of significance: p < 0.05 (multivariate logistic/ordinal/Cox regression models adjusting for age and sex). *Sarcopenia was diagnosed by the lower quintile of height-adjusted appendicular skeletal muscle mass
Clinical features of the subgroups of NAFLD divided by adiposity and sarcopenia status
We further investigated the hepatic and metabolic complications of the sarcopenic NAFLD patients. As shown in Fig. 1 and Figure S2, the prevalence of metabolic syndrome (Fig. 1B), central obesity (Figure S2A), diabetes (Figure S2B), hypertriglyceridemia (Figure S2C) and hypertension (Figure S2D) was similar between the sarcopenic and non-sarcopenic lean NAFLD patients (all p > 0.05), but the risk of carotid plaque (p = 0.008, Fig. 1C) and liver fibrosis (p = 0.001, Fig. 1D) was significantly higher in the sarcopenic lean NAFLD patients. In contrast, the overweight/obese NAFLD patients had increased risk of all metabolic diseases, including metabolic syndrome (Fig. 1B), central obesity (Figure S2A), diabetes (Figure S2B), hypertriglyceridemia (Figure S2C), hypertension (Figure S2D) and carotid plaque (Fig. 1C) (all p < 0.05). However, the presence of sarcopenia was not associated with additional risk of metabolic disorders or liver fibrosis in the overweight/obese NAFLD patients (Fig. 1B–D). Since different definitions of sarcopenia existed currently, to test the stability of the study results under different definitions of sarcopenia, the cutoffs of ASM/height2 used in previous Asian studies were also used to define sarcopenia in our current study. As shown in Figure S3, the presence of sarcopenia diagnosed by another criterion recommended by AWGS was also associated with increased risk of carotid plaque (Figure S3E) and liver fibrosis (Figure S3F) under preserved metabolic status (Figure S3B-D) in the lean NAFLD patients. After a median of 5.2 year follow-up, the cardiovascular mortality was significantly increased in the groups with either sarcopenia or overweight/obesity or both (Fig. 1F), although the all-cause mortality and liver-specific mortality showed no difference among the lean and overweight/obese patients with and without sarcopenia (Fig. 1E and Figure S4).
Sarcopenia and adiposity differentially influenced the hepatic and metabolic complications of NAFLD
The special phenotype of sarcopenic NAFLD patients indicated that sarcopenia might have unique effects on the hepatic and metabolic complications that differ from the conventional metabolic risk factors such as obesity. As shown in Fig. 2, after adjustment for age and sex, overweight/obesity status was independently associated with increased risk of diabetes (odds ratio [OR], 3.35; 95%CI 1.70–6.59), metabolic syndrome (OR, 3.82; 95%CI 2.38–6.11), and hypertriglyceridemia (OR, 2.26; 95%CI 1.42–3.57) as expected, while the presence of sarcopenia was associated with increased risk of carotid plaque (OR, 2.22; 95%CI 1.23–4.02) and liver fibrosis (OR, 2.07; 95%CI 1.24–3.44) but not diabetes or metabolic syndrome. No interaction between overweight/obesity status and sarcopenia was found, except for an interactive effect of sarcopenia and overweight/obesity on the risk of carotid plaque (Pinteraction = 0.044). The association between sarcopenia and carotid plaque remained significant even after further adjustment of the risk of liver fibrosis (OR, 1.97; 95%CI 1.08–3.59) (Figure S5). Since the presence of sarcopenia had no significant association with the components of metabolic syndrome in the NAFLD patients, the correlation of sarcopenia with carotid plaque and liver fibrosis seemed to be mediated by other circulating substances independent of the effect of conventional metabolic risk factors.

Associations of adiposity and sarcopenia with risks of liver fibrosis and metabolic diseases in NAFLD patients. The odds ratios for liver fibrosis, diabetes, metabolic syndrome, hypertriglyceridemia and carotid plaque related to the presence of adiposity or sarcopenia were calculated. Level of significance: p < 0.05 (multivariate logistic/ordinal regression models adjusting for age and sex, and the interactive effect of adiposity and sarcopenia was investigated by entering their interactive item into the statistical models)
Metabolomic profiles of the subgroups of NAFLD divided by adiposity and sarcopenia status
The use of metabolomic examination has enabled us to identify the differences in baseline concentrations of large VLDL (VLDL1) particles in PNPLA3 gene variants carriers with NAFLD, which well explained the protective effect of PNPLA3 rs738409 C > G variant against cardiovascular disease [19]. Inspired from our previous study on the metabolomic profiles in two genes (PNPLA3 and TM6SF2) associated with NAFLD [15], serum metabolomic profiles were further analyzed in NAFLD patients divided by adiposity and sarcopenia status in our current study. As shown in Fig. 3, the overweight/obese NAFLD was featured with a metabolomic profile prone to metabolic and cardiovascular disease, including increased serum VLDL2-VLDL4 components, reduced HDL2-HDL4 components and upregulated levels of several essential amino acids (valine, leucine, isoleucine, phenylalanine and tyrosine), inflammatory metabolites (N-acetylglucosamine/galactosamine-glycoproteins [NAG1]) (all p < 0.05 after FDR correction), no matter whether it is concomitant with sarcopenia or not. Intriguingly, the sarcopenic lean NAFLD patients presented a unique metabolomic profile distinct from the non-sarcopenic lean NAFLD and the overweight/obese NAFLD. Compared with the non-sarcopenic lean NAFLD patients, the sarcopenic lean NAFLD patients had a characterized lipoprotein profile with increased VLDL5 components, TG in LDL4 and LDL5, and reduced cholesterol esters (CE), cholesterol, free cholesterol (FC) and apolipoprotein A2 (ApoA2) in HDL4. Moreover, serum valine and phenylalanine, ketone bodies (β-hydroxybutyric acid and acetoacetate), lactic acid and the inflammation biomarker N-acetylneuraminyl-glycoproteins (NAG2) were significantly elevated, and the serum creatinine was reduced in the sarcopenic lean NAFLD patients (all p < 0.05 after FDR correction) (Fig. 3).

Serum metabolomic profile of the subgroups of NAFLD patients divided by adiposity and sarcopenia status. All components of the metabolomic profile were standardized to their z scores before analysis. Level of significance: p < 0.05 after FDR correction (generalized linear models adjusting for age and sex). *p < 0.05 compared with non-sarcopenic lean NAFLD patients
The metabolomic characterization of sarcopenic lean NAFLD was correlated with the risk of liver fibrosis and carotid plaque
The associations of all metabolomic components with liver fibrosis and carotid plaque were analyzed as shown in Tables S1&2. Among the differentially expressed serum metabolites in the sarcopenic lean NAFLD patients, the reduced CE, FC, CH and ApoA2 in HDL4, and increased branched-chain amino acid valine were significantly associated with increased risk of liver fibrosis (Fig. 4A), while the increased TG in LDL4 and LDL5, valine, lactic acid and NAG2 were associated with increased carotid plaque (Fig. 4B), after adjustment for age, sex and BMI (all p < 0.05).

Sarcopenia-related metabolomic profile related to the risk of liver fibrosis and carotid plaque. The odds ratios and 95%CIs for a liver fibrosis and (carotid plaque per SD metabolomic component were estimated. Level of significance: p < 0.05 after FDR correction (multivariate logistic models adjusting for age, sex and BMI)
In a multivariate logistic regression model, which included all common anthropometric and metabolomic parameters significantly associated with the presence of sarcopenia in all participants (Fig. 3), we identified the variables that were independently associated with sarcopenia, and obtained the sarcopenic characterization score by applying forward multivariate regression analyses as follows (Table S3).
Sarcopenic characterization score = eγ/(1 + eγ).
Where γ = 15.625 + 0.042 × Age (year).
+ 0.469 × Sex (Male = 1, Female = 0).
−0.824 × BMI (kg/m2).
+ 3.088 × Valine (mmol/L).
+ 0.173 × VLDL5-CE (mg/dL).
−11.658 × Creatinine (mmol/L).
The area under the ROC curve (AUROC) of sarcopenic characterization score for diagnosis of sarcopenia was 0.92 (0.86–0.97) in NAFLD patients after 200 times internal cross-validation by a tenfold cross-validation technique (Fig. 5A). The optimal cutoff was 0.365 with sensitivity of 83% and specificity of 82%. We further divided all the NAFLD patients into two groups according to the cutoff of the sarcopenic characterization score. Consistent with the clinical features of the sarcopenic NAFLD patients, the prevalence of liver fibrosis and carotid plaque was significantly higher in the groups with either high sarcopenic characterization score or overweight/obesity, or both, as shown in Fig. 5B, C.

Associations of sarcopenic characterization score and adiposity with risks of liver fibrosis and metabolic diseases in NAFLD patients a A sarcopenic characterization score was established to identify sarcopenia in NAFLD patients (AUROC: 0.92; 95% CI 0.86–0.97). The prevalence of b intermediate- and high-risk advanced liver fibrosis and c carotid plaque were compared among the NAFLD patients divided by sarcopenic characterization score and adiposity status. Level of significance: p < 0.05 (multivariate logistic/ordinal regression models adjusting for age and sex)
Discussion
Both sarcopenia and NAFLD are great health threats in the aging society. Previous studies have demonstrated that the presence of sarcopenia is associated with NAFLD, NASH and liver fibrosis [11,12,13,14]. As the skeletal muscle mass decreases, the prevalence of NAFLD is increasing in the aging populations in the absence of obesity. In the current study among Chinese adults, we found that sarcopenic lean NAFLD accounted for 13.6% of NAFLD patients aged over 45 years. Different from the overweight/obese NAFLD patients who had increased risk of all metabolic diseases and carotid plaque, the sarcopenic lean NAFLD patients were characterized with increased risk of atherosclerotic carotid plaque and liver fibrosis, with relatively good metabolic status, and sarcopenia and adiposity jointly contributed to the increased risk of cardiovascular mortality. Further metabolomic examination revealed that the sarcopenic lean NAFLD patients were characterized by a metabolomic profile distinct from the non-sarcopenic lean NAFLD and the overweight/obese NAFLD. The reduced serum components of HDL4 and elevated LDL4 and LDL5 triglycerides, branched-chain amino acid valine, glycolysis product lactic acid and acute inflammation biomarker NAG2 in the sarcopenic lean NAFLD patients might be responsible for their increased risk of atherosclerotic carotid plaque and liver fibrosis.
Sarcopenia, an age-dependent progressive skeletal muscle disorder involving the loss of muscle mass and function, is a common age-related disease in the middle-aged and older population [22]. Previous studies found the prevalence of sarcopenia in older Chinese were 12.3% in male and 7.6% female [21]. Consistently, the male participants were more likely to suffer from sarcopenia in our results, and the age-related decrease in testosterone, a major hormone regulating skeletal muscle anabolism, might correlate with the accelerated loss of muscle mass in men. Caused by the imbalance between muscle protein anabolic and catabolic pathways, sarcopenia has been recognized to be associated with insulin resistance, increased systemic inflammation, altered myokine secretion and deficiency of trace elements and vitamins [23]. In our current study, a coexistence of NAFLD and sarcopenia was frequently observed in the lean middle-aged and older adults. The crosstalk between the skeletal muscle and liver provides the possibility that sarcopenia and NAFLD can mutually contribute to the development of each other. On one hand, sarcopenia increases hepatic lipogenesis and inhibits fatty acid beta-oxidation by causing insulin resistance and decreasing the secretion of hepatoprotective myokines (interleukin-6, irisin, et al.). On the other hand, liver steatosis promotes skeletal muscle loss through the effect of hepatic insulin resistance and altered serum levels of several hepatokines (fibroblast growth factor-21, leukocyte cell-derived chemotaxin 2, et al.) [24]. In our current study, we found the sarcopenic patients developed NAFLD at lower level of BMI (Table 1), and consistent with previous studies [13, 14], sarcopenia specifically correlated with the risk of liver fibrosis independent of adiposity and insulin resistance, especially in the lean NAFLD patients [14]. The mechanism underlying the association between sarcopenia and liver fibrosis is still unclear, and reduction of circulating hepatoprotective myokines, such as irisin [24], might contribute to the progression of sarcopenic NAFLD, according to previous studies. The metabolomic analysis in our study further indicated that reduced serum HDL4 components and increased branched-chain amino acid valine in the sarcopenic lean NAFLD patients was associated with liver fibrosis. The HDL4 subfraction (1.125–1.21 g/ml) is intestine-derived HDL that functions to prevent lipopolysaccharide binding to and activation of liver macrophages [25], and the reduction of HDL4 components in the sarcopenic lean NAFLD patients might impair individual protective ability against liver fibrosis. Serum valine was found to be associated with advanced liver fibrosis in patients with hepatitis B viral infection previously [26], and reducing valine rapidly restores liver metabolic health in diet-induced obese mice [27]. However, the mechanism underlying the effect of valine on liver fibrosis is still to be elucidated.
Intriguingly, the sarcopenic lean NAFLD had significantly higher risk of carotid plaque than the non-sarcopenic lean NAFLD patients, despite their similar metabolic status and prevalence of diabetes and metabolic syndrome. Previous studies from our and other groups have found that the presence of sarcopenia was associated with increased risk of carotid atherosclerosis [28], and coronary artery disease [29]. Further prospective studies showed that sarcopenia was associated with increased risk of cardiovascular mortality, regardless of adiposity status [30]. The mechanism underlying the deleterious effect of sarcopenia on carotid atherosclerosis has not been fully understood, and systemic inflammation is thought to be causal for the development of cardiovascular disease in sarcopenia. In our current study, 1H-NMR-based metabolomic examination showed that in the lean NAFLD patients with sarcopenia, the TGs in the deleterious small dense LDLs (LDL4 and LDL5), valine, lactic acid and NAG2 were significantly elevated. Small dense LDLs are well recognized risk factors of cardiovascular disease. Recent studies also indicated that branched-chain amino acid, including valine, promotes thrombosis risk [31]. The serum lactic acid and NAG2 might reflect human anaerobic respiration and inflammation status. All the metabolites could correlate with the development of atherosclerotic carotid plaque clinically.
In our current study, a sarcopenic characterization score was established to identify potential sarcopenic patients. The sarcopenic characterization score was composed of age, sex, BMI and three metabolites (VLDL5-CE, valine and creatinine). It has been well recognized that age, sex and BMI were risk factors of sarcopenia [22]. Creatinine is directly produced by the breakdown of creatine in muscle, and branched-chain amino acids were associated with increased risk of sarcopenia in older Chinese adults according to several previous studies [32]. VLDL5 is also called small VLDL, and it has been proven to play a crucial role in residual cardiovascular risk [33], and negatively associated with skeletal muscle mass [34]. Thus, the metabolomic profile could well reflect the metabolic feature of sarcopenia and be used to identify sarcopenic patients in middle-aged and elderly population.
The clinical features of sarcopenic lean NAFLD were not simply a combination of lean NAFLD and sarcopenia. Sarcopenia was usually associated with insulin resistance and risks of diabetes, metabolic syndrome and visceral obesity, in addition to its association with cardiovascular disease and mortality. However, in the sarcopenic lean NAFLD patients, NAFLD developed at lower levels of BMI and almost normal metabolic status, and instead of the conventional risk factors, their unique metabolome might contribute to the increased risk of liver fibrosis and cardiovascular disease as shown in our current study.
Several limitations are associated with our current study. First, the information of physical activity, handgrip strength or gait speed and liver histological fibrosis was not available. Thus, our study results only represented the relationship of sarcopenia defined by skeletal muscle mass with liver fibrosis defined by non-invasive prediction score in the NAFLD patients. Further studies focusing on the relationship of muscle function and mass with NAFLD-related liver histological fibrosis and metabolic complications are still needed. Second, we excluded the patients with other known chronic liver diseases based on the self-reported or physician-recorded history of hepatitis, medication use and other chronic liver diseases, so a few patients with positive serologic markers for hepatitis B or C virus but no previous histology of hepatitis were not completely excluded from our current study. Third, the proportion of sarcopenic overweight/obese NAFLD patients was very low (6.3%) and might preclude analysis of the association of sarcopenia with liver fibrosis and metabolic diseases in the overweight/obese NAFLD patients. Finally, this study investigated the features of sarcopenic lean NAFLD in a Chinese population, and further studies were required to expand the conclusion to participants from different ethnicities.
Conclusion
Both sarcopenia and NAFLD are important age-related metabolic diseases. NAFLD in the middle-aged and older population was characterized by a high proportion of sarcopenic lean patients. These sarcopenic lean NAFLD patients had significantly increased risk of atherosclerotic carotid plaque and liver fibrosis, which was correlated with a characteristic metabolomic profile distinct from non-sarcopenic lean NAFLD and overweight/obese NAFLD patients. Therefore, our study supported the necessity to screen sarcopenia in the middle-aged and older NAFLD patients, which might facilitate the risk stratification and personalized prediction of clinical outcomes in the middle-aged and older NAFLD patients.
Abbreviations
- ALT:
-
Alanine transaminase
- ApoA1:
-
Apolipoprotein A1
- ApoA2:
-
Apolipoprotein A2
- ApoB:
-
Apolipoprotein B100
- ASM/height2 :
-
Height-adjusted appendicular skeletal muscle mass
- AST:
-
Aspartate transaminase
- AWGS:
-
Asian working group for sarcopenia
- BMI:
-
Body mass index
- CE:
-
Cholesterol esters
- DBP:
-
Diastolic blood pressure
- DXA:
-
Dual-energy X-ray absorptiometry
- FC:
-
Free cholesterol
- FDR:
-
False discovery rate
- FIB-4:
-
Fibrosis 4 score
- FPG:
-
Fasting plasma glucose
- HDL:
-
High-density lipoprotein
- HOMA-IR:
-
Homeostasis model assessment for insulin resistance
- hs-CRP:
-
High-sensitivity C-reactive protein
- HR:
-
Hazard ratio
- ICD-10:
-
The 10th revision of international classification of diseases
- IDL:
-
Intermediate density lipoprotein
- LDL:
-
Low-density lipoprotein
- LFC:
-
Liver fat content
- NAFLD:
-
Non-alcoholic fatty liver disease
- NAG:
-
N-acetyl-glycoproteins
- NAG1:
-
N-acetylglucosamine/galactosamine-glycoproteins
- NAG2:
-
N-acetylneuraminyl-glycoproteins
- NASH:
-
Non-alcoholic steatohepatitis
- NHANES III.:
-
Third National Health and Nutrition Examination Survey
- OGTT:
-
Oral glucose tolerance test
- OR:
-
Odds ratio
- PPG:
-
Post-load plasma glucose
- PL:
-
Phospholipids
- SBP:
-
Systolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- VLDL:
-
Very low-density lipoprotein
- 1H-NMR:
-
1-H nuclear magnetic resonance spectroscopy
- 95%CI:
-
95% Confidence interval
References
Younossi ZM. Non-alcoholic fatty liver disease—a global public health perspective. J Hepatol. 2019;70(3):531–544
Yki-Järvinen H. Non-alcoholic fatty liver disease as a cause and a consequence of metabolic syndrome. Lancet Diabetes Endocrinol. 2014;2(11):901–910
Younossi ZM, Stepanova M, Younossi Y, Golabi P, Mishra A, Rafiq N, et al. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut. 2020;69:564–568
Estes C, Anstee QM, Arias-Loste MT, Bantel H, Bellentani S, Caballeria J, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J Hepatol. 2018;69(4):896–904
Wong VW, Chu WC, Wong GL, Chan RS, Chim AM, Ong A, et al. Prevalence of non-alcoholic fatty liver disease and advanced fibrosis in Hong Kong Chinese: a population study using proton-magnetic resonance spectroscopy and transient elastography. Gut. 2012;61(3):409–415
Younossi ZM, Blissett D, Blissett R, Henry L, Stepanova M, Younossi Y, et al. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology. 2016;64(5):1577–1586
Zou B, Yeo YH, Nguyen VH, Cheung R, Ingelsson E, Nguyen MH. Prevalence, characteristics and mortality outcomes of obese, nonobese and lean NAFLD in the United States, 1999–2016. J Intern Med. 2020;288(1):139–151
Shi Y, Wang Q, Sun Y, Zhao X, Kong Y, Ou X, et al. The prevalence of lean/nonobese nonalcoholic fatty liver disease: a systematic review and meta-analysis. J Clin Gastroenterol. 2020;54(4):378–387
Sookoian S, Pirola CJ. Systematic review with meta-analysis: risk factors for non-alcoholic fatty liver disease suggest a shared altered metabolic and cardiovascular profile between lean and obese patients. Aliment Pharmacol Ther. 2017;46(2):85–95
Ye Q, Zou B, Yeo YH, Li J, Huang DQ, Wu Y, et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2020;5(8):739–752
Xia MF, Chen LY, Wu L, Ma H, Li Q, Aleteng Q, et al. The PNPLA3 rs738409 C>G variant influences the association between low skeletal muscle mass and NAFLD: the Shanghai Changfeng Study. Aliment Pharmacol Ther. 2019;50(6):684–695
Hong HC, Hwang SY, Choi HY, Yoo HJ, Seo JA, Kim SG, et al. Relationship between sarcopenia and nonalcoholic fatty liver disease: the Korean sarcopenic obesity study. Hepatology. 2014;59:1772–1778
Koo BK, Kim D, Joo SK, Kim JH, Chang MS, Kim BG, et al. Sarcopenia is an independent risk factor for non-alcoholic steatohepatitis and significant fibrosis. J Hepatol. 2017;66:123–131
Petta S, Ciminnisi S, Di Marco V, Cabibi D, Cammà C, Licata A, et al. Sarcopenia is associated with severe liver fibrosis in patients with non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2017;45:510–518
Xia M, Zeng H, Wang S, Tang H, Gao X. Insights into contribution of genetic variants towards the susceptibility of MAFLD revealed by the NMR-based lipoprotein profiling. J Hepatol. 2021;74(4):974–977
Xia MF, Yan HM, He WY, Li XM, Li CL, Yao XZ, et al. Standardized ultrasound hepatic/renal ratio and hepatic attenuation rate to quantify liver fat content: an improvement method. Obesity (Silver Spring). 2012;20:444–452
Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American society of echocardiography carotid intima-media thickness task force. Endorsed by the society for vascular medicine. J Am Soc Echocardiogr. 2008;21(2):93–111
Jiménez B, Holmes E, Heude C, Tolson RF, Harvey N, Lodge SL, et al. Quantitative lipoprotein subclass and low molecular weight metabolite analysis in human serum and plasma by 1 H NMR spectroscopy in a multilaboratory trial. Anal Chem. 2018;90(20):11962–11971
Xia MF, Ma S, Huang QX, Zeng HL, Ge JY, Xu WJ, et al. NAFLD-related gene polymorphisms and all-cause and cause-specific mortality in an Asian population: the Shanghai Changfeng Study. Aliment Pharmacol Ther. 2022;55(6):705–721
European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity. EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–402
Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, et al. Sarcopenia in Asia: consensus report of the Asian working group for sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101
Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646
Bhanji RA, Narayanan P, Allen AM, Malhi H, Watt KD. Sarcopenia in hiding: the risk and consequence of underestimating muscle dysfunction in nonalcoholic steatohepatitis. Hepatology. 2017;66(6):2055–2065
Kim JA, Choi KM. Sarcopenia and fatty liver disease. Hepatol Int. 2019;13(6):674–687
Han YH, Onufer EJ, Huang LH, Sprung RW, Davidson WS, Czepielewski RS, et al. Enterically derived high-density lipoprotein restrains liver injury through the portal vein. Science. 2021;373(6553):eabe6729
Xie G, Wang X, Wei R, Wang J, Zhao A, Chen T, et al. Serum metabolite profiles are associated with the presence of advanced liver fibrosis in Chinese patients with chronic hepatitis B viral infection. BMC Med. 2020;18(1):144
Yu D, Richardson NE, Green CL, Spicer AB, Murphy ME, Flores V, et al. The adverse metabolic effects of branched-chain amino acids are mediated by isoleucine and valine. Cell Metab. 2021;33(5):905-922.e6
Xia MF, Chen LY, Wu L, Ma H, Li XM, Li Q, et al. Sarcopenia, sarcopenic overweight/obesity and risk of cardiovascular disease and cardiac arrhythmia: a cross-sectional study. Clin Nutr. 2021;40(2):571–580
Ko BJ, Chang Y, Jung HS, Yun KE, Kim CW, Park HS, et al. Relationship between low relative muscle mass and coronary artery calcification in healthy adults. Arterioscler Thromb Vasc Biol. 2016;36(5):1016–1021
Brown JC, Harhay MO, Harhay MN. Sarcopenia and mortality among a population-based sample of community-dwelling older adults. J Cachexia Sarcopenia Muscle. 2016;7(3):290–298
Xu Y, Jiang H, Li L, Chen F, Liu Y, Zhou M, et al. Branched-chain amino acid catabolism promotes thrombosis risk by enhancing tropomodulin-3 propionylation in platelets. Circulation. 2020;142(1):49–64
Yeung S, Zhu Z, Kwok T, Woo J. Serum amino acids patterns and 4-year sarcopenia risk in community-dwelling chinese older adults. Gerontology. 2022;68:736–745
Ma S, Xia M, Gao X. Biomarker discovery in atherosclerotic diseases using quantitative nuclear magnetic resonance metabolomics. Front Cardiovasc Med. 2021;8:681444
Gong H, Liu Y, Lyu X, Dong L, Zhang X. Lipoprotein subfractions in patients with sarcopenia and their relevance to skeletal muscle mass and function. Exp Gerontol. 2022;159:111668
Funding
We have obtained financial supports from the Ministry of Science and Technology of China (2018YFE0201603, 2020YFE0201600), the Shanghai Pujiang Talent Project (20PJ1402300), the Shanghai Municipal Science and Technology Major Project (2017SHZDZX01), the Science and Technology Commission of Shanghai Municipality (16JC1400500, 16411954800), the National Natural Science Foundation of China (81873660, 31821002 and 82100849), and Foundations from Zhongshan Hospital, Fudan University (2020ZSLC58, 2021ZSQN07).
Author information
Authors and Affiliations
Contributions
Study concept and design: MX, XG, HT. Acquisition of data: XZ, QH, SM, LC, QW, LW, XL, HM, QL, QA, MX, HL. Analysis of data: XZ, SM, QH, JG, MX. Technic support and data interpretation: QH, WH. Data management: HL. Manuscript drafting: XZ, MX. Manuscript revision: MX, XG, HT, YH. Obtained funding; XG, HT, MX, XZ. MX and XG are the guarantors of this work and, as such, takes responsibility for the integrity of the work as a whole, from inception to published article.
Corresponding authors
Ethics declarations
Conflict of interests
Xiaopeng Zhu declares that there is no duality of interest. Qingxia Huang declares that there is no duality of interest. Shuai Ma declares that there is no duality of interest. Lingyan Chen declares that there is no duality of interest. Qi Wu declares that there is no duality of interest. Li Wu declares that there is no duality of interest. Hui Ma declares that there is no duality of interest. Xiaoming Li declares that there is no duality of interest. Qian Li declares that there is no duality of interest. Qiqige Aleteng declares that there is no duality of interest. Yu Hu declares that there is no duality of interest. Wanyuan He declares that there is no duality of interest. Jian Gao declares that there is no duality of interest. Huandong Lin declares that there is no duality of interest. Huiru Tang declares that there is no duality of interest. Xin Gao declares that there is no duality of interest. Mingfeng Xia declares that there is no duality of interest.
Ethical approval
The study was approved by the Research Ethics Committees of Zhongshan Hospital, Fudan University (No. 2008-119 and B2013-132).
Informed consent
Each participant provided written informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhu, X., Huang, Q., Ma, S. et al. Presence of sarcopenia identifies a special group of lean NAFLD in middle-aged and older people. Hepatol Int 17, 313–325 (2023). https://doi.org/10.1007/s12072-022-10439-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12072-022-10439-z