
Abstract
CD105 is an ancillary receptor of transforming growth factor beta (TGF-β), which has been suggested as a suitable biomarker for cancer-related angiogenesis and neovascularization (Nassiri et al. in Anticancer Res 31:2283–2290, 2011). However, the clinical significance of CD105 in WHO grade was rarely reported and the effects of CD105 signal transduction pathway on gliomas remain controversial and unclear. To get a convincing conclusion, performing a meta-analysis is essential. Relevant literature studies were included via careful evaluation, and standard mean difference (SMD) and hazard ratio (HR) with 95 % confidence intervals (95 % CIs) was calculated. We also made funnel plots to test the heterogeneity. In the present meta-analysis, a total of 11 eligible literatures involving 796 patients were incorporated. They were all conducted in China, revealing that CD105 overexpression in glioma tissues was strongly linked to high WHO grading (III+IV) (SMD −1.785, 95 % CI −2.133, −1.437; p = 0.000). No significant associations between CD105 and age (SMD −0.505, 95 % CI −1.054, 0.043; p = 0. 071), CD105 and gender (SMD 0.101, 95 % CI −0.103, 0.305; p = 0.333), and CD105 and tumor size (SMD −0.433, 95 % CI −1.326, 0.459; p = 0. 341) were detected. Besides, CD105 expression was closely associated with glioma patients’ 3-year overall survival (OS; n = 2; HR = 4.357, 95 % CI 1.412, 7.303; p = 0.004). On the basis of Begg’s and Egger’s test or funnel plot, no publication bias was detected. In a nutshell, this meta-analysis demonstrated that CD105 overexpression correlates to higher WHO grade and poor survival and could be indicated as a helpful prognostic and diagnostic marker, or a useful therapy target.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glioma is a common primary cerebral tumor. Surgical resection is the usual treatment for glioma in combination with chemotherapy and radiotherapy. Gliomas are classified into four clinical grades (I–IV) on the basis of tumor histopathology according to the World Health Organization (WHO) [1]. Grade I glioma is usually regarded as relatively benign lesions. Grades II, III, and IV gliomas have an infiltrative and aggressive phenotype. They also have poorly demarcated margins and directly invade the adjacent cerebral parenchyma [2]. Since WHO grade can provide surgeons a chance to treat glioma patients as early as they can, it is necessary to seek a helpful and meaningful biomarker to evaluate the grade and predict the prognosis.
CD105 was originally characterized more than two decades ago [3]. It is classified as an accessory receptor for TGF-β, a pleiotropic cytokine [4]. Prominently, its expression is upregulated on actively proliferating endothelial cells [5, 6]. CD105 has thus been recommended as a proper biomarker for tumor-related angiogenesis. The roles of CD105 in the diagnosis, prognosis, and treatment of tumors have been discussed recently [6], including breast cancer [7], squamous cell carcinoma [8], and pancreatic ductal adenocarcinoma [9]. Studies also demonstrated that CD105 played a pivotal role in controlling glioma angiogenesis by virtue of promoting new vascular network and fueling further glioma development through supplying elevated oxygen quantity and other essential metabolites, causing brain invasion and thus worsened prognosis [10–12].
However, CD105’s precise effects on WHO grade and prognosis of gliomas are not yet clear enough. We carried out a meta-analysis to elucidate the practical significance of CD105 and resolve the between-study heterogeneity. This is possible partly because a meta-analysis can reduce the potential bias of sources such as with the selected populations and study methodology. In the present analysis, we extracted data from published articles and systematically evaluated CD105 regarding the WHO grades and prognosis of gliomas.
Methods
Search Strategy
A literature search was conducted through databases of PubMed, Google Scholar, Embase, Wanfang, and Cnki up to April 2015. No restrictions about languages and sources were set. Search key terms were “CD105 (endoglin)” or “CD105,” “gliomas [MeSH],” “expression,” “grade,” etc. we also reviewed the references in retrieved articles to identify other potentially available studies.
Study Selection
Eligible studies were selected by two reviewers independently. If there were disagreement in the process, a third reviewer would help. The inclusion criteria were as follows: (1) The diagnoses of gliomas were confirmed by pathologists; (2) the principle outcomes in literatures focused on WHO grade, gender, age, and overall survival (OS); (3) the level of CD105 expression was identified by virtue of immunohistochemistry (IHC), real-time quantitative PCR (qPCR), reverse transcription PCR (RT-PCR), or western blot (WB); (4) the hazard ratio (HR) value and 95 % confidence interval (CI) of CD105 expression level on survival status could be extracted directly from articles or calculated according to the figures or tables given; and (5) to avoid duplicated studies, only the most recently published and/or the most complete ones were included.
Data Extraction
Through a purpose-designed form, two reviewers independently extracted the following data: The first author name, country, publication year, study methods, histology, WHO grading, patient number, patient age, and positive percentage. Disagreements between the two reviewers, if any, would be solved by discussion with a third reviewer.
Quality Assessment
The publications were read and scored, and a quality assessment was conducted for the eligible studies by the independent reviewers according to the quality scale for biologically prognostic factors established by ELCWP [13]. The scientific design, laboratory methodology, generalizability, and results analysis were evaluated on this scale. The maximum points for each category were 10, and therefore the maximum was 40 points. If necessary, a consensus score was obtained for each category after comparison of the initial scores for the two investigators. The final scores for the categories indicate the percentage of the maximum achievable scores, which ranged from 0 to 100 %. Higher scores represented better methodological quality.
Data Synthesis and Analysis
Differences were expressed as standard mean differences (SMDs) with 95 % CIs. We synthesized the survival outcome data by means of the time-to-event HR as operational measure. If HR and 95 % CI were not directly given in the article, data in tables or/and figures were extracted and HRs with 95 % CI were recalculated by virtue of SPSS19.0, Engauge Digitizer version 4.1, and methods described by Tierney et al. [14] and Parmar et al. [15].
Differences are indicated as SMDs (95%CI). STATA 12.0 (StataCorp LP, College Station, TX, USA) was used for all statistical analyses. Cochran’s Q test, the I 2 test (variation in SMD attributable to heterogeneity), and a Galbraith figure were used to judge heterogeneity among the included studies [16, 17]. If the circles in the Galbraith figure are all distributed in a region bounded by the upper and lower lines, then there is evidence for homogeneity. Also, if p < 0.05 for the Q statistic, then heterogeneity was considered to be significant [18]. I 2 values of 25, 50, and 75 % were used as evidence of low, moderate, and high heterogeneity, respectively [16]. A fixed-effects model was used if there was no evidence of statistical heterogeneity among the studies. A random-effects model (DerSimonian and Laird) was used otherwise [18].
A sensitivity analysis was conducted to determine whether or not the pooled outcomes were stable, and the analysis was done one after another at a time. When assessing one study, another one was neglected for the purpose of meta-analysis. It indicated that the outcomes were not stable if the ignorance of one study affected the process. The funnel plot was used to conduct visual assessment to review any possible publication bias. If the asymmetric plot appeared, the publication bias existed [19]. The publication bias could also be indicated by another method called the Egger linear regression test, which should be run at the p < 0.05 level of significance [20]. Meta regression was not conducted in the research because there were not enough reference sources used.
Traditionally, an observed HR >1 indicated a poor survival for patients with increased CD105 expression. There were two sides for all p values, and it was seen as an extremely large number when p < 0.05. The STATA 12.0 (StataCorp LP, College Station, TX, USA) and Review Manager 5.3 (The Cochrane Collaboration) were both used to conduct data analyses.
Results
Search Results and Characteristics of Studies
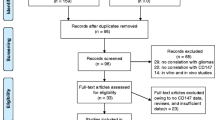
The article searches were carried out as shown in Fig. 1. At first, a literature search from multiple databases generated 93 articles. Of the relevant studies, 73 articles were excluded by the title and abstract, that is, 27 for no correlation with gliomas, 30 for no correlation with CD105 studies, and 16 for in vitro and in vivo studies. Subsequently, the rest of the 20 articles underwent another assessment, among which 9 articles were excluded owing to no CD105 data, reviews, and insufficient data. Interestingly, all included articles were conducted in China. Eventually, 11 articles that met the criteria were included. The general characteristics of 11 studies are summarized in Table 1. A total of 785 patients were included with the mean age of 43.5 and 352 cases of low-grade gliomas (I+II). All 11 studies were conducted in Chinese populations. CD34 staining was counted as microvascular density (MVD), which was obtained by manually counting the positive foci for slides counterstained with hematoxylin. The MVD with positive CD105 stain (CD105-MVD) varies from 8.13 to 45.96. HRs and 95 % CIs were obtained from Kaplan–Meier curves merely in only two studies. All the 11 studies offered WHO grade data, 5 studies analyzed the correlation between CD105 and age/gender, and 4 included the factor of tumor size. CD105 protein in glioma tissues was investigated by the method of IHC in all the 11 studies, among which 3 also adopted qPCR and 1 adopted WB. To reduce the potential bias caused by heterogeneity, we only incorporated the IHC data.

Literature search and selection of articles. PRISMA 2009 Flow Diagram (Moher et al 22)
Study Quality
The putative ELCWP was used to evaluate the quality of all research studies. Table 2 presents the research results. The mean score for all studies was 80.66 %. Across all studies, results analysis obtained a high mean score of 8.28, compared with design (8.02), method (8.07), and generalizability (7.89). The mean global scores in terms of age/gender and tumor size were 82.45 and 82.31 %, respectively. Because the two-sided p values were greater than 0.05 when Student’s t test was used, there was not possible heterogeneity existing between the features of study baseline.
Meta-analysis About CD105 and WHO Grade and Prognosis
We divided WHO grade into low and high grade (III+IV) for the crosstable. Information of WHO grade was available in all the 11 studies which were all continuous data (Table 1). From the Galbraith figure (Fig. 2a), we can see three points fall outside the appointed region, which can be taken as evidence of heterogeneity among these studies (Q = 36.7, d.f. = 10, I 2 = 72.8 %). As showed in Fig. 3a, using a random effect model, SMDs revealed a significant association between CD105 expression and high WHO grade (SMD −1.785, 95 % CI −2.133, −1.437; p = 0.000) suggesting that high CD105 expression in postoperative glioma tissues could predict a high-grade glioma, and high CD105 expression is recommended as a clinical biomarker for diagnosis. The heterogeneity was not significant upon gender (Fig. 2b, Q = 1.73, d.f. = 4, I 2 = 0.0 %) rather than age (Q = 24.53, d.f. = 4, I 2 = 83.7 %) and tumor size (Q = 30.65, d.f. = 3, I 2 = 90.2 %) (figures not shown). There were no significant associations between CD105 and age (Fig. 3b, SMD −0.505, 95 % CI −1.054, 0.043; p = 0. 071), CD105 and gender (Fig. 3c, SMD 0.101, 95 % CI −0.103, 0.305; p = 0.333), and CD105 and tumor size (Fig. 3d, SMD −0.433, 95 % CI −1.326, 0.459; p = 0. 341). Three articles analyzed the value of CD105 overexpression in 3-year overall survival. On the basis of this meta-analysis, CD105 expression level was obviously associated with 3-year OS (HR = 4.357, 95 % CI 1.412, 7.303; p = 0.004) (Fig. 3e) in glioma patients, suggesting CD105 is able to effectively predict the prognosis and provide a helpful hint for early treatments.

Galbraith figure of included studies focusing on the correlation between CD105 and WHO grade a and CD105 and gender b If the circles are all distributed within the region bounded by the upper line and the lower line, it can be taken as an evidence of homogeneity. The farther away from the region, the more obvious the heterogeneity is


Individual and pooled SMD with 95 % CI about CD105 and WHO grade, age, gender, tumor size, and 3-year OS. A random-effect model revealed an association between CD105 and WHO grade (n = 11, SMD −1.785, 95 % CI −2.133, −1.437; p = 0.000) a No significant associations exist between CD105 and age (SMD −0.505, 95 % CI −1.054, 0.043; p = 0. 071) b gender (SMD 0.101, 95 % CI −0.103, 0.305; p = 0.333) c and tumor size (SMD −0.433, 95 % CI −1.326, 0.459; p = 0. 341) d A fixed effect model revealed an association between CD105 and 3-year OS (HR = 4.357, 95 % CI 1.412, 7.303; p = 0.004) e
Sensitivity Analysis and Publication Bias
The effects of each single study on pooled OR or SMD were evaluated using the sensitivity analysis, in which each study was taken out of consideration during the assessment. The outcome showed that the pooled SMDs of CD105 and WHO grade, suggesting a statistically robust result (Fig. 4). Publication bias analysis of these 11 literatures was conducted through the type of funnel plot with the result of symmetric distribution (Fig. 5). Also, Begg’s and Egger’s test were conducted, showing no statistical evidence of publication bias (p = 0.932, 95 % CI −4.42, 4.48).

Sensitivity analysis of included studies. Results were computed by omitting each study in turn. Meta-analysis random-effect estimates (exponential form) were used. The two ends of the dotted lines represent the 95 % CI

Funnel blot was designed to visualize a potential publication bias. Funnel plots’ shape of all studies did not reveal obvious evidence of asymmetry, suggesting that publication bias was also not observed among studies with pathological indicators
Discussion
Recent movements toward antibody-based therapeutic strategies in neoplasms have led to the characterization of some potential antigens. CD105, also called Endoglin, is just one such antigen with widespread popularity. CD105 is a co-receptor of TGF-β, a pleiotropic cytokine controlling cellular proliferation, migration, adhesion, and differentiation [7, 9, 10]. In recent years, studies have demonstrated that CD105-positive vessels play a pivotal role in the biology of gliomas and have an influence in prognosis [10–12]. One of the possible explanations for its prognostic influence is via its role in developing the microvascular niche where stem-like oncocytes preferentially inhabit [22]. Few reports, however, discussed the comprehensive clinical significances of CD105 in glioma patients, and the accurate roles of CD105 in WHO grade and glioma prognosis were not well known. As such, it remains unclear whether or not CD105 can be used as a criteria of gliomas’ WHO grade. Herein, we combined PubMed, Google Scholar, Embase, Wanfang, and Cnki to comprehensively analyze the clinical effects of CD105.
In the present study, we investigated CD105 expression in 11 glioma studies and its association with WHO grade in 796 patients. Here, quality assessment was subjected to the published ELCWP, and there was no sign of marked differences across all studies. If significant heterogeneity was observed among studies, a random effect model, which provides a more conservative standard error and a larger confidence interval, was chosen to determine the pooled SMD/HR estimates. Our analysis showed that CD105 overexpression in glioma tissues was closely associated with high WHO grade (III+IV) (SMD −1.785, 95 % CI −2.133, −1.437; p = 0.000) and there were no significant correlations between CD105 and age (p = 0. 071), gender (p = 0.333), or tumor size (p = 0. 341).
These findings are of potential clinical importance. First, as considering the specific overexpression of CD105 on glioma vasculature, it seems to be a promising target for antiangiogenic therapy. Several approaches targeting CD105 have already been evaluated: (1) CD105-Fc constructs. CD105-Fc, as a chimeric protein, is consisted of the extracellular part of CD105 fused to Fc tail of human IgG. This molecule works like a ligand trap for CD105 ligands including BMP-10 and BMP-9 [23, 24]. Castonguay et al. showed that in BALB/c mice subcutaneously injected with colon denocarcinoma cells, CD105-Fc greatly reduced tumors’ angiogenesis, and thus tumor growth [24]. (2) CD105 vaccines. One research explored the use of a CD105 protein vaccine with low-dose cisplatin. Liver or lung cancer cells were subcutaneously inoculated in mice treated with this protein vaccine, cisplatin, or their combination. Both monotherapies restrained tumor growth, while combination therapy synergistically reduced tumor volume, led to the biosynthesis of auto-antibodies against CD105, and induced endothelia cell apoptosis in vivo [25]. More recently, CD105-based DNA vaccines were also developed and studied in pre-clinical models [26]. (3) CD105 neutralizing antibodies. In vivo, anti-CD105 monoclonal antibody has been observed in mice to inhibit tumor growth and metastasis. This effect is either by destruction of tumor vasculature or by inhibition of tumor angiogenesis [27]. Currently, multiple phase II clinical studies are being carried on, assessing the therapeutic efficacy of TRC105 (an anti-CD105 monoclonal antibody that binds CD105with high avidity and exhibits anti-angiogenic and antitumor effects) treatment alone and in combination with bevacizumab and other anti-tumor agents [28]. These strategies cause specific inhibition of the tumor angiogenesis by either inducing cell death (CD105 vaccine) or blocking CD105 signaling (CD105-Fc and neutralizing antibodies).
Second, improved detection of high-grade glioma will greatly improve standard practice of care for these patients. For those gliomas whose pathological grade is hard to confirm, the expression level of CD105 can indeed provide more additional information to help determine the cellular or molecular pathological nature. Unlike low-grade gliomas, for high-grade ones, it is better to perform more aggressive and more vigorous treatments to expect to improve the quality of life and prolong survival time. The common treatment choices include timely and appropriate chemotherapy, radiotherapy, and molecular targeted therapy against specific antigen like CD105. So to determine the WHO grade and related pathological features of the gliomas is of vital importance to improve therapeutic schedules individually and rationally. Third, CD105 is expressed not only in vascular endothelium, chondrocytes, and blast cells of term placenta but also in early stage or activated blood cells, hence making CD105 also a potential blood biomarker that would be potentially predictive of high-grade gliomas.
Subsequently, we analyzed three articles involving CD105 expression and 3-year overall survival and observed that CD105 expression was significantly associated with 3-year OS (HR = 4.357, 95 % CI 1.412, 7.303; p = 0.004) (Fig. 3) in patients. Thus, it is plausible that CD105 antagonist may be a potential adjuvant therapy for treating gliomas following surgical resection, radiotherapy, and chemotherapy.
Galbraith figure, Cochran’s Q test, and I 2 test (variation in OR attributable to heterogeneity) were all performed to judge the heterogeneity between included studies. When p < 0.05 and/or I 2 > 50 %, the heterogeneity was considered statistically significant. In this meta-analysis, there did exist heterogeneity among studies about WHO grade, age, and tumor size. So, a random effect model was recommended in the analysis. On the other hand, several limitations of this study should be considered as many as possible. CD105 expression in included studies was utterly investigated in Chinese populations and tested by different methods and criteria. Particularly, IHC depended largely on the methodological factors such as primary and secondary antibody titer. However, it was very hard to conduct subgroup analyses by different antibodies to explore the potential bias of method on the pooled results. In addition, most studies did not offer complete data, although it may not affect the bias.
Publication bias can affect the meta-analysis quite a lot [29]. Research studies with negative outcomes were all abandoned, leaving only positive ones for the public. Recently, no publication bias contented Egger’s and Begger’s p value test or funnel plot. The publication bias may occur because the sources were English and Chinese only. Another limitation of this meta-analysis is that it remains unconfirmed whether CD105 represents an independent prognostic indicator beyond predicting glioma grade. It would be of meaningfulness to analyze the subgroup of isocitrate dehydrogenase (IDH)-mutated gliomas since their biology is completely different from IDH-wide type. On the basis of a study by Popov et al., IDH1-positive glioblastomas were associated with a glomeruloid vascular proliferation in the absence of arcade-like structures which was confirmed by CD105 staining [30]. And, an unexpected finding in a current study is a statistically significant association between diffuse and strong CD105 expression by acute myelocytic leukemia blasts and the IDH2 mutation. The authors’ sense is that the CD105 data are stronger than the grading data in predicting, but it is difficult to be sure unless this is specifically addressed [31]. Unfortunately, the included papers do not have IDH status stated for the tumors; thus, the correlation between CD105 and other well-known glioma biomarkers such as IDH, O6-methylguanine-DNA methyltransferase (MGMT) gene promoter methylation, and 1p/19q co-deletion is one of the further research directions.
In conclusion, our meta-analysis demonstrates that CD105 is significantly associated with high grade and functions as an essentially prognostic factor for glioma patients. Moreover, accurate prediction and early regimen of patients who were given surgical resection were possible with pathological CD105 gene or protein assessment. In addition, more evidence is still in demand to support the current research results.
References
Taal W, Bromberg JE, van den Bent MJ (2015) Chemotherapy in glioma. CNS Oncol 4:179–192
Venneti S, Huse JT (2015) The evolving molecular genetics of low-grade glioma. Adv Anat Pathol 22:94–101
Quackenbush EJ, Letarte M (1985) Identification of several cell surface proteins of non-T, non-B acute lymphoblastic leukemia by using monoclonal antibodies. J Immunol 134:1276–1285
Wong SH, Hamel L, Chevalier S, Philip A (2000) Endoglin expression on human microvascular endothelial cells association with betaglycan and formation of higher order complexes with TGF-beta signalling receptors. Eur J Biochem 267:5550–5560
Nassiri F, Cusimano MD, Scheithauer BW et al (2011) Endoglin (CD105): a review of its role in angiogenesis and tumor diagnosis, progression and therapy. Anticancer Res 31:2283–2290
Wikstrom P, Lissbrant IF, Stattin P, Egevad L, Bergh A (2002) Endoglin (CD105) is expressed on immature blood vessels and is a marker for survival in prostate cancer. Prostate 51:268–275
Martinez LM, Labovsky V, de Lujan CM et al (2015) CD105 Expression on CD34-Negative Spindle-Shaped Stromal Cells of Primary Tumor Is an Unfavorable Prognostic Marker in Early Breast Cancer Patients. PLoS One 10:e121421
Nair S, Nayak R, Bhat K, Kotrashetti VS, Babji D (2015) Immunohistochemical expression of CD105 and TGF-beta1 in oral squamous cell carcinoma and adjacent apparently normal oral mucosa and its correlation with clinicopathologic features. Appl Immunohistochem Mol Morphol 24:35–41
Lytras D, Leontara V, Kefala M et al (2015) Microvessel landscape assessment in pancreatic ductal adenocarcinoma: unclear value of targeting endoglin (CD105) as prognostic factor of clinical outcome. Pancreas 44:87–92
Smith SJ, Tilly H, Ward JH et al (2012) CD105 (Endoglin) exerts prognostic effects via its role in the microvascular niche of paediatric high grade glioma. Acta Neuropathol 124:99–110
Clara CA, Marie SK, de Almeida JR et al (2014) Angiogenesis and expression of PDGF-C, VEGF, CD105 and HIF-1alpha in human glioblastoma. Neuropathology 34:343–352
Wang YF, Wang DL, Shi GS, Huang H (2006) Expressions of hTERT, HIF-1alpha and CD105 in gliomas and their clinical significance. Zhonghua Bing Li Xue Za Zhi 35:681–682
Steels E, Paesmans M, Berghmans T et al (2001) Role of p53 as a prognostic factor for survival in lung cancer: a systematic review of the literature with a meta-analysis. Eur Respir J 18:705–719
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR (2007) Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 8:16
Parmar MK, Torri V, Stewart L (1998) Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med 17:2815–2834
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Wang D, Mou ZY, Zhai JX, Zong HX, Zhao XD (2008) Application of Stata software to test heterogeneity in meta-analysis method. Zhonghua Liu Xing Bing Xue Za Zhi 29:726–729
Dickersin K, Berlin JA (1992) Meta-analysis: state-of-the-science. Epidemiol Rev 14:154–176
Stuck AE, Rubenstein LZ, Wieland D (1998) Bias in meta-analysis detected by a simple, graphical test. Asymmetry detected in funnel plot was probably due to true heterogeneity. BMJ 316(469):470–471
Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L (2006) Comparison of two methods to detect publication bias in meta-analysis. JAMA 295:676–680
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097
Paschoal JP, Bernardo V, Canedo NH, Ribeiro OD, Caroli-Bottino A, Pannain VL (2014) Microvascular density of regenerative nodule to small hepatocellular carcinoma by automated analysis using CD105 and CD34 immunoexpression. BMC Cancer 14:72
Hawinkels LJ, Kuiper P, Wiercinska E et al (2010) Matrix metalloproteinase-14 (MT1-MMP)-mediated endoglin shedding inhibits tumor angiogenesis. Cancer Res 70:4141–4150
Castonguay R, Werner ED, Matthews RG et al (2011) Soluble endoglin specifically binds bone morphogenetic proteins 9 and 10 via its orphan domain, inhibits blood vessel formation, and suppresses tumor growth. J Biol Chem 286:30034–30046
Tan GH, Tian L, Wei YQ et al (2004) Combination of low-dose cisplatin and recombinant xenogeneic endoglin as a vaccine induces synergistic antitumor activities. Int J Cancer 112:701–706
Wood LM, Pan ZK, Guirnalda P, Tsai P, Seavey M, Paterson Y (2011) Targeting tumor vasculature with novel Listeria-based vaccines directed against CD105. Cancer Immunol Immunother 60:931–942
Paauwe M, Ten DP, Hawinkels LJ (2013) Endoglin for tumor imaging and targeted cancer therapy. Expert Opin Ther Targets 17:421–435
Liu Y, Tian H, Blobe GC, Theuer CP, Hurwitz HI, Nixon AB (2014) Effects of the combination of TRC105 and bevacizumab on endothelial cell biology. Invest New Drugs 32:851–859
Rockwell S, Kimler BF, Moulder JE (2006) Publishing negative results: the problem of publication bias. Radiat Res 165:623–625
Popov S, Jury A, Laxton R et al (2013) IDH1-associated primary glioblastoma in young adults displays differential patterns of tumour and vascular morphology. PLoS One 8, e56328
Chakhachiro ZI, Zuo Z, Aladily TN et al (2013) CD105 (endoglin) is highly overexpressed in a subset of cases of acute myeloid leukemias. Am J Clin Pathol 140:370–378
Funding statement
This study was supported by the Research Special Fund for Public Welfare Industry of Health (Project No. 201402008). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors state that there are no conflicts of interest to disclose.
Additional information
Xiangyi Kong, Yu Wang and Shuai Liu contributed equally to this work.
Rights and permissions
About this article

Cite this article
Kong, X., Wang, Y., Liu, S. et al. CD105 Over-expression Is Associated with Higher WHO Grades for Gliomas. Mol Neurobiol 53, 3503–3512 (2016). https://doi.org/10.1007/s12035-015-9677-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-015-9677-1