
Abstract
Up to now, survivin has been recommended as a prognostic and diagnostic indicator in glioma patients. However, there are still many controversies. Here, a meta-analysis was conducted to draw a more definitive conclusion on the correlation of survivin with overall survival (OS), age, gender, and WHO grade. Eligible studies were available through careful assessment, and then pooled hazard ratios (HRs) or odds ratios (ORs) with 95 % confidence intervals (95 % CIs) were estimated. Funnel plots were introduced to evaluate the publication bias. Additionally, heterogeneity and sensitivity were also evaluated. In the present meta-analysis, 15 eligible studies with a total of 1,089 patients were incorporated. Survivin expression in gliomas correlated with 2-year OS (n = 8; HR 0.17, 95 % CI 0.11–0.26) and 5-year OS (n = 7; HR 0.12, 95 % CI 0.07–0.22) in patients. In addition, a fixed-effect model revealed a significant association between survivin and age (male/+; OR 2.10, 95 % CI 1.44–3.05) and survivin and WHO grade (I+II/+; OR 0.27, 95 % CI 0.19–0.38). No heterogeneity was observed across all studies. According to Begg’s and Egger’s test and funnel plot, no publication bias was reported. Taken together, our meta-analysis suggests that survivin expression is associated with poor survival, older age, and higher WHO grade and could be suggested as a useful prognostic and diagnostic biomarker, or an effective therapy target.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glioma is the most common one of human brain tumors and makes up 80 % of all malignant brain tumors, involving astrocytes, oligodendrocytes, ependyma, and choroid plexus epithelium [1]. Gliomas are divided into four malignancy grades according to the World Health Organization (WHO), among which low-grade gliomas (grade I and II) are well-differentiated, exhibit benign tendencies, and predict a better prognosis for the patients. It should be noted that glioblastoma portends the worst prognosis in all gliomas, with a median survival time ranging from 9 to 10 months. Therefore, it is quite necessary to investigate an effective biomarker to predict prognosis.
Survivin, located on human chromosome 17q25.3, is a novel member of inhibitor of apoptosis protein family. Generally survivin is present in the embryonic tissues and absent in most normal adult tissues [2]. In recent years, survivin has been characterized as overexpressed in other human tumors, including lung carcinoma [3], breast carcinoma [4], and liver carcinoma [5]. Recent studies also confirmed that survivin played a crucial role in regulating glioma cell mitosis [6] or inhibiting apoptosis by binging caspase-3 and caspace-7 [8]. Consequently, survivin is considered as a potential prognostic biomarker and treatment target.
However, the value of survivin in prognosis and clinicopathology of gliomas is still indefinite, and there even exist conflicts about OS, age, gender, and WHO grade in some reports [9, 10]. Some reports show that high survivin expression is associated with high grade (III+IV) of gliomas, whereas Taiichi S et al. concluded that survivin expression did not relate to high-grade gliomas [11]. Maybe many confounding factors affect the outcome of studies, such as study methods, population selected, and follow-up. Given that the meta-analysis can resolve the between-study heterogeneity, we pooled all results from published articles and systematically evaluated the expression status and implications of survivin in gliomas.
Methods
Search Strategy
A literature search was carried out using Medline, Embase, Ovid, Cnki, and Wanfang databases up to December 2013. There were no limitations of origin and languages. Subjected search terms were the following: “survivin”, “baculoviral inhibitor of apoptosis repeat-containing 5” or “BIRC5”, “gliomas [MeSH]”, “expression”, “prognosis”, or “overall survival”, etc. All references in retrieved articles were scanned to identify other potentially available reports.
Study Selection
Two reviewers independently selected eligible studies. Disagreement between the two reviewers was settled by discussion with the third reviewer. Inclusion criteria were as follows: (1) the patients were confirmed with the diagnosis of gliomas by the department of pathology; (2) the main outcome of studies concentrated on age, gender, WHO grade, and overall survival; (3) survivin expression model was identified by immunohistochemistry (IHC), western blot, or RT-PCR; (4) the value of HR/OR and 95 % CI between survivin expression and the survival status could be obtained from articles directly or calculated based on the figure and table given in articles; (5) for the duplicate articles, only the most complete and/or the recently published one was included—for one study.
Data Extraction
The following data were collected by two reviewers independently using a purpose-designed form: name of the first author, publication year, country, histology, study methods, WHO grade, patient number, mean ages, survival analysis, and follow-up time. Disagreement between two reviewers was settled by the third reviewer.
Quality Assessment
Quality assessment was conducted for eligible studies by independent reviewers by reading and scoring each publication according to the quality scale for biologically prognostic factors established by the European Lung Cancer Working Party (ELCWP) [12]. This scale evaluates the scientific design, laboratory methodology, generalizability, and result analysis. Each category could reach up to ten points, so result maximum could reach up to 40 points. Both investigators compared their calculated scores and, if necessary, achieved a consensus score for each category during a meeting. The final scores represent the percentage of the maximum of achievable scores, ranging from 0 to 100 %. Thus, higher values represent a better methodological quality.
Data Synthesis and Analysis
Survival outcome data were synthesized using the time-to-event HR as the operational measure. HR and 95 % CI have been offered directly by some included studies. As for the studies where HR and 95 % CI were not given directly, data in tables, text, or/and figures of the original papers were extracted and the HR and 95 % CI were further re-calculated by using the software SPSS13.0, Engauge Digitizer version 4.1 and the methods introduced by Tierney et al. [13] and Parmar et al. [14].
To assess heterogeneity among the studies, we used the chi-square test and Q test. If heterogeneity was significant, we used random effect model. Otherwise, we used fixed-effect model. Funnel plots of Begger’s and Egger’s linear regression test were used to investigate publication bias [15].
Sensitivity analysis was performed to examine the stability of the pooled results. Traditionally, an observed HR > 1 indicated a poor survival for patients with increased survivin expression. The effect of survivin on survival and pathology was considered as statistically significant if the corresponding 95 % CI for pooled HR/OR did not overlap 1.
All p values were two-sided, and p < 0.05 was considered as statistically significant. Statistical calculations were all performed using STATA version 11.0 and Revman 5.0.
Results
Search Results and Characteristics of Studies
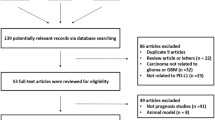
Article retrieval was conducted as shown in Fig. 1. Initially, 91 papers were retrieved. According to the title and abstract of articles, 62 articles not consistent with inclusion criteria were excluded. Then, the remaining 29 articles underwent further identification, among which 14 articles were excluded owing to review or no data (6), not related to survivin (5), and insufficient data (3). Eventually, 15 articles that met the criteria were included.

Literature search and selection of papers
The general characteristics of all 15 studies are summarized in Table 1. The total number of patients was 1,089. Fourteen studies were conducted in Asian populations; only one study was in USA populations. The percentage of positive survivin expression varies from 22.3 to 79.1 %. HRs and 95 % CIs were obtained from Kaplan–Meier curves in eight studies, and then another seven studies merely offered clinicopathological data (age, gender, or WHO grade). Patients with positive survivin were investigated more by IHC (13 studies) than by western blot (1 study) and RT-PCR (1 study). If the nucleus or cytoplasm was stained, survivin expression can be defined as positive. Some studies determined the cutoff value by score combining intensity and percentage, while others used the percentage alone.
Study Quality
Study qualities were assessed according to ELCWP. As shown in Table 2, the mean global score of the studies was 68.8 %. Across all studies, study method obtained a high mean score of 7.8 compared with design (6.5), generalizability (7.2), and results analysis (6.0). The mean global scores in Asia and non-Asia were 69.0 and 64.3 %, respectively. Studies with WHO grade did not exhibit significantly higher scores than non-WHO grade (p = 0.560).
Meta-Analysis about Survivin and 2- and 5-Year OS
As shown in Fig. 2, the pooled HR and 95 % CI about survivin and 2-year OS for all eight studies were 0.17 (95 % CI 0.11–0.26), and no significant heterogeneity was observed (χ 2 = 7.88, p = 0.344, I 2 = 11.1 %). Meanwhile, the pooled HR and 95 % CI about survivin and 5-year OS for all seven studies were 0.12 (95 % CI 0.07–0.22), and there was no significant heterogeneity observed as well (χ 2 = 5.52, p = 0.479, I 2 = 0.0 %). Both results indicated that positive survivin expression predicted poor survival in patients with gliomas (Fig. 2). As expected, significant differences were observed between 2- and 5-year OS using Student’s t test (p = 0.018), suggesting that survivin can better predict the glioma patient prognosis ranging from 2- to 5-year OS.

The individual and pooled HR with 95 % CI about survivin and OS. a A fixed-effect model revealed an association between survivin and 2-year OS (n = 8, HR 0.17, 95 % CI 0.11–0.26). b A fixed-effect model revealed an association between survivin and 5-year OS (n = 7, HR 0.12, 95 % CI 0.07–0.22). No heterogeneity was observed
Meta-Analysis about Survivin and Clinicopathological Indicators
To further identify the impact of survivin on glioma diagnosis as a biomarker, we investigated the association of survivin over-expression with age, gender, and WHO grade. A fixed-effect model revealed a significant association between survivin expression and age (≥median/+; OR 2.10, 95 % CI 1.44–3.05) and survivin and WHO grade (I+II/+; OR 0.27, 95 % CI 0.19–0.38). However, no significant association was observed between survivin and gender (male/+; OR 1.20, 95 % CI 0.81–1.79). In addition, there was no significant heterogeneity observed across all studies with p value 0.600, 0.821, and 0.752, respectively. Taken together, older age and higher grade are both associated with higher survivin expression, and high survivin expression is suggestive of a significant mark for diagnosis.
Publication Bias
In the present meta-analysis, using Begg’s and Egger’s p value test, no publication bias was observed among studies with 2-year OS (p = 0.621, 0.827) and 5-year OS (p = 0.881, 0.301), which suggested that there was no evidence of publication bias. In addition, funnel plot was also used to assess the publication bias in the studies with age, gender, and WHO grade (Fig. 3). Since the shape of the funnel plot including all studies was shown to be symmetric on the whole, the funnel plot demonstrated no publication bias.

Funnel blot was designed to visualize a potential publication bias. Funnel plots’ shape of all studies did not reveal obvious evidence of asymmetry, suggesting that publication bias was also not observed among studies with pathological indicators
Discussion
The involvement of survivin in tumorgenesis has been documented, especially in the regulation of cell proliferation and inhibition of apoptosis. Recently, it was also reported that survivin knockdown can suppress breast cancer proliferation and invasiveness [28]. Owing to its importance in cancer cell biology, survivin has been suggested as a prognostic factor and therapeutic target in other tumors, whereas it is still unclear whether survivin plays an important role in glioma diagnosis or patients prognosis. To date, there have been some controversies about the impact of survivin on gliomas.
In this meta-analysis, we included 15 relevant studies to combine the actual effects of survivin on glioma prognosis and pathology. Here quality assessment was subjected to the published ELCWP, and there was no sign of marked differences across all studies. If significant heterogeneity was observed among studies, a random-effect model, which provides a more conservative standard error and a larger confidence interval, was chosen to determine the pooled HR/OR estimates. Our analysis showed that the pooled HR and 95 % CI about 2-year OS for all eight studies were 0.17 (95 % CI 0.11–0.26) compared with 5-year OS at 0.12 (95 % CI 0.07–0.22). Furthermore, significant differences were observed between 2- and 5-year OS (p = 0.018). These suggested that survivin can better predict glioma patient prognosis from the first 2 to 5 years. On the other hand, the pooled OR and 95 % CI showed a significant association between survivin and age and WHO grade in gliomas, which implies that positive survivin expression could effectively predict the old age or high grade (III+IV) in glioma patients.
Heterogeneity was assessed by the classical Q test. When p < 0.10 and/or I 2 > 50 %, heterogeneity was considered as statistically significant. In this meta-analysis, there exists no significant heterogeneity among studies about age, gender, and WHO grade. So, a fixed-effect model was recommended in the analysis. On the other hand, several limitations of this study should be considered as many as possible. Survivin expression in included studies was mostly measured by IHC. As per traditional method, IHC depended highly on the methodological factors such as primary and secondary antibody titer. However, it was very hard to conduct subgroup analyses by different antibodies to explore the potential bias of method on the pooled results. In addition, there was also a large difference in defining the cutoff value among the studies. Until now, there were still no relevant studies to investigate the putative criteria of the positive survivin expression, which can be the cause of potential bias. In our study, the baseline level of the patients across all studies, such as age and postoperative involvement, was stable, and there was no evidence of upward or downward trends. Unfortunately, most studies did not offer complete results and data, while it may not affect the bias.
Publication bias is a major concern in systematic evaluation that may cause bias. Most studies are inclined to report positive outcomes, while the studies with negative results are often rejected [29]. In the present study, neither Egger’s and Begger’s p value test nor funnel plot implied publication bias. At the same time, it should be noted that the languages of published articles included in this meta-analysis were limited to English and Chinese, which may make other language studies that met our inclusion criteria not included.
In conclusion, survivin expression is associated with older age and higher WHO grade and acts as a significant prognostic factor for glioma patients. Thus, survivin overexpression can help us make decisions for therapeutic projects. Furthermore, prospective studies with more samples are needed, and the association with survivin and more factors like life quality, cognitive level, etc., should be also considered.
References
Louis DN, Pomeroy SL, Cairncross JG (2002) Focus on central nervous system neoplasia. Cancer Cell 1(2):125–128
Ambrosini G, Adida C, Altieri DC (1997) A novel anti-apoptosis gene, survivin, expressed in cancer and lymphoma. Nat Med 3(8):917–921
Lu B, Gonzalez A, Massion PP, Shyr Y, Shaktour B, Carbone DP, Hallahan DE (2004) Nuclear survivin as a biomarker for non-small-cell lung cancer. Brit J Cancer 91(3):537–540
Kennedy SM, O'Driscoll L, Purcell R, Fitz-Simons N, McDermott EW, Hill AD, O'Higgins NJ, Parkinson M, Linehan R, Clynes M (2003) Prognostic importance of survivin in breast cancer. Brit J Cancer 88(7):1077–1083
Montorsi M, Maggioni M, Falleni M, Pellegrini C, Donadon M, Torzilli G, Santambrogio R, Spinelli A, Coggi G, Bosari S (2006) Survivin gene expression in chronic liver disease and hepatocellular carcinoma. Hepatogastroenterology 54(79):2040–2044
Zhen HN, Zhang X, Hu PZ, Yang TT, Fei Z, Zhang JN, Fu LA, He XS, Ma FC (2005) Survivin expression and its relation with proliferation, apoptosis, and angiogenesis in brain gliomas. Cancer 104(12):2775–2783
Kajiwara Y, Yamasaki F, Hama S, Yahara K, Yoshioka H, Sugiyama K, Arita K, Kurisu K (2003) Expression of survivin in astrocytic tumors. Cancer 97(4):1077–1083
Tamm I, Wang Y, Sausville ED, Scudiero DA, Vigna N, Oltersdorf T, Reed JC (1998) IAP-family protein survivin inhibits caspase activity and apoptosis induced by Fas (CD95), Bax, caspases, and anticancer drugs. Cancer Res 58(23):5315–5320
Preusser M, Gelpi E, Matej R, Marosi C, Dieckmann K, Rössler K, Budka H, Hainfellner JA (2005) No prognostic impact of survivin expression in glioblastoma. Acta Neuropathol 109(5):534–538
Shirai K, Suzuki Y, Oka K, Noda SE, Katoh H, Suzuki Y, Itoh H, Ishiuchi S, Sakurai H, Hasegawa M, Nakano T (2009) Nuclear survivin expression predicts poorer prognosis in glioblastoma. J Neuro Oncol 91(3):353–358
Saito T, Arifin MT, Hama S, Kajiwara Y, Sugiyama K, Yamasaki F, Hidaka T, Arita K, Kurisu K (2007) Survivin subcellular localization in high-grade astrocytomas: simultaneous expression in both nucleus and cytoplasm is negative prognostic marker. J Neuro Oncol 82(2):193–198
Steels E, Paesmans M, Berghmans T, Branle F, Lemaitre F, Mascaux C, Meert AP, Vallot F, Lafitte JJ, Sculier JP (2001) Role of p53 as a prognostic factor for survival in lung cancer: a systematic review of the literature with a meta-analysis. Eur Respir J 18(4):705–719
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR (2007) Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 8(1):16
Parmar MK, Torri V, Stewart L (1998) Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med 17(24):2815–2834
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315(7109):629–634
Chakravarti A, Noll E, Black PM, Finkelstein DF, Finkelstein DM, Dyson NJ, Loeffler JS (2002) Quantitatively determined survivin expression levels are of prognostic value in human gliomas. J Clin Oncol 20(4):1063–1068
Song XB, Yuan XH, Jiang PC, Cao CJ (2003) The prognosis and clinicopathology of survivin in glioma patients. Cent Chin Med J 27(6):232–324
Jiao BH, Yao ZG, Qiu SM, Bai BZ (2004) Apoptosis in brain gliomas and expression of apoptosis related genes Fas and survivin. Chin J Neurosurg Dis Res 3(1):20–24
Xie D, Zeng YX, Wang HJ, Wen JM, Tao Y, Sham JST, Guan XY (2006) Expression of cytoplasmic and nuclear survivin in primary and secondary human glioblastoma. Brit J Cancer 94(1):108–114
Pan Y, Hu WH, Xie D, Wu HX, Xiang J, Liu YD, Wu QL, Liu YH (2006) Nuclear expression of survivin in glioma and its correlation to prognosis. Chin J Canc 25(5):635–639
Shou JX, Lin AQ, Wang XJ, Wu JX, Shan Q, Li PD, Liu Q (2006) Expression of survivin in human glioma tissue. Acta Acad Med Z 41(3):566–567
Pan Y, Hu WH, Xie D, Wu QL, Liu YH, Xiang J, Wu XH (2007) Nuclear and cytoplasmic expressions of survivin in glioma and their prognostic value. Chin Med J 87(5):325–329
Liu YF, Shi GS, Zhang S, Zhang JG, Huang H (2008) Correlation of the expression of p33/ING1 and survivin proteins with prognosis in human astrocytoma. J Mod Oncol 16(9):1490–1492
Zhang Z, Su N, Wang Z (2009) Detection of survivin and Bcl-2 in gliomas via tissue microassay. J Inn Mon Univ Nat 15(5):18–20
Kogiku M, Ohsawa I, Matsumoto K, Sugisaki Y, Takahashi H, Teramoto A, Ohta S (2008) Prognosis of glioma patients by combined immunostaining for survivin, Ki-67 and epidermal growth factor receptor. J Clin Neurosci 15(11):1198–1203
Zhen H, Zhang X, Yang T, Hu P, Fu L, Ma F, Wang X, Liang J (2005) Expression of survivin and its significance in human brain glioma. Chin J Clin Oncol 32(1):6–12
Guo D, Xin R, Liu L, Yu D, Wang Z (2004) Survivin protein expression in gliomas and its correlation with malignancy of gliomas. Acta Acad Milita Tert 26(2):162–164
Guan HT, Xue XH, Wang XJ, Li A, Qin ZY (2006) Knockdown of survivin expression by small interfering RNA suppresses proliferation of two human cancer cell lines. Chin Med Sci J 21(2):115–119
Begg CB, Berlin JA (1988) Publication bias: a problem in interpreting medical data. J R Stat Soc A 81(2):107–115
Acknowledgments
This study was supported by Shandong University Science Technology Innovation Foundation (201410422123). We greatly thank Ruiyang Yi in Sandy lab for valuable suggestions and writing.
Disclosure
The authors state that there are no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Shunzeng Lv and Congxin Dai contributed equally to this work.
An erratum to this article is available at http://dx.doi.org/10.1007/s12035-017-0402-0.
This article has been retracted at the request of the Editor-in-Chief and the Publisher. The article shows evidence of irregularities in authorship during the submission process. There is strong reason to believe that the peer review process was compromised and the authors have plagiarized parts from the following article:
Shunzeng Lv, Ekaterina Turlova, Shigang Zhao, Huihui Kang, Mingzhi Han, Hong-Shuo Sun, Prognostics and clinicopathological significance of survivin expression in bladder cancer patients: a meta-analysis. Tumor Biol. (2014) 35: 1565. doi:10.1007/s13277-013-1216-y Received: 23 July 2013
In addition, the article shows similarities with the following article which was submitted within a close timeframe:
Xiangshan Yang, Shunzeng Lv, Yuting Liu, Daotang Li, Ranran Shi, Zhenyu Tang, Jianzhen Fan, Zhongfa Xu, The Clinical Utility of Matrix Metalloproteinase 9 in Evaluating Pathological Grade and Prognosis of Glioma Patients: A Meta-Analysis. Mol Neurobiol (2015) 52: 38. doi:10.1007/s12035-014-8850-2 Received: 20 July 2014
The article “The impact of survivin on prognosis and clinicopathology of glioma patients: a systematic meta-analysis” was received on 26 June 2014.
As such the validity of the content of this article cannot be verified.
About this article

Cite this article
Lv, S., Dai, C., Liu, Y. et al. RETRACTED ARTICLE: The Impact of Survivin on Prognosis and Clinicopathology of Glioma Patients: A Systematic Meta-Analysis. Mol Neurobiol 51, 1462–1467 (2015). https://doi.org/10.1007/s12035-014-8823-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-014-8823-5