
Abstract
Geographic information systems (GIS) offer a very rich toolbox of methods and technologies, and powerful research tools that extend far beyond the mere production of maps, making it possible to cross-link and study the complex interaction of disease data and factors originating from a wide range of disparate sources. Despite their potential indispensable role in cancer prevention and control programmes, GIS are underrepresented in specialised oncology literature. The latter has provided an impetus for the current review. The review provides an eight-year snapshot of geospatial cancer research in peer-reviewed literature (2002–2009), presenting the clinico-epidemiological and methodological findings and trends in the covered corpus (93 papers). The authors concluded that understanding the relationship between location and cancer/cancer care services can play a crucial role in disease control and prevention, and in better service planning, and appropriate resource utilisation. Nevertheless, there are still barriers that hinder the wide-scale adoption of GIS and related technologies in everyday oncology practice.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Geographic Information Systems (GIS) offer a very rich toolbox of methods and technologies that extend far beyond the mere production of maps (cartography). They enable the spatial contextualisation (e.g., physical, biological, environmental, economic, demographic, ethnic, social, cultural, etc.) of health and disease data.
The traditional classification of what GIS can do in cancer and cancer care comprises two broad types of GIS applications, namely geography of disease (cancer epidemiology and outcomes in populations) and geography of healthcare systems (cancer prevention, screening and treatment/care services delivery) [1–3].
The former (geography of disease) encompasses exploration, description, and modelling activities which can include the analysis of the spatiotemporal incidence of cancer and related environmental and other place-associated phenomena, the detection and analysis of disease clusters and patterns, causality analysis, and the generation of new hypotheses. The latter (geography of healthcare systems) deals with the planning, management, and delivery of suitable cancer prevention, screening, treatment, and care services, ensuring among other things adequate and equitable patient access. This paper provides an eight-year snapshot of geospatial cancer research in peer-reviewed literature (2002–2009), presenting the clinico-epidemiological and methodological findings and trends in the covered corpus.
Methodology
Paper search and selection strategy
We searched PubMed (http://pubmed.gov/) using the following query:
(“2002/01/01”[PDat] : “2009/12/31”[PDat]) AND (“Health Place”[Journal] OR “Int J Health Geogr”[Journal] OR “Geospat Health”[Journal]) AND (neoplasms[MeSH Terms] OR cancer[All Fields] OR cancers[All Fields] OR neoplasm[All Fields] OR neoplasms[All Fields] OR oncology[All Fields] OR oncology[All Fields] OR oncologists[All Fields] OR oncological[All Fields] OR tumor[All Fields] OR tumors[All Fields] OR tumour[All Fields] OR tumours[All Fields] OR lesion[All Fields] OR lesions[All Fields] OR carcinogen[All Fields] OR carcinogens[All Fields] OR carcinogenic[All Fields] OR chronic[All Fields])
We limited our search to PubMed-indexed papers published during the period from 1 January 2002 to 31 December 2009 in only three journals that are currently fully dedicated to geospatial research in health and healthcare; namely International Journal of Health Geographics, Geospatial Health, and Health and Place.
Some relevant studies are also published in other journals not specialising in this area of interest, e.g., [4–7], but these were not included in our sample of geospatial cancer research.
Our query retrieved 128 papers in total. The retrieved articles were manually scanned to determine relevance for inclusion. Some articles (n = 45) applied one or more technique(s) directly to an oncological dataset, either in the context of a specific cancer or of an entire cancer dataset. Other articles (n = 41) focused on a method or technique in the context of a generic oncological reference (e.g., distance to cancer care centres) or examined a number of conditions, of which at least one is oncological, or focused on a non-oncological dataset but made clear and adequately relevant generalisations or references to applications to oncological datasets or cancer. We included both classes of articles in our study (n = 86).
We also came across articles (n = 10) that only vaguely referenced oncology in passing, either in their background/introduction or conclusions/discussion sections, and a considerable number of papers (n = 32) that did not contain any explicit oncology reference at all. Of these latter two types of articles (n = 42), we further identified seven papers that are relevant and of interest to our study, bringing the total number of articles included in our snapshot of geospatial cancer research to 93 papers [8–100].
Of all included studies, about 66% were conducted in the United States (this does not necessarily reflect the author’s or authors’ affiliation or geographic location).
Results
Clinico-epidemiological findings and implications
A number of cancer sites and types were covered in our selected corpus of 93 papers.
Table 1 presents a sampler of some of the main clinico-epidemiological findings and implications from the surveyed papers. Table 1 was constructed according cancer sites. Additional relevant references were cited in Table 1 to support, contrast, or discuss/contextualise the findings from our reviewed corpus of papers.
As shown in Table 1, several important clinico-epidemiological phenomena were elucidated. Geographical disparity and diversity in cancer mortality were examined for several cancer sites [8, 13, 35]. The association between cancer risk and exposure to environmental and lifestyle risk factors was examined using different techniques [11, 27, 30, 31, 33, 39, 48, 54]. Two studies examined racial differences in cancer stage at diagnosis and cancer mortality [40, 41]. Interesting relationships between socioeconomic status and self-reported health, cancer incidence, cancer stage, and cancer mortality were assessed [15, 16, 19, 24, 28, 36, 42, 47, 51]. Various GIS methods also explored cancer patterns and outcome among immigrant populations [18, 34]. Spatial and/or temporal clustering for incidence and mortality for some cancer sites was also explored in several studies [20, 21, 23, 25, 32, 45, 46, 52, 55].
Geospatial methodological findings
On data sources for geospatial cancer research
Boscoe et al. [19] provide an overview of some of the unique characteristics of spatial data, followed by an account of the major types and sources of data used in the spatial analysis of cancer, including data from cancer registries, population data, health surveys, environmental data, and remote sensing data. García-Pérez et al. [35] cover a good example of environmental data sources, namely the European Pollutant Emission Register (EPER), a public inventory of pollutant industries created by decision of the European Union. This has since been improved upon by the European Pollutant Release and Transfer Register (E-PRTR—http://ec.europa.eu/environment/air/pollutants/stationary/eper/index.htm). Such environmental data sources can prove useful for quantification of the effect of proximity to different industrial plants on cancer risk and all-cause mortality observed in nearby cities and towns. Viel et al. [96] present a good example of environmental carcinogen (dioxin) exposure modelling involving GIS.
Meteorological data can also prove very useful in cancer studies. For example, Kinoshita et al. [67] studied the geographical distribution of pancreatic cancer in relation to selected climatic factors in Japan.
On disaggregate data privacy issues
The relative rarity of cancer causes a sparse data problem for analysis, both for detecting clusters in data with high spatial variability and for communication of results without violating confidentiality and individuals’ privacy [13, 85, 101]. Confidentiality constraints often preclude the release of disaggregate data about individual cancer patients [102, 103]. Access to individually geocoded (disaggregate) data often involves lengthy and cumbersome procedures through review boards and committees for approval (and sometimes is not possible). Moreover, current data confidentiality-preserving solutions compatible with fine-level spatial analyses often lack flexibility or yield less than optimal results [102].
When data are spatially aggregated to large areas to preserve individuals’ privacy, the ability of researchers to detect disease clusters or to investigate suspected relationships between environmental exposures and disease events is affected in different ways. Exposure assessment data are generally collected for different areas than health and demographic data [102]. Kamel Boulos et al. [103] provide a comprehensive state-of-the-art review of data privacy issues (including privacy-preserving solutions and recommendations) in health GIS studies.
On the use of social deprivation indices
Many countries have their own geography-based index or indices of deprivation that are regularly updated; for example, England has ‘The English Indices of Deprivation 2007’ (http://www.communities.gov.uk/documents/communities/pdf/733520.pdf). Examples of work (from our selected corpus of 93 papers) that used such indices include the three studies by Pearce and colleagues [82–84], as well as [88].
On geocoding and choice of appropriate geographic unit of analysis
Geocoding is the process of finding-associated geographic coordinates (often expressed as latitude and longitude) from other geographic data, such as street addresses, or postal codes. With geographic coordinates, the features can be mapped and entered into GIS software and geostatistical tools for further processing and advanced visualisation. However, geocoding can prove difficult at times. The accuracy and completeness with which it is performed can vary, and this can affect the findings of spatial epidemiologic analyses and lead to bias in a study’s outcomes.
On the importance of ‘place history’ in diseases with long latency such as cancer
Most analyses of spatial clustering of disease have been based on either residence at the time of diagnosis or current residence. An underlying assumption in these analyses is that residence can be used as a proxy for environmental exposure. However, exposures earlier in life and not just those in the most recent period may be of significance [50]. Similarly, there is evidence of a contribution of early life socioeconomic exposures to the risk of chronic diseases, including cancer, in adulthood, but extant studies investigating the impact of the neighbourhood social environment on health tend to characterise only the current social environment [87]. Most cancers develop over a period of 20–30 years and are a result of multiple exposures and the interplay of external factors with the individual’s genetic susceptibility. Because latencies differ by cancer type and most likely by an individual’s susceptibility, little guidance is available for this question [85]. In breast cancer, for example, there is accumulating evidence that early life exposures may contribute to risk. In the study by Han et al. [50], examination of lifetime residential history provided additional information on geographic areas associated with higher risk.
Residential histories are increasingly available (despite complexities involved in obtaining and geocoding historical addresses [87], including data access barriers in relation to individuals’ privacy), raising the possibility of routine surveillance in a manner that accounts for individual mobility and that incorporates models of cancer latency and induction. Jacquez et al. [63, 64] developed new case-only clustering techniques that account for residential mobility, latency and induction periods, relevant covariates. In a similar vein, Rose et al. [87] argue that it should be possible in many cases to characterise the earlier social environment with known levels of measurement error and such an approach should be considered in future studies.
Spatial and aspatial statistics in geospatial cancer research
A large number of studies in our selected corpus papers used spatial and aspatial statistics in their geospatial investigation into cancer, e.g., [44, 57, 70, 80]. Goovaerts et al. [41] raise a number of salient points surrounding the selection of approaches to specific analyses.
Pearce et al. [82] used logistic regression in a study belonging to a larger project on the geography of lung cancer incidence across Scotland. The main aim of their study was to develop a technique for estimating smoking probability for different age/sex groups in small areas across the whole of Scotland using information on smoking behaviour from the Scottish Household Survey. Other studies from our selected corpus of geospatial cancer research papers that used logistic regression include [11, 22, 43, 54, 75].
Bove Jr et al. [20] used GIS in a geographically based exposure assessment to evaluate cancer risk associated with carcinogenic (or potentially carcinogenic) substances in the environment. They employed kriging, a geostatistical method to interpolate the value of a random field at an unobserved location from observations of its values at nearby locations. The disadvantages of kriging, generally speaking, include constant variance assumption and normality. Goovaerts [39] provides a creative modification and application of geostatistical techniques that have in large part been developed for, and proven in, other fields such as population ecology. Goovaerts’ proposed approach accounts for geographic heterogeneity in the population-at-risk and incorporates this information into the stabilisation of the rates and into estimates of the uncertainty through P-field simulation. Capitalising on the abundant geostatistical literature devoted to the modelling of local and spatial uncertainty, plus the recent development of Poisson kriging, Gooaverts [39] presents a novel approach, and the corresponding computer code, to generate realisations of the spatial distribution of risk values, and applies it to age-adjusted breast and pancreatic cancer mortality rates recorded for white females in 295 US counties of the North-east (1970–1994). Two important approaches exist for mapping disease rates, namely geostatistical techniques and Bayesian methods. While important theoretical work has been accomplished separately over the past decades using these two approaches, there has been a lack of synergies between them, and as a result these two approaches have grown as two different disciplines. The study by Goovaerts and Gebreab [42] represents the first work that compares these two approaches using a simulation study and cancer data sets. While any comparison studies can always be criticised (e.g., in this study the simulation method used can favour one of the methods being compared), the geostatistical approach was found to perform better than a full Bayesian approach in this paper.
Bilancia and Fedespina [17] conducted a geographical analysis of lung cancer mortality data in the Province of Lecce, Italy, during the period 1992–2001, using standard statistical methods for disease mapping. Their study offers useful insight into the geographical clustering of lung cancer in the province of Lecce, by estimating the spatial pattern of risk excess in the area and thus contributing some useful statistical evidence towards the generation of new hypotheses for further study about the possible causes for the observed pattern.
Goria et al. [45] conducted an ecological study in four French administrative departments and highlighted an excess risk in cancer morbidity for residents around municipal solid waste incinerators. Their research showed the importance of advanced GIS tools and statistical techniques to better assess weak associations between the risk of cancer and past environmental exposures. In most epidemiological studies, distance is still used as a proxy for exposure. This can lead to significant exposure misclassification. Additionally, in geographical correlation studies the non-linear relationships are usually not accounted for in the statistical analysis. In studies of weak associations, it is important to use advanced methods to better assess dose–response relationships with disease risk.
On the use of univariate vs. multi-method approaches to assess the geographic patterns of cancer
Ideally and whenever practically possible, investigators should adopt an exploratory, integrative, and multi-scalar approach when assessing geographic patterns of cancer, using a variety of techniques for geographic pattern detection at different spatial scales, as different methods will often identify different spatial patterns. Jacquez and Greiling [60, 61] demonstrated an approach employing a battery of techniques to elucidate geographic variation in cancer incidence in Long Island, New York, and to evaluate spatial association with air-borne toxics.
Complete spatial randomness (CSR) is the null hypothesis employed by many statistical tests for spatial pattern, such as local cluster or boundary analysis. CSR is however not a relevant null hypothesis for highly complex and organised systems such as those encountered in the environmental and health sciences in which underlying spatial pattern is present. Goovaerts and Jacquez [37] present a geostatistical approach to filter the noise caused by spatially varying population size and to generate spatially correlated neutral models that account for regional background obtained by geostatistical smoothing of observed mortality rates. A study of the geographical distribution of male and female lung cancer in Nassau, Queens, and Suffolk counties on Long Island, New York, USA (focusing on the same ZIP codes as in [60, 61]) was used to demonstrate this approach.
On measuring geographic access to cancer care and profiling service users
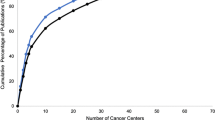
Measuring cancer care facility accessibility, e.g., using a metric such as travel time [14], becomes important when deciding on the sitting of (i.e., choosing the best location for) new cancer screening and care centres, or on the expansion or closure of existing centres, based on the profiled needs of target communities (service users) [88]. The first step in cancer control is identifying where the cancer burden is elevated, which can suggest locations where interventions are mostly needed [86].
An increasing number of studies of spatial accessibility of people to a service use GIS estimates of car travel times to the health services under examination. Haynes et al. [52] compared GIS estimates based on average car speeds on different classes of road and cancer patients’ reports of the time taken to make actual car journeys to hospital and found that the two were closely related.
Mobley et al. [76] make an important contribution to health disparities research through the use of multi-level modelling to examine variables at the macro, community, and individual levels. Their research serves to demonstrate the complexity of historical, social, economic, and cultural factors that impact health and access. They considered and evaluated the interplay between individual, social, cultural, and physical environments, concepts that are generally overlooked in other studies or considered too difficult to collect. Their study demonstrates the importance of understanding place-specific differences in access to care (the example studied in [76] is mammography use across the USA), differences that would be “averaged out” in pooled analyses. Results such as those reported by Mobley et al. can potentially affect the way that access to health services is characterised and impact decisions about service provision to better meet the needs of the public by helping decision-makers optimise their service and resource planning and management decisions.
On the art of cartography (visual communication through maps) and the use of online interactive and animated maps
To communicate population-based cancer statistics, cancer researchers have a long tradition of presenting data in a spatial representation, or map. A comprehensive review by Bell et al. [13] focuses on designing maps to communicate effectively. The biggest challenge is to ensure that maps of health statistics inform without misinforming. For example, Gelman and Price [104] have shown that plotting rates could be very misleading when sample sizes vary by area. Advances in the sciences of cartography, statistics, and visualisation of spatial data are constantly expanding the toolkit available to mapmakers to meet this challenge and avoid such pitfalls.
Cancer mortality maps are used by public health officials to identify areas of excess and to guide surveillance and control activities. Quality of decision-making thus relies on an accurate quantification of risks from observed rates which can be very unreliable when computed from sparsely populated geographical units or recorded for minority populations. Indeed, a major limitation of choropleth maps (thematic shaded or patterned maps) is the common biased visual perception that larger rural and sparsely populated areas are of greater importance. Addressing this limitation, Goovaerts [38] presents a geostatistical methodology that accounts for spatially varying population sizes and spatial patterns in the processing of cancer mortality data. His approach, described in [40], allows the continuous mapping of mortality risk, while accounting locally for population density and areal data through the coherence constraint.
Interactive Web mapping technologies are also opening up access to, and participation in, GIS and geospatial databases for much wider audiences; users only need to have a standard Web browser (some solutions also require a downloadable browser plugin) and an Internet connection [105]. Interested readers are referred to the following specialised tutorial series on ‘Web GIS in practice’, published by the International Journal of Health Geographics: http://www.ij-healthgeographics.com/series/1476-072X-Gis.
Theseira [93] describes an early (2002) example of Internet GIS for the West Midlands Region in England (the Multi-Agency Internet Geographic Information Service (MAIGIS) project) that involved cancer data. She highlights the importance of data sharing between organisations (see also [2]) and also mentions cancer data confidentiality issues in her paper. Yi et al. [99] describe a Web GIS example integrating open source technologies and public health data to create EpiVue, a Web-based cancer information system that is accessible to a wide audience through the Internet (https://epivue.cphi.washington.edu/epivue/). Bhowmick et al. [16] stress the importance of user involvement in map design and the usability aspects of maps based on their experience in developing the online Pennsylvania Cancer Atlas (http://www.geovista.psu.edu/grants/CDC/).
Vieira et al. [95] used animated maps to show spatiotemporal changes. A series of static maps was used to create a movie showing how breast cancer risk in upper Cape Cod, Massachusetts, varied as historical residences changed over space and time. Individual maps were saved as image files and used to create a storyboard in Windows Movie Maker (now known as Windows Live Movie Maker http://download.live.com/moviemaker) and generate a movie (available at http://www.biomedcentral.com/content/supplementary/1476-072X-7-46-S1.wmv) in which each map plays for 0.5 s before transitioning to the next map. Animated maps are also a feature of the Cancer Atlas Viewer, a free Windows software application for exploration of the US National Atlas of Cancer Mortality (http://www.biomedware.com/software/about_Atlas.html).
Popular and less popular software tools
ESRI ArcGIS
ArcGIS (http://www.esri.com/software/arcgis/index.html) is a popular, integrated GIS and mapping software system and components suite from Environmental Systems Research Institute, a GIS software development and services company based in Redlands, California, USA. The US National Cancer Institutes is among the very many third-party entities providing plugins that extend the core functionality of ArcGIS (http://gis.cancer.gov/nci/geovisualization.html#extensions).
Paz et al. [81] used ArcGIS software to geocode the location of the patients’ homes. They also used the ‘spatial join’ tool of the ArcGIS 9 software, which merges geographically referenced information from different geographic layers based on the spatial location of individual features in these layers. Mandal et al. [72] used Hot Spot Analysis (Getis-Ord Gi* statistic) in ArcGIS 9.3 for spatial clustering analysis of breast and prostate cancers in the continental United States between 2000 and 2005 (see http://webhelp.esri.com/arcgisdesktop/9.3/index.cfm?TopicName=Hot_Spot_Analysis_(Getis-Ord_Gi*)_(Spatial_Statistics)). McEntee and Ogneva-Himmelberger [73] also report using ArcGIS and the Gi* statistic.
Scott et al. (2002) [89] illustrate the problems of data shortage in a developing country and report using ESRI Atlas GIS v4, a now out-dated, basic Windows Desktop mapping software application (http://rpmconsulting.com/atlas/AtlasGIS4_0.pdf). ArcMap (ArcView 9.x) in the latest ArcGIS platform includes similar functionality and much more. Their paper provides a useful demonstration of GIS’ potential in the creation of a cancer information system in the context of a developing country (South Africa). Garb et al. [34], on the other hand, describe a novel and unconventional use of GIS (specifically, ArcGIS and its Web mapping component, ArcIMS—http://www.esri.com/software/arcgis/arcims/index.html) to map lesions located in body spaces rather than geographical spaces and locations on the surface of the Earth (the prefix ‘geo’ means Earth). Garb et al. used GIS to examine the findings of transanal endoscopic microsurgery (TEM), a minimally invasive procedure to locate and remove both benign and cancerous lesions of the rectum. Maps of rectal topology were developed in two and three dimensions, highlighting anatomical features of the rectum and the location of lesions found on TEM. Spatial analysis demonstrated a significant relationship between anatomical location of the lesion and procedural failure (clinical outcome). This study demonstrates the feasibility of rendering anatomical locations and clinical events in a GIS and its value in clinical research focusing on individual patients.
Other studies using ArcGIS include [25, 88, 95].
SaTScan
SaTScan™ (http://www.satscan.org/) is a free software that analyses spatial, temporal, and space–time data using the spatial, temporal, or space–time scan statistics. It is designed for any of the following interrelated purposes: (i) perform geographical surveillance of disease, to detect spatial or space–time disease clusters, e.g., of cancer cases, and to see whether they are statistically significant; (ii) test whether a disease is randomly distributed over space, over time, or over space and time; (iii) evaluate the statistical significance of disease cluster alarms; and (iv) perform repeated time-periodic disease surveillance for early detection of disease outbreaks.
A number of statistical methods for evaluating global clustering and local cluster patterns are available. Hinrichsen et al. [56] examined statistical tests for evaluating spatial clustering of disease characteristics, using prostate cancer data from Maryland Cancer Registry, USA (1992–1997). Jackson et al. [59] compared a number of such tests using a dataset of 1950–1969 lung cancer mortality in the USA and employed SaTScan in their study. Gregorio et al. [48] used SaTScan and showed how results of a spatial analysis can differ when the study geography (study area size) is altered. McLaughlin and Boscoe [74] examined the effects of randomisation methods on statistical inference in disease cluster detection using cancer datasets, with findings and recommendations for unbiased statistical inference that are applicable to popular software tools such as SaTScan. Sheehan et al. [90] carried out a study using SaTScan to determine whether observed geographic variations in breast cancer incidence in Massachusetts 1988–1997 are random or statistically significant, whether statistically significant excesses are temporary or time-persistent, and whether they can be explained by covariates such as socioeconomic status (SES) or urban/rural status. Other studies in our corpus of 93 selected papers that used SaTScan include [25, 27, 29, 32, 33, 47, 54, 55, 68, 91, 94, 98, 100].
Goovaerts [43] improves on SaTScan by providing an approach that has the potential of detecting geographic clusters that are not otherwise detected by the conventional spatial scan statistic. Chen et al. [24] address SaTScan’s lack of cartographic support for understanding clusters in their geographic context by providing an interactive visual interface to support the interpretation of SaTScan results. The geovisual analytics approach they describe in [24] facilitates the interpretation of spatial cluster detection methods by providing cartographic representation of SaTScan results and visualisation methods and tools that support selection of SaTScan parameters. Boscoe et al. [18] propose another technique for the display of results of Kulldorff’s spatial scan statistic and related cluster detection methods as a map with a nested or contoured appearance that provides a greater degree of informational content. They demonstrated their technique using prostate cancer mortality data in counties within the contiguous United States during the period 1970–1994.
BUGS and WinBUGS
BUGS (http://www.mrc-bsu.cam.ac.uk/bugs/) is an acronym standing for Bayesian inference Using Gibbs Sampling and is a flexible software for the Bayesian analysis of complex statistical models using Markov chain Monte Carlo (MCMC) methods. Chen et al. [25] used BUGS among other methods and software tools to look at the association between liver cancer and immigration in Ontario, Canada. WinBUGS (http://www.mrc-bsu.cam.ac.uk/bugs/winbugs/contents.shtml) is a version of BUGS offered as a stand-alone program (for Microsoft Windows) with a graphical user interface. Papers that used WinBUGS include [23, 30, 31, 66, 92].
Miscellaneous software tools
Nolasco et al. [77] used the R software (http://www.r-project.org/) to look at associations between mortality and socioeconomic inequalities in Spain. Wheeler [98] also used the R software, in addition to ClusterSeer (http://www.terraseer.com/products_clusterseer.php) and SaTScan, to compare cluster detection methods for childhood leukaemia incidence in Ohio, USA. Another paper using ClusterSeer is the study by Jacquez and Greiling [60], looking at breast, lung, and colorectal cancer in New York, USA. Vinnakota and Lam [97] employed a spatial data mining approach using Classification Based Association (CBA) software (http://www.comp.nus.edu.sg/~dm2/index.html) to discover associations between selected socioeconomic variables and the four most leading causes of cancer mortality in the United States between 1988 and 1992 (colorectal, lung, breast, and prostate cancers). GIS technology was used to integrate these data which were defined at different spatial resolutions, and to visualise and analyse the data mining results.
Basara and Yuan [12] investigated the relationship between environmental conditions and health outcomes in communities using the SOM-GIS (self-organising maps-GIS) method. The software implementation used by Basara and Yuan is Viscovery SOMine (http://www.viscovery.net/somine/). The self-organising map algorithm (SOM) has been applied in medical research to address the need for non-linear analytical methods to study the multifaceted aetiology of certain diseases. Kohonen developed the algorithm to search for patterns within expansive, multivariate, numerical datasets.
The ability to represent, quantify, and model individual exposure through time is a critical component of risk estimation, particularly for diseases with long latency periods (such as cancer). In response to this need, a STIS—Space Time Intelligence System—(http://www.terraseer.com/products_stis.php) has been developed by Avruskin et al. [10] to visualise and analyse objects simultaneously through space and time.
Discussion
There has long been a recognition that place matters in health, from identification of clusters of yellow fever and cholera in the nineteenth century to modern day analyses of regional and neighbourhood effects on cancer patterns using georeferenced cancer data [85]. The use of spatially referenced data in cancer studies is gaining in prominence, fuelled by the development and availability of spatial analytic and geovisualisation tools and the expansion of the linkages between geography and health [19]. The ability to evaluate geographic heterogeneity of cancer incidence and mortality is important in conducting effective cancer surveillance [59] and in developing and monitoring cancer screening programmes. Furthermore, examining geographic variation in cancer patient survival can help identify important prognostic factors that are linked by geography and generate hypotheses for further investigation into survival disparities [55]. GIS can also help in studying the geography of healthcare systems in relation to cancer and in making important service decisions to maximise resource efficiencies and ensure appropriate utilisation of services [76].
While many lessons have been learnt from the spatial analysis of cancer, there are several caveats that apply to many, if not all such analyses. These caveats such as the issue of ‘ecological fallacy’ can substantially detract from a spatial analysis and if not accounted for can lead to weakened and erroneous conclusions [2, 62]. (Ecological fallacy is a flawed interpretation of results of a study, whereby inferences about the characteristics of specific individuals are based solely upon aggregate statistics collected for the group and/or region to which those individuals belong).
Place history is of prime importance in geospatial health research, particularly in the case of diseases with long “incubation” or latency such as cancer, where the effect of risk factors in the patient’s environment might take many years to become manifest as cancer. Many geospatial studies are limited by the lack of disaggregate data and insight into individuals and their place (residential and work) histories, resulting in the wrong assumption of correlations and associations between a disease/patients and features/factors in their current place of residence and/or work at the time study data are collected, and missing the real link between the aetiopathogenesis of the disease and previous residential and work locations.
John Snow’s illustration of his theorised origin of cholera in London via a map of case residences was possible because of the large number of cases in a small geographic area with a single, precisely located exposure [1, 85]. The detection of clusters of a rare disease such as cancer requires sophisticated statistical tools that filter out potentially confounding effects of age, spatially varying population density, and mobility/place histories. Therefore, appropriate application of the statistical methods is mandatory [62, 85].
There is an increasing need for new evidence-based methods and tools that support knowledge construction (to support everyday practice) from complex geospatial datasets related to public health [3]. However, current methods and tools remain difficult for most public health and cancer practitioners to select and use, and results are also frequently difficult to interpret by them and prone to many errors and misinterpretations [2, 3].
To be successful, the design of geospatial methods and tools must be grounded in a solid understanding of the work practices within the domain of use. Bhowmick et al. [15] focused on developing that understanding through the adoption of a user-centred approach to toolset design where they investigated the work of cancer researchers and used the results of that investigation as inputs into the development of design guidelines for new geovisualisation and spatial analysis tools. They conducted key informant interviews focused on use, or potential use, of geographic information, methods, and tools and complemented this with a systematic analysis of published, peer-reviewed articles on geospatial cancer research. Results were used to characterise the typical process of analysis, to identify fundamental differences between intensive users of geospatial methods and infrequent users, and to outline key stages in analysis and tasks within the stages that methods and tools must support. Approaches and findings such as those described by Kamel Boulos [3] and Bhowmick et al. (Epub in 2007) [15] should guide future design and implementation decisions for visual and analytic tools that support cancer prevention and control research and practice.
Another problem with data on human health and cancer is that the data required for analysis are typically scattered across many distributed sources and often collected by different groups and agencies (data sharing difficulties and need for data sharing agreements between different organisations and data custodians) [2, 85]. Accumulating and validating data required for analysis from these multiple sources might take longer than the analysis itself [85].
NAACCR and NCI (United States)
As hinted to above, the full support of cancer dataset custodians (organisations collecting and overseeing such datasets) is also of prime importance in enabling the full realisation of the vision described in [3, 15]. In the United States, the North American Association of Central Cancer Registries, Inc. (NAACCR) established a GIS Ad Hoc Committee to address the appropriate uses of GIS in cancer registry practice (see http://www.naaccr.org/committees/gis). The Committee has published a number of very highly recommended key practical handbooks, including ‘Using Geographic Information Systems Technology in the Collection, Analysis, and Presentation of Cancer Registry Data: A Handbook of Best Practices’ (http://www.naaccr.org/filesystem/pdf/GIS%20handbook%206-3-03.pdf), ‘A Geocoding Best Practices Guide’ (http://www.naaccr.org/filesystem/pdf/Geocoding_Best_Practices.pdf), and a ‘Review of Cluster Analysis Software (http://www.naaccr.org/filesystem/pdf/Final%20Report%20Cluster%20Software%202004-09-27%20rev.pdf).
The US National Cancer Institute (NCI) has been equally active in relation to GIS use in cancer research and practice (see http://gis.cancer.gov/). NCI’s GIS-related applications span GIS database development (e.g., GIS for Breast Cancer Studies on Long Island–LI GI http://li-gis.cancer.gov/), spatial data analysis (covering environmental exposure assessment, statistical modelling, outlier detection for cancer surveillance and cluster identification using tools such as SaTScan), geovisualisation tools development (e.g., http://gis.cancer.gov/nci/geovisualization.html#extensions), and communication of georeferenced statistics (State Cancer Profiles http://statecancerprofiles.cancer.gov and Cancer Mortality Atlas http://www3.cancer.gov/atlasplus/). Moreover, NCI offers funding for GIS grants (http://cancercontrol.cancer.gov/grants/portfolio.asp?codename=spatial/gis%20models) and in 2002, sponsored a meeting of geospatial practitioners and statisticians to develop a series of articles describing the current best practices in the analysis of spatial data [86]. These articles were published in International Journal of Health Geographics [13, 19, 62, 85, 86].
Conclusions
Understanding the relationship between location and cancer/cancer care services can play a key role in disease control and prevention, and in better service planning, and appropriate resource utilisation. Although there are still many barriers, technical (e.g., ease-of-use and interpretation, while avoiding misinformation) and organisational (e.g., data collection, access and sharing; other data issues related to individuals’ privacy and mobility/residential histories), hindering the wide-scale adoption of GIS and related technologies in everyday practice of the health sector, the situation is gradually improving (e.g., NAACCR and NCI activities).
The authors would very much like to see follow-on snapshot papers on specific cancer types (e.g., geospatial research in breast cancer), perhaps also incorporating further data from additional papers published outside our three chosen journals (e.g., [4–7]) and also covering additional years (e.g., 1995–2001 and 2010 (e.g., [146])).
References
Kamel Boulos MN, Roudsari AV, Carson ER. Health geomatics: an enabling suite of technologies in health and healthcare. J Biomed Inf. 2001;34(3):195–219.
Kamel Boulos MN. Towards evidence-based, GIS-driven national spatial health information infrastructure and surveillance services in the United Kingdom. Int J Health Geogr. 2004;3(1):1.
Kamel Boulos MN. Research protocol: EB-GIS4HEALTH UK—foundation evidence base and ontology-based framework of modular, reusable models for UK/NHS health and healthcare GIS applications. Int J Health Geogr. 2005;4(1):2.
Guajardo OA, Oyana TJ. A critical assessment of geographic clusters of breast and lung cancer incidences among residents living near the Tittabawassee and Saginaw Rivers, Michigan, USA. J Environ Public Health. 2009;2009:316249.
Cornelis C, Schoeters G, Kellen E, Buntinx F, Zeegers M. Development of a GIS-based indicator for environmental pesticide exposure and its application to a Belgian case-control study on bladder cancer. Int J Hyg Environ Health. 2009;212(2):172–85.
Hopfer S, Chadwick AE, Parrott RL, Ghetian CB, Lengerich EJ. Assessment of training needs and preferences for geographic information systems (GIS) mapping in state comprehensive cancer-control programs. Health Promot Pract. 2009;10(4):579–87.
Wu KS, Huo X, Zhu GH. Relationships between esophageal cancer and spatial environment factors by using geographic information system. Sci Total Environ. 2008;393(2–3):219–25.
Altmayer CA, Hutchison BG, Torrance-Rynard VL, Hurley J, Birch S, Eyles JD. Geographic disparity in premature mortality in Ontario, 1992–1996. Int J Health Geogr. 2003;2(1):7.
Argeseanu Cunningham S, Ruben JD, Narayan KM. Health of foreign-born people in the United States: a review. Health Place. 2008;14(4):623–35.
Avruskin GA, Jacquez GM, Meliker JR, Slotnick MJ, Kaufmann AM, Nriagu JO. Visualization and exploratory analysis of epidemiologic data using a novel space time information system. Int J Health Geogr. 2004;3(1):26.
Barry J, Breen N. The importance of place of residence in predicting late-stage diagnosis of breast or cervical cancer. Health Place. 2005;11(1):15–29.
Basara HG, Yuan M. Community health assessment using self-organizing maps and geographic information systems. Int J Health Geogr. 2008;7:67.
Bell BS, Hoskins RE, Pickle LW, Wartenberg D. Current practices in spatial analysis of cancer data: mapping health statistics to inform policymakers and the public. Int J Health Geogr. 2006;5:49.
Berke EM, Shi X. Computing travel time when the exact address is unknown: a comparison of point and polygon ZIP code approximation methods. Int J Health Geogr. 2009;8:23.
Bhowmick T, Griffin AL, MacEachren AM, Kluhsman BC, Lengerich EJ. Informing geospatial toolset design: understanding the process of cancer data exploration and analysis. Health Place. 2008;14(3):576–607.
Bhowmick T, Robinson AC, Gruver A, MacEachren AM, Lengerich EJ. Distributed usability evaluation of the Pennsylvania Cancer Atlas. Int J Health Geogr. 2008;7:36.
Bilancia M, Fedespina A. Geographical clustering of lung cancer in the province of Lecce, Italy: 1992–2001. Int J Health Geogr. 2009;8:40.
Boscoe FP, McLaughlin C, Schymura MJ, Kielb CL. Visualization of the spatial scan statistic using nested circles. Health Place. 2003;9(3):273–7.
Boscoe FP, Ward MH, Reynolds P. Current practices in spatial analysis of cancer data: data characteristics and data sources for geographic studies of cancer. Int J Health Geogr. 2004;3(1):28.
Bove GE Jr, Rogerson PA, Vena JE. Case control study of the geographic variability of exposure to disinfectant byproducts and risk for rectal cancer. Int J Health Geogr. 2007;6:18.
Bovell-Benjamin AC, Hathorn CS, Ibrahim S, Gichuhi PN, Bromfield EM. Healthy food choices and physical activity opportunities in two contrasting Alabama cities. Health Place. 2009;15(2):429–38.
Campbell RT, Li X, Dolecek TA, Barrett RE, Weaver KE, Warnecke RB. Economic, racial and ethnic disparities in breast cancer in the US: towards a more comprehensive model. Health Place. 2009;15(3):870–9.
Catelan D, Biggeri A. A statistical approach to rank multiple priorities in environmental epidemiology: an example from high-risk areas in Sardinia, Italy. Geospat Health. 2008;3(1):81–9.
Chen J, Roth RE, Naito AT, Lengerich EJ, MacEachren AM. Geovisual analytics to enhance spatial scan statistic interpretation: an analysis of U.S. cervical cancer mortality. Int J Health Geogr. 2008;7:57.
Chen Y, Yi Q, Mao Y. Cluster of liver cancer and immigration: a geographic analysis of incidence data for Ontario 1998–2002. Int J Health Geogr. 2008;7:28.
Collins DC, Kearns RA, Mitchell H. “An integral part of the children’s education”: placing sun protection in Auckland primary schools. Health Place. 2006;12(4):436–48.
DeChello LM, Sheehan TJ. The geographic distribution of melanoma incidence in Massachusetts, adjusted for covariates. Int J Health Geogr. 2006;5:31.
DeChello LM, Gregorio DI, Samociuk H. Race-specific geography of prostate cancer incidence. Int J Health Geogr. 2006;5:59.
DeChello LM, Sheehan TJ. Spatial analysis of colorectal cancer incidence and proportion of late-stage in Massachusetts residents: 1995–1998. Int J Health Geogr. 2007;6:20.
Downing A, Forman D, Gilthorpe MS, Edwards KL, Manda SO. Joint disease mapping using six cancers in the Yorkshire region of England. Int J Health Geogr. 2008;7:41.
Dreassi E, Lagazio C, Maule MM, Magnani C, Biggeri A. Sensitivity analysis of the relationship between disease occurrence and distance from a putative source of pollution. Geospat Health. 2008;2(2):263–71.
Ed HC, Jacobson H, Soto MF. Evaluating the disparity of female breast cancer mortality among racial groups—a spatiotemporal analysis. Int J Health Geogr. 2004;3(1):4.
Fukuda Y, Umezaki M, Nakamura K, Takano T. Variations in societal characteristics of spatial disease clusters: examples of colon, lung and breast cancer in Japan. Int J Health Geogr. 2005;4:16.
Garb JL, Ganai S, Skinner R, Boyd CS, Wait RB. Using GIS for spatial analysis of rectal lesions in the human body. Int J Health Geogr. 2007;6:11.
Garcia-Perez J, Boldo E, Ramis R, Vidal E, Aragones N, Perez-Gomez B, Pollan M, Lopez-Abente G. Validation of the geographic position of EPER-Spain industries. Int J Health Geogr. 2008;7:1.
Glover TD, Parry DC. A third place in the everyday lives of people living with cancer: functions of Gilda’s Club of Greater Toronto. Health Place. 2009;15(1):97–106.
Goovaerts P, Jacquez GM. Accounting for regional background and population size in the detection of spatial clusters and outliers using geostatistical filtering and spatial neutral models: the case of lung cancer in Long Island, New York. Int J Health Geogr. 2004;3(1):14.
Goovaerts P. Geostatistical analysis of disease data: estimation of cancer mortality risk from empirical frequencies using Poisson kriging. Int J Health Geogr. 2005;4:31.
Goovaerts P. Geostatistical analysis of disease data: visualization and propagation of spatial uncertainty in cancer mortality risk using Poisson kriging and p-field simulation. Int J Health Geogr. 2006;5:7.
Goovaerts P. Geostatistical analysis of disease data: accounting for spatial support and population density in the isopleth mapping of cancer mortality risk using area-to-point Poisson kriging. Int J Health Geogr. 2006;5:52.
Goovaerts P, Meliker JR, Jacquez GM. A comparative analysis of aspatial statistics for detecting racial disparities in cancer mortality rates. Int J Health Geogr. 2007;6:32.
Goovaerts P, Gebreab S. How does Poisson kriging compare to the popular BYM model for mapping disease risks? Int J Health Geogr. 2008;7:6.
Goovaerts P. Visualizing and testing the impact of place on late-stage breast cancer incidence: a non-parametric geostatistical approach. Health Place. 2010;16(2):321–30.
Gorey KM, Luginaah IN, Hamm C, Fung KY, Holowaty EJ. Breast cancer care in the Canada and the United States: ecological comparisons of extremely impoverished and affluent urban neighborhoods. Health Place. 2010;16(1):156–63.
Goria S, Daniau C, de Crouy-Chanel P, Empereur-Bissonnet P, Fabre P, Colonna M, Duboudin C, Viel JF, Richardson S. Risk of cancer in the vicinity of municipal solid waste incinerators: importance of using a flexible modelling strategy. Int J Health Geogr. 2009;8:31.
Gotay CC, Shimizu H, Muraoka M, Ishihara Y, Tsuboi K, Ogawa H. Health attitudes and behaviors: comparison of Japanese and Americans of Japanese and European Ancestry. Health Place. 2004;10(2):153–61.
Gregorio DI, DeChello LM, Samociuk H, Kulldorff M. Lumping or splitting: seeking the preferred areal unit for health geography studies. Int J Health Geogr. 2005;4(1):6.
Gregorio DI, Samociuk H, DeChello L, Swede H. Effects of study area size on geographic characterizations of health events: prostate cancer incidence in Southern New England, USA, 1994–1998. Int J Health Geogr. 2006;5:8.
Grubesic TH, Matisziw TC. On the use of ZIP codes and ZIP code tabulation areas (ZCTAs) for the spatial analysis of epidemiological data. Int J Health Geogr. 2006;5:58.
Han D, Rogerson PA, Bonner MR, Nie J, Vena JE, Muti P, Trevisan M, Freudenheim JL. Assessing spatio-temporal variability of risk surfaces using residential history data in a case control study of breast cancer. Int J Health Geogr. 2005;4(1):9.
Hao Y, Ward EM, Jemal A, Pickle LW, Thun MJ. U.S. congressional district cancer death rates. Int J Health Geogr. 2006;5:28.
Haynes R, Jones AP, Sauerzapf V, Zhao H. Validation of travel times to hospital estimated by GIS. Int J Health Geogr. 2006;5:40.
Henry KA, Boscoe FP. Estimating the accuracy of geographical imputation. Int J Health Geogr. 2008;7:3.
Henry KA, Sherman R, Roche LM. Colorectal cancer stage at diagnosis and area socioeconomic characteristics in New Jersey. Health Place. 2009;15(2):505–13.
Henry KA, Niu X, Boscoe FP. Geographic disparities in colorectal cancer survival. Int J Health Geogr. 2009;8:48.
Hinrichsen VL, Klassen AC, Song C, Kulldorff M. Evaluation of the performance of tests for spatial randomness on prostate cancer data. Int J Health Geogr. 2009;8:41.
Hunter PR, Izsak J, Nehaul L. Changes of neoplasm concentration with geographical co-ordinates. Health Place. 2003;9(4):305–13.
Iredale R, Jones L, Gray J, Deaville J. ‘The edge effect’: an exploratory study of some factors affecting referrals to cancer genetic services in rural Wales. Health Place. 2005;11(3):197–204.
Jackson MC, Huang L, Luo J, Hachey M, Feuer E. Comparison of tests for spatial heterogeneity on data with global clustering patterns and outliers. Int J Health Geogr. 2009;8:55.
Jacquez GM, Greiling DA. Local clustering in breast, lung and colorectal cancer in Long Island, New York. Int J Health Geogr. 2003;2(1):3.
Jacquez GM, Greiling DA. Geographic boundaries in breast, lung and colorectal cancers in relation to exposure to air toxics in Long Island, New York. Int J Health Geogr. 2003;2(1):4.
Jacquez GM. Current practices in the spatial analysis of cancer: flies in the ointment. Int J Health Geogr. 2004;3(1):22.
Jacquez GM, Meliker JR, Avruskin GA, Goovaerts P, Kaufmann A, Wilson ML, Nriagu J. Case-control geographic clustering for residential histories accounting for risk factors and covariates. Int J Health Geogr. 2006;5:32.
Jacquez GM, Meliker J, Kaufmann A. In search of induction and latency periods: space-time interaction accounting for residential mobility, risk factors and covariates. Int J Health Geogr. 2007;6:35.
Jacquez GM, Rommel R. Local indicators of geocoding accuracy (LIGA): theory and application. Int J Health Geogr. 2009;8:60.
Johnson GD. Small area mapping of prostate cancer incidence in New York State (USA) using fully Bayesian hierarchical modelling. Int J Health Geogr. 2004;3(1):29.
Kinoshita S, Wagatsuma Y, Okada M. Geographical distribution for malignant neoplasm of the pancreas in relation to selected climatic factors in Japan. Int J Health Geogr. 2007;6:34.
Klassen AC, Kulldorff M, Curriero F. Geographical clustering of prostate cancer grade and stage at diagnosis, before and after adjustment for risk factors. Int J Health Geogr. 2005;4(1):1.
Kobetz E, Daniel M, Earp JA. Neighborhood poverty and self-reported health among low-income, rural women, 50 years and older. Health Place. 2003;9(3):263–71.
Kravdal O. Does place matter for cancer survival in Norway? a multilevel analysis of the importance of hospital affiliation and municipality socio-economic resources. Health Place. 2006;12(4):527–37.
Lopez-Zetina J, Lee H, Friis R. The link between obesity and the built environment. Evidence from an ecological analysis of obesity and vehicle miles of travel in California. Health Place. 2006;12(4):656–64.
Mandal R, St-Hilaire S, Kie JG, Derryberry D. Spatial trends of breast and prostate cancers in the United States between 2000 and 2005. Int J Health Geogr. 2009;8:53.
McEntee JC, Ogneva-Himmelberger Y. Diesel particulate matter, lung cancer, and asthma incidences along major traffic corridors in MA, USA: a GIS analysis. Health Place. 2008;14(4):817–28.
McLaughlin CC, Boscoe FP. Effects of randomization methods on statistical inference in disease cluster detection. Health Place. 2007;13(1):152–63.
McNamara B, Rosenwax L. Factors affecting place of death in Western Australia. Health Place. 2007;13(2):356–67.
Mobley LR, Kuo TM, Driscoll D, Clayton L, Anselin L. Heterogeneity in mammography use across the nation: separating evidence of disparities from the disproportionate effects of geography. Int J Health Geogr. 2008;7:32.
Nolasco A, Melchor I, Pina JA, Pereyra-Zamora P, Moncho J, Tamayo N, Garcia-Senchermes C, Zurriaga O, Martinez-Beneito MA. Preventable avoidable mortality: evolution of socioeconomic inequalities in urban areas in Spain, 1996–2003. Health Place. 2009;15(3):732–41.
Nummela O, Sulander T, Rahkonen O, Karisto A, Uutela A. Social participation, trust and self-rated health: a study among ageing people in urban, semi-urban and rural settings. Health Place. 2008;14(2):243–53.
Oliver MN, Matthews KA, Siadaty M, Hauck FR, Pickle LW. Geographic bias related to geocoding in epidemiologic studies. Int J Health Geogr. 2005;4:29.
Ott JJ, Paltiel AM, Winkler V, Becher H. The impact of duration of residence on cause-specific mortality: a cohort study of migrants from the Former Soviet Union residing in Israel and Germany. Health Place. 2010;16(1):79–84.
Paz S, Linn S, Portnov BA, Lazimi A, Futerman B, Barchana M. Non-Hodgkin Lymphoma (NHL) linkage with residence near heavy roads—a case study from Haifa Bay, Israel. Health Place. 2009;15(2):636–41.
Pearce J, Boyle P, Flowerdew R. Predicting smoking behaviour in census output areas across Scotland. Health Place. 2003;9(2):139–49.
Pearce J, Boyle P. Examining the relationship between lung cancer and radon in small areas across Scotland. Health Place. 2005;11(3):275–82.
Pearce J, Barnett R, Kingham S. Slip! Slap! Slop! Cutaneous malignant melanoma incidence and social status in New Zealand, 1995–2000. Health Place. 2006;12(3):239–52.
Pickle LW, Waller LA, Lawson AB. Current practices in cancer spatial data analysis: a call for guidance. Int J Health Geogr. 2005;4(1):3.
Pickle LW, Szczur M, Lewis DR, Stinchcomb DG. The crossroads of GIS and health information: a workshop on developing a research agenda to improve cancer control. Int J Health Geogr. 2006;5:51.
Rose KM, Wood JL, Knowles S, Pollitt RA, Whitsel EA, ez Roux AV, Yoon D, Heiss G. Historical measures of social context in life course studies: retrospective linkage of addresses to decennial censuses. Int J Health Geogr. 2004;3(1):27.
Sauerzapf VA, Jones AP, Haynes R, Crawford SM, Forman D. Travel time to radiotherapy and uptake of breast-conserving surgery for early stage cancer in Northern England. Health Place. 2008;14(3):424–33.
Scott D, Curtis B, Twumasi FO. Towards the creation of a health information system for cancer in KwaZulu-Natal, South Africa. Health Place. 2002;8(4):237–49.
Sheehan TJ, DeChello LM, Kulldorff M, Gregorio DI, Gershman S, Mroszczyk M. The geographic distribution of breast cancer incidence in Massachusetts 1988 to 1997, adjusted for covariates. Int J Health Geogr. 2004;3(1):17.
Sheehan TJ, DeChello LM. A space-time analysis of the proportion of late stage breast cancer in Massachusetts, 1988 to 1997. Int J Health Geogr. 2005;4:15.
Sturtz S, Ickstadt K. A descriptive and model-based spatial comparison of the standardised mortality ratio and the age-standardised mortality rate. Geospat Health. 2007;1(2):255–66.
Theseira M. Using Internet GIS technology for sharing health and health related data for the West Midlands Region. Health Place. 2002;8(1):37–46.
Tian N, Gaines WJ, Benjamin ZF. Female breast cancer mortality clusters within racial groups in the United States. Health Place. 2010;16(2):209–18.
Vieira VM, Webster TF, Weinberg JM, Aschengrau A. Spatial-temporal analysis of breast cancer in upper Cape Cod, Massachusetts. Int J Health Geogr. 2008;7:46.
Viel JF, Clement MC, Hagi M, Grandjean S, Challier B, Danzon A. Dioxin emissions from a municipal solid waste incinerator and risk of invasive breast cancer: a population-based case-control study with GIS-derived exposure. Int J Health Geogr. 2008;7:4.
Vinnakota S, Lam NS. Socioeconomic inequality of cancer mortality in the United States: a spatial data mining approach. Int J Health Geogr. 2006;5:9.
Wheeler DC. A comparison of spatial clustering and cluster detection techniques for childhood leukemia incidence in Ohio, 1996–2003. Int J Health Geogr. 2007;6:13.
Yi Q, Hoskins RE, Hillringhouse EA, Sorensen SS, Oberle MW, Fuller SS, Wallace JC. Integrating open-source technologies to build low-cost information systems for improved access to public health data. Int J Health Geogr. 2008;7:29.
Yiannakoulias N. Using population attributable risk to understand geographic disease clusters. Health Place. 2009;15(4):1142–8.
Curtis AJ, Mills JW, Leitner M. Spatial confidentiality and GIS: re-engineering mortality locations from published maps about Hurricane Katrina. Int J Health Geogr. 2006;5:44.
Kamel Boulos MN, Cai Q, Padget JA, Rushton G. Using software agents to preserve individual health data confidentiality in micro-scale geographical analyses. J Biomed Inform. 2006;39(2):160–70.
Kamel Boulos MN, Curtis AJ, AbdelMalik P. Musings on privacy issues in health research involving disaggregate geographic data about individuals. Int J Health Geogr. 2009;8:46.
Gelman A, Price PN. All maps of parameter estimates are misleading. Stat Med. 1999;18(23):3221–34.
Kamel Boulos MN. Chapter 49: Principles and techniques of interactive Web cartography and Internet GIS (in addition to contributions to companion DVD). In: M Madden, editor. Manual of geographic information systems. Bethesda: ASPRS—American Society for Photogrammetry and Remote Sensing; 2009. p. 935–974. (ISBN: 1-57083-086-X)—URL:http://www.asprs.org/gis_manual/index.html.
Andolhe R, Guido LA, Bianchi ER. Stress and coping in perioperative period of breast cancer. Revista da Escola de Enfermagem de USP. 2009;43:711–20.
Vodermaier A, Linden W, Siu C. Screening for emotional distress in cancer patients: a systematic review of assessment instruments. J Natl Cancer Inst. 2009;101:1464–88.
Alexander DD, Cushing CA. Quantitative assessment of red meat or processed meat consumption and kidney cancer. Cancer Detect Prev. 2009;32:340–51.
Hamashima C, Saito H, Sobue T. Awareness of and adherence to cancer screening guidelines among health professionals in Japan. Cancer Sci. 2007;98:1241–7.
Miyazaki K, Sato J, Mukohara K, Kitamura K, Saito S, Ban N. Attitudes of Japanese primary care physicians toward publicly endorsed periodic health examinations: a cross sectional survey. Asian Pac J Cancer Prev. 2007;8:258–62.
Sprague B, Ramchandani R, Trentham-Dietz A, Newcomb P, Gangnon R, Remington P, Hampton J. Socioeconomic status and survival after an invasive breast cancer diagnosis. Cancer Epidemiol Biomarkers Prev. 2010;19:892.
Artinyan A, Mailey B, Sanchez-Luege N, Khalili J, Sun CL, Bhatia S, Wagman LD, Nissen N, Coloquhoun SD, Kim J. Race, ethnicity, and socioeconomic status influence the survival of patients with hepatocellular carcinoma in the United States. Cancer. 2010;116(5):1367–77.
Baker KS, Davies SM, Majhail NS, Hassebroek A, Klein JP, Ballen KK, Bigelow CL, Frangoul HA, Hardy CL, Bredeson C, Dehn J, Friedman D, Hahn T, Hale G, Lazarus HM, LeMaistre CF, Loberiza F, Maharaj D, McCarthy P, Setterholm M, Spellman S, Trigg M, Maziarz RT, Switzer G, Lee SJ, Rizzo JD. Race and socioeconomic status influence outcomes of unrelated donor hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2009;15:1543–54.
Coughlin SS, Ekwueme DU. Breast cancer as a global health concern. Cancer Epidemiol. 2009;33:315–8.
McDonald JT, Neily J. Race, immigrant status, and cancer among women in the United States. J Immigr Minor Health 2009 (in press).
Lee J, Demissie K, Lu SE, Rhoads GG. Cancer incidence among Korean-American immigrants in the United States and native Koreans in south Korea. Cancer Control. 2007;14:78–85.
Bidoli E, Franceschi S, Montella M. Cancer mortality by urbanization and proximity to the sea coast in Campania Region, southern Italy. Tumori. 1998;84:460–6.
Heintz NH, Janssen-Heininger YM, Mossman BT. Asbestos, lung cancers, and mesotheliomas: from molecular approaches to targeting tumor survival pathways. Am J Respir Cell Mol Biol. 2010;42(2):133–9.
Tomasetti M, Amati M, Santarelli L, Alleva R, Neuzil J. Malignant mesothelioma: biology, diagnosis and therapeutic approaches. Curr Mole Pharmacol. 2009;2:190–206.
Driece HA, Siesling S, Swuste PH, Burdorf A. Assessment of cancer risks due to environmental exposure to asbestos. J Expo Sci Environ Epidemiol. 2010;20(5):478–85.
Cokkinides V, Bandi P, McMahon C, Jemal A, Glynn T, Ward E. Tobacco control in the United States—recent progress and opportunities. CA: Cancer J Clin. 2009;59:352–65.
Finney Rutten LJ, Augustson EM, Moser RP, Beckjord EB, Hesse BW. Smoking knowledge and behavior in the United States: sociodemographic, smoking status, and geographic patterns. Nicotine Tob Res. 2008;10:1559–70.
Irvin Vidrine J, Reitzel LR, Wetter DW. The role of tobacco in cancer health disparities. Curr Oncol Rep. 2009;11:457–81.
Schnelzer M, Hammer GP, Kreuzer M, Tschense A, Grosche B. Accounting for smoking in the radon-related lung cancer risk among German uranium miners: results of a nested case-control study. Health Phys. 2010;98(1):20–8.
Pukkala E, Martinsen JI, Lynge E, Gunnarsdottir HK, Sparen P, Tryggvadottir L, Weiderpass E, Kjaerheim K. Occupation and cancer-follow-up of 15 million people in five Nordic countries. Acta Oncol. 2009;48(5):646–790.
El-Serag HB, Lau M, Eschbach K, Davila J, Goodwin J. Epidemiology of hepatocellular carcinoma in Hispanics in the United States. Arch Intern Med. 2007;167:1983–9.
Kato I, Yee CL, Ruterbusch J, Schwartz K. Patterns of cancer in first generation immigrants from the Arab league and other countries. J Registry Manag. 2009;36:71–6. quiz 101-102.
Nasseri K, Mills PK, Allan M. Cancer incidence in the Middle Eastern population of California, 1988–2004. Asian Pac J Cancer Prev. 2007;8:405–11.
Walega P, Kenig J, Richter P, Nowak W. Functional and clinical results of transanal endoscopic microsurgery combined with endoscopic posterior mesorectum resection for the treatment of patients with t1 rectal cancer. World J Surg 2010 (in press) [Epub ahead of print].
Grant WB. An estimate of premature cancer mortality in the U.S. due to inadequate doses of solar ultraviolet-B radiation. Cancer. 2002;94:1867–75.
Niu X, Pawlish KS, Roche LM. Cancer survival disparities by race/ethnicity and socioeconomic status in New Jersey. J Health Care Poor Underserved. 2010;21(1):144–60.
Short LJ, Fisher MD, Wahl PM, Kelly MB, Lawless GD, White S, Rodriguez NA, Willey VJ, Brawley OW. Disparities in medical care among commercially insured patients with newly diagnosed breast cancer: opportunities for intervention. Cancer. 2010;116(1):193–202.
Celaya MO, Rees JR, Gibson JJ, Riddle BL, Greenberg ER. Travel distance and season of diagnosis affect treatment choices for women with early-stage breast cancer in a predominantly rural population (United States). Cancer Causes Control. 2006;17(6):851–6.
Yu XQ. Socioeconomic disparities in breast cancer survival: relation to stage at diagnosis, treatment and race. BMC Cancer. 2009;9:364.
Chan MY, Huang H, Leung LK. 2, 3, 7, 8-Tetrachlorodibenzo-para-dioxin increases aromatase (CYP19) mRNA stability in MCF-7 cells. Mol Cell Endocrinol. 2010;317(1–2):8–13.
Heffernan AE, O’Sullivan A. Pediatric sun exposure. Nurse Pract 1998;23:67–68, 71–78, 83–86.
Torrens R, Swan BA. Promoting prevention and early recognition of malignant melanoma. Dermatol Nurs. 2009;21:115–22. quiz 123.
Zimmerman L, Britton K. Prevention through vigilance: malignant melanoma management. Nurs Manag. 2009;40:26–9. quiz 30.
Rebbeck TR. Genetics, disparities, and prostate cancer. LDI Issue Brief. 2005;10:1–4.
Williams H, Powell IJ. Epidemiology, pathology, and genetics of prostate cancer among African Americans compared with other ethnicities. Methods Mol Biol. 2009;472:439–53.
Meliker JR, Slotnick MJ, Avruskin GA, Schottenfeld D, Jacquez GM, Wilson ML, Goovaerts P, Franzblau A, Nriagu JO. Lifetime exposure to arsenic in drinking water and bladder cancer: a population-based case-control study in Michigan, USA. Cancer Causes Control. 2010;21(5):745–57.
Gulis G, Czompolyova M, Cerhan JR. An ecologic study of nitrate in municipal drinking water and cancer incidence in Trnava District, Slovakia. Environ Res. 2002;88(3):182–7.
Grant WB. Ecologic studies of solar UV-B radiation and cancer mortality rates. Recent Results Cancer Res. 2003;164:371–7.
Grant WB. Epidemiology of disease risks in relation to vitamin D insufficiency. Prog Biophys Mol Biol. 2006;92(1):65–79.
Whitworth KW, Symanski E, Coker AL. Childhood lymphohematopoietic cancer incidence and hazardous air pollutants in southeast Texas, 1995–2004. Environ Health Perspect. 2008;116:1576–80.
St-Hilaire S, Mannel S, Commendador A, Mandal R, Derryberry D. Correlations between meteorological parameters and prostate cancer. Int J Health Geogr. 2010;9:19.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boulos, D.N.K., Ghali, R.R., Ibrahim, E.M. et al. An eight-year snapshot of geospatial cancer research (2002–2009): clinico-epidemiological and methodological findings and trends. Med Oncol 28, 1145–1162 (2011). https://doi.org/10.1007/s12032-010-9607-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12032-010-9607-z