
Abstract
To investigate the expressions of PIM-1 and hK2 mRNA in normal prostate, benign prostatic glandular hyperplasia (BPH), and prostate cancer (PCa), and to explore the association of PIM-1 and hK2 expressions with PCa progression. The samples were harvested from 37 patients with BPH, 23 patients with PCa, and three with normal prostate tissues. Total RNA was extracted from their prostate tissues and analyzed for PIM-1 and hK2 mRNA levels using SYBR green I-based quantitative real-time RT-PCR (QRT-PCR) assays and Southern blot analysis. The differences of gene expressions were calculated based on standard curve. Quantitative expressions of PIM-1 and hK2 mRNA in normal prostate, BPH, and PCa were 1.05 ± 0.04, 2.57 ± 0.74, 4.45 ± 0.63, and 1.02 ± 0.03, 2.264 ± 0.46, 5.905 ± 0.78, respectively. PIM-1 and hK2 were expressed higher in PCa than those in BPH and normal prostate tissues, the differences among which had statistic significance (P < 0.05). Our results support the hypothesis that PIM-1 and hK2 play a significant role in the growth of PCa and the detection of PIM-1 and hK2 mRNA expressions by QRT-PCR provided more reliable and helpful information on diagnosis, treatment, and prognosis of PCa.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In both Europe and the United States, prostate carcinoma (PCa) is the most frequently diagnosed tumor among adult males [1]. Over the past years, incidence of PCa has been on the rise in China; thus the identification of high-risk patients and the prediction of tumor aggressiveness have a great importance for prognosis [2].
PIM-1, an oncogenic serine-threonine kinase of an ill-defined function that has been implicated in lymphomagenesis, plays an important role in apoptosis, proliferation and differentiation of cell, and progression of cancer [3, 4]. It is widely expressed in tissues, with the highest expression found in hematopoietic tissues and testes, and can be induced by a number of cytokines in hematopoietic cells where it enhances cellular survival. Recently, when differentiate expression of PIM-1 in normal prostate and PCa was analyzed by gene chip analysis, over-expression of PIM-1 in PCa has been demonstrated [5, 6]. Human glandular kallikrein (hK2) is an androgen-regulated protein that has high identity with prostate-specific antigen (PSA) and is expressed almost exclusively in prostatic epithelial cells [7, 8]. Although the expression of PSA has been found to be reduced in higher grade and presumably more biologically active disease, the expression of hK2 has been found to increase gradually from benign epithelium to prostatic intraepithelial neoplasia and to prostate cancer. Furthermore, hK2 expression was directly associated with the Gleason grade of the primary tumor, and foci of prostate cancer metastatic to the lymph nodes have been found to demonstrate the highest level of expression [9, 10].
Quantitative real-time RT-PCR (QRT-PCR) is a highly sensitive technique to detect small quantities of mRNA within the peripheral blood, within other body fluids, or tissues. RT-PCR is superior to cytology and immunological approaches in sensitivity and specificity for detecting disseminated cells in peripheral blood [11, 12]. Therefore, in this study we examined the expression of two established molecular markers—PIM-1 and hK2 in the prostate tissues of 37 patients with benign prostatic hyperplasia (BPH), and of 23 patients with PCa for preoperative staging and exploring clinical significance of PIM-1 and hK2 in PCa diagnosis.
Materials and methods
Cases selection
In this study, 23 patients with biopsy-proven PCa (mean age was 70.16 ± 1.29) and 37 patients with biopsy-proven BPH (mean age was 67.18 ± 2.76) treated at the Urology Department of First Municipal People’s Hospital in Guangzhou Medical College were enrolled. In addition three healthy volunteers (mean age was 35.72 ± 2.01 years), without prior history of a malignancy or any urological disease, were recruited as control.
Design of oligonucleotide primers
The Sequences of normal mRNA of PIM-1, hK2, and β-actin gene were obtained from GeneBank in NCBI (National Center for Biotechnology Information) website, and were used to design the primers PIM-1 (F: 5′-ACG CTT GCT CTG TTT GTG G-3′, R: 5′-CTG GAA GGC ACA CCA TCC-3′, 184 bp), hK2 (F: 5′-TCT GTA ATG GTG TGC TTC AAG G-3′, R: 5′-GTG TCC AGC ATC CAG AAA GG-3′, 218 bp), and β-actin (F: 5′-ACT GGA ACG GTG AAG GTG ACA G-3′, R: 5′-GGT GGC TTT TAG GAT GGC AAG-3′, 161 bp). The melting temperature (T m) was estimated by using the formulae of Thomas and Dancis, and Lathe [13]. Relative T m values obtained using 0.3 M as a standard salt concentration helped to design pairs of primers with similar high melting temperatures. The presence of primer dimmers was discarded by analysis of the melting curve in RT-PCR using Cycler IQ software (Bio-Rad Laboratories, Hercules, CA). The designed oligonucleotides were synthesized by SBS Genetech (Beijing, China).
Sample preparation and RNA extraction
Prostate tissue samples obtained from all the cases mentioned above were stored in liquid nitrogen until RNA extraction. Informed consent was obtained from the subjects, and the study was approved by the Zhongshan University Ethics Committee. In all the cases, PCa or BPH was confirmed by pathological diagnosis. Patients undergoing androgen deprivation therapy were excluded from this study. In addition, patients were not permitted to receive androgen-associated treatments or to undergo rectal touching one week prior to sample collection. Total RNA was isolated using TRIZOL reagent (Invitrogen, Madison, US). Samples were diluted in DEPC and supplemented with protease inhibitors (Takara Biotechnology, Dalian, China) prior to storage at −70°C.
Quantitative real time RT-PCR
Single-stranded cDNAs were generated using Superscript II reverse transcriptase (Invitrogen) as per the manufacturer’s directions. In brief, reverse transcription of 2 μg of DNase-I-treated RNA was performed in a 20 μl reaction mixture containing 0.75 μl oligodT, 1 μl Primer Mix (10 mM, reaction concentration was 0.4 mM), 0.25 μl random hexamer, 4 μl 5 × Reaction Buffer, 0.5 μl RNase Inhibitor (Takara Biotechnology), 4 μl dNTP (10 mM), and 1 μl MMLV reverse transcriptase (Promega, Madison, USA).
Quantitative Real-time PCR experiments were performed on a RotorGene 2000 system (Corbett Research, Mortlake, Australia), using SYBR Green PCR Master Mix according to the manufacturer’s protocol (Shanghai Kaifang S&T Company, Shanghai, China). Using β-actin plasmid DNA constructed by us as a positive control and based on 10 times concentration gradients, fluorogenic quantitative PCR was performed between 2 and 20,000 μg/l concentration gradients. The amount of target gene expression was extrapolated from the standard curve and normalized to β-actin. Data were analyzed using Rotor-Gene v5.0 (Corbett Research).
PCR was carried out in 25 μl reaction mixture containing 1 μl cDNA, 2 μl primers, 1.25 μl 20 × SYBR Green I, 0.5 μl 50 × Rox Dye (Invitrogen), 2.5 μl 10 × PCR Buffer (mM MgCl2), 1 μl Mg2+ (25 mmol/l), 2 μl dNTP Mix (2.5 mmol/l per nucleotide), and 0.125 μl Hot Star Taq E (Takara Biotechnology). The thermal cycling conditions were as follows: 4 min at 94°C, 20 s at 94°C, and 20 s at 55°C (35 cycles), and 72°C for 40 s. Duplicate PCR amplifications were performed for each sample.
Southern blot analysis
Genomic DNA was isolated from prostate tissues of all the cases mentioned above by standard methodology [14]. Specific antisense oligonucleotide probes (PIM-1: 5′-CAT CCG CGT CTC CGA CAA CTT GC-3′; hK2: 5′-GCT AGA GCT TAC TCT GA-3′; Clontech, USA) were end-labeled using T4 polynucleotide kinase (Boehringer Mannheim GmbH) and [γ-32P] ATP (Bhabha Atomic Research Centre, India), and used for Southern hybridization. Following agarose gel electrophoresis, DNA was denatured in 0.5 M NaOH and 0.15 M NaCI for 30 min, neutralized for 30 min in Tris-saline buffer (1.5 M Tris-HC1 and 0.15 M NaC1, pH 7.5), blotted by the capillary blot method on Nytran membranes (pore size, 0.22 μm), UV-cross-linked at 254 nm for 2 min, and dried at 80°C for 1 h. The dried membrane was subjected to prehybridization in a solution containing 6× saline-sodium citrate (SSC), 10 mM EDTA (pH 7.5), 2× Denhardt’s solution, 100 μg/ml denatured DNA, and 0.5% SDS for 1 h at 55°C. After adding the labeled probes, the membranes were further incubated at 55°C for 16 h. The membranes were washed in 2 × SSC and 0.05% SDS for 30 min at room temperature and for 20 min at 55°C. They were exposed to X-ray film for 1–2 h and developed.
Statistical analysis
Statistical package SPSS12.0 (SPSS incorporate, Chicago) was used for all analyses. Chi-square test was used for comparison of categorical variables. P < 0.05 was accepted as level of statistical significance. All data are expressed as mean ± SD \( \left( {\overline{X} \pm s} \right) \).
Results
Drawing standard curve
The mean critical threshold (Ct) values for β-actin plasmid DNA concentrations ranging from 0.005 pg to 500 ng per reaction were shown in Table 1 and Fig. 1. Based on the relationship between concentration of β-actin plasmid DNA and Ct value, a standard curve was obtained by software Rotor-Gene 5.0. β-actin plasmid DNA concentrations and Ct values were highly correlated (r = 0.991) (Fig. 2).

Determination of detection limit of PCR for β-actin cDNA. Dilution experiments carried out with 0.5, 0.05, 0.005 ng/reaction, 0.5, 0.05, 0.005,0.0005 pg/reaction of the β-actin plasmid cDNA (from lane 1 to lane 8). QRT-PCR assay results are reproducibly sensitive to at least six copies of PSA cDNA. The lane marked M is molecular weight marker

FQ-PCR standard curve of β-actin plasmid cDNA
Quantitative expressions of PIM-1 and hK2 mRNA in different prostate tissues
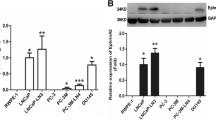
In order to examine the tissue-specific distribution of PIM-1 and hK2 mRNAs in different prostate tissues, we performed Quantitative Real-time RT-PCR and Southern blot analyses. The PIM-1 and hK2 mRNAs showed dominant expression in the PCa tissues (Figs. 3, 4), whereas lower levels were detected in BPH and normal prostate tissues. The expression of β-actin mRNA was detected as an internal standard. The mean PIM-1 and hK2 mRNA levels in tissues from patients with PCa (N = 23) and BPH (N = 37) are shown in Table 2. All values are expressed relative to those in tissues from healthy individuals (N = 3). The quantity expressions of PIM-1 mRNA in normal, BPH, and PCa groups were 1.05 ± 0.04, 2.57 ± 0.75, and 4.45 ± 0.63, respectively, and showed significant differences among three groups (P = 0.0230, 0.0071). On the other hand, PCa tissues were found to express hK2 mRNA in dramatic ally higher levels than BPH and normal tissues (P = 0.0127, 0.0068). On the other hand, the differences in the expression levels of hK2 mRNA between BPH and normal prostate tissues had no statistic significance (Table 3).

SYBR green I-based quantitative RT-PCR analysis of the gene expression in different groups. β-actin was used as an internal standard. M, marker; PIM-1 (184 bp), hK2 (218 bp), and β-actin (161 bp) expressions in prostatic tissues of BPH and PCa group were shown as indicated in the figure

Southern blot analyses of PIM-1 and hK2 expressions in prostate tissues of PCa and BPH cases. The PCR signals are verified by Southern hybridization with PIM-1 and hK2-specific oligonucleotide probes, respectively. M, Marker; lanes 1 and 2 refer to PIM-1 (184 bp) expressed in PCa and BPH tissues, respectively; lanes 3 and 4 refer to hK2 (218 bp) expressed in PCa and BPH tissues, respectively
Discussion
Over the past years, there has been a substantial increase in incidence of PCa among the Chinese males. Thus, early diagnosis and treatment is the key to determine prognosis of PCa. Prostate specific antigen (PSA) as a biomarker for PCa has been widely recognized in clinical practices [15]. However, serum PSA has proven to be an inaccurate diagnostic tool, particularly within the gray zone ranging from 4 to 10 ng/ml, where BPH is often misdiagnosed as PCa at higher serum PSA levels [16]. Adding to the lack of specificity of this marker, PSA levels are known to increase with age in healthy men. Ostrander et al. found that PSA levels increase by 0.04 ng/ml per year in men aged above 60 years [17]. Furthermore, BPH patients on non-surgical treatments may show artificially suppressed serum level of PSA, which would potentially mask the concurrent or subsequent presence of PCa. Therefore, more precise diagnostic approaches are needed for the early diagnosis of PCa and for guiding the clinical management of this disease [18].
It has been suggested that PIM-1, as an important component of signal transduction pathway of cell proliferation, involves in inhibiting cell apoptosis accompanied by anti-apoptosis molecule bcl-2 and Gfi-1 [19, 20]. PIM-1 also promotes formation of important complex via phosphorylation during mitosis. In progression of prostate carcinoma, PIM-1 might transform prostate epithelial into carcinoma cell by combining and activating c-Myb, and inhibiting apoptosis. Overexpression of PIM-1 protein kinase is probably the main transduction pathway in tumorigenesis and progression of PCa. These findings have great significance for exploring progression of prostate carcinoma and improving therapeutic regimen of patients.
hK2 is one of the three serine proteases encoded by the human glandular kallikrein (hK) gene family. Consisting of 287 amino acids and with a 79% amino acid sequence similarity to PSA, hK2 is secreted by prostate epithelia [19, 20]. The mRNAs of both hK2 and PSA are up regulated by androgen and progestogen [21, 22]. It has been demonstrated that serum hK2 levels are more sensitive than serum PSA levels in diagnosing PCa [23]. Consistent with these findings, our data revealed that higher hK2 expression correlates more with cancerous prostate tissue than with benign prostate tissue. As a new detectable serine protease, hK2, due to its specificity in molecular structure, in-vivo distribution, and metabolism, has been showing to be a promising potential in early diagnosis, pathological classification, metastasis monitoring, and the evaluation of chemotherapeutic prognosis of prostate carcinoma [24]. However, studies employing larger sample sizes will be necessary to confirm the utility of hK2 before it is widely implemented in a clinical setting. Nevertheless, it has already been clearly demonstrated that combining hK2 with other PCa serum markers such as total and free PSA, using a multielemental data aggregate analysis method, significantly increases the sensitivity and specificity of early PCa diagnosis and markedly improves PCa management [25, 26].
A cost-effective RT-PCR assay based on SYBR green I has been developed in this study for detecting the gene expression in samples from PCa, BPH, and normal control cases. This panning system only reports the quantitative status of the sample as either positive or negative for PIM-1 and hK2. It could be completed in 1 h and has been a rapid method allowing the fast detection and confirmation of target genes in clinical samples. The use of SYBR green had reduced our material costs for diagnosis by half compared with other methods that used probes. It has been demonstrated that the SYBR green RT-PCR displayed equal or higher sensitivity than the probe-based multiplex assays when RNA, prepared from viruses grown in cell culture or from clinical samples was used as a template. However, using DNA construction as a template rendered the SYBR green assays to become equally or less sensitive (by 1 log unit) than the probe-based multiplex assays [27]. This is likely due to the fact that the optimization of the assays was performed on RNA prepared from viruses grown in cell culture or from clinical samples, and the assays may not be optimal for plasmids isolated from bacterial cell culture. From the results, we found that the expressions of PIM-1 and hK2 mRNA were higher in PCa than those in normal tissue (NT) and BPH, which suggested that PIM-1 and hK2 can be used as diagnostic markers for PCa. Of note, RT-PCR with fluorescent detection, such as has been employed here, not only increases the specificity in detecting substrate, but also allows for the quantification of substrate [28]. Furthermore, because this technique has no use for post-treatment of PCR products, it decreased the possibility of cross contamination of samples.
In conclusion, PIM-1 and hK2 mRNA, as measured by SYBR green I-based RT-PCR, may be useful adjuvant markers for the diagnosis, treatment, and monitoring of PCa. Future studies will be necessary to understand whether PIM-1 and hK2 will be effective in evaluating the management and prognosis of PCa.
References
Kurek R, Nunez G, Tselis N. Prognostic value of combined “triple”-reverse transcription-PCR analysis for prostate-specific antigen, human kallikrein 2, and prostate-specific membrane antigen mRNA in peripheral blood and lymph nodes of prostate cancer patients. Clin Cancer Res. 2004;9(10):5808–14.
Shariat SF, Gottenger E, Nguyen C. Preoperative blood reverse transcriptase-PCR assays for prostate-specific antigen and human glandular kallikrein for prediction of prostate cancer progression after radical prostatectomy. Cancer Res. 2002;62:5974–9.
Zeping W, Bhattacharya N, Weaver M. PIM-1 a serine/threonine kinase with a role in cell survival, proliferation, differentiation and tumorigenesis. Vet Sci. 2001;2(3):167–9.
Wen M, Zhou LQ, Wang JW. Expression of PIM-1 in human prostate cancer. Basic Clin Med. 2005;25:503–6.
Cibull TL, Jones TD, Li L. Overexpression of PIM-1 during progression of prostatic adenocarcinoma. J Clin Pathol. 2006;59(3):285–8. doi:10.1136/jcp.2005.027672.
Bachmann M, Moroy T. The serine/threonine kinase PIM-1. Int J Biochem Cell Biol. 2005;37(4):726–30. doi:10.1016/j.biocel.2004.11.005.
Vaisanen V, Eriksson S, Ivaska KK. Development of sensitive immunoassays for free and total human glandular kallikrein 2. Clin Chem. 2004;50(9):1607–17. doi:10.1373/clinchem.2004.035253.
Yousef GM, Diamandis EP. Expanded human tissue kallikrein family—a novel panel of cancer biomarkers. Tumour Biol. 2002;23(3):185–92. doi:10.1159/000064027.
Slawin KM. Detection of metastatic prostate cancer using a splice variant specific reverse transcriptase-polymerase chain reaction assay for human glandular kallikrein. Cancer Res. 2000;60:7142–8.
Martin BJ, Finlay JA, Sterling K. Early detection of prostate cancer in African-American men through use of multiple biomarkers: human kallikrein 2 (hK2), prostate-specific antigen (PSA), and free PSA (fPSA). Prostate Cancer Prostatic Dis. 2004;7(2):132–7. doi:10.1038/sj.pcan.4500706.
Nolan T, Hands RE, Bustin SA. Quantification of mRNA using real-time RT-PCR. Nat Protoc. 2006;1(3):1559–82. doi:10.1038/nprot.2006.236. 2006.
Bonnet-Duquennoy M, Abaibou H, Tailhardat M. Study of housekeeping gene expression in human keratinocytes using OLISA, a long-oligonucleotide microarray and q RT-PCR. Eur J Dermatol. 2006;16(2):136–40.
Stahl DA, Amann R. Development and application of nucleic acid probes. In: Stackebrandt E, Goodfellow M, editors. Nucleic acid techniques in bacterial systematics. Chichester, United Kingdom: Wiley; 1991. p. 205–48.
Sambrook J, Fritsch EF, Maniatis T. Molecular cloning: a laboratory manual. 2nd ed. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory; 1989.
Thomas J, Gupta M, Grasso Y. Preoperative combined nested reverse transcriptase polymerase chain reaction for prostate-specific antigen and prostate-specific membrane antigen does not correlate with pathologic stage or biochemical failure in patients with localized prostate cancer undergoing radical prostatectomy. J Clin Oncol. 2002;20:3213–8. doi:10.1200/JCO.2002.11.097.
Ciatto S. Reliability of PSA testing remains unclear. BMJ. 2003;327(7417):750.
Camici M. Prostate cancer and prostate specific antigen screening. Minerva Med. 2004;95(1):25–34.
Sokoloff MH, Yang XJ, Fumo M. Characterizing prostatic adenocarcinomas in men with a serum prostate specific antigen level of <4.0 ng/ml. BJU Int. 2004;93(4):499–502. doi:10.1111/j.1464-410X.2003.04657.x.
So A, Goldenberg L, Gleave ME. Prostate specific antigen: an updated review. Can J Urol. 2003;10(6):2040–50.
Haese AC, Noldus J. Human glandular kallikrein 2: a potential serum for predicting the organ confined versus nonorgan confined growth of prostate cancer. Urol. 2000;163:1491–7. doi:10.1016/S0022-5347(05)67649-5.
Ostrander EA, Stanford JL. Genetics of prostate cancer: too many loci, too few genes. Am J Hum Genet. 2000;67(6):1367–75. doi:10.1086/316916.
Hessels D, Verhaegh GW, Schalken JA. Applicability of biomarkers in the early diagnosis of prostate cancer. Expert Rev Mol Diagn. 2004;4(4):513–26. doi:10.1586/14737159.4.4.513.
Obiezu CV, Diamandis EP. Human tissue kallikrein gene family: applications in cancer. Cancer Lett. 2005;224(1):1–22.
Becker C, Piironen T, Pettersson K, Hugosson J, Lilja H. Testing in serum for human glandular kallikrein 2, and free and total prostate specific antigen in biannual screening for prostate cancer. J Urol. 2003;170(4 Pt 1):1169–74. doi:10.1097/01.ju.0000086640.19892.0b.
Haese A, Graefen M, Palisaar J. Serum markers for early detection and staging of prostate cancer Status report on current and future markers. Urologe A. 2003;42(9):1172–87. doi:10.1007/s00120-003-0430-4.
Shah JB, Reese AC, McKiernan JM. PSA updated: still relevant in the new millennium? Eur Urol. 2005;47(4):427–32. doi:10.1016/j.eururo.2004.12.020.
Lai Y-L, Chung Y-K, Tan H-C, Yap H-F, Yap G, Ooi E-E, et al. Cost-effective real-time reverse transcriptase PCR (RT-PCR) to screen for dengue virus followed by rapid single-tube multiplex RT-PCR for serotyping of the virus. J Clin Microbiol. 2007;45(3):935–41. doi:10.1128/JCM.01258-06.
Espy MJ, Uhl JR, Sloan LM. Real-time PCR in clinical microbiology: applications for routine laboratory testing. Clin Microbiol Rev. 2006;19(1):165–256. doi:10.1128/CMR.19.1.165-256.2006.
Acknowledgments
This study was supported by grants from the Natural Science Foundation of Guangdong Province (No. 04003650), the Key Programs of Science and Technology of Guangzhou city (No. 200323-E4053), and the Key Programs of Science and Technology of Health Bureau of Guangzhou city.
Author information
Authors and Affiliations
Corresponding author
Additional information
Hui-chan He and Xue-cheng Bi contributed equally to this article.
Rights and permissions
About this article
Cite this article
He, Hc., Bi, Xc., Zheng, Zw. et al. Real-time quantitative RT-PCR assessment of PIM-1 and hK2 mRNA expression in benign prostate hyperplasia and prostate cancer. Med Oncol 26, 303–308 (2009). https://doi.org/10.1007/s12032-008-9120-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12032-008-9120-9