
Abstract
Background
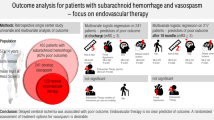
Primary angioplasty has been introduced for the treatment of symptomatic cerebral vasospasm in patients with subarachnoid hemorrhage (SAH). The data regarding the therapeutic benefit of angioplasty in improving patient outcomes are limited, hence its utilization at hospitals remains controversial and currently is not reimbursed by Medicare or major insurance companies.
Methods
We analyzed the data from Nationwide Inpatient Sample (NIS), a nationally representative dataset of all admissions in the United States from 2005 to 2007. We analyzed the prevalence of angioplasty procedure for cerebral vasospasm at the national level. In-hospital mortality, discharge status, length of stay, and cost of hospitalization were compared between hospitals performing angioplasty with those not performing angioplasty in multivariable model, adjusted for patient’s age, utilization of endovascular aneurysm obliteration, and disease severity.
Results
Of the 74,356 estimated patients with nontraumatic SAH, 47% (n = 35,172) were admitted to hospitals that perform angioplasty for cerebral vasospasm and only 1307 patients (3.8%) were treated with angioplasty for vasospasm. In multivariable analysis, after adjustment for patient and hospital characteristics, we found that patients admitted to hospitals performing angioplasty had higher rates of discharge to home without supervision (OR 1.3, 95% CI: 1.1–1.6). There was no difference in in-hospital mortality, length of stay, or cost of hospitalization.
Conclusions
Our analysis suggests that the odds of a patient being discharged to home are better at hospitals performing angioplasty for cerebral vasospasm. Provision of angioplasty may be used as a surrogate marker of model of care in management of patients with SAH.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
It has been more than two decades since Zubkov et al. [1] described the use of angioplasty for treatment of cerebral vasospasm associated with subarachnoid hemorrhage (SAH), followed by a report by Newell et al. [2] which demonstrated feasibility, safety, and angiographic efficacy of angioplasty for symptomatic vasospasm. The high rate of angiographic and clinical improvements after angioplasty have been reported in several studies, however, there is a lack of prospective randomized trials except for a trial evaluating prophylactic angioplasty which did not show any definite improvement in outcome [3].
Currently angioplasty for vasospasm has been incorporated with varying levels of enthusiasm in many institutions based on indirect evidence of angiographic and clinical improvement. The current guidelines by the American Heart Association/American Stroke Association for management of aneurysmal SAH state that cerebral angioplasty may be reasonable after, together with, or in the place of triple-H therapy, depending on the clinical scenario (Class IIb, Level of Evidence B) [4]. The current Medicare policy (NCD) for angioplasty effective from 6 November 2006 does not cover angioplasty for vasospasm related to SAH [5]. In addition, policies of major insurance companies also consider angioplasty with or without stenting of intracranial arteries only experimental and investigational [6, 7]. The current prevalence of this procedure at the national level is not known.
SAH related outcome is multi-factorial, primarily determined by the severity of the initial bleeding. Subsequent outcome is not only determined by the occurrence of complications such as vasospasm and hydrocephalus but also the institutional factors and availability of resources critical to patient care. There is no consensus on the ideal “model of care” at the institutional level in the management of such patients; however, there are certain institutional factors which appear to improve the outcomes of these patients. These include high patient volume, availability of experienced cerebrovascular surgeons, and availability of endovascular and neurocritical care services [4, 8–11]. In this “model of care” with multiple components with overlapping elements, it is very difficult to determine the effect of angioplasty procedure alone on the final outcome of such patients. We considered provision of angioplasty at an institution to be a marker of skilled endovascular services and an independent but important component of model of care in such patients when they develop vasospasm. Our objective was not to measure the efficacy of the procedure alone, but to compare the outcomes at institution level. We analyzed the Nationwide Inpatient Sample (NIS) institution level data from 2005 to 2007 to study the effect of intracranial angioplasty in SAH related vasospasm.
Methods
We compared the rates of variables of interest between hospitals performing intracranial angioplasty with those hospitals not performing angioplasty. In our analysis, we focused on comparison among institutions rather than among individuals since the safety and efficacy of new therapy will be reflected in overall outcomes at the institution provided the sampling period is adequate. Differences in institutional patient populations may still produce bias, but these differences are expected to be smaller [12].
Database Characteristics
We used NIS data from 2005 to 2007, for patients aged 18 years or older. NIS database is one of the Healthcare Cost and Utilization Projects sponsored by the Agency for Healthcare Research and Quality (AHRQ) [13]. The NIS is the largest all-payer inpatient care database in the United States that analyzes national trends in health care utilization, access, charges, quality, and outcomes based on data extracted from approximately 5–8 million hospital stays representing approximately a 20% stratified sample of U.S. community hospitals per year. Each year, hospitals within a stratum have an equal probability of selection for the sample, regardless of whether they appeared in a prior sample. Detailed information on the design of the NIS is available at http://www.hcup-us.ahrq.gov.
Identification of Patients and Procedures
Diagnostic code fields were screened for International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code 430 to identify patients with SAH as primary diagnoses. Patients with head trauma (secondary diagnosis of ICD-9-CM 800.0–801.9, 803.0–804.9, 850.0–854.1, 873.0–873.9), arteriovenous malformation or fistula (ICD-9-CM 747.81), or treatment diagnosis for arteriovenous malformation repair or radiosurgery (ICD-9-CM 39.53 or 92.30) were excluded from analysis of SAH. The procedures for treatment included ICD-9-CM 39.51 (clipping of aneurysm) and ICD-9-CM 39.52 (other surgical repair including wrapping), or ICD-9-CM 39.72 (endovascular repair of an aneurysm). We used ICD-9-CM procedure codes to identify hospitals performing angioplasty for vasospasm with treatment codes ICD-9-CM 00.62 (percutaneous angioplasty of intracranial vessel(s)) and/or ICD-9-CM 39.50 (angioplasty or atherectomy of other non-coronary vessel(s)).
ICD-9-CM 00.62 was introduced in October 2004 by the Centers for Medicare and Medicaid Services (CMS). Wevalidated the accuracy of ICD-9 code 00.62 by using a prospectively collected log of the endovascular procedures from 2005 to 2008 at our center. A sensititvity of 80% and specificity of 100% was observed. After including ICD-9 code 39.50 (angioplasty or atherectomy of other non-coronary vessel(s)), [10] sensitivity was 100%, with a specificity of 100%.
Classification of Hospitals Based on Availability of Angioplasty Procedure
Hospitals were classified as “angioplasty provider” for the year and subsequent years when a procedure (ICD-9 0.62 and/or ICD-9 39.50) was identified in one or more patients. Therefore, a hospital can be classified as “no angioplasty” in 1 year and as an angioplasty hospital in the following years if that hospital performed any angioplasty in subsequent years.
Predictor Variables and Outcomes
The variables abstracted were patients’ age, gender, race/ethnicity, procedures performed (endovascular embolization, surgical treatment, and angioplasty), procedure-related complications, hospital characteristics in which they were treated (rural, urban non-teaching, urban teaching hospitals), length of stay, and total cost of hospitalization. The NIS defines an urban hospital as one located in a metropolitan statistical area and a teaching hospital as one with American Medical Association approved residency program and either membership in the Council of Teaching Hospitals or a ratio of full-time equivalent interns and residents to beds of 0.25 or higher. The outcomes of interest were discharge destination (home without special care versus other as a surrogate of good outcome), in-hospital mortality, length of hospitalization (continuous endpoint), and cost of hospitalization (continuous endpoint).
Determination and Adjustment of Disease Severity
Due to non-availability of SAH specific disease severity scales (Hunt and Hess scale, Glasgow Coma Scale, or World Federation of Neurosurgical Societies) in the NIS data, we used 3M Health Information Systems All Patient Refined Diagnosis Related Group (3M APR-DRG) mortality risk algorithm as a surrogate marker of disease severity. The 4-point ordinal variable (mild, moderate, severe, and extreme) for risk-for-mortality of disease is based on patient’s age and primary and secondary diagnoses; additional adjustment is for in-hospital procedures. This algorithm has been demonstrated to be a reliable and valid risk-of-mortality adjustment system [14].
Statistical Analysis
We used the SAS 9.1 software (SAS Institute Inc., Cary, NC) to convert raw counts generated from the NIS database into weighted counts that we used to generate national estimates. The statistical analyses were performed based on these weighted numbers and incorporated the complex sampling of NIS, following HCUP recommendations [13]. We used the chi-square test for categorical data and analysis of variance for continuous data. To account for the effect of inflation on hospital charges, we used data from the Bureau of Labor Statistic’s medical care component of the Consumer Price Index (CPI) and presented the data in 2007 US dollars. (http://www.bls.gov/cpi/). In addition, we converted hospital charges into hospital costs using the cost-to-charge ratio (CCR) estimates. CCR estimates are constructed using all-payer, inpatient cost and charge information from the detailed reports by hospitals to the CMS. Outcomes of interest were compared between hospitals performing intracranial angioplasty with those admitted to hospitals not performing angioplasty and were compared in two multivariable models: Model 1, including patient characteristics such as age (continuous variable), aneurysm obliteration (surgical, endovascular, or none) and disease severity (four grades); and Model 2, including hospital characteristics (bed size and teaching/location) and SAH case volume at the hospital, in addition to patient characteristics. For differences in length of stay and hospitalization cost, we analyzed outcomes in natural log scale and retransformed to present geometric means.
Results
A total of 74,356 patients with non traumatic SAH were admitted over a 3 years period. This represents the total national estimate derived from the NIS data set. Out of these patients, 47% (35,172) were admitted to hospitals that performed angioplasty for cerebral vasospasm in U.S hospitals between 2005 and 2007. Out of these 35,172 non traumatic SAH admissions at the hospitals performing angioplasty, only 1307 patients (3.8%) were treated with angioplasty for vasospasm related to SAH. A total of 5320 hospitals were analyzed and among those only 452 (8%) of the hospitals had performed angioplasty.
A comparison of basic characteristics between hospitals performing angioplasty for cerebral vasospasm and hospitals not performing angioplasty is provided in Table 1.
Patients in hospitals performing angioplasty for vasospasm were more likely to be younger and women. Patients in hospitals that provided angioplasty for vasospasm also had a higher proportion of both endovascular aneurysm obliteration and surgical clipping procedures. Distribution of disease severity was significantly different between patients in hospitals performing angioplasty and hospitals not performing angioplasty. Hospitals performing angioplasty had overall a lower proportion of patients with the moderate disease severity category and a higher proportion of patients with the highest disease severity category.
Hospitals that performed angioplasty for vasospasm included a higher proportion of high volume hospitals and teaching hospitals (P < 0.0001). Median SAH case volume at the hospitals performing angioplasty was 382 compared to 83 at the hospitals not performing angioplasty. Almost all the hospitals providing angioplasty also provided endovascular embolization procedure compared with 40% of hospitals offering endovascular embolization but not offering angioplasty.
Analysis of Outcome Variables
In univariate analysis, hospitals performing angioplasty had a higher proportion of patients discharged to home without special care compared with hospitals without any provision of angioplasty (see Table 1). Hospital mortality was lower in the hospitals performing angioplasty compared with the hospitals not performing angioplasty. However, hospitals performing angioplasty had a longer duration of mean hospital stay and higher mean costs of hospitalization.
In multivariable model (see Table 2), after adjusting for important predictors of outcomes, patients admitted to hospitals performing angioplasty had higher rates of discharge to home in both models previously described in the Method section. In-hospital mortality was lower in Model 1; however, after adjusting for hospital characteristics, in-hospital mortality decrease was not statistically significant. The length of stay precentage difference was 35% in Model 1, but it was not significant in Model 2. The difference in the cost of hospitalization also decreased when we estimated using Model 1; however, after adjusting in Model 2 the differences were not statistically significant. Tables 3 and 4 further elaborate on Model 2, demonstrating the differential effect of each variable. Factors favorably affecting a patient discharged home include hospitals providing angioplasty, large volume hospital, provision of endovascular embolization, younger age, and lower disease severity. However, in-hospital mortality was mainly affected by disease severity and increased age. Cost of hospitalization was mainly affected by disease severity, age increment by every 5 years, endovascular embolization procedure, hospital volume, teaching status of hospital, and increased SAH case volume. Length of stay was primarily affected by teaching status, SAH case volume, hospital with endovascular embolization provision, disease severity, and increasing age.
Discussion
Johnston [10] has demonstrated a 16% reduction in risk of in-hospital death at institutions that used angioplasty for vasospasm, in a study of 9,534 SAH admissions within 70 centers in the University Health Systems Consortium from 1994 through 1997. In that analysis, angioplasty was used only in about 2% of cases. Only 8% of hospitals in the United States performed angioplasty from 2005 to 2007. Even though about 47% (n = 35,172) of patients were admitted to these hospitals, only 1307 patients (3.8%) were treated with angioplasty for vasospasm related to SAH. Angioplasty has been recommended as an option by American Heart Association/American Stroke Association but the prevalence has not been high, probably due to factors like lack of skilled endovascular services at institutions, lack of randomized trial showing change in outcome, and lack of reimbursement. As would be expected, a higher proportion of large volume urban teaching hospitals were performing angioplasty.
Our findings suggest that hospitals performing angioplasty for SAH related vasospasm have almost a twofold greater chance of having patients discharged to home and 18% lower in-hospital mortality after adjustment of patient characteristics. After patient and hospital characteristics adjustment, including SAH volume, these patients are more likely to be discharged home. In our analysis, these differences were independent of endovascular embolization and disease severity index, both of which have already been proven to influence outcome in SAH patients [4]. Moreover, in the multivariate model of independent predictors of outcomes in such patients, we confirmed our observation of favorable outcome of patients being discharged home without supervision in the hospitals performing angioplasty. Compared with study reported by Johnston [10] derived from study population that included both ruptured and unruptured aneurysm, our study included all spontaneous SAH cases. In their multivariable analysis, endovascular treatment was the only factor that reduced inpatient mortality which is similar to our observation. They did not include patient discharge status as their outcome parameter. Unlike our observation, in Johnston [10] analysis institutional factors were not associated with increased hospital charges, however, length of stay was shorter at institutions treating more aneurysms by endovascular techniques and institutions with higher treatment volume, findings similar to our analysis.
Our analysis shows that angioplasty for SAH related vasospasm is mainly offered by high volume hospitals which have been associated with better outcome in the management of SAH patients in previous studies [8–11]. Our analysis emphasizes that hospital size and SAH volume are important variables affecting outcomes. Large hospital size is associated with better likelihood of discharge to home and higher SAH patient volume is associated with decreased in-hospital mortality. The improved outcome has been attributed to the multidisciplinary care provided at the high volume hospitals, including neurocritical care by intensivists [15–17], greater procedural experience by hospital [18], and greater number of experienced nursing staff and other resources dedicated to the treatment of such critical patients. Since we cannot adjust for all the potential differences in patient related interventions between hospitals, we cannot distinguish between the beneficial effect of aggressive and attentive multidisciplinary care and that of more skilled neurointerventional specialists [10]. However, higher level of neurological expertise of a hospital in the management of SAH patients may be expected by the SAH case volume at a hospital. In the multivariate model of predicting independent factors affecting outcomes favorably, hospitals performing angioplasty were associated with higher discharge rate to home, independent of SAH case volume.
Because detailed procedure-related cost information is not available in the NIS, the total hospital costs were used as a surrogate for cost information. In our analysis, in multivariable Model 2 (Table 2), hospitals performing angioplasty did not have a significant increase in the cost of hospitalization or length of stay. Even though our data provides indirect inference about the resource utilization of the hospitals, cost effectiveness cannot be performed from this analysis. In a previous analysis of SAH patients, it has already been demonstrated that lengths of stay were longer, and hospital costs were greater in both univariate and multivariable models among high SAH volume hospitals [8]. We also found similar results. However, given the high costs of long-term care, an intervention that produces even a modest reduction in disability is often cost-effective when lifetime or societal impacts are considered [19]. A cost-utility analysis by Bardach et al. [20] suggested that transferring a SAH patient from a low- to a high-volume hospital would result in a gain of 1.60 quality-adjusted life-years at a cost of $10,548 per quality-adjusted life-year. Our analysis demonstrates low rates of treatment by either endovascular or surgical procedures among non traumatic SAH patients. A total of 41% of patients underwent endovascular embolization and about 42% of patients underwent surgical treatment. About 57% of patients were treated by either modality at hospitals performing angioplasty compared with 26% at hospitals not performing angioplasty. Similar findings have been noted in other studies. Johnston [10] included only academic medical centers, where a higher treatment rate can be expected compared with larger and more diverse patients population treated at other hospitals. In the afore-mentioned study, 43% of patients in the ruptured aneurysmal SAH did not receive any treatment. Another population based study in US showed treatment rates of about 45% by either surgical or endovascular modalityt [21]. There are probably many reasons for the low rate of treatment. First, not all patients admitted for a non traumatic acute SAH have intracranial aneurysms. The proportion of patients with SAH who do not have a intracranial aneurysm ranges from 4 to 37% [21]. Although we made an attempt to exclude arteriovenous malformations and arteriovenous fistulas, there may be some patients who may have SAH related to such abnormalities. There is also a high early mortality rate (within 24 h) reported in up to 22% of non traumatic SAH [22] thereby decreasing the treatment rates further.
The limitations of the data used in the present study must be acknowledged. The NIS database lacks SAH specific disease severity scales. We adjusted for disease severity using the 3M APR-DRG mortality risk algorithm, which has been used previously as a surrogate marker of disease severity [14]. This disease severity model for estimation of mortality has been used in a similar population based study of SAH [21]. This scale incorporates data for events occurring within a hospitalization, which may be related to the procedures performed during the hospitalization rather than just the baseline disease severity. We believe it was an appropriate surrogate model since it impacts all the outcome variables as would be expected from the SAH specific disease severity scale. Moreover, given the distribution of sample at the national level and interpretation of the data at the institutional level, the individual factors may not impact the results significantly. Another limitation is that the outcomes available for analyses in this study (discharge destination, length of hospitalization, and hospitalization costs) are not necessarily related directly to neurological and/or functional outcomes but can also also be influenced by the payer status and social factors. A further limitation includes the small percentage of angioplasties performed (3.6%), thus making it hard to casually attribute better outcomes to this procedure alone. Our analysis objective was not to evaluate the efficacy of the procedure alone, but to analyze the outcomes at the institution level.
Conclusions
Our analyses suggests that overall the prevalence of angioplasty procedure for SAH is low. The odds of discharge to home were higher in SAH patients treated at hospitals performing angioplasty for cerebral vasospasm. Our analysis suggests that the provision of angioplasty may be a surrogate marker of model of care in management of patients with SAH.
References
Zubkov YN, Nikiforov BM, Shustin VA. Balloon catheter technique for dilatation of constricted cerebral arteries after aneurysmal SAH. Acta Neurochir. 1984;70:65–79.
Newell DW, Eskridge JM, Mayberg MR, Grady MS, Winn HR. Angioplasty for the treatment of symptomatic vasospasm following subarachnoid hemorrhage. J Neurosurg. 1989;71:654–60.
Zwienenberg-Lee M, Hartman J, Rudisill N, et al. Effect of prophylactic transluminal balloon angioplasty on cerebral vasospasm and outcome in patients with Fisher grade III subarachnoid hemorrhage: results of a phase II multicenter, randomized, clinical trial. Stroke. 2008;39:1759–65.
Bederson JB, Connolly ESJ, Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 2009;40:994–1025.
Ncd for Percutaneous Transluminal Angioplasty (PTA) (20.7. http://www.cms.hhs.gov/mcd/viewncd.asp?ncd_id=20.7&ncd_version=8&basket=ncd%3A20%2E7%3A8%3APercutaneous+Transluminal+Angioplasty+%28PTA%29.;2009.
http://notes.bluecrossmn.com/web/medpolman.nsf/8178b1c14b1e9b6b8525624f0062fe9f/eb9611de760de2128625717100690182?OpenDocument&Highlight=0,percutaneous. Accessed 12 Sept 2009.
http://www.aetna.com/cpb/medical/data/200_299/0276.html). Accessed 12 Sept 2009.
Bardach NS, Zhao S, Gress DR, Lawton MT, Johnston SC. Association between subarachnoid hemorrhage outcomes and number of cases treated at California hospitals. Stroke. 2002;33:1851–6.
Cross DWT III, Tirschwell DL, Clark MA, et al. Mortality rates after subarachnoid hemorrhage: variations according to hospital case volume in 18 states. J Neurosurg. 2003;99:810–7.
Johnston SC. Effect of endovascular services and hospital volume on cerebral aneurysm treatment outcomes. Stroke. 2000;31:111–7.
Qureshi AI, Suri MFK, Nasar A, et al. Changes in cost and outcome among US patients with stroke hospitalized in 1990 to 1991 and those hospitalized in 2000 to 2001. Stroke. 2007;38:2180–4.
Wen SW, Kramer MS. Uses of ecologic studies in the assessment of intended treatment effects. J Clin Epidemiol. 1999;52:7–12.
HCUP Databases. Healthcare Cost and Utilization Project (HCUP). Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/nisoverview.jsp. 2009.
Shukla R, Fisher R, Fisher R. Testing of 3M’s APR-DRG Risk Adjustment for Hospital Mortality Outcomes. Abstr Acad Health Serv Res Health Policy Meet. 2002;19:11.
Berman MF, Solomon RA, Mayer SA, Johnston SC, Yung PP. Impact of hospital-related factors on outcome after treatment of cerebral aneurysms. Stroke. 2003;34:2200–7.
Mirski MA, Chang CW, Cowan R. Impact of a neuroscience intensive care unit on neurosurgical patient outcomes and cost of care: evidence-based support for an intensivist-directed specialty ICU model of care. J Neurosurg Anesthesiol. 2001;13:83–92.
Suarez JI, Zaidat OO, Suri MF, et al. Length of stay and mortality in neurocritically ill patients: impact of a specialized neurocritical care team. Crit Care Med. 2004;32:2311–7.
Matz PG. Editorial comment—spontaneous subarachnoid hemorrhage: volume, experience, and outcome. Stroke. 2003;34:2206–7.
Matchar DB. The value of stroke prevention and treatment. Neurology. 1998;51:S31–5.
Bardach NS, Olson SJ, Elkins JS, et al. Regionalization of treatment for subarachnoid hemorrhage: a cost-utility analysis. Circulation. 2004;109:2207–12.
Shea AM, Reed SD, Curtis LH, et al. Characteristics of nontraumatic subarachnoid hemorrhage in the United States in 2003. Neurosurgery. 2007;61:1131–7.
Pobereskin LH. Incidence and outcome of subarachnoid haemorrhage: a retrospective population based study. J Neurol Neurosurg Psychiatry. 2001;70:340–3.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khatri, R., Tariq, N., Vazquez, G. et al. Outcomes After Nontraumatic Subarachnoid Hemorrhage at Hospitals Offering Angioplasty for Cerebral Vasospasm: A National Level Analysis in the United States. Neurocrit Care 15, 34–41 (2011). https://doi.org/10.1007/s12028-010-9423-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-010-9423-5