
Abstract
Intracerebral hemorrhage (ICH) is a devastating and relatively common disease affecting as many as 50,000 people annually in the United States alone. ICH remains associated with poor outcome, and approximately 40–50% of afflicted patients will die within 30 days. In reports from the NIH and AHA, the importance of developing clinically relevant models of ICH that will extend our understanding of the pathophysiology of the disease and target new therapeutic approaches was emphasized. Traditionally, preclinical ICH research has most commonly utilized two paradigms: clostridial collagenase-induced hemorrhage and autologous blood injection. In this article, the use of various species is examined in the context of the different model types for ICH, and a mechanistic approach is considered in evaluating the numerous breakthroughs in our current fund of knowledge. Each of the model types has its inherent strengths and weaknesses and has the potential to further our understanding of the pathophysiology and treatment of ICH. In particular, transgenic rodent models may be helpful in addressing genetic influences on recovery from ICH.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Intracerebral hemorrhage (ICH) is a devastating and relatively common disease affecting as many as 50,000 people annually in the United States alone. ICH remains associated with poor outcome, and approximately 40–50% of afflicted patients will die within 30 days. Unfortunately, little improvement has been made in the mortality rate over the last 20 years [1]. To address this issue, the National Institutes of Health issued a priorities report in 2005 [2], and the American Heart Association released a recent set of clinical guidelines for the first time in nearly a decade [3]. In these reports, the importance of developing clinically relevant models of ICH that will extend our understanding of the pathophysiology of the disease and target new therapeutic approaches was emphasized.
Traditionally, preclinical ICH research has most commonly utilized two paradigms: clostridial collagenase-induced hemorrhage and autologous blood injection. Aside from these established methods, there exist a few other models that are less frequently employed, including hypertensive dog and rat models and a murine amyloid angiopathy model. While a model for amyloid angiopathy represents a distinctly separate mechanism for intracerebral hemorrhage, the hypertensive animal models are arguably the most clinically relevant in nature; however, they provide the poorest experimental design due to the immense degree of variability in hemorrhage size and extent of injury. A different approach has been to subject the brain to direct arterial pressures to create a hematoma. In this method, an artery, usually femoral, is cannulated with the opposite end stereotactically placed into the brain. Blood is then allowed to infuse at arterial pressures for a specified period of time resulting in a modestly well-controlled parenchymal hemorrhage. Assuming that human intracerebral hemorrhage is due to arterial rupture and not microvascular injury, the advantage of this method is that it directly mimics the human condition. However, the procedure is somewhat difficult to perform and control rendering the model inconsistent. Ultimately, when evaluating the relative advantages and liabilities of each model, it is important to keep in mind the objective of the experimental question. For instance, large animal models may be useful for addressing questions of cerebral physiology following ICH, whereas transgenic rodent models may be particularly useful in furthering our understanding of the molecular mechanisms associated with post-hemorrhage brain injury. In particular, transgenic rodent models may be helpful in addressing genetic influences on recovery from ICH, such as has been observed with the APOE polymorphism [4]. Each of the model types has its inherent strengths and weaknesses and has the potential to further our understanding of the pathophysiology and treatment of ICH (Table 1).
Collagenase-induced ICH Model
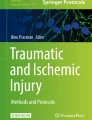
Injection of clostridial collagenase into brain parenchyma is a common method of inducing a reproducible basal ganglia hemorrhage. Introduced in the early 1990s by Rosenberg et al. [5], the model is thought to closely represent spontaneous ICH in humans. Collagenases are proteolytic intracellular enzymes that catalyze the hydrolysis of collagen. As collagen is a fundamental component of the basal lamina of the blood–brain barrier, collagenase injection results in the dissolution of extracellular matrix around cerebral capillaries and results in ‘spontaneous’ hemorrhage at the injection site. The advantages of this model are its simplicity and consistency, dose-dependent hemorrhage size, and ease of adaptation to multiple species, including pig, mouse, and rat [5]. Unfortunately, bacterial collagenase by itself can elicit an inflammatory response that is more intense than that observed in blood infusion models [6]. Whether the human inflammatory response is similar to either the blood injection or collagenase-induced models is debatable and unanswerable at present. However, it has been shown in vitro that collagenase alone does not result in apoptosis that is seen in vivo with ICH [7]. The collagenase model demonstrates its clinical relevance by conceptually integrating small vessel breakdown to produce hemorrhage and allows a controllable amount of variability in hemorrhage size. Additionally, it may imitate the ‘bleeding–rebleeding’ phenomenon seen in the human condition. Overall, the collagenase model mimics the human disease in several distinct features, is straightforward to establish, allows for rapid accumulation of data with the opportunity to evaluate transgenic effects, but probably has some inflammatory effects that may be unrelated to hematoma (Fig. 1).

Hematoxyllin and Eosin stain of intracerebral hemorrhage after collagenase injection into a mouse basal ganglia
Autologous Blood Injection Model
Injection of whole blood into various brain regions is another common method for modeling ICH in the laboratory. Blood injection has been available since the mid-1980s and has been used in a variety of species. In the anesthetized animal, a needle is stereotactically inserted into a specified area of the brain; and a precise volume of autologous whole blood is infused over a specified time, thereby producing a consistent hemorrhage volume. The obvious disadvantage to this technique is that it does not emulate small vessel rupture, which is thought to be the etiology of the vast majority of spontaneous intracranial hemorrhages in humans. Additionally, there may be problems with ‘back flow’ of blood along the needle track and ventricular rupture [8]. Blood “reflux” has been largely resolved by the development of a ‘double injection’ technique by Deissberger et al. [9], whereby a small amount of blood is infused and allowed to clot along the needle track with subsequent infusion of the remainder of the blood volume. Blood injection allows for clinically relevant comparisons in that the mechanistic effects examined are strictly related to the presence of blood within parenchymal brain tissue; however, there is no opportunity to evaluate rebleeding or the effects of microvascular breakdown. As with the collagenase model, autologous blood injection is also a relatively simple procedure that can be rapidly applied to all animal species and allows for transgenic applications (Fig. 2).

Fresh mouse brain 6 h after collagenase injection into left basal ganglia
Species
Primate
Though clearly an excellent animal in which to study translational mechanisms and one of the first to be characterized in ICH, primates are complex to house and are often prohibitively expensive, and accordingly there is a relative paucity of ICH research in this species. Primate models lend themselves to examination of cerebral physiology, and published reports have evaluated the effect of blood pressure manipulation on cerebral blood flow (CBF). CBF was globally reduced for 1 h after ICH induction and most reduced at the periphery of the hematoma with blood flow below ischemic threshold, leading to the theory of perihematomal ischemic penumbra [10]. Additionally, cerebral vasodilation after ICH resulted in increased hematoma size while vasoconstriction resulted in increased ischemia and cerebral infarction [11]. Despite the potential for readily translatable experimental results, further research is likely to be limited in primates due to expense and increasing regulatory oversight.
Feline
Though suitable for neurophysiologic study, there are few recent ICH investigations employing a cat model, possibly due to their companion status and availability of other equally useful animal models. All reported studies used autologous blood infusion and have addressed the relationship between intracranial pressure (ICP), hematoma formation, and blood flow. The first study found location and size of hemorrhage determined ICP elevation and functional outcome [12], while others have suggested a correlation between elevated ICP and decreased CBF after ICH [13]. It is unlikely that feline models will become more prevalent due to availability of other more useful and more commonly employed species.
Canine
As one of the original ICH models, the dog is well suited to physiological and surgical study; however, it is also considered a companion animal and remains expensive to use. There exist two models in the dog: a hypertensive model in which iatrogenic systemic hypertension results in spontaneous hemorrhage, and an autologous blood injection model. Early dog studies defined lethal volumes and locations for hematomas [14], the existence of an ischemic penumbra [15], assessed the use of sonography [6, 16], and investigated cerebrospinal fluid changes, which pre-date the use of microdialysis catheters [17, 18]. More recently, the dog model has been used for investigating imaging techniques, brain physiology, surgical interventions, and therapeutic interventions. From imaging studies involving the dog model, three distinct stages of ICH have been identified (acute, subacute, and chronic) based on correlative histological and radiological criteria [15]. Furthermore, Weingarten et al. [19] evaluated different magnetic resonance imaging (MRI) sequences to distinguish venous, arterial, and intraventricular blood signals. Dog models are also useful in the study of cerebral physiology and have been used to assess the effects of anemia on cerebral hemodynamics [20] and the changes in cellular microenvironments after ICH [21]. With the development of minimally invasive surgical techniques, the dog has also been used to evaluate the safety of stereotactic hematoma aspiration [22]. Finally, Qureshi et al. [23] have preformed several therapeutic studies in the dog model. Initially, they demonstrated that pharmacologic reduction of mean arterial pressure after ICH with labetolol did not result in decreased regional blood flow or deleterious ICP effects, a result that has been translated to humans [24]. In a separate study, this group found that hypertonic saline had an equal and more sustained effect than mannitol in controlling elevated ICP in global [25] and regional [26] measurements after ICH, which is similar to findings in other human brain injury states [27]. It appears that the dog model, despite its companion status and expense, will continue to be used at least occasionally for ongoing physiology and surgical research.
Porcine
At present, porcine models have largely replaced ICH canine models for evaluation of surgical and physiological interventions in large animals. The abundance of white matter in the porcine model makes it particularly relevant, as it is similar to the proportion of white-to-gray matter found in humans. The swine model has been utilized to evaluate changes in somatosensory evoked potential changes after ICH [28], and more recent publications have focused on ICH effects on cortical excitability at anatomic locations distal to the hematoma with or without corpus callosum transection [29–31]. With the publication of the Surgical Treatment of ICH (STICH) trial results [32], enthusiasm for surgical treatment has waned, although technological advancements in clot extraction have generated multiple endeavors using the porcine model to evaluate surgical clot removal augmented with tissue plasminogen activator (t-PA) at both hyperacute (less than 6 h) [33] and long-term (10 days) [34] time points. Although delayed clot extraction may be associated with inflammatory responses and secondary neuronal injury, this may be ameliorated with the addition of N-methyl-d-aspartate (NMDA) receptor antagonists [35]. Additionally, with the advent of new intraparenchymal brain monitors, the pig has been employed to evaluate the value of brain tissue oxygen partial pressure monitoring [36]. Finally, the porcine model has been useful in evaluating causes of and intervention on perihematomal edema [37]. Investigations have focused on the role of plasma protein accumulation [38] and the relative effects of red cell or plasma infusion into deep hemispheric white matter [39] with the finding that secondary inflammation requires both blood components. Investigators have recently demonstrated the effects of profound local hypothermia on perihematomal edema and interleukin expression [40], as well as the palliative effects of heme-oxygenase inhibitors [41, 42]. The porcine model appears to hold promise for future use to mimic human neurophysiology and pioneer new surgical techniques.
Lapine
The rabbit is one of the larger small-animal models, which makes it more practical in studying surgical techniques and physiologic responses to acute brain injury than its smaller rodent counterparts. Rabbits are easily housed, relatively inexpensive when compared to larger animals, and do not present the companion status of the cat or dog. Using autologous blood injection, the model was originally developed in the early 1980s by Kaufman et al. [43] to determine lethal clot volumes and appropriate analysis of edema. Since then the rabbit model has been used to examine imaging techniques, surgical innovations, and the pathophysiology of secondary injury. In this model, MRI has been used to study hyperacute (less than 6 h) [44] and longer-term (10 days) [45] changes after ICH. Of the surgical techniques evaluated, the rabbit model has been especially useful in evaluating minimally invasive clot removal. For example, one study demonstrated the efficacy and safety of urokinase in clot lysis up to 24 h after injury [46]. These observations have been repeated using t-PA, which is clinically available [47]. With the advent of microdialysis catheters the rabbit was used to analyze the cellular microenvironment with respect to glutamate and other amino acids [48]. The autologous blood injection model has been incorporated into the rabbit species to quantify intact, reversibly injured, and necrotic cells up to 24 h after injury [49] and to clarify the interaction of astrocytes and microglia in the initiation the iron storage and hemosiderin formation [50]. Furthermore Koeppen et al. [51] used the rabbit to determine the effects of heme-oxygenase-1 on ferritin biosynthesis and subsequent secondary injury. A novel study examined post-injury ileus as a marker of DRG degeneration after ICH [52]. The role of volatile anesthetics has also been studied in the rabbit, and a recent study investigated the hemodynamic and ICP effects of sevoflurane after hemorrhage [53]. Thus, although its use to study genomic effects is limited, there is good potential for the continued utilization of the rabbit model to study physiology and procedural interventions when large animal models are either unavailable or disadvantageous.
Murine
Due to cost-effectiveness and availability of transgenic systems, rats, and increasingly mice, have gained popularity for ICH research in recent years. Both autologous blood and collagenase injection have been established, with the basal ganglia being the most common site of injury, although other areas have been described. One of the disadvantages of these animals is the relative paucity of white matter when compared to pigs, dogs, or primates, as most of the rodent brain consists of cortex or deep gray matter structures (i.e., basal ganglia). At present, transgenic systems exist primarily in the mouse, making this the optimal model for studying genomic effects on ICH and secondary mechanisms of injury. The use of rodent models began in the mid-1980s with the evaluation of mass effect, ICP, and CBF. The first model described involved cannulation of the femoral artery with stereotactic placement of ICH under direct arterial pressures [54]. Follow-up studies utilized stereotactic placed balloons [55] and showed a positive correlation between ICP and hematoma volume and negative correlation with blood flow [56]. The first use of autologous blood injection was reported by Nath et al. [57], who explored hemodynamic and ICP changes after hemorrhage. Subsequent studies in the rat have evaluated the roles of thrombin [58], complement [59, 60], oxidative stress [61, 62], apoptosis [7, 63], and pro-inflammatory cascades [64, 65] in the generation of secondary injury (Table 2).
Mechanisms of Injury
Whereas neuronal injury associated with ICH was initially considered a relatively static insult caused by the mass effect of the intracranial blood clot and subsequent development of ischemic penumbra, during the last decade preclinical models have provided a wealth of information regarding the mechanisms of secondary injury involved in ICH. These data suggest the evolution of a more dynamic evolution of the destructive processes, which consequently may represent therapeutic targets. Currently the term ‘neurohemoinflammation’ has been coined to describe the initial inflammatory effects after the brain is exposed to blood components. Though ultimately inflammatory mechanisms seem to converge into final common pathways of cellular impairment, ‘neurohemoinflammation’ is an apt descriptive term for the reactions that occur specifically after hemorrhage. The current preclinical models have provided a strong case for a vigorous inflammatory response to ICH including cytokine release, microglial and astrocytic activation, pro-inflammatory cascades, and apoptosis.
Inflammation
Pro-inflammatory cytokines produce damaging enzymatic cascades, and there is substantial evidence from animal models that CNS inflammatory responses play a significant role in the self-propagating mechanisms of secondary injury after ICH [64]. Nuclear factor kappaB (NF-κB) is a transcription factor that translocates to the nucleus within hours of ICH, and is associated with the upregulation of a number of inflammatory and apoptotic genes, including interleukin 1-beta (IL-1β) and tumor necrosis factor-alpha (TNF-α) [38]. This inflammatory cascade is amplified by the fact that IL-1β and TNF-α are also potent activators of NF-κB [66]. Depending on the animal model used, cytokines are appreciably increased as early as 2 h after hemorrhage. In the autologous blood [60] and collagenase-induced [67] rodent ICH models, TNF-α was increased at 2 and 4 h, respectively.
The inflammatory cascade may serve as a target for therapeutic intervention, and a recent review demonstrates some of the possible target sites [68]. For example, there is evidence that inhibition of cytokine expression can decrease post-hemorrhagic edema and secondary neuronal injury. After autologous blood injection, rats virally transfected with an IL-1β receptor antagonist gene developed less edema than controls [69, 70]. Infusion of TNF-α antisense oligodeoxynucleotide into the injured cerebral hemisphere decreased both edema and neurological deficit after collagenase-induced hemorrhage in the rat [67]. Heat shock proteins (HSP) have been reported to reduce cell injury and inflammation. Using a collagenase-induced ICH rat model, Sinn et al. [71] reduced the levels of several inflammatory markers, including matrix metalloproteinases, interleukins, and macrophage inhibitory protein by pharmacologically inducing HSP70 expression. Finally, pharmacologic activation of peroxisome proliferator activated receptor-γ (PPAR-γ), a nuclear hormone receptor, suppressed NF-κB activation and improved neurological outcome in a mouse ICH model [72]. Further work should focus on the extent to which cytokines contribute to long-term neurocognitive injuries and whether targeted therapy can ameliorate acute secondary injury mechanisms or improve chronic cognitive deficits.
Microglial Activation and Astrogliosis
Microglial activation is a cornerstone of the neuroinflammatory response, and facilitates a variety of adaptive responses, including phagocytosis of necrotic cells, recruitment of hematogenous leukocytes, and astroglial activation. After experimental ICH, deliberate manipulation to decrease microglial recruitment results in retained hematoma and increased numbers of necrotic cells [73]. There is also some evidence that microglia may attempt to rescue dying cells after hemorrhage by producing trophic factors such as brain-derived neurotrophic factor [74]. However, one of the primary functions of activated microglia appears to be the initial clearing of heme degradation products [51], and their reactivity is probably affected by a number of factors including endogenous t-PA [73] and plasma components [39, 50].
Although many of these microglial functions are adaptive, it is probable that excessive microglial activation exacerbates CNS inflammation and oxidative stress, and may contribute to secondary injury after ICH. As a consequence of the increased number and activity, microglia have been linked to increased reactive oxygen species [75], cytokines [76], iron metabolism [77], complement [78], and proteases [65, 79] in multiple mechanisms of brain injury. In ICH, activated microglia exist in tissue adjacent to the hematoma within an hour of autologous blood infusion. Subsequently, activated microglia increased in number up to 7 days after injury, with subsequent reduction in numbers over several weeks [50, 74, 80–82].
Inhibition of microglial activation with minocycline, an inhibitor of matrix metalloproteinases, in a collagenase-induced rat ICH model produced neurobehavioral improvement [83], but did not decrease neuronal loss [84]. Furthermore, tuftsin fragment 1–3, a potent microglial inhibitory factor, improved both neurological severity scores and hemorrhage size after collagenase-induced ICH in mice [73]. Atorvastatin, an HMG-CoA reductase inhibitor, decreased microglial accumulation and improved functional outcomes but did not affect hemorrhage size [85]. Finally, two experiments demonstrated that administration of the volatile anesthetic sevoflurane decreased [86] while propofol infusion increased [87] microglial activation after autologous blood injection in the rat. Thus, pharmacological interventions that affect microglial function may ultimately become an important therapeutic target. Although the increase in activated microglia is temporally associated with tissue destruction, it is probable that microglia serve an adaptive function as well, and separating out the beneficial from the destructive effects remains a challenge for rational pharmaceutical design.
Astrocyte activation occurs in concert with microglial activation, although the role of astrocyte function in ICH has not been studied as extensively. Several studies found an initial loss of astroglia followed by increased infiltration in the perihematomal area, specifically in pericapillary tissue, using both glial fibrillary acidic protein and vimentin as markers [50, 70, 88]. This response seems to require, or at least be magnified by, some as yet undefined plasma protein(s) given that the injection of whole blood causes more glial activation than injection of erythrocytes alone [50]. Of the remaining studies evaluating astroglial induction and proliferation, one revealed that clot extraction did not reduce astroglial activation after collagenase administration in rats [89], and the other, though of unclear significance, demonstrated uncontrolled astroglial proliferation in a single animal following embryonic stem cell transplantation after ICH in the rat [90].
Matrix Metalloproteinases
Matrix metalloproteinases (MMPs) are a family of zinc-dependent endopeptidases that degrade the extracellular matrix and are known to be elevated, and their inhibitors depleted, after multiple types of brain injury, including ICH [91]. Their role in brain injury is complex and likely includes interaction with microglia, apoptosis, disruption of the blood–brain barrier, and thrombin generation [79]. Of the 23 known mammalian MMPs, four have been studied in detail: MMP-2, -3, -9, and -12. MMP-12 has been shown to be the most elevated and is associated with poor outcome in murine ICH [92]. MMP-2 and -3 have been found to increase in tissue adjacent to the hematoma after collagenase-induced hemorrhage [93]. However, MMP-9 is currently the most thoroughly studied MMP in the setting of ICH [29, 71, 91, 93–96]. MMP-9 is increased early in ICH, and its presence can be found from 48 h to 7 days in both cerebral hemispheres [29] Additionally, deletion of the gene for MMP-9 resulted in upregulation of MMP-2 and -3, which was associated with worse edema, hemorrhage and neurologic deficit [93]. The association of a genetic deficiency of MMP-9 with MMP-2 and -3 is unclear, as is the explanation of poorer clinical outcomes with the absence of MMP-9. Interestingly, MMP-9 has been correlated with microhemorrhages in aged mice, and its production is stimulated by amyloid-beta peptide over expression in a murine model of cerebral amyloid angiopathy [94]. The collagenase rat model has been used to demonstrate increases in MMP-2 and MMP-9 greater than 16 h after ICH induction, and the suggestion that MMPs contribute to secondary edema was corroborated by the finding that addition of BB-1101, a non-selective MMP inhibitor, diminished edema [91, 97]. Further evidence that MMP inhibitors might serve a therapeutic role was suggested by the reduction in oxidative stress associated with GM6001, an inhibitor of MMP-9 function [95]. Inhibition of MMP-12 may also be one mechanism by which administration of minocycline improves neurological severity scores and reduces perihematomal cellular loss [83]. Thus, although MMPs may serve as potential therapeutic targets, the exact role of this family of proteases remains to be defined in ICH.
Apoptosis
Numerous investigators have demonstrated that apoptosis occurs adjacent to the ICH lesion, as evidenced by the increase in terminal deoxynucleotidyl transferase mediated dUtp nick end label (TUNEL)-positive cells [67, 81]. In preclinical models, apoptosis begins approximately 24 h after lesioning with predominant involvement of neurons and glia [7], a finding that has been replicated in humans [63]. Although intracellular pathways associated with apoptosis are complex, attention has focused on the role of caspase activation. Following autologous blood injection, caspase activation, is localized to perihematomal cells undergoing apoptosis [98]. Injection of zVADfmk, a non-selective caspase inhibitor, into the cerebral ventricular system reduced TUNEL-positive cell density after collagenase-induced ICH in rats [7]. Heat shock protein (HSP) 70 has also been implicated in apoptotic pathways as early as 24 h after experimental ICH [99]. Finally, caspase activity and apoptosis peaks at 24 h, and is less evident at 72 h following autologous blood injection in the rat [100].
However, apoptosis is likely related to multiple pathways of ICH-induced cell injury, as evidenced by the finding that memantine, an NMDA antagonist, reduces apoptosis, but also decreases microglial recruitment, bcl-2 upregulation, and caspase-3, t-PA, and MMP-9 expression [96]. Consistent with this, when memantine was administered with celecoxib, a selective cycloxgenase-2 inhibitor, apoptosis was further reduced [101]. Apoptosis has been associated with other inflammatory pathways and markers including TNF-α [67], MMPs [83], interleukins, microglial inhibitory protein-1 [71], NF-κβ [72], and other caspases [102]. The relationship between these markers and apoptotic pathways remains to be defined.
The association between apoptosis and secondary injury after ICH needs to be translated and tested in humans to determine whether pharmacologic intervention against delayed cell death is a viable clinical strategy. In a rat collagenase model, FK-506 decreased apoptosis at 2 days but did not ultimately decrease neuronal loss at 9 weeks [103]. Involvement of TNF-α is supported by the reduction in apoptosis and TNF-α with the use of the A2A specific receptor agonist CGS 2160 in the rat collagenase model [104]. NF-κβ has been implicated in several studies, including use of 15-deoxy-δ (12,14)-prostaglandin J2 (15d-PGJ2) to increase PPARγ and reduce apoptosis and NF-κβ(activation [72]. However, complexity of this interaction is suggested by tauroursodeoxycholic acid (TUDCA), an endogenous bile acid, activating the Akt-1 protein kinase B-α survival pathway and modulating Bcl-2 expression and NF-κβ activity presumably to reduce apoptosis [105]. Not only did the use of erythropoietin (EPO) in a rat collagenase model reduce apoptosis but also microglial activation, mRNA levels of TNF-α, Fas and Fas-L, as well as the activities of caspase-8, -9, and -3 [102].
Complement
Complement activation is a component of the humoral immune response and is likely important in the pathogenesis of many neurological disorders. It may be particularly important in the development of post-hemorrhagic edema in ICH due to complement-induced hemoglobin release by erythrolysis. It is also likely that complement activation is involved in cytokine production [106]. There is ample evidence that complement activation plays a role in the response to ICH. Hua et al. [59] demonstrated a perihematomal increase in C9, which is important in the generation of the membrane attack complex. Treatment with N-acetylheparin, to inhibit complement activation, decreased perihematomal edema. Treating rats with cobra venom factor after ICH induction replicated the association between complement activation and edema formation [60]. Another venom defibrase, DF-521 batroxobin, reduced ICAM-1 expression and C3 & C9 brain content up to 72 h after ICH in the rat [107]. Other investigators demonstrated that ICH increases CR3 expression, a complement receptor, which is expressed by activated microglia [50, 80]. CR3-deficient mice had less edema at 3 days and improved neurobehavioral outcomes after autologous blood injection [108]. Contrary to these findings, Nakamura et al. [109] found greater perihematomal edema formation in C5 deficient mice after autologous blood injection compared with wild type cohorts.
The interplay between different complement factors, receptors, and activators is complicated. However, the majority of evidence suggests a role for complement activation in the formation of edema after experimental ICH making this a potential target for intervention to prevent secondary injury.
Oxidative Stress
Reactive oxygen species (ROS) contribute to secondary injury in ICH. Extracellular iron created from hemoglobinolysis generates ROS and subsequent pathological processes [110]. In cell culture models of neuronal injury, the free radical scavenger, U83836E, significantly reduced hemoglobin-induced neuronal death, providing evidence that modulating hemoglobin breakdown may ameliorate oxidative stress in animals [62]. In experimental ICH models protein carbonyl formation is increased in both the pig and rat. In the porcine model, protein carbonyl was detected within minutes after autologous blood injection [39]. In the rat there were associated reductions in superoxide dismutase (SOD) activity, increased DNA fragmentation, and increased heme-oxygenase-1 (HO-1) expression [111]. C3-deficient mice demonstrated less HO-1 expression at 3 days after ICH, possibly linking complement pathways with ROS production [108]. In other transgenic systems, inducing hemorrhage in NADPH KO mice resulted in less edema, improved neurologic function, and decreased mortality [112]. HO-2 KO mice displayed attenuated neuronal injury after whole blood injection [113]. In the rat, treatment with the antioxidants dimethylthiourea or alpha-phenyl-N-tert-butyl nitrone (PBN), reduced neurological dysfunction after collagenase-induced hemorrhage [114] as did the chelating agent deferoxamine [109]. Oxidative stress has been implicated in the mechanisms of endothelial injury that occur in the hypertensive rat, which has implications in the etiology of primary ICH formation [115]. Thus, therapeutic strategies targeting iron-generated ROS may be a fruitful area for further research and translation into human studies [116, 117].
Genetic Influences
The importance of genetic influences on modifying outcome after ICH is only beginning to be fully appreciated. The availability of transgenic murine systems has made this the species of choice in to study genetic influences in ICH. One of the first rodent models of hemorrhage due to amyloid angiopathy was developed in a transgenic mouse that overexpressed amyloid precursor protein [118]. Often, the deletion of genes associated with inflammation may provide unexpected results, emphasizing the complexity of inflammatory pathways. For example, following collagenase injection, C5 deficient mice have increased brain edema 3 days after ICH [119]. This finding was similar after deletion of the MMP-9 gene with resultant worsening of neuroseverity scores [93], although MMP-12 deficiency resulted in improved functional outcomes [92]. The t-PA deficient mouse has been used to evaluate the role of endogenous fibrinolytics with findings that it may assist in hemorrhage clearance and contribute to functional recovery [73]. However, Thiex et al. [120] examined the effects of ICH in t-PA deficient mice to determine the role of exogenous t-PA administration in brain edema formation. Their findings suggest that endogenous t-PA is of limited importance in the face of an immense edema-promoting effect of exogenous t-PA. Finally, the role of oxidative stress was assessed in a gp91 phox (a subunit of the NADPH oxidase enzyme) KO mice subjected to collagenase-induced ICH. As expected, mice unable to express NADPH oxidase demonstrated less edema, mortality, and ICH volume supporting the contention that ROS are important in ICH evolution [112].
One of the more intriguing clinical observations made in recent years is the suggestion that APOE polymorphism may influence clinical outcomes after ICH. The three common human protein isoforms of apoE, designated apoE2, apoE3, and apoE4, are encoded on human chromosome 19, and differ by single amino acid interchanges at residues 112 and 158: E3 (Cys112 Arg158); E4 (Arg112 Arg158); E2 (Cys112 Cys158) [121]. Several clinical studies have implicated the APOE4 polymorphism with increased mortality and poor functional outcome following ICH [4, 122]. The availability of targeted replacement APOE animals has allowed for the exploration of these isoform-specific effects in acute injury models [123]. These experiments have demonstrated the importance of apoE in modifying brain inflammatory responses after injury [124, 125], which is a finding that is likely germane to ICH. Moreover, these observations have suggested that administration of apoE-mimetic therapeutics reduce secondary neuronal injury and, thereby, improve functional outcomes following acute brain injury [126–128] and may be translatable to human ICH.
Imaging Techniques
The use of computerized tomographic (CT) scanning revolutionized the management of acute brain injury, and the rise of magnetic resonance imaging (MRI) has provided even more detailed imaging. Both modalities have continued to evolve over the years to include a variety of techniques including angiography, venography, and perfusion sequences. These multimodal imaging techniques continue to play an increasingly important role in preclinical modeling of ICH. The earliest publication evaluated the use of MRI pulse sequences in comparison to CT and gross sectioning of dog brains over the week following ICH induction finding gradient-echo MR images as useful as CT in delineating hemorrhage [19]. Additionally, MRI sequencing was employed in the collagenase-induced ICH rat model over 3 weeks following hemorrhage formation and found good correlation with edema, neutrophil and macrophage infiltration, and selective cellular death [129]. With the refinement of imaging technology, this model was also used with MRI diffusion mapping to refute the concept of perihematomal ischemia (ischemic penumbra) [130]. Finally, the MRI was validated in the acute (under 6 h) [44] and hyperacute (30 min) phases of ICH with histological hemorrhage size in an autologous blood injection rabbit model [45]. Several projects have employed imaging as an outcome measure for therapeutic interventions including the calcium channel antagonist levemopamil [131], a variety of antioxidants [61, 114], the anti-inflammatory fuicodan [132], a neurotrophic factor axokine [133], fibrinolysis for clot evacuation [9], and long-term outcome measures [34]. Imaging provides a useful mechanism to study progression of secondary injury in a living animal, and reduces the total number of animals necessary to produce meaningful results (Fig. 3).

Evolution of parenchymal hematoma in ApoE4 mouse. T2-weighted RARE spin echo images at 2 h show predominantly low signal hematoma within the right basal ganglia, consistent with deoxyhemoglobin and intracellular methemoglobin. At 72 h, there is conversion to predominantly high signal, consistent with extracellular methemoglobin
Therapeutic Interventions
Surgical
Although a recent review of possible procedural interventions demonstrated a number of methods ready for translation into humans [134], at present, the clinical management of ICH is largely directed toward treatment of arterial and intracranial hypertension, and providing supportive care. Though the STICH trial [32] did not support surgical management for supratentorial hemorrhages, the availability of new devices and more rigorous patient selection affords the possibility of a beneficial procedural intervention. To this end, the MISTIE trial investigators are currently examining the use of stereotactic clot lysis, the CLEAR IVH trial is addressing intraventricular clot lysis, and STICH II is evaluating subsets of patients that might benefit from surgical clot removal [135]. Experiments in animals have evaluated different methods of hematoma evacuation and dissolution. Early (under 4 h) clot lysis and aspiration reduced hematoma volumes by up to 70% in the autologous blood injection porcine model [33]. However, others have been unable to document reduced edema formation after surgical clot extraction in the same species [136]. More recent therapeutics includes the evaluation of sonothrombolysis. Microbubble-enhanced sonothrombolysis (MEST) has received recent attention in ischemic stroke and was the subject of study in a rat collagenase-induced ICH model [137]. However, MEST did not improve hemorrhage size, edema or degree of apoptosis when applied 3 h after ICH.
Medical
Currently there is limited medical intervention approved for use in the clinical setting. Though recombinant activated factor VII appeared promising by reducing early hemorrhage growth in humans, data from a definitive phase III trial presented at the 2007 American Academy of Neurology Annual Meeting failed to demonstrate improvement in clinical outcomes. Interestingly in the only preclinical data published, recombinant factor VIIa decreased hematoma size in a rat collagenase model when measured at 24 h after hemorrhage induction, but edema was unaffected [138].
Preclinical studies have reported benefit from induced hypothermia in ICH, although the effect is not powerful. Reduced edema in rats 24 h after autologous blood injection was associated with better preserved blood–brain barrier function [138]. At the same time, it has been reported that the timing of onset of hypothermia may be important with early onset being associated with increased hemorrhage after collagenase injection in the rat while a delayed onset of prolonged hypothermia improved neurologic outcome [139]. Finally combination of delayed hypothermia onset and constraint-induced movement therapy yielded a better neurologic outcome than either treatment alone [140].
In addition to the metalloporphyrin heme-oxygenase (HO) inhibitors mentioned above [41, 42, 51, 141], there have been several studies investigating other potential treatments including glutamate receptor antagonists [142], a cyclooxygenase-2 (COX-2) inhibitor [143], HMG Co-A reductase inhibitors [85] and human erythropoietin [102]. In a blood injection rat model, increased glucose metabolism, measured by perihematomal [14C]-2-deoxyglucose uptake, was blocked by the glutamate receptor antagonists NBQX and MK-801 while it was increased with glutamate receptor activation by NMDA and AMPA [142]. Lee et al. [96] corroborated these findings by administering memantine, a noncompetitive NMDA receptor antagonist, in a collagenase-induced rat model and found improved functional outcomes with decreased markers for apoptosis. Though COX-2 inhibitors have recently fallen out of general favor due to concerns over cardiac pathology, celecoxib improved neuroseverity scores, apoptotic markers, brain edema, and brain prostaglandin E2 expression in both collagenase-induced and autologous blood injection models in the rat [143]. There has also been renewed interest in the role of HMG Co-A reductase inhibitors (‘statins’) in acute brain injury. In ICH there is limited human data, but atorvastatin reduced neurologic deficient and neuronal loss 1 week after injury, a finding that was associated with histological improvement in synaptogenesis, neuronal migration, and immature neurons [144]. Additionally, erythropoietin reduced TNF-α, apoptotic markers, and edema while increasing nitric oxide synthase protein expression and improving neurologic scores [102]. Finally, there have been two studies evaluating the use of stem cell transplantation after ICH induction. Intravenous administration of human bone marrow in a rat ICH model improved neuroseverity scores and mitotic activity, and decreased overall tissue loss [145], whereas introduction of intraventricular embryonic neural stem cells 7 days after ICH produced neurons and astrocytes adjacent to hematomal cavities with lasting effect up to 28 days after transplantation [90].
Conclusion
At present, there are a variety of different preclinical models for study of spontaneous ICH, each with its own inherent advantages and inabilities. These models have been used to delve into a variety of different mechanistic ICH questions with potentially clinically relevant results. Unfortunately, to date there continues to be little therapeutic intervention available to humans, and there is much to learn about the primary etiology of ICH as well as mechanisms of secondary injury. Of the models in current use, the porcine model best lends itself to the study of physiology and procedural interventions, while small rodent models may be best suited for mechanistic studies of secondary neuronal injury. Definition of long-term pathological and functional (both neurologic and neurocognitive) outcomes is possible in current models but remains to be defined. Given the paucity of options available in the current clinical setting, information gained from these models will require intense translational effort to define relevance to the human condition, where there continues to be a great need for therapeutic intervention.
References
Broderick JP, Adams HP Jr., Barsan W, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1999;30(4):905–15.
Priorities for clinical research in intracerebral hemorrhage: report from a National Institute of Neurological Disorders and Stroke workshop. Stroke 2005;36(3):e23–41.
Broderick J, Connolly S, Feldmann E, et al. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke 2007;38(6):2001–23.
McCarron MO, Weir CJ, Muir KW, et al. Effect of apolipoprotein E genotype on in-hospital mortality following intracerebral haemorrhage. Acta Neurol Scand 2003;107(2):106–9.
Rosenberg GA, Estrada E, Wesley M, Kyner WT. Autoradiographic patterns of brain interstitial fluid flow after collagenase-induced haemorrhage in rat. Acta Neurochir Suppl (Wien) 1990;51:280–2.
Enzmann DR, Britt RH, Lyons BE, Buxton JL, Wilson DA. Natural history of experimental intracerebral hemorrhage: sonography, computed tomography and neuropathology. AJNR Am J Neuroradiol 1981;2(6):517–26.
Matsushita K, Meng W, Wang X, et al. Evidence for apoptosis after intercerebral hemorrhage in rat striatum. J Cereb Blood Flow Metab 2000;20(2):396–404.
Yang GY, Betz AL, Chenevert TL, Brunberg JA, Hoff JT. Experimental intracerebral hemorrhage: relationship between brain edema, blood flow, and blood–brain barrier permeability in rats. J Neurosurg 1994;81(1):93–102.
Deinsberger W, Hartmann M, Vogel J, et al. Local fibrinolysis and aspiration of intracerebral hematomas in rats. An experimental study using MR monitoring. Neurol Res 1998;20(4):349–52.
Bullock R, Brock-Utne J, van Dellen J, Blake G. Intracerebral hemorrhage in a primate model: effect on regional cerebral blood flow. Surg Neurol 1988;29(2):101–7.
Laurent JP, Molinari GF, Oakley JC. Primate model of cerebral hematoma. J Neuropathol Exp Neurol 1976;35(5):560–8.
Tomita H, Ito U, Ohno K, Hirakawa K. Chronological changes in brain edema induced by experimental intracerebral hematoma in cats. Acta Neurochir Suppl (Wien) 1994;60:558–60.
Kobari M, Gotoh F, Tomita M, et al. Bilateral hemispheric reduction of cerebral blood volume and blood flow immediately after experimental cerebral hemorrhage in cats. Stroke 1988;19(8):991–6.
Steiner L, Lofgren J, Zwetnow NN. Characteristics and limits of tolerance in repeated subarachnoid hemorrhage in dogs. Acta Neurol Scand 1975;52(4):241–67.
Takasugi S, Ueda S, Matsumoto K. Chronological changes in spontaneous intracerebral hematoma—an experimental and clinical study. Stroke 1985;16(4):651–8.
Lillehei KO, Chandler WF, Knake JE. Real time ultrasound characteristics of the acute intracerebral hemorrhage as studied in the canine model. Neurosurgery 1984;14(1):48–51.
Sussman BJ, Barber JB, Goald H. Experimental intracerebral hematoma. Reduction of oxygen tension in brain and cerebrospinal fluid. J Neurosurg 1974;41(2):177–86.
Sugi T, Fujishima M, Omae T. Lactate and pyruvate concentrations, and acid-base balance of cerebrospinal fluid in experimentally induced intracerebral and subarachnoid hemorrhage in dogs. Stroke 1975;6(6):715–9.
Weingarten K, Zimmerman RD, Deo-Narine V, Markisz J, Cahill PT, Deck MD. MR imaging of acute intracranial hemorrhage: findings on sequential spin-echo and gradient-echo images in a dog model. AJNR Am J Neuroradiol 1991;12(3):457–67.
Lee EJ, Hung YC. Marked anemic hypoxia deteriorates cerebral hemodynamics and brain metabolism during massive intracerebral hemorrhage. J Neurol Sci 2001;190(1–2):3–10.
Yin W, Tibbs R, Aoki K, Badr A, Zhang J. Metabolic alterations in cerebrospinal fluid from double hemorrhage model of dogs. Acta Neurochir Suppl 2002;81:257–63.
Mukai H, Yamashita J, Kitamura A, Ito H. Stereotactic Aqua-Stream and Aspirator in the treatment of intracerebral hematoma. An experimental study. Stereotact Funct Neurosurg 1991;57(4):221–7.
Qureshi AI, Wilson DA, Hanley DF, Traystman RJ. Pharmacologic reduction of mean arterial pressure does not adversely affect regional cerebral blood flow and intracranial pressure in experimental intracerebral hemorrhage. Crit Care Med 1999;27(5):965–71.
Powers WJ, Zazulia AR, Videen TO, et al. Autoregulation of cerebral blood flow surrounding acute (6–22 h) intracerebral hemorrhage. Neurology 2001;57(1):18–24.
Qureshi AI, Wilson DA, Traystman RJ. Treatment of elevated intracranial pressure in experimental intracerebral hemorrhage: comparison between mannitol and hypertonic saline. Neurosurgery 1999;44(5):1055–63; discussion 63–4.
Qureshi AI, Suri MF, Ringer AJ, Guterman LR, Hopkins LN. Regional intraparenchymal pressure differences in experimental intracerebral hemorrhage: effect of hypertonic saline. Crit Care Med 2002;30(2):435–41.
Ware ML, Nemani VM, Meeker M, Lee C, Morabito DJ, Manley GT. Effects of 23.4% sodium chloride solution in reducing intracranial pressure in patients with traumatic brain injury: a preliminary study. Neurosurgery 2005;57(4):727–36; discussion -36.
Mun-Bryce S, Wilkerson AC, Papuashvili N, Okada YC. Recurring episodes of spreading depression are spontaneously elicited by an intracerebral hemorrhage in the swine. Brain Res 2001;888(2):248–55.
Mun-Bryce S, Wilkerson A, Pacheco B, et al. Depressed cortical excitability and elevated matrix metalloproteinases in remote brain regions following intracerebral hemorrhage. Brain Res 2004;1026(2):227–34.
Mun-Bryce S, Roberts LJ, Hunt WC, Bartolo A, Okada Y. Acute changes in cortical excitability in the cortex contralateral to focal intracerebral hemorrhage in the swine. Brain Res 2004;1026(2):218–26.
Mun-Bryce S, Roberts L, Bartolo A, Okada Y. Transhemispheric depolarizations persist in the intracerebral hemorrhage swine brain following corpus callosal transection. Brain Res 2006;1073–1074:481–90.
Mendelow AD, Gregson BA, Fernandes HM, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet 2005;365(9457):387–97.
Wagner KR, Xi G, Hua Y, et al. Ultra-early clot aspiration after lysis with tissue plasminogen activator in a porcine model of intracerebral hemorrhage: edema reduction and blood–brain barrier protection. J Neurosurg 1999;90(3):491–8.
Thiex R, Kuker W, Muller HD, et al. The long-term effect of recombinant tissue-plasminogen-activator (rt-PA) on edema formation in a large-animal model of intracerebral hemorrhage. Neurol Res 2003;25(3):254–62.
Thiex R, Weis J, Krings T, et al. Addition of intravenous N-methyl-D-aspartate receptor antagonists to local fibrinolytic therapy for the optimal treatment of experimental intracerebral hemorrhages. J Neurosurg 2007;106(2):314–20.
Hemphill JC III, Morabito D, Farrant M, Manley GT. Brain tissue oxygen monitoring in intracerebral hemorrhage. Neurocrit Care 2005;3(3):260–70.
Wagner KR, Xi G, Hua Y, et al. Lobar intracerebral hemorrhage model in pigs: rapid edema development in perihematomal white matter. Stroke 1996;27(3):490–7.
Wagner KR, Xi G, Hua Y, Kleinholz M, de Courten-Myers GM, Myers RE. Early metabolic alterations in edematous perihematomal brain regions following experimental intracerebral hemorrhage. J Neurosurg 1998;88(6):1058–65.
Wagner KR, Packard BA, Hall CL, et al. Protein oxidation and heme oxygenase-1 induction in porcine white matter following intracerebral infusions of whole blood or plasma. Dev Neurosci 2002;24(2–3):154–60.
Wagner KR, Beiler S, Beiler C, et al. Delayed profound local brain hypothermia markedly reduces interleukin-1beta gene expression and vasogenic edema development in a porcine model of intracerebral hemorrhage. Acta Neurochir Suppl 2006;96:177–82.
Wagner KR, Hua Y, de Courten-Myers GM, et al. Tin-mesoporphyrin, a potent heme oxygenase inhibitor, for treatment of intracerebral hemorrhage: in vivo and in vitro studies. Cell Mol Biol (Noisy-le-grand) 2000;46(3):597–608.
Gong Y, Tian H, Xi G, Keep RF, Hoff JT, Hua Y. Systemic zinc protoporphyrin administration reduces intracerebral hemorrhage-induced brain injury. Acta Neurochir Suppl 2006;96:232–6.
Kaufman HH, Pruessner JL, Bernstein DP, Borit A, Ostrow PT, Cahall DL. A rabbit model of intracerebral hematoma. Acta Neuropathol (Berl) 1985;65(3–4):318–21.
Gustafsson O, Rossitti S, Ericsson A, Raininko R. MR imaging of experimentally induced intracranial hemorrhage in rabbits during the first 6 hours. Acta Radiol 1999;40(4):360–8.
Alemany Ripoll M, Gustafsson O, Siosteen B, Olsson Y, Raininko R. MR follow-up of small experimental intracranial haemorrhages from hyperacute to subacute phase. Acta Radiol 2002;43(1):2–9.
Narayan RK, Narayan TM, Katz DA, Kornblith PL, Murano G. Lysis of intracranial hematomas with urokinase in a rabbit model. J Neurosurg 1985;62(4):580–6.
Thai QA, Pradilla G, Legnani FG, Kretzer RM, Hsu W, Tamargo RJ. Lysis of intracerebral hematoma with stereotactically implanted tissue plasminogen activator polymers in a rabbit model. J Neurosurg 2006;105(3):424–9.
Qureshi AI, Ali Z, Suri MF, et al. Extracellular glutamate and other amino acids in experimental intracerebral hemorrhage: an in vivo microdialysis study. Crit Care Med 2003;31(5):1482–9.
Qureshi AI, Ling GS, Khan J, et al. Quantitative analysis of injured, necrotic, and apoptotic cells in a new experimental model of intracerebral hemorrhage. Crit Care Med 2001;29(1):152–7.
Koeppen AH, Dickson AC, McEvoy JA. The cellular reactions to experimental intracerebral hemorrhage. J Neurol Sci 1995;134(Suppl):102–12.
Koeppen AH, Dickson AC, Smith J. Heme oxygenase in experimental intracerebral hemorrhage: the benefit of tin-mesoporphyrin. J Neuropathol Exp Neurol 2004;63(6):587–97.
Aydin MD, Erdogan AR, Cevli SC, Gundogdu C, Dane S, Diyarbakirli S. Ganglionary mechanisms of spasticity and ileus in cerebral hemorrhage: an experimental study. Int J Dev Neurosci 2006;24(7):455–9.
Karwacki Z, Kowianski P, Morys J, Dziewiatkowski J, Kaczmarek E, Suchorzewska J. Effect of sevoflurane on intracranial pressure and cardiovascular function in rabbits with experimental intracerebral haematoma. Med Sci Monit 2001;7(2):212–7.
Bullock R, Mendelow AD, Teasdale GM, Graham DI. Intracranial haemorrhage induced at arterial pressure in the rat. Part 1: Description of technique, ICP changes and neuropathological findings. Neurol Res 1984;6(4):184–8.
Sinar EJ, Mendelow AD, Graham DI, Teasdale GM. Experimental intracerebral hemorrhage: effects of a temporary mass lesion. J Neurosurg 1987;66(4):568–76.
Kingman TA, Mendelow AD, Graham DI, Teasdale GM. Experimental intracerebral mass: description of model, intracranial pressure changes and neuropathology. J Neuropathol Exp Neurol 1988;47(2):128–37.
Nath FP, Jenkins A, Mendelow AD, Graham DI, Teasdale GM. Early hemodynamic changes in experimental intracerebral hemorrhage. J Neurosurg 1986;65(5):697–703.
Xi G, Keep RF, Hoff JT. Erythrocytes and delayed brain edema formation following intracerebral hemorrhage in rats. J Neurosurg 1998;89(6):991–6.
Hua Y, Xi G, Keep RF, Hoff JT. Complement activation in the brain after experimental intracerebral hemorrhage. J Neurosurg 2000;92(6):1016–22.
Xi G, Hua Y, Keep RF, Younger JG, Hoff JT. Systemic complement depletion diminishes perihematomal brain edema in rats. Stroke 2001;32(1):162–7.
Peeling J, Del Bigio MR, Corbett D, Green AR, Jackson DM. Efficacy of disodium 4-[(tert-butylimino)methyl]benzene-1,3-disulfonate N-oxide (NXY-059), a free radical trapping agent, in a rat model of hemorrhagic stroke. Neuropharmacology 2001;40(3):433–9.
Wang X, Mori T, Sumii T, Lo EH. Hemoglobin-induced cytotoxicity in rat cerebral cortical neurons: caspase activation and oxidative stress. Stroke 2002;33(7):1882–8.
Qureshi AI, Suri MF, Ostrow PT, et al. Apoptosis as a form of cell death in intracerebral hemorrhage. Neurosurgery 2003;52(5):1041–7; discussion 7–8.
Allan SM, Rothwell NJ. Inflammation in central nervous system injury. Philos Trans R Soc Lond B Biol Sci 2003;358(1438):1669–77.
Wang J, Dore S. Inflammation after intracerebral hemorrhage. J Cereb Blood Flow Metab 2007;27(5):894–908.
Barnes PJ, Karin M. Nuclear factor-kappaB: a pivotal transcription factor in chronic inflammatory diseases. N Engl J Med 1997;336(15):1066–71.
Mayne M, Ni W, Yan HJ, et al. Antisense oligodeoxynucleotide inhibition of tumor necrosis factor-alpha expression is neuroprotective after intracerebral hemorrhage. Stroke 2001;32(1):240–8.
Wagner KR. Modeling intracerebral hemorrhage: glutamate, nuclear factor-kappa B signaling and cytokines. Stroke 2007;38(2 Suppl):753–8.
Masada T, Hua Y, Xi G, Yang GY, Hoff JT, Keep RF. Attenuation of intracerebral hemorrhage and thrombin-induced brain edema by overexpression of interleukin-1 receptor antagonist. J Neurosurg 2001;95(4):680–6.
Masada T, Hua Y, Xi G, et al. Overexpression of interleukin-1 receptor antagonist reduces brain edema induced by intracerebral hemorrhage and thrombin. Acta Neurochir Suppl 2003;86:463–7.
Sinn DI, Chu K, Lee ST, et al. Pharmacological induction of heat shock protein exerts neuroprotective effects in experimental intracerebral hemorrhage. Brain Res 2007;1135(1):167–76.
Zhao X, Zhang Y, Strong R, Grotta JC, Aronowski J. 15d-Prostaglandin J2 activates peroxisome proliferator-activated receptor-gamma, promotes expression of catalase, and reduces inflammation, behavioral dysfunction, and neuronal loss after intracerebral hemorrhage in rats. J Cereb Blood Flow Metab 2006;26(6):811–20.
Wang J, Rogove AD, Tsirka AE, Tsirka SE. Protective role of tuftsin fragment 1–3 in an animal model of intracerebral hemorrhage. Ann Neurol 2003;54(5):655–64.
Imamura N, Hida H, Aihara N, et al. Neurodegeneration of substantia nigra accompanied with macrophage/microglia infiltration after intrastriatal hemorrhage. Neurosci Res 2003;46(3):289–98.
Colton CA, Gilbert DL. Microglia, an in vivo source of reactive oxygen species in the brain. Adv Neurol 1993;59:321–6.
Hanisch UK. Microglia as a source and target of cytokines. Glia 2002;40(2):140–55.
Koeppen AH. The history of iron in the brain. J Neurol Sci 1995;134(Suppl):1–9.
Van Beek J, Chan P, Bernaudin M, Petit E, MacKenzie ET, Fontaine M. Glial responses, clusterin, and complement in permanent focal cerebral ischemia in the mouse. Glia 2000;31(1):39–50.
Wang J, Tsirka SE. Contribution of extracellular proteolysis and microglia to intracerebral hemorrhage. Neurocrit Care 2005;3(1):77–85.
Gong C, Hoff JT, Keep RF. Acute inflammatory reaction following experimental intracerebral hemorrhage in rat. Brain Res 2000;871(1):57–65.
Hickenbottom SL, Grotta JC, Strong R, Denner LA, Aronowski J. Nuclear factor-kappaB and cell death after experimental intracerebral hemorrhage in rats. Stroke 1999;30(11):2472–7; discussion 7–8.
Xue M, Del Bigio MR. Intracerebral injection of autologous whole blood in rats: time course of inflammation and cell death. Neurosci Lett 2000;283(3):230–2.
Power C, Henry S, Del Bigio MR, et al. Intracerebral hemorrhage induces macrophage activation and matrix metalloproteinases. Ann Neurol 2003;53(6):731–42.
Wasserman JK, Schlichter LC. Neuron death and inflammation in a rat model of intracerebral hemorrhage: effects of delayed minocycline treatment. Brain Res 2007;1136(1):208–18.
Jung KH, Chu K, Jeong SW, et al. HMG-CoA reductase inhibitor, atorvastatin, promotes sensorimotor recovery, suppressing acute inflammatory reaction after experimental intracerebral hemorrhage. Stroke 2004;35(7):1744–9.
Karwacki Z, Kowianski P, Dziewiatkowski J, et al. Quantitative analysis of influence of sevoflurane on the reactivity of microglial cells in the course of the experimental model of intracerebral haemorrhage. Eur J Anaesthesiol 2006;23(10):874–81.
Karwacki Z, Kowianski P, Dziewiatowski J, et al. The effect of propofol on astro- and microglial reactivity in the course of experimental intracerebral haemorrhage in rats. Folia Neuropathol 2006;44(1):50–8.
Yokota H, Yoshikawa M, Hirabayashi H, et al. Expression of ciliary neurotrophic factor (CNTF), CNTF receptor alpha (CNTFR-alpha) following experimental intracerebral hemorrhage in rats. Neurosci Lett 2005;377(3):170–5.
Altumbabic M, Peeling J, Del Bigio MR. Intracerebral hemorrhage in the rat: effects of hematoma aspiration. Stroke 1998;29(9):1917–22; discussion 22–3.
Nonaka M, Yoshikawa M, Nishimura F, et al. Intraventricular transplantation of embryonic stem cell-derived neural stem cells in intracerebral hemorrhage rats. Neurol Res 2004;26(3):265–72.
Rosenberg GA, Estrada EY, Mobashery S. Effect of synthetic matrix metalloproteinase inhibitors on lipopolysaccharide-induced blood–brain barrier opening in rodents: Differences in response based on strains and solvents. Brain Res 2006.
Wells JE, Biernaskie J, Szymanska A, Larsen PH, Yong VW, Corbett D. Matrix metalloproteinase (MMP)-12 expression has a negative impact on sensorimotor function following intracerebral haemorrhage in mice. Eur J Neurosci 2005;21(1):187–96.
Tang J, Liu J, Zhou C, et al. Mmp-9 deficiency enhances collagenase-induced intracerebral hemorrhage and brain injury in mutant mice. J Cereb Blood Flow Metab 2004;24(10):1133–45.
Lee JM, Yin K, Hsin I, et al. Matrix metalloproteinase-9 in cerebral-amyloid-angiopathy-related hemorrhage. J Neurol Sci 2005;229–230:249–54.
Wang J, Tsirka SE. Neuroprotection by inhibition of matrix metalloproteinases in a mouse model of intracerebral haemorrhage. Brain 2005;128(Pt 7):1622–33.
Lee ST, Chu K, Jung KH, et al. Memantine reduces hematoma expansion in experimental intracerebral hemorrhage, resulting in functional improvement. J Cereb Blood Flow Metab 2006;26(4):536–44.
Rosenberg GA, Navratil M. Metalloproteinase inhibition blocks edema in intracerebral hemorrhage in the rat. Neurology 1997;48(4):921–6.
Gong C, Boulis N, Qian J, Turner DE, Hoff JT, Keep RF. Intracerebral hemorrhage-induced neuronal death. Neurosurgery 2001;48(4):875–82; discussion 82–3.
Matz PG, Lewen A, Chan PH. Neuronal, but not microglial, accumulation of extravasated serum proteins after intracerebral hemolysate exposure is accompanied by cytochrome c release and DNA fragmentation. J Cereb Blood Flow Metab 2001;21(8):921–8.
Felberg RA, Grotta JC, Shirzadi AL, et al. Cell death in experimental intracerebral hemorrhage: the “black hole” model of hemorrhagic damage. Ann Neurol 2002;51(4):517–24.
Sinn DI, Lee ST, Chu K, et al. Combined neuroprotective effects of celecoxib and memantine in experimental intracerebral hemorrhage. Neurosci Lett 2007;411(3):238–42.
Lee ST, Chu K, Sinn DI, et al. Erythropoietin reduces perihematomal inflammation and cell death with eNOS and STAT3 activations in experimental intracerebral hemorrhage. J Neurochem 2006;96(6):1728–39.
Peeling J, Yan HJ, Corbett D, Xue M, Del Bigio MR. Effect of FK-506 on inflammation and behavioral outcome following intracerebral hemorrhage in rat. Exp Neurol 2001;167(2):341–7.
Mayne M, Fotheringham J, Yan HJ, et al. Adenosine A2A receptor activation reduces proinflammatory events and decreases cell death following intracerebral hemorrhage. Ann Neurol 2001;49(6):727–35.
Rodrigues CM, Sola S, Nan Z, et al. Tauroursodeoxycholic acid reduces apoptosis and protects against neurological injury after acute hemorrhagic stroke in rats. Proc Natl Acad Sci USA 2003;100(10):6087–92.
Sayah S, Ischenko AM, Zhakhov A, Bonnard AS, Fontaine M. Expression of cytokines by human astrocytomas following stimulation by C3a and C5a anaphylatoxins: specific increase in interleukin-6 mRNA expression. J Neurochem 1999;72(6):2426–36.
Wu G, Huang FP. Effects of venom defibrase on brain edema after intracerebral hemorrhage in rats. Acta Neurochir Suppl 2005;95:381–7.
Yang S, Nakamura T, Hua Y, et al. Intracerebral hemorrhage in complement C3-deficient mice. Acta Neurochir Suppl 2006;96:227–31.
Nakamura T, Keep RF, Hua Y, Schallert T, Hoff JT, Xi G. Deferoxamine-induced attenuation of brain edema and neurological deficits in a rat model of intracerebral hemorrhage. J Neurosurg 2004;100(4):672–8.
Wagner KR, Sharp FR, Ardizzone TD, Lu A, Clark JF. Heme and iron metabolism: role in cerebral hemorrhage. J Cereb Blood Flow Metab 2003;23(6):629–52.
Wu J, Hua Y, Keep RF, Schallert T, Hoff JT, Xi G. Oxidative brain injury from extravasated erythrocytes after intracerebral hemorrhage. Brain Res 2002;953(1–2):45–52.
Tang J, Liu J, Zhou C, et al. Role of NADPH oxidase in the brain injury of intracerebral hemorrhage. J Neurochem 2005;94(5):1342–50.
Qu Y, Chen-Roetling J, Benvenisti-Zarom L, Regan RF. Attenuation of oxidative injury after induction of experimental intracerebral hemorrhage in heme oxygenase-2 knockout mice. J Neurosurg 2007;106(3):428–35.
Peeling J, Yan HJ, Chen SG, Campbell M, Del Bigio MR. Protective effects of free radical inhibitors in intracerebral hemorrhage in rat. Brain Res 1998;795(1–2):63–70.
Suzuki K, Nakazato K, Kusakabe T, Nagamine T, Sakurai H, Takatama M. Role of oxidative stress on pathogenesis of hypertensive cerebrovascular lesions. Pathology international 2007;57(3):133–9.
Nakamura T, Keep RF, Hua Y, Nagao S, Hoff JT, Xi G. Iron-induced oxidative brain injury after experimental intracerebral hemorrhage. Acta Neurochir Suppl 2006;96:194–8.
Nakamura T, Keep RF, Hua Y, Hoff JT, Xi G. Oxidative DNA injury after experimental intracerebral hemorrhage. Brain Res 2005;1039(1–2):30–6.
Winkler DT, Bondolfi L, Herzig MC, et al. Spontaneous hemorrhagic stroke in a mouse model of cerebral amyloid angiopathy. J Neurosci 2001;21(5):1619–27.
Nakamura T, Xi G, Hua Y, Schallert T, Hoff JT, Keep RF. Intracerebral hemorrhage in mice: model characterization and application for genetically modified mice. J Cereb Blood Flow Metab 2004;24(5):487–94.
Thiex R, Mayfrank L, Rohde V, Gilsbach JM, Tsirka SA. The role of endogenous versus exogenous tPA on edema formation in murine ICH. Exp Neurol 2004;189(1):25–32.
Weisgraber KH. Apolipoprotein E: structure–function relationships. Advances in protein chemistry 1994;45:249–302.
Alberts MJ, Graffagnino C, McClenny C, et al. ApoE genotype and survival from intracerebral haemorrhage. Lancet 1995;346(8974):575.
Sullivan PM, Mezdour H, Aratani Y, et al. Targeted replacement of the mouse apolipoprotein E gene with the common human APOE3 allele enhances diet-induced hypercholesterolemia and atherosclerosis. J Biol Chem 1997;272(29):17972–80.
Lynch JR, Pineda JA, Morgan D, et al. Apolipoprotein E affects the central nervous system response to injury and the development of cerebral edema. Ann Neurol 2002;51(1):113–7.
Lynch JR, Tang W, Wang H, et al. APOE genotype and an ApoE-mimetic peptide modify the systemic and central nervous system inflammatory response. J Biol Chem 2003;278(49):48529–33.
Lynch JR, Wang H, Mace B, et al. A novel therapeutic derived from apolipoprotein E reduces brain inflammation and improves outcome after closed head injury. Exp Neurol 2005;192(1):109–16.
Gao J, Wang H, Sheng H, et al. A novel apoE-derived therapeutic reduces vasospasm and improves outcome in a murine model of subarachnoid hemorrhage. Neurocrit Care 2006;4(1):25–31.
Laskowitz DT, McKenna SE, Song P, et al. COG1410, a novel apolipoprotein E-based peptide, improves functional recovery in a murine model of traumatic brain injury. J Neurotrauma 2007;24(7):1093–107.
Del Bigio MR, Yan HJ, Buist R, Peeling J. Experimental intracerebral hemorrhage in rats. Magnetic resonance imaging and histopathological correlates. Stroke 1996;27(12):2312–9; discussion 9–20.
Orakcioglu B, Fiebach JB, Steiner T, et al. Evolution of early perihemorrhagic changes–ischemia vs. edema: an MRI study in rats. Exp Neurol 2005;193(2):369–76.
Elger B, Seega J, Brendel R. Magnetic resonance imaging study on the effect of levemopamil on the size of intracerebral hemorrhage in rats. Stroke 1994;25(9):1836–41.
Del Bigio MR, Yan HJ, Campbell TM, Peeling J. Effect of fucoidan treatment on collagenase-induced intracerebral hemorrhage in rats. Neurol Res 1999;21(4):415–9.
Del Bigio MR, Yan HJ, Xue M. Intracerebral infusion of a second-generation ciliary neurotrophic factor reduces neuronal loss in rat striatum following experimental intracerebral hemorrhage. J Neurol Sci 2001;192(1–2):53–9.
Xi G, Keep RF, Hoff JT. Pathophysiology of brain edema formation. Neurosurg Clin N Am 2002;13(3):371–83.
Mendelow AD, Unterberg A. Surgical treatment of intracerebral haemorrhage. Curr Opin Crit Care 2007;13(2):169–74.
Thiex R, Kuker W, Jungbluth P, et al. Minor inflammation after surgical evacuation compared with fibrinolytic therapy of experimental intracerebral hemorrhages. Neurol Res 2005;27(5):493–8.
Stroick M, Alonso A, Fatar M, et al. Effects of simultaneous application of ultrasound and microbubbles on intracerebral hemorrhage in an animal model. Ultrasound Med Biol 2006;32(9):1377–82.
Kawai N, Nakamura T, Nagao S. Early hemostatic therapy using recombinant factor VIIa in a collagenase-induced intracerebral hemorrhage model in rats. Acta Neurochir Suppl 2006;96:212–7.
MacLellan CL, Davies LM, Fingas MS, Colbourne F. The influence of hypothermia on outcome after intracerebral hemorrhage in rats. Stroke 2006;37(5):1266–70.
Maclellan CL, Grams J, Adams K, Colbourne F. Combined use of a cytoprotectant and rehabilitation therapy after severe intracerebral hemorrhage in rats. Brain Res 2005;1063(1):40–7.
Huang FP, Xi G, Keep RF, Hua Y, Nemoianu A, Hoff JT. Brain edema after experimental intracerebral hemorrhage: role of hemoglobin degradation products. J Neurosurg 2002;96(2):287–93.
Ardizzone TD, Lu A, Wagner KR, Tang Y, Ran R, Sharp FR. Glutamate receptor blockade attenuates glucose hypermetabolism in perihematomal brain after experimental intracerebral hemorrhage in rat. Stroke 2004;35(11):2587–91.
Chu K, Jeong SW, Jung KH, et al. Celecoxib induces functional recovery after intracerebral hemorrhage with reduction of brain edema and perihematomal cell death. J Cereb Blood Flow Metab 2004;24(8):926–33.
Seyfried D, Han Y, Lu D, Chen J, Bydon A, Chopp M. Improvement in neurological outcome after administration of atorvastatin following experimental intracerebral hemorrhage in rats. J Neurosurg 2004;101(1):104–7.
Seyfried D, Ding J, Han Y, Li Y, Chen J, Chopp M. Effects of intravenous administration of human bone marrow stromal cells after intracerebral hemorrhage in rats. J Neurosurg 2006;104(2):313–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
James, M.L., Warner, D.S. & Laskowitz, D.T. Preclinical Models of Intracerebral Hemorrhage: A Translational Perspective. Neurocrit Care 9, 139–152 (2008). https://doi.org/10.1007/s12028-007-9030-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-007-9030-2