
Abstract
Physical abuse of children has many manifestations. Depending on the type of force involved, specific injury patterns are produced on the body of the child, the morphology and localization of which are forensically relevant in terms of diagnostic classification as child abuse. Typical patterned bruising includes, for example, tramline bruises resulting from blows with oblong, stick-like objects. In addition to rounded or one-sided horseshoe-shaped bite injuries, injuries of different ages, clustered injuries (e.g., three or more individual injuries in the same body region), and thermal injuries are typical results of abuse. Abusive scalds are usually characterized by a symmetrical impression and localization with sharp delineation of the scald wound edges, in contrast to accidental scalding injuries with radiating splash patterns ending in tapered points. The coloration of a hematoma can help indicate the time when the injury occurred. Lack of a coherent and comprehensible explanation for accidental injury constitutes grounds for suspecting abuse. Suspicions should be raised in cases of a delayed visit to a doctor, waiting for an unusually long period before summoning emergency medical help for serious injuries to a child, and when differing versions of a purported accident are provided. Documentation of the findings is highly relevant in later reviews of the diagnosis, for instance, when new relevant facts and investigative results come to light in subsequent criminal proceedings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Physical abuse of children usually takes the form of simple physical violence, but the manifestations are extremely diverse. Children may be beaten with the flat of the hand, fist, or other objects against the head, buttocks, torso or limbs, or kicked in these places. They may be thrown against walls and furniture or onto the floor. They might be bitten, choked, throttled or have their hair pulled or torn out in tufts. The outer ear can be twisted or pulled. Children may be doused or showered with ice-cold or hot/boiling water or placed or forced into a bathtub with hot water. Heated objects might be pressed onto their skin (e.g., the tip of a lit cigarette or a metal spoon) or they might be forced into partial or complete immobility by fettering or bondage with ropes or chains or forced into very narrow spaces (e.g., boxes and crates).
Depending on the nature of the force and the scale of the attack, hematomas, lacerations, abrasions, choke marks, throttling marks, thermal injuries in the form of scalds and burns, or skin necrosis resulting from sustained exposure to very cold temperatures are produced on the surface of the child’s body.
Localized results of abuse beneath the protective layer of skin include fractures and distortions affecting bones, ligaments, and joints. Internal organs such as the liver, spleen, and pancreas, as well as the stomach and/or intestines, may be injured or ruptured. Life-threatening or even fatal bleeding inside the abdomen often results from these injuries. Fatal late complications such as peritonitis or septicemia also occur as direct causal results of such abuse.
Patterned bruising can be inflicted upon children with various objects such as electric cables, cooking spoons, bludgeons, and dog leashes.
The “negative impression” of the object used for beating and thus injury is not the only essential diagnostic criterion for cutaneous injuries in child abuse. The location of injuries, the presence of so-called “clustered” injuries and injuries of different ages (“repeated injuries”) can also be highly decisive in diagnosing cases of child abuse.
The present paper addresses the classification of cutaneous injuries in child abuse and the typical findings. In addition to the traditional criteria given in Table 1, “hidden injuries,” findings resulting from forced closure of airways and thermal lesions, are also addressed regarding their diagnostic classification and interpretation in cases of child abuse.
Classification of cutaneous injuries of child abuse
Localization
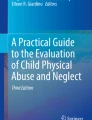
The criterion localization of injuries can contribute decisively to differentiation between accidental origin (e.g., falling while playing, climbing or romping at home or outdoors) and abuse-related causes (Fig. 1a, b). The forehead, tip of the nose, and chin are injury locations typical of accidental falls. Typical locations for abuse-related injuries to the face are the eyes (monocular hematoma or “raccoon eyes”), lips and oral mucosa (also within the oral cavity), and the outer ears (Fig. 2) [1–4]. Injuries on the back and buttocks (Fig. 3) and on the lateral and posterior sides of the thighs and soles of the feet (Fig. 4) are also typical results of abuse. The same applies to injuries localized on the outer sides of the forearms and back of the hands (so-called “defensive injuries”) [1].

Injury localization on a child. a Localizations typical of accidental falling. b Localizations typical of abuse

Hematoma of the right external ear as a result of severe pulling of the ear and slapping (♂, 2 years of age)

Large hematoma on the buttocks as a result of blows with a hand on bared buttocks (♂, 3 years of age)

Scald on the soles of the feet (♀, 4 weeks of age)
Patterned bruising/patterned injuries
Because of their morphology (including the outline, spared area within the injury, distances between structures, and size), patterned injuries allow for conclusions as to the weapon used (“instrumentality”). A “negative impression” of the object used to strike the child, and thus directly causing the injury, is produced on a scale of 1:1 (Fig. 5).

Patterned bruising corresponding to the sole of a sport shoe resulting from a kick in the face (♂, 2 years of age)
“Tramline” bruises are a form of child abuse injury that is repeatedly observed; these represent a classic example of a patterned injury. Blows administered with oblong, stick-like objects (Fig. 6), straps, or electric cables (Fig. 7), produce typical tramline bruises characterized by an area of central pallor outlined by two narrow parallel lines of bruising [1]. The blow presses vascular blood into the adjacent vessels under considerable pressure. The vessels cannot withstand the rapid intravascular pressure increase and rupture, resulting in strip-shaped hematomas along the edges of the impacted area (Fig. 8). The central area of pallor reproduces the shape and size of the object used to deliver the blow (a careful photographic documentation with scale is a prerequisite for later interpretation and reconstruction of events).

Tramline bruises due to a blow from a stick. Note central pallor outlined by two narrow parallel lines of bruising (♀, 5 years of age)

Tramline bruises on the lower arm as a result of whipping with a mobile phone charger cable (♀, 13 years of age)

Pathogenesis of tramline bruises (see text for further details)
Finger impressions may also be left on a child’s body as a result of slapping, mainly on the face, with corresponding tramline bruises; an imprint of the entire hand that struck the blow may also be produced in the form of a patterned hematoma. Punches, in which the knuckles strike the child, produce, depending on the intensity of the blow, rounded hematomas with a diameter of 0.8–1.5 cm on the child’s skin (Fig. 9).

Older hematomas of different ages on the back (♂, 2 years of age)
Bite injuries
Bite injuries show a typical pattern since they reproduce the imprint of the teeth/dentition that caused them (Fig. 10). Bite marks usually have a rounded to oval form because of the two opposing horseshoe-shaped imprints of the upper and lower jaws. In adult dentition, the distance between the canines exceeds 2.5 cm; in children this distance does not exceed 2.5 cm [5]. The center of a bite hematoma may also show a suction component near the actual bite injury (the causal mechanism is the same as for a “love bite” or “hickey”). One-sided bite injuries, in which the impression of the opposing upper or lower jaw is lacking, are also frequently observed, in particular, on children’s extremities (Fig. 11). Therefore, a rounded or oval form is not necessarily required for diagnosis of a bite injury [4–7].

Two directly adjacent bite marks on lower leg of a child inflicted by an adult (♀, 3 years of age)

One-sided horseshoe-shaped bite injury inflicted by an adult on the lower leg of an infant (♂, 2 months of age)
Repeated injuries
The term repeated injuries refers to the coexistence of injuries of different ages. The decisive criterion in such cases is the variation in hematoma coloration [8]. Confirmation of repeated injuries is not restricted to hematomas on the body surface. Radiological evidence of fractures of different ages, i.e., coexistence of fresh fractures alongside healing or healed fractures, is also a diagnostic indication of abuse—assuming internal pathologies such as brittle-bone disease, specific bone mineralization disorders involving calcium or phosphate metabolism disorders and vitamin D deficiency (rickets) have been excluded [9].
Clustered injuries
The term clustered injuries refers to three or more individual injuries in the same body region (Fig. 12). Clustered injuries cannot be explained by accidents involving falling or repeated accidental or inadvertent bumping up against the edge of something, for example, during wild romping or playing [10].

Clustered injuries on the left upper and lower arm and on the left flank (♀, 9 years of age)
Hidden/discrete injuries
Even in a completely unclothed child, injuries to the oral cavity and the region behind the ears are not seen at first glance and are only revealed by a more detailed examination.
Injuries to the oral mucosa within the oral cavity, on the inner side of the lips or labial frenulum, can be caused, for example, by forced insertion and retraction of a finger or object (e.g., a spoon used in feeding).
During the physical examination, both ear flaps must be folded over anteriorly somewhat to investigate the skin region otherwise covered by the ear. Hematomas or skin tears may be hidden around the base of the external ear (caused by violent pulling or twisting of the ear). The skin region behind the ears is also a predilection site for petechia as a sign of strangulation.
Among the various forms of injuries to the neck, marks due to manual strangulation often have an unspecific appearance (Fig. 13). They may be observed as superficial reddening of the skin only, without any additional skin abrasions or scratches caused by fingernails, and are easily confused with transient skin irritations, e.g., those resulting from wearing tight or scratchy clothing at the neck.

Cutaneous marks due to manual strangulation (♂, 7 years of age)
Findings resulting from mechanical occlusion of the external airways
Forced mechanical obstruction or occlusion of the mouth, or both the mouth and nose at the same time—not only to prevent the child from screaming, but also to break his or her will by causing fear of death (via inducing a sensation of suffocation)—may leave few traces such as tiny, discrete patchy skin abrasions around the mouth and nose, facial petechiae or sometimes no traces at all [11, 12]. Although presumably rare, intentional asphyxiation of infants in most cases remains almost impossible to distinguish from sudden infant death syndrome (SIDS) or sudden unexplained infant death (SUID) [13]. An unambiguous pattern of trace evidence is found in only a few (fatal) cases with large areas of dry skin around the breathing orifices, in some cases with patterned areas of uninjured skin (Fig. 14). These spared areas correspond to skin areas not covered by the fingertips where superficial epithelium detachment and subsequent drying did not occur later.

Fatal smothering. This baby was choked to death by occlusion of the mouth and nose by the hand of an adult. Large areas of dried skin next to smaller areas of uninjured skin correspond to skin areas not covered by the fingers of the perpetrator (♂, 4 days old at death)
Thermal injuries
Hypothermia induced by cold water, e.g., from long-lasting showering of the child with ice-cold water, is not detectable by any outwardly visible signs. The skin changes (primary pallor followed by transient hyperemia) are nonspecific and are no longer detectable at the time of examination, so that suspicion of intentionally induced hypothermia could only arise based on measurement of body temperature in the absence of a coherent explanation for hypothermia.
In addition to abusive intent, effects of heat application may also result from accidents (possibly involving neglect of supervisory responsibility, which could then be criminally pursued as, for example, manslaughter). It is usually possible to arrive at a differentiated conclusion based on the injury pattern (localization and morphology) against the background of the information provided as to the course of events.
Thermal heat injuries are further differentiated as either scalds (direct skin contact with hot liquid, and less frequently with water or steam) or burns (direct skin contact with an open flame or hot object, or on rare occasions, heat irradiation into the skin from an object).
The severity of the resulting thermal lesion is the product of temperature and exposure time.
Scalds
Symmetrical scalds on the extremities due to immersion of or placing the child in hot bathwater are typical of abuse. But unilateral scalds are also observed (Fig. 15). The sharp boundary of scalding at the edges (bath water level) is essential for the correct diagnostic classification. Accidental dousing with hot water always results in scald injuries in the form of splash patterns ending in tapered points and non-uniform (blurred) edges [14].

Stocking-pattern scalding caused by forcing the child into 75 °C hot bathwater (♂, 3 years of age)
Burns
Contact burns are caused by pressing a heated object against the skin or pressing the child’s body against such an object (e.g., a hotplate; Fig. 16). The criteria that must be checked for contact burns resulting from abusive treatment are localization (in particular, the back, buttocks, and outer sides of the arms and legs) and patterned injury (for potential reproduction of the outline of the hot object on the skin, e.g., a metal spoon).

Burn injury on buttocks caused by pressing the bared buttocks of the child onto a hot hotplate (♂, 1 year of age)
A typical cigarette burn is rounded to slightly oval, often with a central depression, and between 0.5 and 1 cm in diameter (Fig. 17) [15].

Cigarette burns on the back (♀, 6 years of age)
The question of plausibility: discrepancy versus congruence
The lack of a coherent and comprehensible explanation for accidental injury, assuming exclusion of possible differential diagnoses (injuries due to illness or internal causes), is highly suspicious for abuse [1, 16]. Although such a suspicion may be occasioned by a wide variety of circumstances, discrepancies between the injury as presented and the incident as described would normally be strongly indicative. The investigator must be highly attentive and must subject the described incident to critical scrutiny if such discrepancies are to be uncovered. It must be determined initially whether the explanation of how the injury occurred as provided by the parents or other caregivers present when it occurred is congruent with the established findings. For example, bilateral or symmetrical injuries, not only to the face or on the head, would speak against an accident involving a fall. It must also be determined with critical acuity whether the motor development of the child (which of course depends on not only the age of the child but also the support provided by caregivers in the child’s previous history) is congruent with what is described [4, 17, 18]. For example, an unassisted 2-year-old child would not be capable of climbing onto a cooker and switching it on (and subsequently suffering thermal injuries from the hotplates), either in terms of the motor capabilities or the cognitive planning and execution required for such complex actions.
A delayed visit to a doctor, waiting unusually long before calling for emergency medical help, or presenting the child in an emergency ward for serious injuries, regardless of the type of injury, is always highly suspicious. This also applies when differing versions of a purported accident are provided.
However, forensic practice has repeatedly shown that there are sometimes ordinary explanations for injuries that have a nearly similar morphological appearance as those typically abuse-related [14, 19]. For instance, a particular Asian massage technique in which cutaneous hyperemia is induced by use of various objects such as coins, spoons or special scrapers can result in suspicious skin lesions [1]. Although these techniques, when used as alternative therapeutic methods, are not painful, the intracutaneous hematomas that occasionally result from those practices, particularly on the back, are readily misinterpreted as tramline bruises as a result of, for example, blows with a stick.
Documentation of findings
Securing and recording of findings is highly relevant in later reviews of the diagnosis, for instance, when new relevant facts and investigative results come to light in subsequent criminal proceedings.
Documentation of findings must include, in addition to a detailed description of the criteria listed in Table 1 (optional), the type of injury involved (e.g., hematoma, abrasion, and thermal lesion), dimensions, and photographic documentation including a visual scale [20].
Abnormal behavior of the child during the examination (e.g., fear, utter passivity, excessive conformity, extreme submissiveness, aggression, and destructive behavior) should be interpreted as an urgent indication for consultation with a child psychiatrist or a psychologist with appropriate training and experience.
Key points
-
1.
The diagnostic criteria for cutaneous injuries in child abuse are localization, patterned bruising, repeated injuries (juxtaposition of injuries of different ages) and clustered injuries (three or more individual injuries in the same body region).
-
2.
Thermal injuries and bite injuries in children are always suspicious of abusive origin.
-
3.
Detailed documentation of findings (i.e., photographic documentation with a visual scale), among other things, is absolutely essential for any subsequent criminal proceedings.
-
4.
A thorough examination of the whole body of the affected child in a calm and neutral atmosphere, as well as competent and advanced diagnostics as needed (for instance, imaging techniques, laboratory analyses, and consultation by medical specialists), is essential to the wellbeing of the child—also with a view to exoneration of wrongly suspected parents or caregivers.
-
5.
Possible differential diagnoses of cutaneous lesions in children must be taken into account (if necessary, including consultation by a dermatological specialist).
References
Swerdlin A, Berkowitz C, Craft N. Cutaneous signs of child abuse. J Am Acad Dermatol. 2007;57:371–92.
Chen W, Balaban R, Stanger V, Haruvi R, Zur S, Augarten A. Suspected child abuse and neglect: assessment in a hospital setting. Isr Med Assoc J. 2002;4:617–23.
Pierce MC, Kaczor K, Aldridge S, O’Flynn J, Lorenz DJ. Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics. 2010;125:67–74.
Sugar NF, Taylor JA, Feldman KW. Bruises in infants and toddlers: those who don’t cruise rarely bruise. Puget Sound Pediatric Research Network. Arch Pediatr Adolesc Med. 1999;153:399–403.
Vale GL. Dentistry, bite marks and the investigation of crime. J Calif Dent Assoc. 1996;24:29–34.
Freeman AJ, Senn DR, Arendt DM. Seven hundred seventy eight bite marks: analysis by anatomic location, victim and biter demographics, type of crime, and legal disposition. J Forensic Sci. 2005;50:1436–43.
Page M, Taylor J, Blenkin M. Reality bites—A ten-year retrospective analysis of bitemark casework in Australia. Forensic Sci Int. 2012;216:82–7.
Nuzzolese E, Di Vella G. The development of a colorimetric scale as a visual aid for the bruise age determination of bite marks and blunt trauma. J Forensic Odontostomatol. 2012;30:1–6.
Kocher MS, Kasser JR. Orthopaedic aspects of child abuse. J Am Acad Orthop Surg. 2000;8:10–20.
Maguire S, Mann MK, Sibert J, Kemp A. Are there patterns of bruising in childhood which are diagnostic or suggestive of abuse? A systematic review. Arch Dis Child. 2005;90:182–6.
Oehmichen M, Gerling I, Meissner C. Petechiae of the baby’s skin as differentiation symptom of infanticide versus SIDS. J Forensic Sci. 2000;45:602–7.
Bohnert M, Grosse Perdekamp M, Pollak S. Three subsequent infanticides covered up as SIDS. Int J Legal Med. 2005;119:31–4.
Baker AM. Pediatric asphyxial deaths. In: Collins KA, Byard RW, editors. Forensic pathology of infancy and childhood. New York: Springer; 2014. p. 207–28.
Ellis P. Cutaneous findings in children. In: Collins KA, Byard RW, editors. Forensic pathology of infancy and childhood. New York: Springer; 2014. p. 243–65.
Faller-Marquardt M, Pollak S, Schmidt U. Cigarette burns in forensic medicine. Forensic Sci Int. 2008;176:200–8.
Oranje A, Bilo RA. Skin signs in child abuse and differential diagnosis. Minerva Pediatr. 2011;63:319–25.
Carpenter RF. The prevalence and distribution of bruising in babies. Arch Dis Child. 1999;80:363–6.
Jayakumar P, Barry M, Ramachandran M. Orthopaedic aspects of paediatric non-accidental injury. J Bone Joint Surg Br. 2010;92:189–95.
Li YMM, Wells D. Skin conditions mimicking pediatric inflicted injury. In: Collins KA, Byard RW, editors. Forensic pathology of infancy and childhood. New York: Springer; 2014. p. 267–89.
Melville JD, Lukefahr JL, Cornell J, Kellogg ND, Lancaster JL. The effect of image quality on the assessment of child abuse photographs. Pediatr Emerg Care. 2013;29:607–11.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tsokos, M. Diagnostic criteria for cutaneous injuries in child abuse: classification, findings, and interpretation. Forensic Sci Med Pathol 11, 235–242 (2015). https://doi.org/10.1007/s12024-015-9671-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12024-015-9671-y