
Abstract
CT scanning is an intrinsic component of the workup of all admissions to the Victorian Institute of Forensic Medicine. Using a new system of preliminary examination a decision is made by the coroner as to whether or not an autopsy should occur following consultation with a forensic pathologist. This study examines 318 consecutive cases for the month of July 2010 where the deceased had a preliminary examination including a CT scan which was primarily interpreted by a forensic pathologist. Findings relate to the age and sex of the deceased, the value of CT scanning, pathologist variability in advising an autopsy examination as well as the input from our sessional radiologist. A breakdown of natural versus unnatural death is provided. Overall the process is effective in developing interaction between the medical and legal elements at the VIFM in efforts to process admissions in the most suitable manner.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The preliminary examination and the Victorian coronial system
The Coroners system in the State of Victoria has undergone significant changes as a consequence of the introduction of the Coroners Act (Vic) in 2008 [1].
Under Victoria’s coronial system of death investigation, deaths reportable to the coroner include those which are unexpected, unnatural, violent, accidental, and certain medical procedure-related deaths.
The process is one of independent investigation of death, and the stated objectives of the legislation are to reduce preventable deaths, promote public health, and safety, have regard to the distress of relatives, acknowledge cultural and religious beliefs, and avoid unnecessary delays while at all times giving due consideration to privacy issues.
Over recent years there has been a gradual acknowledgment that the “traditional” full autopsy may not necessarily be required in some cases in order to address coronial requirements or reasonably foreseeable issues of medicolegal importance. As a result, the concept of a preliminary examination has evolved. This procedure allows medical input into the coronial decision making process, noting that Australian coroners are trained in law and not in medicine (although some are nurses or scientists).
Presentation of a body to the VIFM is considered sufficient authority for the performance of a number of procedures, collectively termed preliminary examination. This process draws upon information from a number of sources including a police statement of the circumstances of death, scene photography if available, routine admission CT scanning, examination of medical records, visual inspection of the external aspect of the body, and analysis of body fluids—for instance toxicological screening (Fig. 1).

Preliminary examination pro forma
Armed with this information a pathologist and coroner conduct a daily meeting to discuss the preliminary findings relating to all admissions over the previous day, with the coroner then making a decision with respect to the necessity of an autopsy. The family is informed of the coroner’s decision and their views as to this decision are taken into consideration but are not determinative.
Other parties with a legitimate interest in the type of investigation undertaken may include other family members, clinicians, lawyers, and police.
In summary, the new preliminary examination process requires direct engagement between the medical and legal arms of the death investigation process and requires that families are fully informed of the process.
Methods
This study reviewed 318 cases in the month of July 2010 that underwent preliminary examination and included a full body CT scan on admission. Some cases were not suitable for CT scanning due to excessive weight or girth. Details considered for the purposes of this study included sex, age, type of death (i.e. natural or unnatural) and, of the unnatural death cases a subcategorization into cases of accidental or traumatic death and those considered to be suicide. The cause of death was obtained from the pathologist’s report.
The pathologist involved in each case was recorded as was the number and type of procedures (autopsies or inspections) ultimately performed. Six pathologists and eight coroners were involved during the month of July.
A major interest of this study was the evaluation of the role of the CT scan in this decision making process.
Results
During the month of July 2010 preliminary examinations and full body admission CTs were performed on 318 admissions at VIFM. Five other admissions did not receive CT scanning due to issues of size/weight.
Sex and age
There were 209 males and 109 females. The average male age was 56.5 years with a median age of 57 years. The average female age was 68.9 and the median age 77 years. There were only two females under the age of 20, including a 1 day old baby. There were eleven males less than 20 years of age, including three infants.
Outcomes
Six pathologists were involved in the preliminary examination process in the month of July. When a post-mortem was not ordered by a coroner, the pathologist would provide a report detailing relevant background circumstances, medical history, CT scan findings plus an external inspection of the body. This is referred to as an I and R, or inspection and report. The rates of post-mortem and inspection and report (I and R) are tabulated in Fig. 2.

Inspection and reports by pathologist
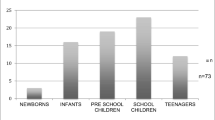
Clear trends were identified when tabulating the number of I and Rs within age groups. These findings are presented in Fig. 3.

Inspection and reports by age
Breakdown of cases: natural versus non-natural
Of the 318 cases examined 124 cases related to accidents, suicides, homicides, and cases with no ascertained cause of death. The remaining 194 cases were therefore deemed to be natural causes, predominantly cardiac related and other general medical diseases, but also including 15 deaths due to complications following a fractured neck of femur.
Figure 4 displays the number of cases in each group and how they were followed up.

All cases examined (318) with the breakdown of natural (194) versus non-natural (124) deaths, also displaying the numbers of post-mortems and inspection and reports performed in these two groups
Non-natural deaths
Within this group of 124 deaths there were 33 suicides, 76 accidents, 9 unascertained, and 6 homicide investigations.
Methods of suicide were hanging (18), carbon monoxide poisoning (4), drugs (3), plastic bag asphyxia (3), trauma, e.g., train (3) and gunshot (2).
Suicide related deaths having I and R included 23 cases (23/33 = 69 %). Figure 5 details the breakdown of follow up for these cases.

Representation of the number of I and Rs and PMs performed in the accident group. MV motor vehicle incidents, Fall (predominantly from a height), water-relating to drowning deaths, AutoE autoerotic
Accident related deaths were further subcategorized with 26 drug related deaths (not clearly related to suicide), 18 deaths due to falls, 24 motor vehicle incidents, 1 autoerotic death, 4 water related deaths, and 3 traumatic deaths occurring in workplaces.
Accidental deaths where I and R was performed numbered 44 cases (44/76) = 59 %. This is displayed in Fig. 6.

Representation of the number of I and Rs and PMs performed in the suicide group. CO carbon monoxide poisoning, Pl Bag plastic bag asphyxia, Trauma includes being struck by a train, GSW gun shot wound
Natural deaths
As noted in an earlier graph this included 194 cases with 114 post-mortems and 80 I and Rs. Further dissection of the data from this group highlights the decision making process in the group of cases with age 50 years or less.
In the age group 50 years or less there were 35 cases of which 3 had I and Rs. This latter group included a cardiomyopathy, a cerebral palsy sufferer with breast cancer, and a placental hemorrhage. Therefore 32 cases (91.4 %) underwent post-mortem examination.
CT findings
A definite cause of death was identified in 8/138 cases (6 %). These included two cases of intracerebral hemorrhage, one acute subdural hemorrhage, two brain stem hemorrhages, two hemopericardiums where there had not been resuscitation and two ruptured abdominal aortic aneurysms. All of these cases were processed as I and Rs.
Radiologist review
As noted previously the forensic pathologist is primarily interpreting the admission CT. The pathologists have undergone in house training from a forensic radiologist and have access to this sessional radiologist in problematic cases. At the time of the preliminary examination further consultation was undertaken in 7 of 318 cases (7/318 = 2.3 %). Cases may be reviewed after this preliminary examination, however an evaluation of this was not part of this project.
Discussion
This project has reviewed 318 sequential cases from July 2010 at VIFM where there were preliminary examinations which included routine CT scanning. The process highlights a new era where imaging analysis in association with medical histories and the wishes of family members can be combined and assessed. Guided by this information and determination from a forensic pathologist the coroner is then able to provide a direction as to whether or not a post-mortem examination is required.
The use of CT scanning clearly has advantages in cases where there is accidental or suicidal death. In approximately half of accidental deaths a complete autopsy was not deemed necessary. Similarly in suicide related deaths only 31 % went on to autopsy. It is noted that VIFM also has a facility where extensive overnight toxicology can be performed. A significant number of overdose cases can be substantiated with this testing and carbon monoxide levels are invaluable in motor vehicle exhaust gas associated suicides.
In what are generally described as “natural deaths” CT scanning has a role, however there were only 8 cases out of 138 in that grouping where a definitive diagnosis could be made. This then resulted in a determination for inspection and reports (I and Rs) and no post-mortem examination. This relatively low number reflects the fact that cases of, for example, marked coronary artery calcification, were not included as a definitive diagnosis until a post-mortem examination had been performed.
It is noted that there is some variation between pathologists providing a reasonable cause of death and that the age of the deceased may be a factor in this decision making process. In those 90 years or older post-mortem examinations were infrequent, while those younger than 50 years without a history of trauma or suicide were almost invariably fully examined with autopsy. In total there was a variation among the six pathologists in determining requirement for autopsy with a range of 35–70 %, the average for the month being 54 %.
Suicides in this series numbered 33 with by far the largest number of cases being associated with hanging. Interestingly only 27 % of these proceeded to autopsy. No cases of carbon monoxide poisoning proceeded.
In the accidental death category consisting of 76 cases the biggest groups were motor vehicle related and drug related deaths. Only 21 % of motor vehicle associated deaths had autopsies, these usually relating to issues as to pre-existing medical illness being a causative factor in the incident. Less confidence was generated with overnight drug testing as drug related deaths had a much higher autopsy rate at 73 %. This appears to relate to uncertainty as to the effect of natural disease in those regularly taking illicit drugs.
CT scans are primarily read by forensic pathologists who have undergone training with our forensic radiologist. Our group of pathologists has now had extensive experience in the narrowly focused field of reporting in the post-mortem setting. The confidence levels of those involved are reflected in the low initial consultation review rate of less than 3 %.
The CT scan is a very useful tool for excluding some injuries and pathologies, such as the ubiquitous collapse with possible head strike, where the CT scan can clearly document a lack of intracerebral hemorrhage and associated skull fractures.
Overall the process is effective in developing interaction between the medical and legal elements at the VIFM in efforts to process admissions in the most suitable manner.
Key points
-
1.
A new system of preliminary examination utilizing routine CT scanning of admissions allows discussion between medical and legal practitioners in determining the requirement for post-mortem examination.
-
2.
The use of CT scanning is very effective in documenting injuries in cases of accidental death.
-
3.
In a small number of cases of natural death a clear cause of death can be determined from the CT scan.
Reference
Coroners Act Vic. www.legislation.vic.gov.au (2008).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bedford, P.J. Routine CT scan combined with preliminary examination as a new method in determining the need for autopsy. Forensic Sci Med Pathol 8, 390–394 (2012). https://doi.org/10.1007/s12024-012-9349-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12024-012-9349-7