
Abstract
Neuropathy and peripheral artery disease represent the main pathophysiological conditions underlying diabetic foot. Several studies showed that Lipoprotein(a)—Lp(a)—and homocysteine (Hcy) can be associated with diabetic complications, but their relationship with diabetic foot is unclear. Aim of this study was to investigate whether Lp(a) and Hcy were associated with diabetic foot ulcerations, classified according to the presence of peripheral artery disease (PAD) or neuropathy. From among consecutive type 2 diabetic attending at the Diabetic Foot Clinic 27 subjects with vascular diabetic foot (VDF), 43 with neuropathic diabetic foot (NDF) and 52 controls without foot ulceration, neuropathy, and PAD were enrolled. Both Lp(a) (26.1 ± 22.7 vs. 14.9 ± 19.5 mg/dl; P = 0.003) and Hcy levels (15.4 ± 5.7 vs. 12.2 ± 5.1 μmol/l; P = 0.022) were significantly greater in the VDF group than in controls. Lp(a) levels were significantly lower in the NDF group than in controls (6.9 ± 8.1 versus 14.9 ± 19.5 mg/dl; P = 0.009), while no difference in Hcy levels was found. Multiple logistic regression analysis showed that Hcy was associated with VDF (OR: 1.11; 95% CI: 1.07–14.1; P = 0.048). Lp(a) did not enter the model, but its P-value was very near to the significant level (OR: 1.09; 95% CI: 0.99–12.05; P = 0.059). Moreover, low Lp(a) levels were associated with NDF (OR: 0.84; 95% CI: 0.21–0.96; P = 0.039). Our study has shown for the first time that high Lp(a) and Hcy levels are associated with the development of VDF, while low Lp(a) levels appear to be associated with delayed wound healing in patients with neuropathic foot ulcerations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lipoprotein(a)—Lp(a)—is a LDL-like particle that contains a specific apolipoprotein, named apolipoprotein(a) [1]. Lp(a) is a recognized cardiovascular risk factor [1, 2], since several studies have shown an association between high Lp(a) levels and cardiovascular disease (CVD) [1–6]. Lp(a) concentrations are mostly genetically committed [1]. Some studies have shown that Lp(a) may play a role in the development of some diabetic complications, such as coronary artery disease (CAD), stroke, and peripheral artery disease (PAD) [7–12]
Homocysteine (Hcy), a sulphydryl aminoacid derived from the metabolism of methionine, is a genetically determined risk factor for the development of CVD [13, 14]. Experimental studies have demonstrated that the reactivity of the sulphydrilic group of Hcy is involved in the mechanisms underlying changes of vascular endothelial cells that contribute to atherosclerosis and thrombosis [13, 14]. Some studies have also shown that high Hcy levels can be associated with diabetic complications, not only with macrovascular disease but also with neuropathy [11, 15].
The lifetime risk of a patient with diabetes mellitus to develop foot ulceration is about 25% [16]. Foot ulceration is a common complication of diabetes and increases greatly the risk of limb amputation [17]. About 80% of non-traumatic amputations are caused by the presence of diabetes and 85% of these amputations are preceded by a foot ulceration [17]. This implies that the presence of foot ulceration is considered an important risk for morbidity, mortality, and disability. Foot ulceration is due to an interplay of several risk factors [17]. Among them, neuropathy and PAD should be considered the most important pathophysiological conditions. In particular, neuropathy seems to increase the risk of foot ulceration by 7-fold [18], while PAD can cause a poor wound healing [17]. The early identification of diabetic patients at high risk for foot ulceration can be useful to prevent future limb amputations. Clearly to obtain this result, it may be important the identification of subjects at risk before the occurrence of neuropathy and PAD.
Some studies showed an association of both Lp(a) and Hcy levels with PAD [12, 19], but others did not [20]. A relationship between Lp(a) and diabetic neuropathy was not observed by specific studies [9, 21], while conflicting results are available in the literature on the association between Hcy and neuropathy [15, 19, 22].
Some studies observed an association of both Lp(a) and Hcy with the presence of lower extremity wound, but these studied did not evaluated the presence of neuropathy and/or PAD [23, 24]. An interesting recent study has evaluated the possible relationship of Lp(a) and Hcy with the prevalence of diabetic foot ulcerations in type 2 diabetic patients [25]. Even if in that study the presence of neuropathy and/or PAD was evaluated, information on the role of Lp(a) and Hcy in the pathophysiology of diabetic foot was not given.
Aim of this study was to investigate in a group of type 2 diabetic patients whether Lp(a) and Hcy levels were associated with diabetic foot ulcerations, classified according to the presence of PAD or neuropathy.
Materials and methods
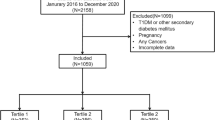
For this study, 195 consecutive patients with type 2 diabetes mellitus were recruited at the Diabetic Foot Clinic of the Clinical Institute “Beato Matteo” Vigevano, Italy. We enrolled both patients without foot ulcers who were attending at the Clinic for periodic feet examination and subjects with foot ulcerations. Exclusion criteria were: age <45 and >70 years, type 1 diabetes, any disease other than diabetes associated with edema, foot ulcer and/or polyneuropathy (such as cirrhosis, kidney disease, heart failure, vasculitis, alcohol abuse), previous foot ulcers, any condition modifying Lp(a) and/or Hcy levels (such as liver or renal disease, vitamin supplementation) amputation of any cause, neoplasia, limited life-expectancy.
Diabetes was diagnosed according to the American Diabetes Association criteria [26]. Hypertension was diagnosed according to the European Society of Hypertension/European Society of Cardiology criteria [27] or in the presence of a specific treatment. Patients with AER < 30 mg/day were considered normoalbuminuric; patients with AER between 30 and 299 mg/day were considered microalbuminuric [28]. Patients were considered smokers if current smokers or ex-smokers. Family history of CAD was considered positive in the presence of a documented myocardial ischemia or infarction in a first-degree relative. Prior CVD was defined as a documented personal history of CAD and/or stroke. Body mass index (BMI) was calculated by the following formula: kg/m2.
In all the patients, the presence of PAD was evaluated both by the ABI (ankle brachial index), which represents the ratio of systolic blood pressure in the ankle to that measured at the level of the brachial artery, and the transcutaneous oxygen tension or transcutaneous oximetry (TcPO2), as assessed by TCM4 Radiometer (Medical Aps, Bronshoj, Denmark).
To assess the presence of distal polyneuropathy nerve conduction testing [29] were performed at a stable skin temperature of 31°C and a room temperature of 24°C using a Medelec electrophysiological system (Synergy Oxford Instruments Oxford, UK) [30].
Venous blood samples were taken from subjects after fasting for 12 h. Cholesterol, HDL, and triglycerides were measured by an automatic analyzer HITACHI 737 (Tokio-Japan). LDL was calculated by the Friedewald’s formula [31]. Glycated hemoglobin (HbA1c) was measured by high-performance liquid chromatography (Biorad, Richmond, CA). AER was measured by nephelometry (Beckmann, Milan, Italy). Lp(a) plasma concentrations were determined by a sandwich-ELISA method (Macra-Lp(a) SDI, Newark, Delaware). Plasma Hcy level was measured by high-performance liquid chromatography.
The study population was subdivided into three groups: 1. Patients with vascular diabetic foot (VDF—n = 27): the group included subjects with a foot ulceration, ABI ≤ 0.9, TcPO2 < 40 mmHg [32] and absence of polyneuropathy according to nerve conduction studies. 2. Patients with neuropathic diabetic foot (NDF—n = 43): the group included subjects with foot ulceration, documented polyneuropathy according to nerve conduction studies, ABI > 0.9 and TcPO2 > 40 mmHg [32]. 3. Controls (n = 52): the group included subjects without foot ulceration, absence of polyneuropathy according to nerve conduction studies, ABI > 0.9, TcPO2 > 40 mmHg [30]. Seventy-three patients with neuro-vascular ulcerations, without foot ulceration but with polyneuropathy and/or PAD, were excluded from the study.
Statistical analysis
Both NDF and VDF group was separately compared with controls in every analysis. To assess differences in variables normally distributed, such as cholesterol, LDL, HDL, BMI, the Student t test was utilized. Because of the highly “skewed” distribution of some variables, such as Lp(a) and triglycerides levels, to compare their values the Mann–Whitney U-test was used. The Pearson Chi-squared test was exploited for frequency comparison. A multiple logistic regression analysis with the presence of foot ulceration as the dependent variable was performed. Variables were categorized as previously shown [11, 33–36]. We used the recognized cut-off of 30 mg/dl for Lp(a) [1]. Nevertheless, since Lp(a) levels were significantly lower in NDF patients compared with controls, we tested both a cut-off of 20 mg/dl and a cut-off of 10 mg/dl. Odds ratios (ORs) were estimated and the results were given as ORs and 95% CI. Data were presented as means ± SD, unless otherwise stated. P < 0.05 was considered significant.
Results
Table 1 reports biological and clinical characteristics of the diabetic patients without foot ulcerations, polyneuropathy, and PAD (controls), those with NDF and those with VDF. As shown, no significant differences in age, BMI, and glycemic control were observed between controls and each group with diabetic foot.
Patients with NDF show diabetes duration longer than that of controls. Smokers and the percentages of subjects with prior CVD, family history of CAD, micro or macroalbuminuria were significantly higher in the VDF group than in controls. No significant differences in diabetes duration, lipid parameters, and treatment with statins were observed between subjects with VDF and controls.
Lp(a) levels were significantly lower in patients with NDF than in controls (6.9 ± 8.1 vs. 14.9 ± 19.5 mg/dl; P = 0.009), while no difference in Hcy levels (12.4 ± 5.6 vs. 12.2 ± 5.1 μmol/l; P = 0.549) was found between NDF group and controls. Both Lp(a) (26.1 ± 22.7 vs. 14.9 ± 19.5 mg/dl; P = 0.003) and Hcy (15.4 ± 5.7 vs. 12.2 ± 5.1 μmol/l; P = 0.022) levels were significantly greater in subjects with VDF than in controls.
A multiple logistic regression analysis was performed with the presence of NDF as the dependent variable and the following as predictive variables: age, gender, BMI, diabetes duration, HbA1c, hypertension, known CVD, family history of CAD, cholesterol, triglycerides, LDL, HDL, microalbuminuria, smoking, Lp(a), and Hcy. All potential predictive variables were tested. VDF patients were not included in this analysis. Table 2 reports the results of the analysis. Diabetes duration was the only predictor of NDF Lp(a), and Hcy did not enter the model. When a cut-off of 10 mg/dl for Lp(a) was used, low Lp(a) levels were significantly associated with the presence of NDF in our diabetic subjects, as reported in Table 2.
Also a multiple logistic regression analysis with the same predictive variables, but with the presence of VDF as the dependent variable was performed. NDF patients were not included in this analysis. Table 3 shows that prior CVD, smoking habits and high Hcy levels were independently associated with the presence of vascular foot ulcerations in diabetes. Lp(a) did not enter the model, but its P-value was very close to the significant level (OR: 1.09; 95% CI: 0.99–12.05; P = 0.059).
Discussion
Diabetic foot represents a common and severe complication of diabetes [17]. Indeed, about 85% of limb amputations are preceded by a foot ulceration [17]. Moreover, diabetic foot is often characterized by severe infections and represents a major risk for mortality in diabetes [17, 37]. This implies that the early identification of diabetic subjects at high risk for foot ulcerations could permit the prevention of their severe complications. To implement effective strategies of prevention of diabetic foot, it may be very useful to identify specific and early predictors. Certainly, a systematic and frequent examination of the feet should be done in all diabetic patients with the aim to identify those at high risk of diabetic foot [38]. It is necessary to detect foot deformities, but also the presence of diabetic neuropathy and PAD, since these two conditions represent the main pathophysiological conditions underlying foot ulcerations. Nevertheless, preventive measures of diabetic foot could be more effective, if patients at high risk of NDF and VDF can be identified before the occurrence of neuropathy and PAD.
Our study first shows that high Hcy levels and to a lesser extent high Lp(a) levels could be predictive of the development of VDF ulcerations. Really, this finding is quite expected, since both Hcy and Lp(a) are recognized risk factors for PAD [12, 19]. If a foot ulceration occurs, PAD may cause poor wound healing. This outlines the importance to prevent PAD. Subjects with high Lp(a) and Hcy levels could be more prone to develop PAD: this may imply that in these subjects a more aggressive control of traditional cardiovascular risk factors should be adopted. In addition, it may be of interest to understand whether a reduction in Hcy and Lp(a) levels could reduce the risk of PAD and VDF. Some large studies showed that the reduction in Hcy levels by vitamin supplementation may not reduce significantly cardiovascular events [39]. This should be also verified for the development of VDF. Lp(a) levels can be reduced by the use of niacin and recently it has been suggested to treat high Lp(a) levels to reduce the cardiovascular risk [40]. Specific studies should verify whether the reduction in Lp(a) levels can modify the risk of VDF.
The novel intriguing finding of this study regards the fact that low Lp(a) levels can be associated with NDF. The pathophysiological explanation of this finding is not easy, since no study has ever found an association between low Lp(a) levels and diabetic neuropathy. This suggests that low Lp(a) levels do not seem to be a risk factor for NDF via diabetic neuropathy. On the contrary, low Lp(a) levels could be responsible for the impaired wound healing of foot ulcerations due to neuropathy. In other words, one can speculate that among patients who develop neuropathic foot ulcerations, those with lower Lp(a) levels could have some problem to obtain an adequate and rapid wound healing. The mechanism by which this could happen is unclear. Nevertheless, it is important to remember that, although the physiologic role of Lp(a) remains elusive, some authors have suggested a role of Lp(a) in tissue reparation and wound healing [1, 41].
In our study, we did not find any association between Hcy and NDF. This result is in contrast with the finding of the recent paper of Gonzales et al. [25]. Hcy levels can be affected by several clinical or pharmacological conditions, such as renal disease, vitamin deficiency or supplementation [39], treatment with metformin [42]. In our study, we excluded patients with any condition modifying Hcy levels and there was no difference in the percentage of patients treated with metformin between NDF group and control. In addition, we did not group together patients with NDF and VDF. However, we cannot exclude a role of Hcy in NDF, since an association between neuropathy and Hcy has been observed [15] and hyperhomocysteinemia was seen to be directly associated with the presence of lower limb wounds [24, 25].
Therefore, our data suggest that Lp(a) may have a role both in VDF and NDF. High Lp(a) levels could favor PAD, which is the main responsible for VDF. On the contrary, low Lp(a) may delay wound healing among subjects with neuropathy. If these findings will be confirmed by larger studies, there may be important clinical implications: indeed, it may be useful to reduce Lp(a) levels to prevent PAD and other vascular pathologies. Nevertheless, caution should be paid to excessively decrease Lp(a) levels, particularly, if neuropathy is present. However, specific intervention studies are needed.
The first study limitation is that our investigation is not longitudinal, but case-controlled. Prospective data are needed to confirm our findings. Second, our population is relatively small. Nevertheless, the identification of neuropathy and PAD was rigorous, since very effective instrumental diagnostic methods were used in all the patients. In addition, to better evaluate the relationship between the risk factor and each main pathophysiological mechanism of diabetic foot, we excluded patients with neuro-ischemic foot ulcerations. Third, we hypothesized that the relationship between Lp(a) and NDF is linked to an impaired wound healing due to low Lp(a) levels and not to a possible association between Lp(a) and neuropathy. We are aware that this is a speculative interpretation because of the lack of a specific group of patients with neuropathy without foot ulcerations. Finally, it is important to remember that Lp(a) is considered a reactant of acute-phase, since its levels increase when inflammation is present [1]. So we cannot exclude that the presence of inflammation due to foot ulcerations could modify Lp(a) levels in NDF and VDF groups. In addition, Lp(a) levels could be affected by microalbuminuria [1]. So in patients with VDF Lp(a) may be increased, since the percentage of subjects with microalbuminuria is higher in the VDF group than in controls. This implies that the real impact of Lp(a) on diabetic foot ulcerations has to be further investigated by prospective studies and/or by the assessment of apo(a) polymorphism that can be modified by environmental conditions [1]. However, many nontraditional risk factors other than Lp(a) and Hcy can have a role in the development of diabetic foot ulcerations [20, 43]. So it may be of clinical interest the identification of a panel of risk factors to stratify the individual risk of each diabetic patient of developing foot ulcerations. This may permit personal programs of prevention of diabetic foot together with an early treatment of foot ulceration by specific multidisciplinary approach [17, 37, 38, 44].
In conclusion, our study first shows that high Lp(a) and Hcy levels are associated with the development of VDF, while low Lp(a) levels may be hypothesized to contribute to delayed wound healing in patients with neuropathic foot ulcerations.
References
C. Gazzaruso, A. Garzaniti, D. Geroldi, Genetics and cardiovascular risk: a role for apolipoprotein (a) polymorphism. Cardiologia 44, 347–354 (1999)
I. Gouni-Berthold, H.K. Berthold, Lipoprotein(a): current perspective. Curr. Vasc. Pharmacol. 2011. [Epub ahead of print]
C. Gazzaruso, A. Garzaniti, P. Buscaglia, G. Bonetti, C. Falcone, P. Fratino, G. Finardi, D. Geroldi, Association between apolipoprotein(a) phenotypes and coronary heart disease at a young age. J. Am. Coll. Cardiol. 33, 157–163 (1999)
J. Danesh, R. Collins, R. Peto, Lipoprotein(a) and coronary heart disease: a meta-analysis of prospective studies. Circulation 102, 1082–1085 (2000)
A. Bennet, E. Di Angelantonio, S. Erqou, G. Eiriksdottir, G. Sigurdsson, M. Woodward, A. Rumley, G.D. Lowe, J. Danesh, D. Gudnason, Lipoprotein(a) levels and risk of future coronary heart disease: large-scale prospective data. Arch. Intern. Med. 168, 598–608 (2008)
The Emerging Risk Factors Collaboration, Lipoprotein(a) concentration and the risk of coronary heart disease, stroke and nonvascular mortality. JAMA 302, 412–423 (2009)
P. Buscaglia, C. Gazzaruso, Garzaniti, G. Bonetti, A. Porta, A. Negri, G. Vandelli, G. Finardi, P. Fratino, D. Geroldi, Lipoprotein(a) and proliferative diabetic retinopathy in tipe II diabetes mellitus: a role for isoforms with low molecular weight. Diabetes Nutr. Metab. 9, 129–137 (1996)
C. Gazzaruso, A. Garzaniti, S. Giordanetti, C. Falcone, E. De Amici, D. Geroldi, P. Fratino, Assessment of asymptomatic coronary artery disease in apparently uncomplicated type 2 diabetic patients. Diabetes Care 25, 1418–1424 (2002)
C. Gazzaruso, A. Garzaniti, P. Buscaglia, G. D’Annunzio, A. Porta, G. Vandelli, R. Lorini, G. Finardi, P. Fratino, D. Geroldi, Lipoprotein(a) levels and apolipoprotein(a) polymorphism in type 1 diabetes mellitus: relationships to microvascular and neurological complications. Acta Diabetol. 35, 13–18 (1998)
C. Gazzaruso, A. Garzaniti, C. Falcone, D. Geroldi, G. Finardi, P. Fratino, Association of lipoprotein(a) levels and apolipoprotein(a) phenotypes with coronary artery disease in type 2 diabetic patients and in non diabetic subjects. Diabet. Med. 18, 589–594 (2001)
C. Gazzaruso, A. Garzaniti, S. Giordanetti, C. Falcone, P. Fratino, Silent coronary artery disease in type 2 diabetes mellitus: the role of Lipoprotein(a), homocysteine and apo(a) polymorphism. Cardiovasc. Diabetol. 1, 5 (2002)
H. Osakawa, K. Tokunaga, F. Kawakami, Comparison of risk factors of macrovascular complications. Peripheral vascular disease, cerebral vascular disease, and coronary heart disease in Japanese type 2 diabetes mellitus. J. Diabetes Complicat. 14, 307–313 (2000)
L.L. Humprey, R. Fu, K. Rogers, M. Freeman, M. Helfand, Homocysteine level and coronary artery disease incidence: a systematic review and meta-analysis. Mayo Clin. Proc. 83, 1203–1212 (2008)
N. Khandanpour, Y.K. Loke, F.J. Meyer, B. Jennings, M.P. Armon, Homocystein and peripheral arterial disease: systematic review and meta-analysis. Eur. J. Vasc. Endovasc. Surg. 38, 316–322 (2009)
S.G. Bruce, T.K. Young, Prevalence and risk factors for neuropathy in a Canadian First Nation community. Diabetes Care 31, 1837–1841 (2008)
N. Singh, D.G. Armstrong, B.A. Lipsky, Preventing foot ulcers in patients with diabetes. JAMA 293, 217–228 (2005)
M.P. Khanolkar, S.C. Bain, J.W. Stephens, The diabetic foot. Q. J. Med. 101, 685–695 (2008)
G.E. Reiber, L. Vilekyte, E.J. Boyko, M. Del Aguila, D.G. Smith, L.A. Lavery, A.J. Boulton, Causal pathways for incident lower extremity ulcers in patients with diabetes from two settings. Diabetes Care 22, 157–162 (1999)
D.A. De Luis, N. Fernandez, M.L. Arranz, R. Aller, O. Izaola, E. Romero, Total homocysteine levels relation with chronic complications of diabetes, body composition, and other cardiovascular risk factors in a population of patients with diabetes type 2. J. Diabetes Complicat. 19, 42–46 (2005)
M.T. Garcia-Unzueta, C. Pesquera, E. Calzada et al., Blood-soluble Fas levels are increate in type 2 diabetica patients with peripheral vascular disease. Horm. Metab. Res. 38, 673–677 (2006)
R.E. Maser, D.C. Usher, G.S. DeCherney, Little association of lipid parameters and large sensory nerve fiber function in diabetes mellitus. J. Diabetes Complicat. 10, 54–59 (1996)
E.K. Hoogeven, P.J. Kostense, G.D. Valk et al., Hyperhomocysteinemia is not related to risk of distal somatic polyneuropathy: the Hoorn study. J. Intern. Med. 246, 561–566 (1999)
K. Unluhizarci, S. Muhtaroglu, S. Kabak, F. Bayram, F. Kelestimur, Serum lipoprotein(a) levels in patients with diabetic foot lesions. Diabetes Res. Clin. Pract. 71, 119–123 (2006)
E.M. Schwartzfarb, P. Romanelli, Hyperhomocysteinemia and lower extremity wounds. Int. J. Low. Extrem. Wounds 7, 126–136 (2008)
R. Gonzalez, T. Pedro, J.T. Real, S. Martinez-Hervas, M.R. Abellan, R. Lorente, A. Priego, M. Catala, F.J. Chaves, J.F. Ascaso, R. Carmena, Plasma homocysteine levels are associated with ulceration of the foot in patients with type 2 diabetes mellitus. Diabetes Metab. Res. Rev. 26, 115–120 (2010)
The Expert Committee on the diagnosis and classification of diabetes mellitus, Report of the Expert Committee on the Diagnosis and classification of diabetes mellitus. Diabetes Care 20, 1183–1197 (1997)
G. Mancia, G. De Backer, A. Dominiczak et al., ESH-ESC task force on the management of arterial hypertension. 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension. J. Hypertens. 25, 1751–1762 (2007)
A. Giustina, P. Perini, P. Desenzani, S. Bossoni, P. Ianniello, M. Milani, G. Davì, G. Romanelli, Long-term treatment with the dual antithrombotic agent picotamide decreases microalbuminuria in normotensive type 2 diabetic patients. Diabetes 47, 423–430 (1998)
S. Tesfaye, A.J. Boulton, P.J. Dyck et al., Toronto diabetic neuropathy expert group. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity and treatments. Diabetes Care 33, 2285–2293 (2010)
C.H. Gibbons, R. Freeman, A. Veves et al., Diabetic neuropathy: a cross-sectional study of the relationships among test of neurophysiology. Diabetes Care 33, 2629–2634 (2010)
W.T. Friedewald, R.I. Levy, D.S. Fredrickson, Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 18, 499–502 (1972)
C.E. Fife, D.R. Smart, P.J. Sheffield, H.W. Hopf, G. Hawkins, D. Clarke, Transcutaneous oximetry in clinical practice: consensus statements from an expert panel based on evidence. Undersea Hyperb. Med. 36, 43–53 (2009)
C. Gazzaruso, S. Giordanetti, E. De Amici, G. Bertone, C. Falcone, D. Geroldi, P. Fratino, S.B. Solerte, A. Garzaniti, Relationship between erectile dysfunction and silent myocardial ischemia in apparently uncomplicated type 2 diabetic patients. Circulation 110, 22–26 (2004)
C. Gazzaruso, S.B. Solerte, A. Pujia, A. Coppola et al., Erectile dysfunction as a predictor of cardiovascular events and death in diabetic patients with asymptomatic coronary artery disease angiographically proven. A potential protective role for statins and 5-phosphodiesterase inhibitors. J. Am. Coll. Cardiol. 51, 2040–2044 (2008)
C. Gazzaruso, A. Coppola, T. Montalcini, et al., Screening for asymptomatic coronary artery disease can reduce mortality and morbidity in type 2 diabetic patients. Intern. Emerg. Med. (2011). doi: 10.1007/s11739-011-0527-5
C. Gazzaruso, A. Coppola, T. Montalcini, et al., Erectile dysfunction can improve the effectiveness of the current guidelines for the screening for asymptomatic coronary artery disease in diabetes. Endocrine. 2011. doi: 10.1007/s12020-011-9523-9
J. Apelqvist, The foot in perspective. Diabetes Metab. Res. Rev. 24, S110–S115 (2008)
J. Apelqvist, K. Bakker, W.H. van Houtum, N.C. Schaper, on behalf of the International Working Group on the Diabetic Foot (IWGDF) Editorial Board. Practical guidelines on the management and prevention of the diabetic foot. Diabetes Metab. Res. Rev. 24, S181–S187 (2008)
J.M. Abraham, L. Cho, The homocysteine hypothesis: still relevant to the prevention and treatment of cardiovascular disease? Clevel. Clin. J. Med. 77, 911–918 (2010)
B.G. Nordestgaard, M.J. Chapman, K. Ray et al., European Atherosclerosis Society Consensus Panel Lipoprotein(a) as a cardiovascular risk factor: current status. Eur. Heart J. 31, 2844–2853 (2010)
M.L. Koschinsky, Novel insights into Lp(a) physiology and pathogenicity: more question than answers? Cardiovasc. Hematol. Disord. Drug Targets 6, 267–278 (2006)
G. Ntaios, C. Savopoulos, S. Chatzopoulos, D. Mikhailidis, A. Hatzitolios, Iatrogenic hyperhomocysteinemia in patients with metabolic syndrome: a systematic review and metaanalysis. Atherosclerosis 214, 11–19 (2011)
M. Erdogan, S. Solmaz, M. Canataroglu et al., Plasma thrombin-activable fibrinolysis inhibitor (TAFI) antigen levels in diabetic foot ulcers. Endocrine 37, 449–454 (2010)
K. Aydin, M. Isildak, J. Karakaya, A. Gurlek, Change in amputation predictors in diabetic foot disease: effect of multidisciplinary approach. Endocrine 38, 87–92 (2010)
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gazzaruso, C., Coppola, A., Montalcini, T. et al. Lipoprotein(a) and homocysteine as genetic risk factors for vascular and neuropathic diabetic foot in type 2 diabetes mellitus. Endocrine 41, 89–95 (2012). https://doi.org/10.1007/s12020-011-9544-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-011-9544-4