
Abstract
Hyperhomocysteinemia in patients with diabetes mellitus (DM) has been proposed as a new risk factor for coronary artery disease (CAD). Due to the prevalence of DM and CAD in the Iranian population and the relatively high economic burden, research on these new risk factors sounds necessary. This study investigated the relationship between hyperhomocysteinemia and coronary heart disease in patients with type 2 diabetes. This study was a hospital-based cross-sectional study performed on 100 diabetic patients with indications of coronary artery angiography. After the measurement of serum HbA1c and homocysteine, the patients went through coronary angiography and, based on the results, were divided into two groups of normal and obstructed coronary arteries. Serum homocysteine and other related risk factors were further compared between the two groups. The mean serum homocysteine of patients was 13.18 ± 3.64 μmol/L in general and 15.02 ± 3.7 μmol/L in those with coronary artery obstruction. With hyperhomocysteinemia defined as serum homocysteine of ≥ 14 μmol/L, 48% of diabetic patients had hyperhomocysteinemia, of which 83% had coronary artery obstruction. The relationship between serum homocysteine and coronary artery obstruction was significant (P < 0.001). The serum homocysteine was the highest in patients with three-vessel involvement (15.39 ± 3.5 μmol/L), which was significantly higher than those with normal coronary arteries (P < 0.001). The mean serum homocysteine of diabetic patients (type II) with coronary artery disease was significantly higher than those with normal coronary arteries. It was also significantly higher in patients with three-vessel involvement than those with no vessel involvement.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
According to the last WHO fact sheet on cardiovascular disease (updated January 2015), cardiovascular diseases are responsible for 17.5 million deaths annually. In both the developed and most of the developing countries, it is the reason for nearly one-third of adult deaths. Of these deaths, 7.4 million are due to coronary heart disease and 6.7 million are caused by stroke. Current studies indicate that it is a major health problem in the eastern Mediterranean region and Middle Eastern countries including Iran (Mendis et al. 2015).
The atherosclerosis of coronary arteries is one of the most prevalent diseases of the last century, which is associated with high annual morbidity and mortality. In diabetic patients, the prevalence and mortality rate of coronary artery diseases are almost two to three times higher than the general population (Kannel and McGee 1979). In Iran, diabetes is a major public health problem and most of the patients are not even aware of their disease (Hadaegh et al. 2008). The reported prevalence of diabetes in Iran based on a national study of risk factors for non-communicable diseases was 7.7%, equivalent to 2 million patients in the Iranian population aged between 25 and 64 years in 2008 (Esteghamati et al. 2008). The International Diabetes Federation has also reported the estimated prevalence of diabetes in Iran in 2013 to be 8.43% in the Iranian population aged 20 to 79 years (Unwin et al. 2013). Diabetes mellitus imposes both direct and indirect costs on the patients, which is much higher in comparison to many other diseases. There are a few documented studies on the assessment of costs associated with diabetes mellitus in Iran. The mean diabetes-related expenditure per Iranian with diabetes (USD) was reported to be 471 USD by the International Diabetes Federation (IFD Diabetes Atlas, 6th edition) (Unwin et al. 2013). Based on the last released research of the American Diabetes Association on March 6, 2013, on economic costs of diabetes in the US, the estimated total economic cost of diagnosed diabetes has risen from $174 billion (in 2007, dollars) to $245 billion in 2012, which shows a 41% increase. This emphasizes the fact that diabetes imposes a major burden on the society (American Diabetes Association 2013).
Besides the common classic risk factors known for coronary artery diseases, newer risk factors, such as serum homocysteine level, lipoprotein (a), and C-reactive protein, have been proposed. The role of these novel cardiovascular risk factors is elucidated more and more every day (Antoniades et al. 2009; Humphrey et al. 2008). Moreover, it has been shown that lipoprotein (a), homocysteine, and apolipoprotein (a) polymorphism are each independently associated with silent coronary artery disease in patients with diabetes mellitus, type II (Gazzaruso et al. 2002).
In a study by Mohammadi et al. in 2005, the serum level of homocysteine was measured in patients with diabetes mellitus type II and glucose intolerance, and compared with that of the control group. However, there was found no significant difference between them (Mohammadi et al. 2005). In another cross-sectional study, Sharifkazemi et al. studied the serum level of homocysteine in 197 Iranian patients who had undergone coronary angiography. Hyperhomocysteinemia was found to be an independent risk factor of coronary artery disease. In patients without any risk factor, there was a linear relationship between the serum level of homocysteine and number of affected coronary arteries (Kazemi et al. 2006). Sadeghian et al. also studied the serum level of homocysteine in patients with early coronary artery disease in a cross-sectional study in 2006. The study was performed on 225 patients younger than 45 years who had undergone coronary angiography. Early coronary atherosclerosis was evident in 43% of the patients. The serum level of homocysteine was significantly higher in male patients than the control group (Sadeghian et al. 2006).
In a study by Gazzaruso et al. in Italy, the serum homocysteine level was measured in diabetic patients (type II) who had silent coronary artery disease. It was shown that the serum level of homocysteine and lipoprotein (a) is higher in diabetic patients with coronary artery disease than those without it (Gazzaruso et al. 2002). Audelin et al. in a review article on the effect of homocysteine on cardiovascular diseases in diabetic patients concluded that hyperhomocysteinemia is only associated with increased mortality (Audelin and Genest 2001). Hoogeveen et al. studied the relationship between hyperhomocysteinemia and cardiovascular diseases in diabetic patients compared with patients with glucose intolerance and non-diabetic patients. They measured the morning serum homocysteine level of 631 white patients aged 50–75 and the data were matched for sex, age, blood pressure, smoking, and hypercholesterolemia. However, homocysteine was found to be a strong risk factor for cardiovascular disease in patients with diabetes mellitus type II (Hoogeveen et al. 1998). In a large cohort of 830 patients aged between 45 and 64 years with diabetes mellitus II, serum homocysteine was found to be an independent predictor of coronary heart disease death and all events (Soinio et al. 2004). In another study, Mojiminiyi et al. studied the relationship of serum homocysteine, lipoprotein (a), and C-reactive protein (CRP) to coronary heart diseases in patients with type 2 diabetes mellitus. It was found that serum homocysteine and CRP are significantly higher in patients with cardiovascular disease than the control group (Mojiminiyi et al. 2002). A similar study by Akalin et al. in Turkey showed that the plasma level of homocysteine and inflammatory markers in diabetic patients with coronary atherosclerosis is significantly greater than those without it (Akalin et al. 2008). Okada et al. also studied the level of serum homocysteine in Japanese diabetic and non-diabetic patients, who had undergone coronary angiography. It was revealed that the degree of coronary stenosis in diabetic patients with hyperhomocysteinemia is greater than those with normal serum homocysteine level (Okada et al. 1999).
In this study, the level of serum homocysteine and its relationship to the atherosclerosis of coronary arteries were studied in diabetic patients who had undergone coronary angiography. Because of the relatively high prevalence of diabetes mellitus and coronary artery disease in the Iranian population, the identification and study of the etiologies of coronary atherosclerosis are considered one of the essential health priorities of the country.
Methods
Study participants
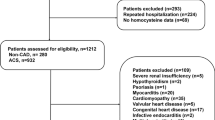
This study was a hospital-based cross-sectional study performed on patients with diabetes mellitus type II in order to study the relationship between hyperhomocysteinemia and coronary artery obstruction in Iranian diabetic patients. A total of 100 diabetic patients with indications of coronary artery angiography who came to the angiography department of Shahid Mostafa-Khomeini hospital, were included in the study. The patients were selected by simple non-random sampling method. All the patients who had renal failure, hypothyroidism, rheumatic diseases, drug history of vitamin B12 or folate combinations, and past history of infection in the last 2 months had been excluded from the study. Diabetes mellitus was defined as current treatment with insulin or oral hypoglycemic agents, or diabetic-range fasting blood sugar according to the American Diabetes Association criteria (Dormandy et al. 2005). The indications of coronary artery angiography were the definitive indications based on AHA/ACC guideline on coronary angiography (Mann et al. 2014).
The patients were first visited by a cardiologist and after a full history was elicited from them and the physical examination, they went through laboratory tests including the measurement of serum homocysteine and HbA1c. The questionnaire of demographic data was filled for all the patients. To measure the serum level of homocysteine and HbA1c, 5 mL of fasting blood (10–12 h) was drawn from each patient in EDTA test tubes. In less than an hour, the blood samples were centrifuged with a rotation speed of 1550 revolutions per 10 min to separate the sera. An amount of 1.5 mL of each patient’s serum was separated and used for the measurement of HbA1c by the kits (Pars-Azmoon, Tehran, Iran) using the turbidimetry technique. The rest of the serum was kept at − 20 °C. The homocysteine level of these sera was measured by ELISA kits and using the HPLC device equipped with fluorescence detector (RF-551).
At last the patients went through coronary angiography. All the angiography films of the patients were interpreted by an experienced cardiologist. The severity of coronary artery obstruction was reported based on the criteria of coronary artery diseases. Based on the results, the patients were further divided into two groups: (1) those with obstruction of more than 50% in the main arteries or their branches and (2) those who had normal coronary arteries as controls.
Statistical analysis and data analysis methods
The statistical analysis of the data was done using SPSS statistics software package 16 (Hosseini et al. 2016; Sharif et al. 2016; Kashani et al. 2012; Jalali et al. 2016). The tests used for the analysis of the data were t test, chi-square, and ANOVA (Lotfi et al. 2016; Nikzad et al. 2013; Kashani et al. 2013). The results of the study were reported as mean ± standard deviation. The significance level was defined as a P value of less than 0.05.
Ethical considerations
The goals and all the steps of the study were explained completely for all the patients. The patients participated in the study on their own will and they could anytime withdraw from the study. No charge was imposed on the patients. Written consent was obtained from all the patients before the study (Sharif et al. n.d.; Saba et al. 2017; Piroozmand et al. 2017). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments.
Results
A total of 100 patients with diabetes mellitus type II, 60% male and 40% female (Table 1), were studied. The patients were aged from 48 to 78 years old with an average age of 64.14 ± 7.18. It was found that 66% of patients have some degree of coronary artery obstruction, among which 19 patients (19%) had two and 47 patients (47%) had three-vessel involvement. It is to be noted that only three patients had one vessel involvement and because they had evidence of milder involvement of other vessels, they were considered among those patients with two-vessel involvement. The average age of patients with two- and three-vessel involvement was 63.89 ± 5.7 and 66.45 ± 7.9, respectively, and that of normal patients was 61.9 ± 5.6. The mean age of patients with coronary artery obstruction was significantly higher than that of patients without it (P < 0.01). However, no significant relationship was found between age and the number of involved vessels.
The past history of hypertension was present in 75% of patients, 24% were smokers, and 67% had a family history of cardiovascular diseases in their first-degree relatives. The complete set of patients’ demographic data is visible in Table 1. There was not found any significant relationship between coronary artery obstruction and hypertension, smoking, and family history of cardiovascular diseases in this study.
The mean serum homocysteine of patients was 13.18 ± 3.64 μmol/L in general (Table 2) and 15.02 ± 3.7 μmol/L in those with coronary artery obstruction. The relationship between hyperhomocysteinemia, assuming different definitions, and coronary artery obstruction is shown in Fig. 1. With hyperhomocysteinemia defined as serum homocysteine more than 14 μmol/L, 48% of diabetic patients (48 patients) had hyperhomocysteinemia, of which 40 patients (83%) had coronary artery obstruction and 8 (17%) had normal coronary arteries. With a definition of more than 15 μmol/L, the frequency of hyperhomocysteinemia in diabetic patients was 32%, of which only 3 patients (10%) were normal and the other 29 (90%) had coronary artery obstruction. There was a significant relationship between serum homocysteine and coronary artery obstruction (P < 0.001).

Hyperhomocysteinemia in diabetic patients with coronary artery obstruction. Hyperhomocysteinemia was defined assuming different cut-offs
As shown in Table 2, serum homocysteine was the highest in patients with three-vessel involvement (15.39 ± 3.5 μmol/L), which was significantly higher than those with normal coronary arteries (P < 0.001). However, no significant difference was found between the homocysteine level of patients with three- and two-vessel involvement, and also those with two and no vessel(s) involvement. The mean HbA1c, FBS, and BMI of the patients were 8 ± 1.38 mmol/L, 162 ± 40.2 mg/dL, and 23.26 ± 4.9 Kg/m2, respectively (Table 2). There was found no significant difference between HbA1c, FBS, and BMI of the patients with and without coronary artery obstruction.
In 72% of patients, the age of onset of diabetes was above 50 years, while only in 4% it was below 40 years. While 41% of patients had a duration of diabetes of more than 10 years, in 15% it was less than 5 years. Further data is shown in Table 3. The age of onset and duration of diabetes were compared between patients with and without coronary artery obstruction but the difference was not significant.
As shown in Fig. 2, the mean serum homocysteine was the lowest (10.98 ± 2.43 μmol/L) in patients with an age of onset of diabetes between 30 and 39 years, and highest (14.51 ± 3.69 μmol/L) in those with an age of onset above 50 years. However, the difference was not statistically significant. Nevertheless, it was found to be the highest (15.1 ± 3.9 μmol/L) in those patients with a duration of diabetes more than 10 years, and the lowest (12.88 ± 2.6 μmol/L) in those with a duration between 5 and 10 years, with their difference being significant (P < 0.05) (Fig. 2). There was found no significant relationship between HbA1c and BMI and the age of onset and duration.

The mean serum homocysteine in different groups of diabetic patients according to the duration and age of onset
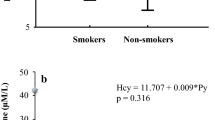
The mean serum homocysteine of smokers and non-smokers were 14.1 ± 3.06 and 13.65 ± 3.67 μmol/L, respectively, and the difference between them was not statistically significant. However, there was a significant relationship between the level of serum homocysteine and blood pressure (P < 0.05) and in hypertensive patients, it was higher (14.47 ± 3.7 μmol/L) than normotensive patients (12.5 ± 2.7 μmol/L).
Discussion
The atherosclerosis of coronary arteries is one of the most common diseases of the last century, which is associated with a high mortality rate. Hyperhomocysteinemia has been established as an independent risk factor of atherosclerosis (Perry et al. 1995; Atkinson et al. 2008; Shekelle 2006). It is also known that diabetes mellitus hastens the development of atherosclerosis itself (Kasper et al. 2015). To clarify the relationship between hyperhomocysteinemia and development of atherosclerosis and coronary artery disease in diabetic patients, this study compared the serum homocysteine of diabetic patients (type II) with and without coronary artery obstruction.
In our study, the mean serum homocysteine of diabetic patients was 13.18 ± 3.64 μmol/L, whereas it was 13.5 ± 3.6 μmol/L and 12.78 ± 2.5 μmol/L in Hoogeveen and Okada studies, respectively (Hoogeveen et al. 1998; Okada et al. 1999). The difference would be explained by the difference in races and diets of the studied populations. The mean HbA1c was 8 ± 1.38 mmol/L, while it was 8.43 ± 3.2 mmol/L and 8.09 ± 1.75 mmol/L in Okada and Akalin studies, respectively (Akalin et al. 2008; Okada et al. 1999). It is likely that serum HbA1c is determined the most by the degree to which blood sugar is controlled. The prevalence of coronary artery obstruction was 66% in our study, while it was 80% and 45% in Gazzaruso and Akalin studies, respectively (Gazzaruso et al. 2002; Akalin et al. 2008). The difference could be due to the difference in the studied population and also the different criteria used for coronary angiography. As in Gazzaruso study, the patients had been screened for silent coronary artery disease (Gazzaruso et al. 2002).
In our study, the mean serum homocysteine of patients with coronary artery obstruction was significantly more than that of patients with normal coronary arteries. It was also found to be significantly higher in patients with three-vessel involvement than those with no involvement. However, no significant difference was found between the homocysteine level of patients with three- and two-vessel involvement, and also those with two and no vessel(s) involvement. In our study, only a few patients had one-vessel involvement and because they had evidence of milder involvement of other vessels, they were considered among those patients with two-vessel involvement. This could be because these patients were less willing to take part in the study. In the studies of Mojiminiyi, Okada, and Akalin, the mean serum homocysteine of patients with coronary artery obstruction had been significantly more than that of patients with normal coronary arteries. There was also reported a significant relationship between the number of involved coronary vessels and mean serum homocysteine (Mojiminiyi et al. 2002; Akalin et al. 2008; Okada et al. 1999). The results of Gazzaruso and Hoogeveen studies were the same and showed a significant relationship between hyperhomocysteinemia and coronary artery obstruction in diabetic patients (type II) (Gazzaruso et al. 2002; Hoogeveen et al. 1998). However, Audelin study only showed a significant relationship between hyperhomocysteinemia and coronary artery disease mortality in patients with diabetes mellitus type II (Audelin and Genest 2001).
Current study showed no relationship between smoking and coronary artery disease in diabetic patients, while in Framingham study, smoking was established as a risk factor of coronary artery disease. This might be because hyperinsulinemia or hyperglycemia in diabetic patients plays a more prominent role than smoking in the development of atherosclerosis (Mann et al. 2014). Our study showed no relationship between hypertension and BMI and coronary artery obstruction in diabetes mellitus type II, however, Gazzaruso study showed otherwise (Gazzaruso et al. 2002). This could be due to the low number of patients studied. In this study, there was no significant relationship between the age of onset and duration of diabetes mellitus type II and mean serum homocysteine, which is consistent with the findings of Mojiminyi and Akalin studies (Mojiminiyi et al. 2002; Akalin et al. 2008). However, the mean serum homocysteine was significantly higher in patients with a duration of diabetes more than 10 years than those with a duration between 5 and 10 years, which could be due to the non-random sampling method of our study. It seems that the age of onset and duration of diabetes mellitus type II have no impression on the level of serum homocysteine, and instead, diet and genetic predisposition may play more prominent roles. This study showed no relationship between the age of onset and duration of diabetes mellitus type II and BMI, which is consistent with the findings of Gazzaruso and Hoogeveen studies (Gazzaruso et al. 2002; Hoogeveen et al. 1998).
There is more to be known about how diabetes mellitus affects the serum level of homocysteine. The reason behind the hyperhomocysteinemia seen in patients with diabetes mellitus type II without nephropathy still remains unknown (Zbidi et al. 2010; Wijekoon et al. 2007). As folate combinations lower the level of serum homocysteine in these patients, it appears that the low level of folate in these patients is a point trigger for the development of atherosclerosis. As it could be a possible way to lower the risk of coronary artery disease in patients with diabetes mellitus type II using folate combinations, more studies are required to be done in this regard (Okada et al. 1999; Wijekoon et al. 2007; Bondar et al. 2006).
Conclusion
The mean serum homocysteine of diabetic patients (type II) with coronary artery obstruction was significantly higher than that of those with normal coronary arteries. It was also significantly higher in patients with three-vessel involvement than those with no vessel involvement. There was a significant relationship between the serum level of homocysteine and coronary artery disease in patients with diabetes mellitus type II.
References
Akalin A, Alatas O, Colak O (2008) Relation of plasma homocysteine levels to atherosclerotic vascular disease and inflammation markers in type 2 diabetic patients. Eur J Endocrinol 158(1):47–52
American Diabetes Association (2013) Economic costs of diabetes in the U.S. in 2012. Diabetes Care 36(4):1033–1046
Antoniades C et al (2009) Homocysteine and coronary atherosclerosis: from folate fortification to the recent clinical trials. Eur Heart J 30(1):6–15
Atkinson W, Elmslie J, Lever M, Chambers ST, George PM (2008) Dietary and supplementary betaine: acute effects on plasma betaine and homocysteine concentrations under standard and postmethionine load conditions in healthy male subjects. Am J Clin Nutr 87(3):577–585
Audelin MC, Genest J (2001) Homocysteine and cardiovascular disease in diabetes mellitus. Atherosclerosis 159(2):497–511
Bondar I et al (2006) Hyperhomocysteinemia in coronary artery disease and hemostasis disorders in patients with type 2 diabetes mellitus. Klin Med 85(5):30–33
Dormandy JA, Charbonnel B, Eckland DJA, Erdmann E, Massi-Benedetti M, Moules IK, Skene AM, Tan MH, Lefèbvre PJ, Murray GD, Standl E, Wilcox RG, Wilhelmsen L, Betteridge J, Birkeland K, Golay A, Heine RJ, Korányi L, Laakso M, Mokáň M, Norkus A, Pirags V, Podar T, Scheen A, Scherbaum W, Schernthaner G, Schmitz O, Škrha J, Smith U, Tatoň J (2005) Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial in macroVascular Events): a randomised controlled trial. Lancet 366(9493):1279–1289
Esteghamati A, Gouya MM, Abbasi M, Delavari A, Alikhani S, Alaedini F, Safaie A, Forouzanfar M, Gregg EW (2008) Prevalence of diabetes and impaired fasting glucose in the adult population of Iran: National Survey of Risk Factors for Non-Communicable Diseases of Iran. Diabetes Care 31(1):96–98
Gazzaruso C et al (2002) Silent coronary artery disease in type 2 diabetes mellitus: the role of lipoprotein (a), homocysteine and apo (a) polymorphism. Cardiovasc Diabetol 1(1):5
Hadaegh F, Bozorgmanesh MR, Ghasemi A, Harati H, Saadat N, Azizi F (2008) High prevalence of undiagnosed diabetes and abnormal glucose tolerance in the Iranian urban population: Tehran Lipid and Glucose Study. BMC Public Health 8:176
Harrison T, Kasper D, Fauci A (2015) Harrison's Principles of Internal Medicine 19/E 2015: McGraw-Hill Education
Hoogeveen EK, Kostense PJ, Beks PJ, Mackaay AJC, Jakobs C, Bouter LM, Heine RJ, Stehouwer CDA (1998) Hyperhomocysteinemia is associated with an increased risk of cardiovascular disease, especially in non–insulin-dependent diabetes mellitus a population-based study. Arterioscler Thromb Vasc Biol 18(1):133–138
Hosseini ES, Moniri R, Goli YD, Kashani HH (2016) Purification of antibacterial CHAPK protein using a self-cleaving fusion tag and its activity against methicillin-resistant Staphylococcus aureus. Probiotics Antimicrob Proteins 8(4):202–210
Humphrey LL, Fu R, Rogers K, Freeman M, Helfand M (2008) Homocysteine level and coronary heart disease incidence: a systematic review and meta-analysis. Mayo Clin Proc 83(11):1203–1212
Jalali HK, Salamatzadeh A, Jalali AK, Kashani HH, Asbchin SA, Issazadeh K (2016) Antagonistic activity of Nocardia brasiliensis PTCC 1422 against isolated Enterobacteriaceae from urinary tract infections. Probiotics Antimicrob Proteins 8(1):41–45
Kannel W, McGee D (1979) Diabetes and glucose tolerance as risk factors for cardiovascular disease: the Framingham study. Diabetes Care 2(2):120–126
Kashani HH et al (2012) Synergism effect of nisin peptide in reducing chemical preservatives in food industry. Life Scie J Acta Zhengzhou Univ Overseas Edition 9(1):496–501
Kashani HH et al (2013) Expression of galectin-3 as a testis inflammatory marker in vasectomised mice. Cell J (Yakhteh) 15(1):11
Kazemi MS et al (2006) Homocysteine level and coronary artery disease. Angiology 57(1):9–14
Lotfi A et al (2016) Comparing the effects of two feeding methods on metabolic bone disease in newborns with very low birth weights. Global J Health Sci 8(1):249
Mann DL, Zipes DP, Libby P, Bonow RO (2014) Braunwald's heart disease e-book: a textbook of cardiovascular medicine. Elsevier Health Sciences
Mendis S, Davis S, Norrving B (2015) Organizational update: the world health organization global status report on noncommunicable diseases 2014; one more landmark step in the combat against stroke and vascular disease. Stroke 46(5):e121–e122
Mohammadi M et al (2005) Is there any difference in the plasma homocysteine levels of diabetes mellitus type II patients, impaired glucose tolerance subjects and normal people? J Shahid Sadoughi Univ Med Sci 13(3):26–30
Mojiminiyi O et al (2002) Association of C-reactive protein with coronary heart disease risk factors in patients with type 2 diabetes mellitus. Diabetes Res Clin Pract 58(1):37–44
Nikzad H, Haddad Kashani H, Kabir-Salmani M, Akimoto Y, Iwashita M (2013) Expression of galectin-8 on human endometrium: molecular and cellular aspects. Iran J Reprod Med 11(1):65–70
Okada E, Oida K, Tada H, Asazuma K, Eguchi K, Tohda G, Kosaka S, Takahashi S, Miyamori I (1999) Hyperhomocysteinemia is a risk factor for coronary arteriosclerosis in Japanese patients with type 2 diabetes. Diabetes Care 22(3):484–490
Perry IJ, Morris RW, Ebrahim SB, Shaper AG, Refsum H, Ueland PM (1995) Prospective study of serum total homocysteine concentration and risk of stroke in middle-aged British men. Lancet 346(8987):1395–1398
Piroozmand A, Kashani HH, Zamani B (2017) Correlation between Epstein-Barr virus infection and disease activity of systemic lupus erythematosus: a cross-sectional study. Asian Pac J Cancer Prev 18(2):523–527
Saba M et al (2017) Diagnostic value of neuron-specific enolase (NSE) and cancer antigen 15-3 (CA 15-3) in the diagnosis of pleural effusions. Asian Pac J Cancer Prev 18:257
Sadeghian S et al (2006) Homocysteine, vitamin B12 and folate levels in premature coronary artery disease. BMC Cardiovasc Disord 6(1):38
Sharif MR, Kashani HH, Ardakani AT, Kheirkhah D, Tabatabaei F, Sharif A (2016) The effect of a yeast probiotic on acute diarrhea in children. Probiotics Antimicrob Proteins 8(4):211–214
Sharif A, Kashani HH, Nasri E, Soleimani Z, Sharif MR (2017) The role of probiotics in the treatment of dysentery: a randomized double-blind clinical trial. Probiotics and antimicrobial proteins 9(4):380–385
Shekelle P (2006) Lowering homocysteine with folic acid and B vitamins did not prevent vascular events in vascular disease. Evid Based Med 11(4):104
Soinio M, Marniemi J, Laakso M, Lehto S, Rönnemaa T (2004) Elevated plasma homocysteine level is an independent predictor of coronary heart disease events in patients with type 2 diabetes mellitus. Ann Intern Med 140(2):94–100
Unwin N, Whiting D, Guariguata L (2013) International Diabetes Federation. IDF diabetes atlas. Brussels, Belgium: International Diabetes Federation
Wijekoon E, Brosnan M, Brosnan J (2007) Homocysteine metabolism in diabetes. Biochem Soc Trans 35(5):1175–1179
Zbidi H, Redondo P, López J, Bartegi A, Salido G, Rosado J (2010) Homocysteine induces caspase activation by endoplasmic reticulum stress in platelets from type 2 diabetics and healthy donors. Thromb Haemost 103(5):1022–1032
Acknowledgments
The researcher wishes to express his appreciation to the full cooperation of the patients and personnel who participated in this study and the Clinical Research Center of Shahid Mostafa Khomeini Hospital.
Availability of data and materials
The dataset used in this study is available with the authors and can be made available upon request.
Funding
The financial support for the current research was provided by Research Deputy of Shahed University of Medical Sciences, Tehran, Iran.
Author information
Authors and Affiliations
Contributions
All the authors participated in the study design. Mohammad Reza Rajabi and Mohammad Reza Razzaghof collected and documented the data and assisted in preliminary data analysis. Mohammad Reza Rajabi wrote the initial draft. Mohammad Reza Rajabi and Hamed Haddad Kashani in draft revision, data analysis, and editing of the final draft.
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no competing interests.
Informed consent
Informed consent or a substitute for it was obtained from all patients included in the study.
Ethics approval and consent to participate
This study was approved be Shahed University of Medical Sciences under the grant number of 16/35/10/3560 in 14 July 2015. The informed consent form was signed by all parents. All procedures involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and ethical standards of the institutional and national research committee of Shahed University of Medical Sciences and obtained ethics committee permission number of SHUM.REG.1393.136.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rajabi, M.R., Razzaghof, M.R. & Haddad Kashani, H. Hyperhomocysteinemia and increased risk of coronary artery disease in Iranian patients with diabetes mellitus type II: a cross-sectional study. Comp Clin Pathol 29, 223–230 (2020). https://doi.org/10.1007/s00580-019-03027-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00580-019-03027-5