
Abstract
To study the psychosocial profile of patients of acromegaly in a developing country setting. Seventeen patients with acromegaly underwent a cross-sectional assessment regarding their socio-demographic and clinical profile, life events, social support, coping, dysfunction, quality of life and psychiatric morbidity. Seventeen demographically matched healthy participants (free from psychological morbidity) acted as the control group. The acromegaly group had predominance of urban married males (64.7%) with mean age 36.05 ± 17.06 years (range = 15–61), and mean duration of illness of 36.05 ± 42.5 (range = 4–240) months. Six subjects (i.e., GHQ-positive group) scored positive (indicating presence of psychiatric morbidity) on the General Health Questionnaire-12 giving a psychiatric morbidity rate of 33.33%, with five fulfilling an ICD-10 diagnosis. Compared to the GHQ-negative group, the GHQ-positive group had more number of life events in the entire lifetime, used significantly more number of emotional coping strategies, had more dysfunction, and poorer quality of life (in domains of physical health, social relationship, and general well-being). Psychiatric morbidity occurs in a significant percentage of patients with acromegaly. Presence of psychiatric morbidity is associated with dysfunction and poorer quality of life.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acromegaly is a rare, chronic debilitating, and disfiguring disorder with a low incidence (3–4 per million) and prevalence (36–69 per million) [1, 2]. The rarity may add to the delay in the diagnosis and increase complications and problems [3]. Often caused by a pituitary tumor that secretes excess growth hormone (GH), acromegaly is associated with enlargement of extremities, multi-organ dysfunction, functional limitations, diminished productivity, social isolation, and poor quality of life [4, 5]. Recent studies have also shown that proper treatment of acromegaly also leads to improvement in quality of life [6, 7]. Because of disfigurement, functional limitations and poor quality of life, acromegaly is also associated with psychological disturbances [4, 5]. The stress of disfigurement and the side effects of medications and radiotherapy may add to the psychological problems [4]. Psychological morbidity has been reported in the form of lability of mood and personality changes [8], psychological distress, social fears and poor well-being [9], depression [10–12], post-traumatic stress disorders [13], and psychosis [14]. The psychosocial milieu of the developing countries may possibly be more severely stigmatizing for disfigurement than that of the developed countries [15, 16]. The research data on psychological aspects of acromegaly being sparse and almost exclusively from the western countries, the present research was planned as a cross-sectional study of psychosocial profile of acromegaly in India, a developing country.
Material and methods
Setting
The study was carried out at the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh. PGIMER is a multi-specialty teaching tertiary-care hospital providing services to a major area of North India and catering to approximately 40 million people.
Design
Cross-sectional assessment
Sample
Participants were recruited between August 1999 and March 2001 on the basis of purposive sampling based on inclusion and exclusion criteria. The purposive sample comprised two groups: acromegaly patients (N = 17) and matched healthy controls (N = 17).
The acromegaly group included patients of both genders and age range 20–50 years who were seeking outpatient or inpatient treatment from the Endocrinology services of the Institute. The patients were identified and listed by the Consultant Endocrinologist (AKB) from the existing departmental records. Most of them were on active follow-up and treatment. As per the study protocol, patients with established diagnosis of acromegaly or who were diagnosed during the study period were identified for recruitment. The prospective patients were contacted during their routine follow-up visits or by writing letters to them if they were missing such visits. In addition, newly diagnosed patients with acromegaly were also included in the study. Acromegaly was diagnosed (a) clinically by classical morphological features and (b) biochemically by high basal growth hormone (GH) and its non-supressability (>2 ng/ml) within 1–2 h after 50–100 gm glucose load [17, 18]. Imaging studies were carried out to substantiate the source of growth hormone. Patients with pseudo-acromegaly (i.e., those with presence of acromegaloid features in the absence of elevated growth hormone), dilantin therapy, insulin resistance syndrome, and primary hypothyroidism were excluded. There were no refusers. However, the recruitment was purposive in that it entirely depended on the availability of the psychologist and the cases were missed during her absence.
The healthy control group comprised subjects recruited from the attendants/relatives of the patients attending the dermatology outpatient department of the Institute. The recruitment was based on an estimated group-matching with acromegaly patients for age, gender, education, marital status, locality, and the control group subjects being free from any major physical or psychiatric illness. Presence or absence of possible psychiatric morbidity was determined by administration of General Health Questionnaire-12 Item (GHQ-12) as explained in the next section.
Instruments
The following instruments, as required, were used in the two groups:
-
1.
Sociodemographic profile sheet: Specially developed for this study, it was used to record the relevant sociodemographic data on age, gender, education, marital status, and locality for both the groups.
-
2.
Clinical profile sheet: Specifically developed for this study, it was used to record the following clinical details about acromegaly: duration of illness, age at onset, growth hormone (GH) levels-basal and at 30 mins, 60 mins, 90 mins, and 120 mins after 75 gm glucose load, and blood glucose (BG) levels—fasting and postprandial.
-
3.
Presumptive Stressful Life Events Scale (PSLES) [19]: Based on Stressful Life Events Scale of Holmes and Rahe [20], PSLES has been standardized with 51 life events relevant to the Indian setting. Based on their data the authors reported that an adult in India experienced an average of 10 events (mean ± SD: 10.34 ± 5.40) in a lifetime and 2 events (mean ± SD: 1.90 ± 2.62) in the past one year without suffering any physical or psychological disturbance. In the present study the number of life events was recorded for the lifetime, before onset and after onset of acromegaly.
-
4.
Social Support Questionnaire (SSQ) [21]: A Hindi language adaptation of Social Support Questionnaire [22], it assesses the perceived social support. It has a test-retest reliability of 0.59 and correlation with clinician’s assessment at 0.80 and with items of social support from Family Interactions Pattern Scale [23] at 0.65. The 18 items of the scale are rated from 1 to 4, and a higher score in the possible range of 1 to 72 indicates a better social support.
-
5.
Coping Strategies Check List - Hindi (CSCL) [24]: A self-administered yes/no checklist with high reliability, CSCL lists coping strategies used by people to deal with the situations which trouble them. The checklist covers all stressors and is not disease specific. The 36 strategies have been factored into 5 factors: denial, internalize, externalize, emotional outlet, and anger. A higher score indicates greater use of coping strategies. A Hindi translation with Cronbach’s alpha of 0.64 was developed and has been earlier used in our center [25].
-
6.
Dysfunction Analysis Questionnaire (DAQ) [26]: Developed at PGIMER, this questionnaire assesses the dysfunction as compared to the pre-illness level of functioning across five areas—social, vocational, personal, family, and cognitive. Five point scaling of 50 item gives a possible disability score range of 46 to 100 for individual domains and 206 to 500 for the total, a higher score indicating a higher dysfunction. With a proven validity and reliability (test-retest reliability of 0.77–0.92 for various domains) this questionnaire in Hindi language provides norms for the local population and has been widely used in India on different clinical populations.
-
7.
WHO Quality of Life Scale-Bref (WHOQOL-B): A shorter version of the WHOQOL 100 item scale, WHOQOL-B is a self-administered psychometrically sound cross-cultural instrument developed in 15 centers across developing and developed countries [27]. As a generic scale available in Hindi language [28], it profiles the subjective (rather than the objective) evaluation of the QOL in the past 2 weeks for 4 domains: physical health, psychological health, social relationship, and environment. The 26 items are scored 1–5 to give domain scores and a total score range of 26 to 130, a higher score indicating a better quality of life. At the time of planning and initiation of this study no acromegaly-specific quality of life instrument was available [29].
-
8.
General Health Questionnaire–12 (GHQ-12): GHQ-12 is a derivative of General Health Questionnaire that was developed as a valid and reliable self-administered 60-item screening measure for psychological problems in primary care and community settings [30]. GHQ-12 used in the present study is based on the Hindi translation of the 60-item General Health Questionnaire that has been standardized in India and in Indian population [31, 32] and has been used in our center earlier in research with patients suffering with vitiligo and psoriasis [16, 33, 34]. In the present study, to define a case with possible psychiatric morbidity a score ≥2 was used. This is because GHQ scores of 1 or 2 are considered as the best cutoff or threshold for psychiatric diagnosis [35]. The HC group had GHQ scores of <2 indicating absence of psychological distress and psychiatric morbidity.
-
9.
Comprehensive Psychopathological Rating Scale (CPRS) [36]: CPRS assesses the full range of psychopathology with a high reliability. Each scale step is operationally defined on the basis of intensity, frequency, and duration of the symptoms. The 65 items are explicitly described and scored from 0 to 3. Two indices have been derived from the CPRS: Anxiety Index (AI) with 7 items [37] and Depression Rating Scale (MADRS) with 10 items [38].
-
10.
International Classification of Diseases-10th revision (ICD-10) [39]: ICD-10 was used to arrive at the clinical diagnoses based on a detailed psychiatric assessment.
Procedure
The Consultant Endocrinologist (AKB) confirmed the diagnosis of acromegaly and after proper informed consent as per the protocol, carried out the initial recruitment and assessment using the sociodemographic and clinical profile sheets. Thereafter, the psychologist (RM) administered the PSLES, SSQ, CSCL, DAQ, WHOQOL-B, and GHQ-12 on the same day, over a maximum of two sessions of 1–2 h each. Those with GHQ score ≥2 were interviewed in detail by a Consultant Psychiatrist (NG) who used CPRS and ICD-10, and determined the presence/absence and severity of the psychiatric illness. Additionally, the psychologist (RM) recruited matched subjects for the control group based on GHQ score <2.
Ethical considerations
All the subjects were recruited on the basis of a written informed consent assuring confidentiality and freedom of choice of participation. The study had been cleared by the Research Ethics Committee of the Institute.
Statistical analysis
Non-parametric variables were subjected to Chi-square analysis, while parametric variables were analyzed using Student’s t-test.
Results
Demographic profile
As per the study design the acromegaly and healthy control groups had similar sociodemographic profiles in terms of age in years, education in years, gender, marital status, and locality.
Whole group: The sample had a predominance of urban married males (64.7%) with education ranging 0–14 years (Mean ± SD: 8.05 ± 4.66 years), age ranging 15–61 years (36.05 ± 17.06 years), age at onset ranging 14–60 years (Mean ± SD: 33.05 ± 16.02 years), and duration of illness ranging 4–240 months (Mean ± SD: 36.05 ± 42.55 months). All patients were post-operative, and were evaluated within 12 months of surgery. The mean basal GH level done within 3 preceding months was 27.05 (sd: ± 22.89) and it remained non-suppressible at 60 min (Mean ± SD: 19.99 ± 19.98) after glucose load. All patients had macroadenoma of >10 mm. In the post-operative phase all were being treated with ketoconazole, radiotherapy, hormone supplements, and orthopedic services as required.
The life events were reported at a mean of 6.58 events before and 1.88 events after the onset of acromegaly. The perceived social support was scored at a mean of 51.82. The number of coping strategies used ranged from a mean of 0.88 for emotional to 3.41 for denial and 10.23 for all strategies taken together. The reported dysfunction ranged from 47.05 for family domain to 49.29 for personal domain and 48.60 for mean of all domains considered together. The QOL scores ranged from 5.58 for general well-being to 21.23 for environmental health domain and 70.75 for all domains taken together (Table 1).
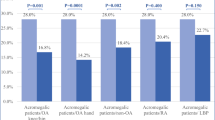
GHQ positive vs GHQ negative subgroups: By study design the healthy control group subjects were all GHQ negative. Out of 17 acromegaly subjects, 6 were GHQ positive (scores ≥2), giving a psychological morbidity prevalence of 35.29%. The two acromegaly sub-groups—GHQ positive (N = 6) and GHQ negative (N = 11)—were comparable on sociodemographic profile (locality, marital status, sex, age, and education) and illness profile (age at onset, duration of illness, operated number of months back, and the growth hormone levels).
The two subgroups were also similar for the psychological profile in terms of the life events before and after the onset of acromegaly, social support, coping strategies used (except emotional), and for psychological health and environmental health domains and total score of QOL. However, the GHQ positive subgroup had significantly more life events in the entire lifetime (t = 2.75, P < 0.05), more use of emotional coping strategy (t = 2.19, P < 0.05), more dysfunction—all domains (P = 2.58 to 2.86, P < 0.05) and total (t = 3.02, P < 0.01), and poorer QOL in domains of physical health (t = 2.19, P < 0.05), social relationship (t = 2.19, P < 0.05), and general well-being (t = 2.56, P < 0.05) (Table 1).
The psychopathology scores for GHQ-positive cases were: CPRS–21.87 ± 16.48; MADRS–4.37 ± 4.30; and ASI–19.87 ± 16.63. Out of the 6 GHQ-positive cases, 5 had a diagnosable psychiatric disorder as per the ICD-10 (Table 2).
Discussion
The demographic and clinical profile of our acromegaly cases is similar to the one described in the standard references [18]. The 3-year delay in diagnosis compared to 9 years in late 1980/early 1992 series of Duncan and Wass [18] may reflect improvement in health care availability and utilization. The excess of married urban males may reflect the cultural norm in India of almost universal marriage and of urban subjects using health services more often [40].
In our study the psychiatric morbidity (as per GHQ cut off ≥2) was 35.29%. Out of the 6 GHQ-positive subjects, five (29.4% of the whole sample) met the ICD-10 diagnostic criteria for a psychiatric diagnosis. These data on psychiatric morbidity can be compared with only one study [41] that used GHQ-60, PSE, and ICD-9 and identified GHQ ‘threshold’ score ≥12 in 10 out of 51 (19.6%) subjects and PSE/ICD-9 diagnoses of depression in 5 out of 41 cases (12.2%, 2 cases of manic depression and 3 cases of neurotic depression). Our study results are similar in that all the cases with psychiatric morbidity suffered from some form of depression. In contrast though our rates of both GHQ-12 and ICD-10 assessed psychiatric morbidity were one and a half to two times higher; these differences could be due to one or more of the following factors operating individually or in varying combinations—sampling, ethno-biological, or socio-cultural factors.
WHOQOL results reflected a moderate QOL with mean scores ranging from 5.58 (general well-being) to 21.23 (environmental health) and 70.75 for all domains considered together. These findings are comparable to those in acromegaly reporting QOL being impaired and worsening after radiotherapy [42, 43] as also of the DSM-IV diagnosed major depression patients who reported mean scores ranging from 4.60 (general well-being) to 18.50 (environmental health) and 66.02 for all domains taken together [44]. Thus the QOL seems to be moderately impaired in subjects suffering with acromegaly.
As there are no data about dysfunction, social support, coping strategies, and life events in acromegaly literature, we compared the same with acromegaly data with other physical illnesses. The reported dysfunction in our sample was mild with the mean domain scores ranging from 47.05 (family) to 47.64 (social) and 48.60 for total score. This dysfunction profile indicates lesser disability in comparison to patients in India with vitiligo and psoriasis whose mean disability scores were 54.40 and 58.60, respectively [16]. The reasons for this may be that the more externally disfiguring dermatological conditions contribute to greater dysfunction. The number of coping strategies used by our sample was low ranging from a mean of 0.88 (emotional) to 3.41 (denial) and 10.23 for all strategies taken together. This is low (with different usage) in comparison to post-mastectomy pre-radiotherapy breast cancer subjects at our center whose mean scores ranged from the lowest of 0.33 (anger) to 9.53 (denial) and 19.27 for all strategies taken together [25]. Understandably the perceived stress and the degree and nature of coping needed in acromegaly are dissimilar to that in a potentially life-threatening malignancy like breast cancer. The perceived social support in our sample was moderate with a mean of 51.12, which is comparable to the mean of 56.66 among the healthy adult female population [21]. The reported life events at a mean of 6.58 events before and 1.88 events after the onset (mean of 3 years) of acromegaly and during lifetime (8.47) were acceptable, though somewhat lower compared to the general population in whom the expected number is 10 events in lifetime and <2 events in the previous year [19]. This pattern of less life events (both in the lifetime and in the years preceding or following the onset of acromegaly) implies, in all probability, a lack of association between increases in the life events with onset of acromegaly.
Differences between GHQ positive and GHQ negative subgroups
GHQ-positive subgroup experienced more lifetime events, more dysfunction in most of the domains, and poorer QOL in the domains of physical health, social relationship, and general well-being. Also, the CPRS scores indicated mild to moderate severity of the psychiatric symptoms. This suggests that the psychiatric morbidity is related to the impact of the disease, and not to demographic, other psychological, and clinical variables including the growth hormone levels. This also implies that our study has not indicated whether or not there are any culture/social milieu-specific aspects to psychopathology in acromegaly. Also, our data did not reflect a consistent relationship between depression and growth hormone levels [45].
References
A.F Daly, P. Petrossians, A. Beckers, J. Endocrinol. Invest. 28 (Suppl 11), 67–69 (2005)
J. Etxabe, S. Gaztambide, P. Latorre, J.A. Vazquez, J Endocrinol Invest. 16, 181–187 (1993)
P. Coskeran, Nurs. Times. 95, 50–52 (1999)
S. Ezzat, G.E. Wilkins, Y. Patel, E. Ur, O. Rorstad, O. Serri, Clin. Invest. Med. 19, 259–270 (1996)
L.J. Woodhouse, A. Mukherjee, S.M. Shalet, S. Ezzat, Endocr. Rev. 27, 287–317 (2006)
S.J. Neggers, M.O. van Aken, W.W. de Herder, R.A. Feelders, J.A. Janssen, X. Badia, S.M. Webb, A.J. van der Lely, J. Clin. Endocrinol. Metab. 2008 Jul 22. [Epub ahead of print] (2008)
A.N. Paisley, S.V. Rowles, M.E. Roberts, S.M. Webb, X. Badia, L. Prieto, S.M. Shalet, P. Trainer, J. Clin. Endocrinol. (Oxf.) 67, 358–362 (2007)
P. Pantanetti, N. Sonino, G. Arnaldi, M. Boscaro, J. Endocrinol. Invest. 26(Suppl 8), 35–38 (2003)
N. Sonino, G.A. Fava, F. Fallo, M. Boscaro, Psychother. Psychosom. 54, 140–144 (1990)
T.L. Avery, Br. J. Psychiatry. 122, 599–600 (1993)
A. Margo, Acromegaly and depression. Br. J. Psychiatry. 139, 467–468 (1981)
E.M. Whitehead, S.M. Shalet, D. Davies, B.A. Enoch, D.A. Price, C.G. Beardwell, Clin. Endocrinol. 17, 271–277 (1982)
K. Furman, K. Ezzat, Psychother. Psychosom. 67, 147–153 (1998)
D.B. Schulte, Schweiz. Arch. Neurol. Neurochir. Psychiatr. 118, 357–377 (1976)
S.K. Chaturvedi, G. Singh, N. Gupta, Dermatol Clin. 23, 635–642 (2005)
S.K. Mattoo, S. Handa, I. Kaur, N. Gupta, R. Malhotra, J. Dermatol. 28, 424–432 (2001)
I. Shimon, S. Melmed, Psychother. Psychosom. 67, 119–124 (1998)
E. Duncan, J.A.H. Wass, Clin. Endocrinol. 50, 285–293 (1999)
G. Singh, D. Kour, H. Kour, Indian J. Psychiatry. 26, 107–114 (1984)
T.H. Holmes, R.H. Rahe, J. Psychosom. Res. 11, 213–218 (1967)
R. Nehra, P. Kulhara, S.K. Verma, Indian J. Clin. Psychol. 23, 33–39 (1996)
L. Pollock, R. Harris, Psychological Report. 53, 446 (1983)
R.S. Bhatti, D.K. Subhakrishna, B.L. Ageior, Indian J. Psychiatry. 28, 211–216 (1986)
C.L. Cooper, E.B. Faragher, Psychol. Med. 22, 447–455 (1992)
Y. Sharma, S.K. Mattoo, P. Kulhara, S.C. Sharma, P. Sharan, German J. Psychiatry. 6, 40–48 (2003)
D. Pershad, S.K. Verma, S. Malhotra, A. Malhotra, Measurement of Dysfunction and Dysfunction Analysis Questionnaire (National Psychological Corporation, Agra, 1985)
S.M. Skevington, M. Lotfy, K.A. O’Connell, WHOQOL Group, A report from the WHOQOL group. Qual. Life Res. 13, 299–310 (2004)
S. Saxena, K. Chandramani, R. Bhargava, Natl. Med. J. Ind. 11, 160–166 (1998)
S.M. Webb, L. Prieto, X. Badia, M. Albareda, M. Catala, S. Gaztambide, T. Lucas, C. Paramo, A. Pico, A. Lucas, I. Halperin, G. Obiols, R. Astorga, Clin. Endocrinol. 57, 251–258 (2002)
D. Goldberg, The Detection of Psychiatric Illness by Questionnaire, Maudsley Monograph No. 21 (Oxford University Press, London, 1972)
S. Gautam, M. Nijhawan, P. Kamal, Indian J. Psychiatry. 29, 63–66 (1987)
K.S. Jacob, D. Bhugra, A.H. Mann, Indian J. Psychiatry. 39, 196–199 (1997)
S.K. Mattoo, S. Handa, I. Kaur, N. Gupta, R. Malhotra, J. Eur. Acad. Dermatol. Venereol. 16, 573–578 (2002)
S.K. Mattoo, S. Handa, I. Kaur, N. Gupta, R. Malhotra, German J. Psychiatry. 8, 17–22 (2005)
A. Cano, R.P. Sprafkin, D.J. Scaturo, L.J. Lantinga, B.H. Fiese, F. Brand, Prim Care Companion J. Clin. Psychiatry. 3, 206–210 (2001)
M. Åsberg, S.A. Montgomery, C. Perris, D. Schalling, G. Sedvall, Acta. Psychiatr. Scand. Suppl. 271, 5–28 (1978)
E.W. Martinsen, S. Friis, A. Hoffait, Acta Psychiatr. Scand. 80, 492–498 (1989)
S.A. Montgomery, M. Åsberg, Br. J. Psychiatry. 134, 382–389 (1979)
World Health Organization, The International Classification of Diseases-10th revision (World Health Organization, Geneva, 1992)
National Council for Applied Economic Research (NCAER), Household Survey of Medical Care (NCAER, New Delhi, 1992)
R.T. Abed, J. Clark, M.H.F. Elbadawy, M.J. Cliffe, Acta Psychiatr. Scand. 75, 635–639 (1987)
S.V. Rowles, L. Prieto, X. Badia, S.M. Shalet, S.M. Webb, P.J. Trainer, J. Clin. Endocrinol. Metab. 90, 3337–3341 (2005)
N.R. Biermasz, S.W. van Thiel, A.M. Pereira, H.C. Hoftijzer, A.M. van Hemert, J.W.A. Smit, J.A. Romijn, F. Roelfsema, J. Clin. Endocrinol. Metab. 89, 5369–5376 (2004)
N. Painuly, P. Sharan, S.K. Mattoo, Psychiatry Res. 153, 39–45 (2007)
J.D. Amsterdam, G. Maislin, B. Skolnick, N. Berwish, A. Winokur, Biol. Psychiatry. 26, 265–278 (1989)
Acknowledgment
The research was funded by a Research Grant from the Postgraduate Institute of Medical Education and Research, Chandigarh.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mattoo, S.K., Bhansali, A.K., Gupta, N. et al. Psychosocial morbidity in acromegaly: a study from India. Endocr 34, 17–22 (2008). https://doi.org/10.1007/s12020-008-9112-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-008-9112-8