
Abstract
Autism spectrum disorder (ASD) and attention-deficit hyperactivity disorder (ADHD) are two developmental disorders that affect children worldwide, and are linked to both genetic and environmental factors. This study aims to investigate the levels of lead, manganese, and zinc in each of ASD, ADHD, and ASD with comorbid ADHD in Syrian children born or grown during the Syrian crisis. Lead and manganese were measured in the whole blood, and zinc was measured in the serum in 31 children with ASD, 29 children with ADHD, and 11 children with ASD with comorbid ADHD (ASD-C) compared with 30 healthy children, their ages ranged between 3 and 12 years. Blood lead levels were higher in the groups of ASD-C (245.42%), ASD (47.57%), and ADHD (14.19%) compared with control. Lead levels were significantly higher in children with ASD in the age of 5 or less compared with control, and they were also higher in the male ASD compared with females (P = 0.001). Blood manganese levels were lower in the groups of ASD-C (10.35%), ADHD (9.95%, P = 0.026), and ASD (9.64%, P = 0.046). However, serum zinc levels were within the reference range in all groups of study. Lead and manganese were positively correlated with each other (P = 0.01). Lead increase and manganese decrease may associate with the incidence of ASD, ADHD, or the co-occurrence of both of them together. Further studies are needed to examine the relationship between metal levels and the co-occurrence of ASD and ADHD together.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a developmental disorder that causes social difficulties, non-verbal communication challenges, and is characterized with patterns of restricted and repetitive behaviors [1]. ASD is firstly diagnosed in the childhood, and its signs are demonstrated obviously at the age of 2–3 years [2]. Attention-deficit hyperactivity disorder (ADHD) is one of the most common developmental disorders that are generally first diagnosed at the age of school due to the problems with the schoolwork. ADHD affects 8.4% of children and 2.5% of adults worldwide [3]. ADHD comorbidity is common in ASD, and it has been documented to affect up to 30% of children with ASD [4]. In addition, Diagnostic and Statistical Manual of Mental Disorders in its 5th Edition (DSM-V) allows a comorbid diagnosis of ADHD with ASD [5]. Although genetics play a major role in both ASD and ADHD [6], the recent studies suggest that environmental factors may play an important role in combination with genetic susceptibility in ASD and ADHD etiology [7, 8]. Moreover, many studies revealed a dysregulation in toxic metals such as lead and mercury, as well as essential metals in both ASD and ADHD [9,10,11,12,13,14,15,16].
Lead is a toxic metal that can literally affect all organs even in low levels [17], but its neurotoxicity has received a greater attention in children, since it has many adverse neurological and behavioral impacts on the developing brain [18, 19]. Children who live in old houses can be exposed to lead-based paints by eating paint chips. Furthermore, children are susceptible to lead during pregnancy, because it has the ability to cross placenta [20].
Manganese is an essential metal that is important for mental health, because it contributes to the brain protection against free radicals that can damage brain cells in the neurons due to its antioxidant properties, particularly its role in superoxide dismutase (SOD) [21].
Zinc is also an essential metal that it is involved in the structure and function of the brain [22]. It regulates cellular connections in hippocampus, and regulates the activity of the pituitary axis [23]. Zinc also has antioxidant effects, and its deficiency in the brain can cause widespread nerve damage by increasing the formation of free radicals [24]. Poor zinc levels in children have been associated with reduced learning ability, apathy, lethargy, and mental retardation [25].
One study in China [9] found that children with ASD had dramatically increased blood levels of lead (P ≤ 0.01), and decreased blood levels of manganese (≤ 0.05). However, Rahbar [10] did not find any difference in blood levels of manganese in his study. In Al-Ayadhi study [11], lead levels were increased, while manganese levels were decreased in hair samples of both of autistic and attention-deficit disorder children, while there was no difference in zinc levels.
Adams et al. [12] found in their study significant higher levels of lead in red blood cells of children with ASD (P = 0.002). One study in Korea [13] found children with ADHD had higher levels of lead in blood (P = 0.003).
In Li et al. study [14] and Al-baz study [15], zinc levels were decreased in serum of ASD and ADHD children, respectively. However, in Yousef et al. study [16], zinc levels were increased in blood samples of children with ADHD (P = 0.005).
In war zones in general, and in the Syrian crisis in particular, children exposure to lead has increased due to bomb explosions and bullets that polluted the environment. The crisis also has a detrimental effect on children nutrition in several areas, due to shortage in food, which leads to essential metal deficiency.
The present research aims at investigating lead, zinc, and manganese levels in children diagnosed with ASD, ADHD, and ASD with comorbid ADHD, and to determine whether these metals play a role in neurodevelopmental disorders during the Syrian crisis.
Methods
Participants
This case-control study was conducted on 101 children: 71 patients, comprising 31 children with ASD, 29 children with ADHD, in addition to 11 children with ASD of comorbid ADHD (ASD-C) and of hyperactive subtype as well. Control group comprised 30 healthy properly matched children. Children were diagnosed based on DSM-5 criteria, and they were assessed on Childhood Autism Rating Scale (CARS), a tool that aids in the diagnosis of ASD completed by clinicians depending on parent report and direct observations, and ADHD rating scales, a diagnostic tool also based on parent or teacher report.
The ages of the participating children ranged between 3 and 12 years, and males formed the largest part of the participating children. Patients were recruited from Children Hospital, and from associations concerned with the rehabilitation of mentally challenged children. All subjects compiled a questionnaire included age of diagnosis, maternal and paternal age at contraception, consanguineous marriage, the presence of mother dental amalgam fillings, and if the child took all vaccinations. The protocol of the investigation was approved by the Ethics Committee at Damascus University. Moreover, informed consent was obtained from the parents of the examined children before joining the study, and blood sampling was performed in the presence of parents.
Collection of Blood Samples
Five milliliters of venous blood samples was collected from the cubital vein, and were divided in two tubes: the first is a heparinized blood collection tube, and the second is a vacuum blood collection tube, where lead and manganese levels were determined in whole blood, and zinc levels were measured in the serum. All measurements were carried out in Al-Khateeb Lab in Damascus, Syria.
Lead and Manganese Measurements
Blood samples were digested by microwave-assisted acid digestion method using Microwave Digestion Speedwave Entry (Berghof, Germany) based on the method of Gok et al. [26]. Three milliliters of freshly prepared mixture of concentrated nitric acid and hydrogen peroxide [HNO3-H2O2] (2:1 v/v) was added to 1 ml of whole blood. After that, it was digested in microwave for 21 min, while the temperature was raised gradually to 180 °C.
The measurements of lead and manganese were carried out using a ZEEnit 700p atomic absorption spectrometer (Analytik Jena AG, Germany), with the following conditions: 3.0 and 7.0 mA lamp current, 283.3 nm and 279.5 nm, 0.8 and 0.2 nm for lead and manganese, respectively, 20 μl sample volume, and 200 ml/min gas flow.
Zinc Colorimetric Assay
Serum zinc level is one of the most commonly used indices for evaluating zinc deficiency, and it was implemented in many studies previously. The measurements were carried out using auto analyzer Olympus AU400 (Olympus, Tokyo, Japan) provided with multi-wavelength diffraction grating spectrophotometer by colorimetric assay using 5-Br-PAPS commercially available kit (Dialab, Australia) at 560 nm. This method depends on the ability of zinc to form a chelate complex with 2-(5-bromo-2 pyridylazo)-5-(N-propyl-N-sulfo-propylamino-phenol) (5-Br-PAPS), while the absorption of this complex is proportional to the total zinc concentration in the sample.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) computer program Version 25 was used. The results were expressed as the mean ± SD. The logistic regression analysis was used to study the relationship between metal levels and cases, where the metals were considered as independent variable, and the probability of the case as one dependent binary variable. The change in the odds ratio of each case was estimated to assess the extent of the effects of the metals, and it was calculated as [Exp(B) − 1] × 100 per unit increase in blood concentrations, where negative values represent a decrease in odds of the case while positive values represent an increase. Kruskal-Wallis test was employed to compare metal levels between the three cases and control, and the test was used to analyze bivariate data. Spearman’s rank correlation coefficient was obtained to assess the correlation between measured metal levels. A par value of 0.05 or lower was assumed significant.
Results
The Sociodemographic Data
Table 1 shows the sociodemographic data of the participants.
Metal Levels in the Study Groups
The levels of lead, manganese, and zinc are represented in Table 2. Lead levels were elevated in the groups of ASD, ADHD-H, and ASD-C compared with the controls with no significance. The highest levels of lead were in ASD-C group with increase of 245.42%. While concentrations of lead were elevated in ASD and ADHD-H groups with increase of 47.57% and 14.19%, respectively, without significance. The levels of manganese were significantly lower in each of ASD, ADHD-H groups comparing with the control group (P = 0.026, P = 0.03, respectively). In ASD-C group, the levels of manganese were lower than control but not significantly different. The decrease was 9.64%, 9.95%, and 10.35% in ASD, ADHD-H, and ASD-C, respectively. There was no difference in zinc levels in any of the groups studied compared with the control.
Comparison of Metal Levels Between Cases and Control According to Age Groups
Further analyses of comparison were applied according to different age groups (Table 3). Table 3 shows that lead levels were significantly high in children with ASD comparing with controls in the group of children age 5 or less (P = 0.008).
Metal Level Comparison Between Males and Females
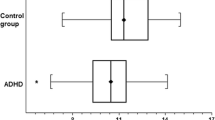
Metal levels were compared between males and females in each group (Table 4). Table 4 shows that lead levels were significantly high in the males of control and ASD groups compared with females (P = 0.01, 0.001 respectively). Manganese levels were significantly low in the males of control group compared with females (P = 0.002).
The Logistic Regression Analysis Results and the Change in the Odd Ratio
Tables 5, 6, and 7 show logistic regression analysis results of metals in each of ASD, ADHD-H, and ASD-C, respectively. The strongest association was found in manganese followed by lead, and there was no association with zinc in both ASD and ADHD groups. For ASD-C group, none of the metals had any association. The odd ratio of ASD increased by 147.5% when lead concentration increased by 1 μg/dl, and by 44.9% when manganese concentration decreased by 1 ng/ml. on the other hand; the odd ratio of ADHD increased by 146.8% when lead concentration increased by 1 μg/dl, and by 58.6% when manganese concentration decreased by 1 ng/ml.
The Correlation Between the Measured Three Metals
Table 8 shows the correlation between the measured three metals. It shows that lead and manganese are positively correlated with each other. Zinc is negatively correlated with lead and manganese with no significance.
Discussion
Lead Levels in the Study Groups
This study found that lead levels were high in the groups of ASD, ADHD, and ASD-C but without any significant difference. After adjusting the age, lead levels were significantly increased in ASD group compared with control group in the age of 5 and less (P = 0.008). Our findings were consistent with previous studies that showed adverse neurodevelopmental and behavioral impacts of lead at low levels [18, 19].
It is well established that the adverse effects of lead are greater on the developing brain and that the CNS is more sensitive to low concentrations of toxic substances at early childhood period [27]. Children absorb 50% of lead by gastrointestinal route, five times more than adults who absorb only 10% [28, 29].
The vulnerability of both ASD and ADHD patients to be affected by low levels of lead may be due to individual differences and genetic variability which plays an important role in the natural ability to detoxification [30,31,32]. Several studies have shown that ASD and ADHD patients are poor detoxifiers, and they have low levels of the essential enzymes that are important for lead detoxification, where many studies showed that ASD children have lower levels of both GST and vitamin E compared with controls [30, 33, 34]. Ceylan et al. showed low effectiveness for GSH-Px in ADHD patients [35]. Several studies have also shown an elevation in oxidative stress biomarkers in both ASD and ADHD patients [35,36,37]. Rose et al. found that children with ASD have ALAD2 that correlates with lower glutathione, which may play an important role in their susceptibility to lead toxicity [38]. Lead lowers the levels of neurotransmitters, leading to detrimental effect on cognition and behavior [39]. Besides, lower neurotransmitter levels were found in each of ASD and ADHD compared with controls [40, 41].
In this study, the highest blood lead levels were observed in ASD-C group although there was no significant difference compared with control; this may be attributed to the small sample size. Many studies have shown that lead levels are well associated with the severity of ASD and ADHD. Adams et al. found a strong correlation between the levels of lead and the severity of autism (P < 0.0003) [9]. Blaurock-Busch et al. also found a significant positive correlation between lead and verbal communication (P = 0.02), plus general impression (P = 0.008) [42]. Moreover, Huang et al. found that each 1 μg/dl increase in blood lead is positively correlated with hyperactivity and restless-impulsivity and hyperactivity-impulsivity scores according to CRS-R scale [43].
Many studies have shown that the co-occurrence of ADHD and ASD is associated with lower quality of life, and lower performance and adaptation more than when each occurring alone [44]. Rao and Landa found in their study that the comorbidity of ADHD and ASD associates with increased social impairment severity, and lower cognitive functioning, and more retardation in adaptive functioning than in children with ASD only [45]. According to the previous findings, increase of the blood lead levels may be associated with the increased risk of the comorbidity of ADHD and ASD.
In this study, lead levels were significantly high in the males of control group and ASD group compared with females. Our finding corresponds with Joo et al. and Counter et al., studies where lead levels were higher in males [10, 46]. Jedrychowski et al. study showed that the adverse effects of lead on the cognition and behaviors of males were more than in females [47]. This may be attributed to estrogen role in regulating neurons in the brain, where males have less number of estrogen receptors, what makes them more susceptible to the adverse effects of lead [47].
Manganese Levels in the Groups of the Study
Manganese levels were significantly low in both of ASD and ADHD groups compared with controls, and they were also low in ASD-C group but without significance. Our study corresponded to Qin et al. study whereas manganese levels were significantly low in ASD patients compared with controls [11]. Ayadhi el al. also found that manganese levels were low in hair samples of ASD children [13]. Our findings did not correspond with several studies that showed increase in manganese levels in ASD and ADHD patients [16, 48], which may be attributed to the geographic difference for these studies, different levels of manganese in the drinking water. The circumstances of the Syrian crisis may also affect the nutrition of those children. Genetic difference such as polymorphisms in manganese transporters SLC30A10 and SLC39A8 may influence manganese homeostasis, and has a direct effect on manganese levels in blood [49]. Manganese is considered an essential and toxic metal which exhibits a biphasic dose-response relationship with neurological, cognitive, and behavioral outcomes [50]. Manganese affects neurotransmitter release, and stimulates faster and more effective electrical impulse movements throughout the brain, thus improving brain function [51].
Zinc Levels in the Groups of the Study
In this study, serum zinc levels were within the normal range of 70–120 μg/dl in all groups [52], and they were slightly higher in the groups of ASD, ADHD, and ASD-C groups with no significant value. Our study coincided with several previous studies that found no difference in serum zinc levels between ASD patients and controls [14, 53]. Our results did not correspond with studies that found low levels of zinc in the children with ASD and ADHD compared with controls [15, 54]. The difference between these values may be due to the geographical variation of these studies, and the different levels of zinc in soil, as well as, in diets. Zinc deficiency may have occurred either at the mother’s stage of pregnancy or at neonatal stage, where such cases have been found to result in brain damage [55,56,57].
The Correlation Between Measured Metals
In the present study, there is a positive correlation between lead and manganese. Our finding corresponds with Mehra and Thakur’s study which found a positive correlation between lead and manganese in hair samples of workers exposed to lead [58]. This may be due to the lead ability to affect essential elements in body and their bioavailability [59,60,61]. Manganese is a cofactor of SOD, and many studies showed that lead decreases SOD levels [62].
Conclusions
In conclusion, the obtained data showed that blood lead levels were higher in the groups of ASD-C, ASD, and ADHD-H compared with controls. Lead levels were significantly higher in children with ASD in the age of 5 or less compared with control, and they were also higher in the males of ASD comparing with females. Blood manganese levels were lower in the groups of ASD-C, ADHD, and ASD, and they were significantly lower in ADHD and ASD (P = 0.026, 0.046, respectively). However, serum zinc levels were within the reference range in all groups of study. Lead and manganese were positively correlated with each other. Lead elevation and manganese decrease may associate with the incidence of ASD, ADHD, or the co-occurrence of both of them together. Further studies are needed to examine the relationship between metal levels and the co-occurrence of ASD and ADHD together.
Strength of this Study
This is the first study of its kind in Syria, attempting to study the association between a toxic metal concentration, two essential metals levels, and the occurrence of ASD and ADHD in children born or grown during the Syrian crisis that started in 2011.
Limitation of the Study
Small sample size was a drawback in this study, but logistical and financial factors limited the ability to reach more autistic children.
References
American Psychiatric Association (2018). Autism spectrum disorder. Retrieved from https://www.psychiatry.org/patients-families/autism/what-is-autism-spectrum-disorder. Accessed Nov 2019
Centers for Disease Control and Prevention (2018). Autism spectrum disorder (ASD). Retrieved from https://www.cdc.gov/ncbddd/autism/facts.html. Accessed Dec 2019
American Psychiatric Association (2017). ADHD. Retrieved from https://www.psychiatry.org/patients-families/adhd/what-is-adhd. Accessed Nov 2019
Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G (2008) Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. J Am Acad Child Adolesc Psychiatry 47(8):921–929
Ramtekkar UP (2017) DSM-5 changes in attention deficit hyperactivity disorder and autism spectrum disorder: implications for comorbid sleep issues. Children 4(8):62
Thapar A, Cooper M, Rutter M (2017) Neurodevelopmental disorders. Lancet Psychiatry 4(4):339–346
Polańska K, Jurewicz J, Hanke W (2012) Exposure to environmental and lifestyle factors and attention-deficit/hyperactivity disorder in children—a review of epidemiological studies. Int J Occup Med Environ Health 25(4):330–355
Tarver J, Daley D, Sayal K (2014) Attention-deficit hyperactivity disorder (ADHD): an updated review of the essential facts. Child Care Health Dev 40(6):762–774
Qin YY, Jian B, Wu C, Jiang CZ, Kang Y, Zhou JX, Yang F, Liang Y (2018) A comparison of blood metal levels in autism spectrum disorder and unaffected children in Shenzhen of China and factors involved in bioaccumulation of metals. Environ Sci Pollut Res 25(18):17950–17956
Rahbar MH, Samms-Vaughan M, Dickerson AS, Loveland KA, Ardjomand-Hessabi M, Bressler J, Shakespeare-Pellington S, Grove ML, Pearson DA, Boerwinkle E (2014) Blood manganese concentrations in Jamaican children with and without autism spectrum disorders. Environ Health 13(1):69
Al-Ayadhi LY (2005) Heavy metals and trace elements in hair samples of autistic children in Central Saudi Arabia. Neurosciences (Riyadh, Saudi Arabia) 10(3):213–218
Adams JB, Audhya T, McDonough-Means S, Rubin RA, Quig D, Geis E et al (2013) Toxicological status of children with autism vs. neurotypical children and the association with autism severity. Biol Trace Elem Res 151(2):171–180
Joo H, Choi JH, Burm E, Park H, Hong YC, Kim Y, Ha EH, Kim Y, Kim BN, Ha M (2018) Gender difference in the effects of lead exposure at different time windows on neurobehavioral development in 5-year-old children. Sci Total Environ 615:1086–1092
Li W, Han S, Gregg TR, Kemp FW, Davidow AL, Louria DB, Siegel A, Bogden JD (2003) Lead exposure potentiates predatory attack behavior in the cat. Environ Res 92(3):197–206
Elbaz F, Zahra S, Hanafy H (2017) Magnesium, zinc and copper estimation in children with attention deficit hyperactivity disorder (ADHD). Egyptian J Med Human Genet 18(2):153–163
Yousef S, Adem A, Zoubeidi T, Kosanovic M, Mabrouk AA, Eapen V (2011) Attention deficit hyperactivity disorder and environmental toxic metal exposure in the United Arab Emirates. J Trop Pediatr 57(6):457–460
ATSDR, U (2007). Toxicological profile for lead. US Department of Health and Human Services, 1, 1–2
Lanphear BP, Hornung R, Khoury J, Yolton K, Baghurst P, Bellinger DC et al (2005) Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Perspect 113(7):894–899
Ha M, Kwon HJ, Lim MH, Jee YK, Hong YC, Leem JH, Sakong J, Bae JM, Hong SJ, Roh YM, Jo SJ (2009) Low blood levels of lead and mercury and symptoms of attention deficit hyperactivity in children: a report of the children’s health and environment research (CHEER). Neurotoxicology 30(1):31–36
Carbone R, Laforgia N, Crollo E, Mautone A, Iolascon A (1998) Maternal and neonatal lead exposure in southern Italy. Neonatology 73(6):362–366
DRI (2005). Institute of Medicine, Food and Nutrition Board, Dietary Reference Intakes: energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids
Black MM (1998) Zinc deficiency and child development. Am J Clin Nutr 68(2):464S–469S
Pan E, Zhang XA, Huang Z, Krezel A, Zhao M, Tinberg CE, Lippard SJ, McNamara JO (2011) Vesicular zinc promotes presynaptic and inhibits postsynaptic long-term potentiation of mossy fiber-CA3 synapse. Neuron 71(6):1116–1126
Bao B, Ahmad A, Azmi A, Li Y, Prasad A, Sarkar FH (2014) The biological significance of zinc in inflammation and aging. In: Inflammation, advancing age and nutrition. Academic Press, pp 15–27
Pfeiffer CC, Braverman ER (1982) Zinc, the brain and behavior. Biol Psychiatry
Gok, S., Kazanci, F. H., Erdamar, H., Gokgoz, N., Hartiningsih, S., & Dane, S. (2016). Is it possible to remove heavy metals from the body by wet cupping therapy (Al-hijamah)?
Grandjean P, Landrigan PJ (2006) Developmental neurotoxicity of industrial chemicals. Lancet 368(9553):2167–2178
Alexander FW, CLAYTON BE, Delves HT (1974) Mineral and trace-metal balances in children receiving normal and synthetic diets. Int J Med 43(1):89–111
Ziegler EE, Edwards BB, Jensen RL, Mahaffey KR, Fomon SJ (1978) Absorption and retention of lead by infants. Pediatr Res 12(1):29–34
Alabdali A, Al-Ayadhi L, El-Ansary A (2014) A key role for an impaired detoxification mechanism in the etiology and severity of autism spectrum disorders. Behav Brain Funct 10(1):14
Koch L (2013) Cancer: polymorphisms in detoxification genes increase HMTC risk and match tumour phenotype. Nat Rev Endocrinol 9(3):128
McFadden SA (1996) Phenotypic variation in xenobiotic metabolism and adverse environmental response: focus on sulfur-dependent detoxification pathways. Toxicology 111(1–3):43–65
Al-Yafee YA, Al-Ayadhi LY, Haq SH, El-Ansary AK (2011) Novel metabolic biomarkers related to sulfur-dependent detoxification pathways in autistic patients of Saudi Arabia. BMC Neurol 11(1):139
Ceylan M, Sener S, Bayraktar AC, Kavutcu M (2010) Oxidative imbalance in child and adolescent patients with attention-deficit/hyperactivity disorder. Prog Neuro-Psychopharmacol Biol Psychiatry 34(8):1491–1494
Hyman, M. (2004, September). The impact of mercury on human health and the environment. In Tulane University School of Public Health and Tropical Medicine. General Meeting. Tulane University, New Orleans (Vol. 23)
Söğüt S, Zoroğlu SS, Özyurt H, Yılmaz HR, Özuğurlu F, Sivaslı E et al (2003) Changes in nitric oxide levels and antioxidant enzyme activities may have a role in the pathophysiological mechanisms involved in autism. Clin Chim Acta 331(1–2):111–117
Chauhan A, Chauhan V, Brown WT, Cohen I (2004) Oxidative stress in autism: increased lipid peroxidation and reduced serum levels of ceruloplasmin and transferrin-the antioxidant proteins. Life Sci 75(21):2539–2549
Rose S, Melnyk S, Savenka A, Hubanks A, Jernigan S, Cleves M, James SJ (2008) The frequency of polymorphisms affecting lead and mercury toxicity among children with autism. Am J Biochem Biotechnol 4(2):85–94
Finkelstein Y, Markowitz ME, Rosen JF (1998) Low-level lead-induced neurotoxicity in children: an update on central nervous system effects. Brain Res Rev 27(2):168–176
El-Ansary AK, Bacha AB, Al-Ayahdi LY (2011) Relationship between chronic lead toxicity and plasma neurotransmitters in autistic patients from Saudi Arabia. Clin Biochem 44(13):1116–1120
Bellgrove MA, Hawi Z, Lowe N, Kirley A, Robertson IH, Gill M (2005) DRD4 gene variants and sustained attention in attention deficit hyperactivity disorder (ADHD): effects of associated alleles at the VNTR and− 521 SNP. Am J Med Genet B Neuropsychiatr Genet 136(1):81–86
Blaurock-Busch E, Amin OR, Rabah T (2011) Heavy metals and trace elements in hair and urine of a sample of Arab children with autistic spectrum disorder. Maedica 6(4):247–257
Huang S, Hu H, Sánchez BN, Peterson KE, Ettinger AS, Lamadrid-Figueroa H et al (2015) Childhood blood lead levels and symptoms of attention deficit hyperactivity disorder (ADHD): a cross-sectional study of Mexican children. Environ Health Perspect 124(6):868–874
Vora, P., & Sikora, D. (2011). Society for developmental and behavioral pediatrics. San Antonio
Rao PA, Landa RJ (2014) Association between severity of behavioral phenotype and comorbid attention deficit hyperactivity disorder symptoms in children with autism spectrum disorders. Autism 18(3):272–280
Counter SA, Buchanan LH, Ortega F (2001) Gender differences in blood lead and hemoglobin levels in Andean adults with chronic lead exposure. Int J Occup Environ Health 7(2):113–118
Jedrychowski W, Perera F, Jankowski J, Mrozek-Budzyn D, Mroz E, Flak E, Edwards S, Skarupa A, Lisowska-Miszczyk I (2009) Gender specific differences in neurodevelopmental effects of prenatal exposure to very low-lead levels: the prospective cohort study in three-year olds. Early Hum Dev 85(8):503–510
Sanders AP, Henn BC, Wright RO (2015) Perinatal and childhood exposure to cadmium, manganese, and metal mixtures and effects on cognition and behavior: a review of recent literature. Curr Environ Health Rep 2(3):284–294
Wahlberg KE, Guazzetti S, Pineda D, Larsson SC, Fedrighi C, Cagna G et al (2018) Polymorphisms in manganese transporters SLC30A10 and SLC39A8 are associated with children’s neurodevelopment by influencing manganese homeostasis. Front Genet 9:664
Vollet K, Haynes EN, Dietrich KN (2016) Manganese exposure and cognition across the lifespan: contemporary review and argument for biphasic dose–response health effects. Curr Environ Health Rep 3(4):392–404
Takeda A (2003) Manganese action in brain function. Brain Res Rev 41(1):79–87
Smith JC, Butrimovitz GP, Purdy WC (1979) Direct measurement of zinc in plasma by atomic absorption spectroscopy. Clin Chem 25(8):1487–1491
Adams JB, Romdalvik J, Ramanujam VS, Legator MS (2007) Mercury, lead, and zinc in baby teeth of children with autism versus controls. J Toxic Environ Health A 70(12):1046–1051
Arora M, Reichenberg A, Willfors C, Austin C, Gennings C, Berggren S, Lichtenstein P, Anckarsäter H, Tammimies K, Bölte S (2017) Fetal and postnatal metal dysregulation in autism. Nat Commun 8:15493
Hurley LS, Swenert’on H (1966) Congenital malformations resulting from zinc deficiency in rats. Proc Soc Exp Biol Med 123(3):692–696
Caldwell DF, Oberleas D, Clancy JJ, Prasad AS (1970) Behavioral impairment in adult rats following acute zinc deficiency. Proc Soc Exp Biol Med 133(4):1417–1421
Yasuda H, Yoshida K, Yasuda Y, Tsutsui T (2011) Infantile zinc deficiency: association with autism spectrum disorders. Sci Rep 1:129
Mehra R, Thakur AS (2016) Relationship between lead, cadmium, zinc, manganese and iron in hair of environmentally exposed subjects. Arab J Chem 9:S1214–S1217
Pizent A, Jurasović J, Telišman S (2003) Serum calcium, zinc, and copper in relation to biomarkers of lead and cadmium in men. J Trace Elem Med Biol 17(3):199–205
Al-Nasser IA, Hashem AR Lead, zinc and copper concentrations in hair. Nails Blood
Godwin HA (2001) The biological chemistry of lead. Curr Opin Chem Biol 5(2):223–227
Flora G, Gupta D, Tiwari A (2012) Toxicity of lead: a review with recent updates. Interdiscip Toxicol 5(2):47–58
Funding
The study was partially funded by the University of Damascus University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Research Involving Human Participants and/or AnimalsStatement of Human Rights
The protocol of the investigation was approved by the Ethics Committee at Damascus University. Moreover, informed consent was obtained from the parents of the examined children before inclusion into the study, and blood sampling was performed in the presence of parents.
Informed Constant
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hawari, I., Eskandar, M.B. & Alzeer, S. The Role of Lead, Manganese, and Zinc in Autism Spectrum Disorders (ASDs) and Attention-Deficient Hyperactivity Disorder (ADHD): a Case-Control Study on Syrian Children Affected by the Syrian Crisis. Biol Trace Elem Res 197, 107–114 (2020). https://doi.org/10.1007/s12011-020-02146-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-020-02146-3