
Abstract
The aim of this study was to investigate the relationship of blood lead (Pb) levels with copper (Cu), zinc (Zn), calcium (Ca), magnesium (Mg), iron (Fe), and hemoglobin (Hb) in children aged from 0–6 years in Wuhan, China. A total of 1047 children from six communities, which were randomly selected in Wuhan city and three communities, located in the urban area and others in the suburban area, were recruited for this study between November 2012 and July 2013. The levels of elements in the blood were detected using an atomic absorption spectrometer, and Hb level was tested by an automated hematology analyzer. The results showed that the mean blood lead level (BLL) is 33.72 ± 19.03 μg/L. The BLL was significantly higher among boys than girls (P < 0.05). Higher BLL was also observed in suburbs compared to that in urban areas (P < 0.05). The BLL and Zn level were gradually increased with age. The elevated rate of BLL in children was 20.9 %, while the Zn deficiency rate was 65.0 %. And, the level of Hb in higher BLL group was significantly lower. Negative correlations of the blood levels of Pb with those of Cu (r = −0.087, P = 0.005), Mg (r = −0.102, P = 0.001), and Fe (r = −0.091, P = 0.003) were observed. These data suggested that the elevated rate of BLL in children from Wuhan is still higher according to the updated reference values in the USA. The deficiency of Cu, Mg, and Fe may indicate the elevation of lead absorption. The dietary supplement of Zn, Ca, and Fe in children requires more attention.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Lead, as a metal element, is found ubiquitously in the environment, and its adverse effect on human health is an important global environmental problem [1, 2]. Floating in the air or attaching to objects, Pb can be absorbed into the human body through the respiratory tract, gastrointestinal tract, or skin. Exposure to high level of lead could harm nearly every system in the body, such as gastrointestinal, hematopoietic, cardiovascular, immune, reproductive, excretory system [3–7], and particularly the nervous system, which is the most sensitive target [8, 9]. Children are more vulnerable than adults to lead exposure because of the growth and development of their neurological and behavioral characteristics [9–11]. Even low levels of lead exposure are associated with impairment of childhood cognitive function and abnormal infant behaviors [12, 13]. Childhood with elevated blood lead levels (BLLs) may result in behavioral disturbances, learning, and concentration difficulties [14].
Essential elements like Cu, Zn, Ca, Mg, and Fe play important roles in the regulation and maintenance of various physiological functions in the human body despite low requirements of them [15]. These elements are key components of metalloenzymes, and they are involved in crucial biological functions, such as oxygen transport, free radical scavenging, and hormonal activity [16]. Their blood levels are often considered as an important modifier of the metabolism and toxicity of heavy metals such as lead [17]. Previous study showed that low dietary intakes of Fe, Zn, Cu, and Ca in children have been associated with increased BLLs [18], but the correlation between BLLs and essential elements is not well understood. Besides, lead exposure has an influence on the hematological system. Decreasing trend of the hemoglobin level has been found with increasing BLLs in children [19, 20].
In this study, we evaluated the concentrations of Pb, Cu, Zn, Ca, Mg, Fe, and Hb in the blood of children aged 0∼6 years from Wuhan, China. The aim was to analyze the blood level of these elements and hemoglobin in different genders, residential areas, and age groups and to investigate the relationship of BLLs with Cu, Zn, Ca, Mg, Fe, and Hb in those children.
Materials and Methods
Study Population
Six communities (an administrative region delimited by the government of Wuhan city) in this study were randomly selected in Wuhan city. Three communities were located in the urban area, and others were in the suburban area. Children aged 0–6 years in these communities were recruited for this study between November 2012 and July 2013. The study population consisted of 1047 children (602 boys and 445 girls; 654 from the urban area and 393 from the suburban area). Subjects were divided into five age groups: 0-year-old group, N = 455; 1-year-old group, N = 214; 2-year-old group, N = 122; 3-year-old group, N = 104; and 4∼6-year-old group, N = 162.
The procedures of the study were explained to all the participants and their parents before informed consent were signed. The experimental protocol was reviewed and approved by the Medical Ethics Committee of School of Medicine, Wuhan University.
Sample Collection and Analysis
Blood samples were collected in the Community Health Center and then analyzed in the lab of Renmin Hospital at Wuhan University. One venous blood sample was collected in a vacuum tube (BD, USA) containing EDTA-K2 for hemoglobin detection. Hemoglobin concentrations were determined immediately using an automated hematology analyzer (ADVIA™ 120, Bayer, USA) according to the reference method for hemoglobinometry in human blood by the National Health and Family Planning Commission of the People’s Republic of China in 2011.
Another fasting venous blood sample was collected into a lead-free vacuum tube (BD, USA) containing heparin sodium for element detection. Then, 80 μL of whole blood sample was added to the special tube with 5 % HNO3 and immediately vortexed before storage at 0–4 °C until further analysis. The analysis of all samples was conducted in the same laboratory. Precaution was taken to avoid contamination. Tubes and glassware were soaked in 10 % nitric acid solution for 24 h and rinsed five to six times with ultra-pure double-distilled deionized water. As part of contamination control, all reagents, glassware, and sample collection devices were checked for contamination with selected elements. The whole blood levels of Pb were detected using graphite furnace atomic absorption spectrometer (283.3 nm) equipped with tungsten atomizer (BH2100, Bohui, China). The concentrations of Cu, Zn, Ca, Mg, and Fe were measured by flame atomic absorption spectrometer (BH5100, Bohui, China) using hollow cathode lamps (324.7, 213.9, 422.7, 285.2, and 248.3 nm for Cu, Zn, Ca, Mg, and Fe, respectively). Each sample was analyzed in duplicate, and the mean of both measurements was used as the final value.
Quality controls were ensured by analyzing reference materials provided by General Administration of Quality, Inspection and Quarantine of the People’s Republic of China (GBW(E) 090033, 090034, 090035, and 090036 for lead and GBW(E) 080915, 080916, and 080917 for Cu, Zn, Ca, Mg, and Fe). Reference samples were analyzed before and after ten routine sample measurements. The values of these reference samples were in agreement with the provided ranges.
Elevated BLL was defined as higher than 50 μg/L according to the recommendation of the US CDC Advisory Committee on Childhood Lead Poisoning Prevention [21]. Other reference values of whole blood used in this lab were as follows: Cu 0.75–2.50 mg/L; Ca 62–84 mg/L; Mg 27.2–50.1 mg/L; Fe 420–660 mg/L; Zn 3.79–6.54 mg/L (0∼1 year), 4.05–7.19 mg/L (1∼2 years), 4.32–7.85 mg/L (2∼3 years), 4.71–8.50 mg/L (3∼4 years), and 5.00–11.12 mg/L (4∼13 years); and Hb 11–16 g/dL.
Statistical Analysis
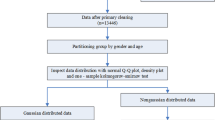
Data are expressed as mean ± SD (standard deviation). As to the normally distributed data, such as the concentrations of Cu, Zn, Ca, Mg, Fe, and Hb, Student’s t test was used to compare the difference of the two groups. And, differences of means in multiple groups were compared using one-way ANOVA, followed by LSD test for multiple pairwise comparisons. While as non-Gaussian distributed data, the difference in BLLs was assessed by nonparametric tests. Chi-square tests were used to examine the discrepancy and the trend of different group rates. Partial correlation tests were used to demonstrate the relationships of BLLs with Cu, Zn, Ca, Mg, Fe, and Hb in children. A P < 0.05 was considered statistically significant. The statistical analyses were conducted using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA).
Results
Concentration of Metal Elements and Hemoglobin in the Blood
The descriptive data including arithmetic mean, standard deviation, range, geometric mean, median, percentiles 25 and 75 of all elements, and hemoglobin in whole blood of all the participants are summarized in Table 1. BLLs of the children ranged from 4.72 to 96.49 μg/L, the mean value was 33.72 ± 19.03 μg/L, and the median of BLLs was 33.98 μg/L. No child had BLL ≥100 μg/L.
Table 2 presents the comparisons of the whole blood levels of Pb, Cu, Zn, Ca, Mg, Fe, and Hb in different age groups. The BLLs of children in 0- and 1-year-old groups were lower than those of the other three groups (P < 0.05). The blood concentrations of Pb and Zn both had a tendency to increase with the age groups. In addition, the blood concentrations of Cu, Ca, Mg, Fe, and Hb in different age groups were also significantly different.
The rates of elevated BLL and deficiencies of Cu, Zn, Ca, Mg, Fe, and Hb in different age groups are shown in Table 3. The elevated BLL rate of all the children is 20.9 %, and the highest rate was 38.3 % of the 4∼6-year-old children. Few children were found to have Cu and Mg deficiency. On the other hand, the deficiencies of Zn, Ca, Fe, and Hb were common. In general, 65.0 % of the children were Zn-deficient. The deficiency rates of Ca, Fe, and Hb were 23.4, 28.9, and 7.2 %, respectively. Chi-square test results revealed that the elevated BLL rates increased with age for children aged 0–6 years old in Wuhan, and the deficiency rates of Zn, Ca, Fe, and Hb were also significantly different (P < 0.001).
Effect of Gender and Residential Area on the Blood Level of Elements and Hemoglobin
Tables 4 and 5 show the blood levels of Pb, Cu, Zn, Ca, Mg, Fe, and Hb by gender and residential area. The BLLs of boys were significantly higher than those of girls (34.12 ± 18.20 vs. 31.18 ± 20.10 μg/L, P < 0.05). Similar results were found in Fe (457.97 ± 68.70 vs. 450.15 ± 59.20 mg/L) and Hb (12.90 ± 1.52 vs. 12.63 ± 1.60 g/dL) (P < 0.05, P < 0.01, respectively). However, the blood levels of Cu and Zn in boys were slightly lower than those in girls (Cu, 1.14 ± 0.27 vs. 1.18 ± 0.33 mg/L; Zn, 3.81 ± 1.09 vs. 4.05 ± 1.08 mg/L) (P < 0.05, P < 0.01, respectively). No gender differences were found in other elements. On the other hand, lower BLLs were found in the children from the urban group than the suburban group (30.73 ± 18.06 vs. 33.38 ± 18.00 μg/L, P < 0.05). The blood concentrations of Cu in the children from urban area were higher than suburban area (1.19 ± 0.31 vs. 1.10 ± 0.27 mg/L) (P < 0.01), whereas the blood levels of Mg, Fe, and Hb (Mg, 37.42 ± 4.37 vs. 38.15 ± 4.37 mg/L; Fe, 451.27 ± 0.32 vs. 460.76 ± 70.93 mg/L; Hb, 12.67 ± 1.30 vs. 12.98 ± 1.90 g/dL) of the urban children were significantly lower (P < 0.01, P < 0.05, P < 0.01, respectively).
Correlation Analysis
In order to analyze the effect of Pb on essential elements, we defined the BLL ≥50 μg/L as a cut-off value. All the children were divided into two different groups according the BLLs. Table 6 shows the mean values of other elements and Hb concentration of these two groups. The blood zinc levels of children in the BLLs <50 μg/L group were significantly lower compared to children from BLLs ≥50 μg/L group (3.87 ± 1.10 vs. 4.07 ± 1.05 mg/L, P < 0.05). On the other hand, the concentrations of Fe and Hb in BLLs <50 μg/L group were significantly higher than those values in the BLLs ≥50 μg/L group (Fe, 458.53 ± 61.44 vs. 441.22 ± 74.28 mg/L; Hb, 12.87 ± 1.57 vs. 12.47 ± 1.48 g/dL; both P < 0.01).
After controlling for age, gender, and residential area, partial correlation analysis showed that BLLs were inversely correlated with the blood levels of Cu (r = −0.087, P = 0.005) as shown in Table 7. Negative correlations were also found between the blood concentrations of Pb and Mg (r = −0.102, P = 0.001) and Pb and Fe (r = −0.091, P = 0.003).
Discussion
Lead exposure is a child health concern around the world, especially in developing countries [22]. The adverse effects of lead on human health are well known, especially for children under 6 years of age [23]. According to the report in 2005 [24], the mean BLL of children aged 0–6 years in Wuhan was 67.39 μg/L, while the study in 2011 [25] showed a value of 54.54 μg/L (sample collected between 2004 and 2008). In our study, the mean BLL for Wuhan children was 33.72 μg/L, which revealed the progressive decline of BLLs in children from Wuhan city. This would be most likely due to the change of using unleaded gasoline and reductions of industrial lead pollution.
As shown in Table 2, the BLL trends to increase with the age groups. The trend was consistent with other studies [26, 27]. The elevated BLL rates were also increased by age (Table 3), and the highest BLL rate was 38.3 % in 4–6-year-age group. This can be explained by the following reason: lead exposure of children in China may come primarily from outdoor sources rather than from indoor ones [28], and elder children were more likely to play outdoor, so the chances of lead exposure for them were much higher.
The higher BLLs among boys might be explained by the differences in behavior related to lead exposure. Compared with girls, boys spend more time on outdoor activities and have more hand-to-mouth and object-to-mouth activities, which have been associated with higher BLLs [29]. It could be proposed that boys may have higher absorption rates by eating more or drinking more. We also noticed that children in suburban areas had higher BLLs than those in urban areas (Table 5), which was consistent with the investigation in Taiyuan City [30]. This may be because of lead-acid battery plant migration to the suburbs to improve urban air quality in recent years.
Our study revealed that although the blood levels of Zn were increased with the age groups, the total deficiency rate of Zn was 65.0 %, which suggests that the Zn deficiency problem of children in Wuhan was quite serious. The essential trace element Zn plays a vital role in some biological functions including cellular division, protein synthesis, and nucleic metabolism [31, 32]. More efforts should be made in order to popularize the adverse outcomes of Zn deficiency in childhood health education. The deficiency of Ca, Fe, and Hb was also common in Wuhan children while few have the Cu and Mg deficiency. These results were consistent with previous reports [33, 34]. So, the dietary supplement of Zn, Ca, and Fe in the children requires more attention.
In the present study, the blood levels of Zn in the BLLs <50 μg/L group were significantly lower compared to the BLLs ≥50 μg/L group (P < 0.05). While partial correlation analysis results showed that no significant correlation was found between the blood levels of Pb and Zn, which was in consistent with the investigation conducted in Chengdu city [35]. Since the blood levels of Zn were positively correlated with age, a possible explanation for this discrepancy is the different age structures of the two groups.
Our study had revealed the negative correlations between the blood levels of Pb with Cu, Mg, and Fe (Table 7). In the report of Patra [36], a negative correlation between the blood levels of Pb and Cu was found, which were consistent with the present study. However, some studies demonstrated that BLLs were not significantly correlated with blood copper levels [17, 37]. As an essential element in the function of enzymes and manipulating important biological polyphosphate compounds, Mg in blood was significantly decreased in the occupational lead exposure workers [38]. The negative correlation of blood Pb and Mg in our research was also in accordance with the previous study [37].
In addition, iron deficiency was confirmed to be associated with subsequent lead poisoning based on the longitudinal study by Wright and his colleagues [39]. In a cross-sectional study, BLLs were found to be negatively correlated with blood iron levels [40]. Furthermore, recent study revealed that the BLLs of iron-deficient infants decreased significantly compared with pretreatment levels after iron therapy [41]. The results summarized in Tables 6 and 7 were in agreement with the above studies, which indicated that the blood Fe levels decrease as the BLLs rise.
Lead poisoning was a known cause of microcytic anemia [42] by impairment of heme synthesis and increased rate of red blood cell destruction. Animal research and human investigation both showed that hemoglobin concentration decreased significantly with rising blood lead concentration [43, 44]. Similar result was found in this study; the hemoglobin concentration of children with higher BLLs was significantly lower than that of the children with lower BLLs (Table 6). However, the negative correlation has no significance. This may be that the level of Hb was also affected by other factors, such as the level of Fe, Zn, and so on.
In conclusion, although the BLLs of children have declined, high lead level in children from Wuhan childhood remains a public health issue, with the overall elevated BLL rate according to the new standard [21] of 20.9 %. Meanwhile, the deficiency of and need for the supplementation of Zn, Ca, and Fe had been recognized. We also found that the BLLs were influenced by the status of certain essential trace elements in children. The appropriate volume supplements of Cu, Mg, and Fe in diet were a protective factor contributing to reduce the risk of lead exposure in children.
References
Cobanoglu U, Demir H, Sayir F, Duran M, Mergan D (2010) Some mineral, trace element and heavy metal concentrations in lung cancer. Asian Pac J Cancer Prev 11(5):1383–1388
Renzi M, Perra G, Guerranti C, Mariottini M, Baroni D, Volterrani M, Graziosi M, Specchiulli A, Focardi S (2009) Assessment of environmental pollutants in ten southern Italy harbor sediments. Toxicol Ind Health 25(4–5):351–363. doi:10.1177/0748233709104868
Staessen J, Yeoman WB, Fletcher AE, Markowe HL, Marmot MG, Rose G, Semmence A, Shipley MJ, Bulpitt CJ (1990) Blood lead concentration, renal function, and blood pressure in London civil servants. Br J Ind Med 47(7):442–447. doi:10.1136/oem.47.7.442
Al-Neamy FR, Almehdi AM, Alwash R, Pasha MA, Ibrahim A, Bener A (2001) Occupational lead exposure and amino acid profiles and liver function tests in industrial workers. Int J Environ Health Res 11(2):181–188. doi:10.1080/09603120020047564
Herman DS, Geraldine M, Venkatesh T (2007) Evaluation, diagnosis, and treatment of lead poisoning in a patient with occupational lead exposure: a case presentation. J Occup Med Toxicol 2:7. doi:10.1186/1745-6673-2-7
Bonde JP, Joffe M, Apostoli P, Dale A, Kiss P, Spano M, Caruso F, Giwercman A, Bisanti L, Porru S, Vanhoorne M, Comhaire F, Zschiesche W (2002) Sperm count and chromatin structure in men exposed to inorganic lead: lowest adverse effect levels. Occup Environ Med 59(4):234–242. doi:10.1136/Oem.59.4.234
Martin D, Glass TA, Bandeen-Roche K, Todd AC, Shi W, Schwartz BS (2006) Association of blood lead and tibia lead with blood pressure and hypertension in a community sample of older adults. Am J Epidemiol 163(5):467–478. doi:10.1093/aje/kwj060
Chiodo LM, Jacobson SW, Jacobson JL (2004) Neurodevelopmental effects of postnatal lead exposure at very low levels. Neurotoxicol Teratol 26(3):359–371. doi:10.1016/j.ntt.2004.01.010
Khan DA, Qayyum S, Saleem S, Ansari WM, Khan FA (2010) Lead exposure and its adverse health effects among occupational worker’s children. Toxicol Ind Health 26(8):497–504. doi:10.1177/0748233710373085
Rohlman DS, Anger WK, Tamulinas A, Phillips J, Bailey SR, McCauley L (2001) Development of a neurobehavioral battery for children exposed to neurotoxic chemicals. Neurotoxicology 22(5):657–665. doi:10.1016/S0161-813x(01)00049-3
Absalon D, Slesak B (2010) The effects of changes in cadmium and lead air pollution on cancer incidence in children. Sci Total Environ 408(20):4420–4428. doi:10.1016/j.scitotenv.2010.06.030
Canfield RL, Henderson CR Jr, Cory-Slechta DA, Cox C, Jusko TA, Lanphear BP (2003) Intellectual impairment in children with blood lead concentrations below 10 μg per deciliter. N Engl J Med 348(16):1517–1526. doi:10.1056/NEJMoa022848
Mendelsohn AL, Dreyer BP, Fierman AH, Rosen CM, Legano LA, Kruger HA, Lim SW, Barasch S, Au L, Courtlandt CD (1999) Low-level lead exposure and cognitive development in early childhood. J Dev Behav Pediatr 20(6):425–431. doi:10.1097/00004703-199912000-00004
Jarup L (2003) Hazards of heavy metal contamination. Br Med Bull 68:167–182. doi:10.1093/Bmb/Ldg032
Stathopoulou MG, Kanoni S, Papanikolaou G, Antonopoulou S, Nomikos T, Dedoussis G (2012) Mineral intake. Prog Mol Biol Transl Sci 108:201–236. doi:10.1016/B978-0-12-398397-8.00009-5
Parsons PJ, Barbosa F Jr (2007) Atomic spectrometry and trends in clinical laboratory medicine. Spectrochim Acta Atom Spectrosc 62(9):992–1003. doi:10.1016/j.sab.2007.03.007
Ahamed M, Singh S, Behari JR, Kumar A, Siddiqui MK (2007) Interaction of lead with some essential trace metals in the blood of anemic children from Lucknow, India. Clin Chim Acta 377(1–2):92–97. doi:10.1016/j.cca.2006.08.032
Mahaffey KR (1990) Environmental lead toxicity: nutrition as a component of intervention. Environ Health Perspect 89:75–78. doi:10.2307/3430900
Bergdahl IA, Vahter M, Counter SA, Schutz A, Buchanan LH, Ortega F, Laurell G, Skerfving S (1999) Lead in plasma and whole blood from lead-exposed children. Environ Res 80(1):25–33. doi:10.1006/enrs.1998.3880
Tripathi RM, Raghunath R, Mahapatra S, Sadasivan S (2001) Blood lead and its effect on Cd, Cu, Zn, Fe and hemoglobin levels of children. Sci Total Environ 277(1–3):161–168. doi:10.1016/S0048-9697(00)00871-8
Laidlaw MA, Zahran S, Pingitore N, Clague J, Devlin G, Taylor MP (2014) Identification of lead sources in residential environments: Sydney Australia. Environ Pollut 184:238–246. doi:10.1016/j.envpol.2013.09.003
Liu JH, Ai YX, McCauley L, Pinto-Martin J, Yan CH, Shen XM, Needleman H (2012) Blood lead levels and associated sociodemographic factors among preschool children in the South Eastern region of China. Paediatr Perinat Epidemiol 26(1):61–69. doi:10.1111/j.1365-3016.2011.01234.x
Lidsky TI, Schneider JS (2003) Lead neurotoxicity in children: basic mechanisms and clinical correlates. Brain 126:5–19. doi:10.1093/Brain/Awg014
Zhang SM, Dai YH, Xie XH, Fan ZY, Tan ZW (2005) Study on blood lead level and related risk factors among children aged 0–6 years in 15 cities in China. Chin J Epidemiol 26(9):651–654, in Chinese
Tan ZW, Dai YH, Xie XH, Zhang SM, Fan ZY, Jia N (2011) Blood lead status and influencing factors among preschool children in urban areas of China. Chin J Pediatr 49(4):294–300, in Chinese
Wang S, Zhang J (2006) Blood lead levels in children, China. Environ Res 101(3):412–418. doi:10.1016/j.envres.2005.11.007
Zhang SM, Dai YH, Xie XH, Fan ZY, Tan ZW, Zhang YF (2009) Surveillance of childhood blood lead levels in 14 cities of China in 2004–2006. Biomed Environ Sci 22(4):288–296. doi:10.1016/S0895-3988(09)60058-1
Xie XH, Tan ZW, Jia N, Fan ZY, Zhang SM, Lu YY, Chen L, Dai YH, Xie XH, Tan ZW, Jia N, Fan ZY, Zhang SM, Lu YY, Chen L, Dai YH (2013) Blood lead levels among children aged 0 to 6 years in 16 cities of China, 2004–2008. Chin Med J Peking 126(12):2291–2295
Ko S, Schaefer PD, Vicario CM, Binns HJ (2007) Relationships of video assessments of touching and mouthing behaviors during outdoor play in urban residential yards to parental perceptions of child behaviors and blood lead levels. J Expo Sci Environ Epidemiol 17(1):47–57. doi:10.1038/sj.jes.7500519
Li BH (2005) Blood Pb contents of children living in Taiyuan city. J Shanxi Med Uni 36(02):184–186. doi:10.3969/j.issn.1007-6611.2005.02.019 (in Chinese)
Sazawal S, Black RE, Menon VP, Dinghra P, Caulfield LE, Dhingra U, Bagati A (2001) Zinc supplementation in infants born small for gestational age reduces mortality: a prospective, randomized, controlled trial. Pediatrics 108(6):1280–1286
Kosar F, Sahin I, Acikgoz N, Aksoy Y, Kucukbay Z, Cehreli S (2005) Significance of serum trace element status in patients with rheumatic heart disease—a prospective study. Biol Trace Elem Res 107(1):1–9. doi:10.1385/Bter:107:1:001
Chen X, Fan YH, Di JX (2009) Retrospective survey of trace element levels of 0–6 years old children. Contemp Med. doi:10.3969/j.issn.1009-4393.2009.36.132. (in Chinese)
Li GT, Lu F, Xu HF (2012) The analysis of trace elements in blood of infants in Wuhan. Chin J Birth Health Heredit 20(12):124. (in Chinese)
Wang H, Shi H, Chang L, Zhang X, Li J, Yang Y, Jiang Y (2012) Association of blood lead with calcium, iron, zinc and hemoglobin in children aged 0–7 years: a large population-based study. Biol Trace Elem Res 149(2):143–147. doi:10.1007/s12011-012-9413-x
Patra RC, Swarup D, Sharma MC, Naresh R (2006) Trace mineral profile in blood and hair from cattle environmentally exposed to lead and cadmium around different industrial units. J Vet Med A Physiol Pathol Clin Med 53(10):511–517. doi:10.1111/j.1439-0442.2006.00868.x
Wu Y, Yang X, Ge J, Zhang J (2011) Blood lead level and its relationship to certain essential elements in the children aged 0 to 14 years from Beijing, China. Sci Total Environ 409(16):3016–3020. doi:10.1016/j.scitotenv.2011.04.050
Anetor JI, Ajose OA, Adebiyi JA, Akingbola TS, Iyanda AA, Ebesunu MO, Babalola OO, Aadeniyi FA (2007) Decreased thiamine and magnesium levels in the potentiation of the neurotoxicity of lead in occupational lead exposure. Biol Trace Elem Res 116(1):43–51. doi:10.1007/BF02685917
Wright RO, Tsaih SW, Schwartz J, Wright RJ, Hu H (2003) Association between iron deficiency and blood lead level in a longitudinal analysis of children followed in an urban primary care clinic. J Pediatr 142(1):9–14. doi:10.1067/mpd.2003.mpd0344
Shah F, Kazi TG, Afridi HI, Baig JA, Khan S, Kolachi NF, Wadhwa SK, Shah AQ (2010) Environmental exposure of lead and iron deficit anemia in children age ranged 1–5 years: a cross sectional study. Sci Total Environ 408(22):5325–5330. doi:10.1016/j.scitotenv.2010.07.091
Park S, Sim CS, Lee H, Kim Y (2014) Effects of iron therapy on blood lead concentrations in infants. J Trace Elem Med Biol 28(1):56–59. doi:10.1016/j.jtemb.2013.11.003
Staudinger KC, Roth VS (1998) Occupational lead poisoning. Am Fam Physician 57(4):719–726
Katavolos P, Staempfli S, Sears W, Gancz AY, Smith DA, Bienzle D (2007) The effect of lead poisoning on hematologic and biochemical values in trumpeter swans and Canada geese. Vet Clin Pathol 36(4):341–347
Yilmaz H, Keten A, Karacaoglu E, Tutkun E, Akcan R (2012) Analysis of the hematological and biochemical parameters related to lead intoxication. J Forensic Leg Med 19(8):452–454. doi:10.1016/j.jflm.2012.04.001
Acknowledgments
The authors thank all members in Professor CH. Wang’s laboratory at Wuhan University for their valuable assistances and Dr. Guoxun Chen at The University of Tennessee at Knoxville for comments of the manuscript. The project was supported by the National Natural Science Foundation of China (No. 81172628) and the Fundamental Research Funds for the Central Universities (No. 2014305020201).
Conflict of Interest
The authors declare that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Jingping Ye and Chuang Du contributed equally to this study and share first authorship.
Rights and permissions
About this article

Cite this article
Ye, J., Du, C., Wang, L. et al. Relationship of Blood Levels of Pb with Cu, Zn, Ca, Mg, Fe, and Hb in Children Aged 0∼6 Years from Wuhan, China. Biol Trace Elem Res 164, 18–24 (2015). https://doi.org/10.1007/s12011-014-0200-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-014-0200-8