
Abstract
This study was to investigate blood lead (Pb) and cadmium (Cd) levels and time trend in rural Chinese children derived from the China Nutrition and Health Survey 2002 and 2012 (CNHS 2002, CNHS 2012). In total, 1698 and 1581 of rural Chinese children were selected from the CNHS 2002 and the CNHS 2012 databases, respectively. The blood Pb and Cd levels were determined by inductively coupled plasma mass spectrometer (ICP-MS), whilst the prevalence of blood Pb levels >5 µg/dL and blood Cd levels >0.5 µg/L and the corresponding reference values (RV95s: the upper limit of 95% confidence interval of 95th percentile) were together calculated. From the CNHS 2002 to the CNHS 2012, median concentrations in blood were severally decreased from 6.3 to 3.1 µg/dL for Pb and from 0.64 to 0.39 µg/L for Cd. The prevalence of blood Pb levels >5 µg/dL had decreased from 63.6 to 14.2%, together with blood Cd levels >0.5 µg/L prevalence from 62.7 to 33.5%, respectively. The RV95s of blood Pb and Cd levels were 15.2 µg/dL and 1.54 µg/L in the CNHS 2002, as well as 6.3 µg/dL and 1.12 µg/L in the CNHS 2012. In conclusion, blood Pb and Cd levels had been obviously improved in rural Chinese children during the past 10 years. However, the risks of Pb and Cd exposure are still serious and required to have continuous health monitoring and evaluation, even call for greater collaboration of the government and society.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Lead (Pb) and cadmium (Cd) are two ubiquitous heavy metals that have great toxicological significance in the general population [1, 2]. Excess Pb and Cd exposure has been widely recognized to have a range of adverse health effects, including neurological, cardiovascular, hematological, nephrotoxic, carcinogenic, and genotoxic effects [3, 4]. Nevertheless, a considerable amount of industrial pollutants containing Pb and Cd have been discharged so far and persistently stayed in the environment. With advanced industrialization and urbanization, further aggravation of bioaccumulation in food chains reaches humans.
Children appear to be the most susceptible to adverse effects from Pb and Cd exposure and have a higher health burden as compared to other groups in the population [5], due to higher basal metabolic rate, larger food uptake, and lower toxin elimination rate. In children, excess Pb and Cd exposure can cause numerous negative effects, including impaired neurodevelopment, developmental delay, reduced intelligence quotient, and serious adverse outcomes on bone composition and development [6, 7]. From the viewpoint of public health, there is a pressing need for adequate information regarding adverse events from Pb and Cd exposure. Thus, as an effective tool, human biomonitoring is progressively playing an essential role in identifying and targeting high-risk groups, evaluating interventions, and tracking exposures over time [8].
Blood samples are currently one of the most common choices in laboratory analyses for assessing recent and past exposures to chemical pollutants. Reference values (RVs) are currently recommended to detect the levels in individuals with higher exposures to a substance of interest [9]. Thus, RV95s were further defined as the 95th percentile’s upper limit of the 95% confidence interval (CI) of the measured pollutants, indicating the upper margin of the current background exposure of the general population to a given pollutant at a given time [10]. To date, several reference values for blood Pb and Cd levels have been successively established in some countries, such as the USA [11], Canada [12], Germany [13], Belgium [14], and Korea [15]. However, there is still a paucity of national data on blood Pb and Cd levels in Chinese children, especially those living in rural areas. Coincidently, the conduction of the China Nutrition and Health Survey in 2002 and 2012 (CNHS 2002 and CNHS 2012) provided the valuable opportunities to evaluate and understand pollutant exposure implications in rural Chinese children in the past and in future.
Therefore, the purpose of this study was to investigate national data of blood Pb and Cd levels from the CNHS 2002 and CNHS 2012 databases and delineate the time trend in rural Chinese children. Furthermore, it could be used for the exposure risk assessments for the formulation of public health policies and their management.
Materials and Methods
Study Population
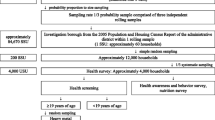
This study was carried out from the CNHS in 2002 and 2012, both covering 31 provinces, autonomous regions, and municipalities in China (Hong Kong, Macao, and Taiwan were excluded). A detailed description of the CNHS 2002 and CNHS 2012 survey designs and sampling strategies has been reported elsewhere [16]. The recommended sample size for determining the reference value was at least 120 according to the International Federation of Clinical Chemistry (IFCC) guidelines; the sample size of each survey was estimated to be at least 1440, for an alpha level of 0.05, when considering residence region (general, poor), sex (male, female), and age group (6–7 years, 8–9 years, 10–11 years). All participants were then selected based on the CNHS 2002 and CNHS 2012 databases using a multistage stratified random sampling method. Information from included children was retrieved and reviewed, and signed consent forms were also examined. The study protocol was approved by the Ethics Committee of the National Institute for Nutrition and Health of the Chinese Center for Disease Control and Prevention.
Collection and Determination of Blood Samples
Blood samples were drawn from each participant after a fasting period of over 8 h using a BD vacutainer blood collection tube containing heparin lithium for venipuncture in the CNHS 2002 and CNHS 2012. Blood samples were stored frozen at −70 ℃ in the biobanks of the CNHS 2002 and CNHS 2012 without freeze-thawing, until analysis. In this study, blood samples were chosen based on the inclusion of children with a strict one-to-one association. Blood samples (100 μL) were melted, vortexed, and diluted in a 1:25 (v/v) solution of 0.5% (v/v) HNO3 and 0.05% (v/v) Triton X-100 (Sigma, USA). Blood Pb and Cd levels were determined using a triple quadrupole inductively coupled plasma mass spectrometer (Q-ICP-MS, PerkinElmer, NexION® 350D, USA) equipped with an autosampler (PerkinElmer, model AS-93 plus, USA). Daily analytical conditions were optimized to meet the requirements of the analysis.
For quality control, the certified reference materials (Seronorm™ Trace Elements Whole Blood Level-2 and Level-3, Norway) were run with prepared blood once every 20 samples, to assess the accuracy and precision of the method. The limits of detection (LOD) and quantification (LOQ) of the method were calculated as 3- and 10-fold the standard deviation of the concentrations of 11 independent blank replicates multiplied by the corresponding dilution multiple. In this study, the LOD for the method was 0.24 µg/L for Pb and 0.02 µg/L for Cd, and the LOQ for the method was 0.79 µg/L for Pb and 0.06 µg/L for Cd, respectively. The intra- and inter-day precisions were 1.0% and 4.8% for Pb, and 1.3% and 5.0% for Cd. The recoveries of Pb and Cd in whole blood with level-2 and level-3 reference materials were 96.7% and 106.7%, respectively. Sample preparations and analysis were performed in an ISO class 6 clean room at the Key Laboratory of Trace Element Nutrition of the National Health Commission of the National Institute for Nutrition Health at the Chinese Center for Disease Control and Prevention.
Statistical Analysis
All statistical analyses were conducted using SAS 9.3 (SAS Institute, Cary, NC, USA). Categorical variables were analyzed using the χ2 test and continuous variables were assessed using the Kolmogorov-Smirnov (K-S) test. Subgroups were classified according to residence region, sex, age group, and BMI status. BMI status was divided by the Z scores of the BMI-for-age growth reference for 5–19 years (thinness was defined as <−2 SD, overweight >1 SD, and obese was considered >2 SD) as suggested by the World Health Organization (WHO). Blood Pb and Cd levels were described in terms of median (M0), interquartile range (IQR), and 95% reference intervals (2.5th to 97.5th percentile). The following values (5 μg/dL for Pb and 0.5 μg/L for Cd) were selected as the cutoff values [17, 18], justifying the threshold for determination of “elevated” levels. The prevalence of elevated blood Pb and Cd was further calculated. In addition, the RV95s of blood Pb and Cd levels were estimated using the CNHS 2002 and CNHS 2012. Differences between subgroups were compared using the Mann-Whitney or Kruskal-Wallis tests. P<0.05 was considered significant.
Results
Characteristics of Study Population
For the included children, average age was 8.6 ± 1.7 years and 9.1 ± 1.8 years; average height was 127.6 ± 11.3 cm and 132.2 ± 12.5 cm; average weight was 25.6 ± 6.5 kg and 30.0 ± 10.1 kg; and BMI was 15.5±1.9 and 16.8±3.2. The sampling characteristics of the children included in the CNHS 2002 and CNHS 2012 are presented in Table 1. In total, 3279 (1698 versus 1581) rural Chinese children were included in the statistical analysis. There were no significant differences in the demographic characteristics between the CNHS 2002 and CNHS2012 (P>0.05).
Blood Pb and Cd Levels
Table 2 shows that median blood Pb concentration had decreased from 6.3 µg/dL in the CNHS 2002 to 3.1 µg/dL in the CNHS 2012. The overall change in blood Pb levels is shown in Fig. 1. Significant differences were observed in residence region, sex, age group, and BMI status (P<0.001). In the CNHS 2002, median blood Pb concentration was significantly higher in boys (6.6 µg/dL) than girls (6.0 µg/dL) (P<0.05), as well as in the general (6.8 µg/dL) than poor rural areas (4.6 µg/dL) (P<0.05). In the CNHS 2012, median blood Pb concentration was significantly higher in boys (3.3 µg/dL) than girls (2.9 µg/dL) (P<0.05), but significantly lower in the general (3.0 µg/dL) than poor rural areas (3.5 µg/dL) (P<0.05). In addition, the median blood Pb concentration changed slightly with increased age and BMI. Of these, the overweight subgroup had the lowest blood Pb levels among the BMI groups.

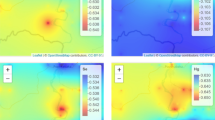
The time change of blood Pb levels in rural Chinese children between 2002 and 2012
As presented in Table 3 and Fig. 2, median blood Cd concentration was 0.64 µg/L in the CNHS 2002 and 0.39 µg/L in the CNHS 2012. There was a significant decrease in the CNHS 2012 as compared with the CNHS 2002 (P<0.05). In the CNHS 2002, a significant difference was observed in the blood Cd levels for residence region and sex (P<0.01). It was fluctuated slightly with increased age and BMI status, but without a significant difference (P>0.05). There was no significant difference in residence region or age group in the CNHS 2012 (P<0.01), but it was different for the residence regions during the CNHS in 2002.

The time change of blood cadimum levels in rural Chinese children between 2002 and 2012
Assessment for Pb and Cd Exposure
As shown in Table 4, there was a distinct decline in the overall or subgroup in the last 10 years. The prevalence of blood Pb levels >5 µg/dL decreased from 63.6% in the CNHS 2002 to 14.2% in the CNHS 2012. The percentage of samples with blood Cd levels of >0.5 µg/L had also diminished from 62.7 to 33.5%. In the CNHS 2002, the prevalence of blood Pb levels of >5 µg/dL was significantly higher in the general than in the poor rural areas (P<0.05). However, no significant difference was observed in sex, age group, or BMI status (P>0.05). In the CNHS 2012, there was no significant difference in sex, age group, or BMI status for the prevalence of samples with blood Pb levels >5 µg/dL (P>0.05).
Reference Values for Blood Pb and Cd
According to the estimation, the RV95s of blood Pb and Cd levels were 15.2 µg/dL and 1.54 µg/L, respectively in the CNHS 2002, as well as 6.3 µg/dL and 1.12 µg/L, respectively in the CNHS 2012 (Table 5). Regardless of the overall or subgroup analyses, a declining trend of RV95s of blood Pb and Cd levels was observed in the CNHS 2012 as compared with the CNHS 2002.
Discussion
Reliable data on blood Pb and Cd levels were obtained in rural Chinese children derived from the CNHS in 2002 and 2012. The median blood Pb and Cd levels had greatly decreased from 6.3 to 3.1 µg/dL for Pb and from 0.64 to 0.39 µg/L for Cd. The prevalence of blood Pb levels >5 µg/dL and Cd levels >0.5 µg/L had 4.5 times (63.6 to 14.2%) and 1.9 times (62.7 to 33.5%) decrease, respectively. In addition, the RV95s of blood Pb and Cd levels were 15.2 µg/dL and 1.54 µg/L in the CNHS 2002, respectively, as well as 6.3 µg/dL and 1.12 µg/L in the CNHS 2012, respectively. From a public health research perspective, the time changes in blood Pb and Cd levels could embody an inspiring improvement toward a healthy living environment and awareness.
To date, human biomonitoring has been conducted and documented in certain populations [19, 20]. Given that Pb and Cd exposure is mainly derived from contaminated air, dust, food, water, or jewelry, inhalation of cigarette smoke, or improper handling of the metal itself [21]. Several effective interventions have been implemented, such as bans on lead-based paint and gasoline, tobacco control, good hygiene, and dietary habits. Our findings confirm that exposure levels of Pb and Cd in rural Chinese children are gradually declining. Nevertheless, blood Pb levels (6.3 µg/dL or 3.1 µg/dL) were still higher in rural Chinese children as compared with Americans at 1.2 µg/dL [11] or Australian’s 1.5 µg/dL [22]. It was only similar to the Italian’s 3.4 µg/dL [23], even approaching half of the Brazilian’s 6.5 µg/dL [24] while the literature reported a level of 8.9 µg/dL in China [25]. By contrast, blood Cd levels (0.64 µg/L or 0.39 µg/L) were relatively consistent with Cd exposures in Korea (0.30 µg/L) [26] and Brazil (0.48 µg/L) [27], but far higher than the German levels (<0.06 μg/L). From the above comparison, we illustrate that Pb and Cd exposure is still of great concern, although blood Pb and Cd levels have decreased considerably in just the last 10 years.
A 10% significantly higher blood Pb level was observed in boys compared to girls. This subtle difference was in line with previous studies from Korea [28], Germany [17], and the USA [29]. This may be explained by more sources of Pb exposure and higher hematocrit levels in boys [30]. Notably, the contrasting blood Pb and Cd levels were observed in the residence regions between the CNHS 2002 and the CNHS 2012. Blood Pb and Cd levels were positively associated with increased age and BMI. The distribution and time trend could be attributed to the socioeconomic factors and bioaccumulation in adipose tissue. In addition, Cd exposure in Asia is generally higher than in Europe or the USA due to higher daily intake of rice and vegetables grown in locally contaminated soil [31]. The RV95s of Pb and Cd blood levels are regularly regarded as convenient tools for early warnings in public health. We tentatively estimated the RV95s of blood Pb and Cd levels in rural Chinese children. They were indeed different in the CNHS 2002 versus the CNHS 2012, and out of line with other countries and regions. As previously reported, the RV95s of blood Pb and Cd levels could be variable and will play an important role in future risk assessments.
This study was the first nationwide population-based study derived from the CNHS 2002 and the CNHS 2012 and reported reliable data on blood Pb and Cd levels in rural Chinese children. However, this study had some limitations. First, the gap between the two surveys should be prudently considered when comparing residential regions, because of the non-one-to-one correspondence in rural areas and only a little in the readjustment district. Second, the RV95s of blood Pb and Cd levels always fluctuate with changes in population, and they are also determined by the ambient environment and monitoring times. Blood Pb and Cd levels in excess RV95s only indicate elevated risks in advance. Third, there is still a lack of information on sociodemographic and environmental factors, and a longitudinal and professional correlation analysis could not be performed.
Conclusions
This study obtained reliable data on Pb and Cd exposures in rural Chinese children derived from the CNHS 2002 and the CNHS 2012. These findings indicate that the exposure risks of Pb and Cd in rural Chinese areas significantly decreased from the CNHS 2002 to the CNHS 2012. Nevertheless, regardless of the RV95s of Pb and Cd exposures, the exposure risks are still rather high, and it is necessary to focus continuous attention, provide in-depth monitoring, and conduct health evaluations, together with greater collaboration between the government and society.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
References
Jarup L (2003) Hazards of heavy metal contamination. Br Med Bull 68:167–182
Tchounwou PB, Yedjou CG, Patlolla AK, Sutton DJ (2012) Heavy metal toxicity and the environment. Exp Suppl 101:133–164
Rehman K, Fatima F, Waheed I, Akash MSH (2018) Prevalence of exposure of heavy metals and their impact on health consequences. J Cell Biochem 119(1):157–184
Satarug S, Gobe GC, Vesey DA, Phelps KR (2020) Cadmium and lead exposure, nephrotoxicity, and mortality. Toxics 8(4):86
Zeng X, Xu X, Boezen HM, Huo X (2016) Children with health impairments by heavy metals in an e-waste recycling area. Chemosphere 148:408–415
Laborde A, Tomasina F, Bianchi F, Brune MN, Buka I, Comba P, Corra L, Cori L, Duffert CM, Harari R, Iavarone I, McDiarmid MA, Gray KA, Sly PD, Soares A, Suk WA, Landrigan PJ (2015) Children’s health in Latin America: the influence of environmental exposures. Environ Health Perspect 123(3):201–209
Al Osman M, Yang F, Massey IY (2019) Exposure routes and health effects of heavy metals on children. Biometals 32(4):563–573
Kolossa-Gehring M, Fiddicke U, Leng G, Angerer J, Wolz B (2017) New human biomonitoring methods for chemicals of concern-the German approach to enhance relevance. Int J Hyg Environ Health 220(2 Pt A):103–112
Schulz C, Angerer J, Ewers U, Kolossa-Gehring M (2007) The German Human Biomonitoring Commission. Int J Hyg Environ Health 210(3–4):373–382
Ewers U, Krause C, Schulz C, Wilhelm M (1999) Reference values and human biological monitoring values for environmental toxins Report on the work and recommendations of the Commission on Human Biological Monitoring of the German Federal Environmental Agency. Int Arch Occup Environ Health 72(4):255–260
Calafat AM (2012) The U.S. National Health and Nutrition Examination Survey and human exposure to environmental chemicals. Int J Hyg Environ Health 215(2):99–101
Saravanabhavan G, Werry K, Walker M, Haines D, Malowany M, Khoury C (2017) Human biomonitoring reference values for metals and trace elements in blood and urine derived from the Canadian Health Measures Survey 2007–2013. Int J Hyg Environ Health 220(2 Pt A):189–200
Schulz C, Angerer J, Ewers U, Heudorf U, Wilhelm M, Human Biomonitoring Commission of the German Federal Environment A (2009) Revised and new reference values for environmental pollutants in urine or blood of children in Germany derived from the German Environmental Survey on Children 2003–2006 (GerES IV). Int J Hyg Environ Health 212(6):637–647
Hoet P, Jacquerye C, Deumer G, Lison D, Haufroid V (2021) Reference values of trace elements in blood and/or plasma in adults living in Belgium. Clin Chem Lab Med 59(4):729–742
Lee JW, Lee CK, Moon CS, Choi IJ, Lee KJ, Yi SM, Jang BK, Yoon BJ, Kim DS, Peak D, Sul D, Oh E, Im H, Kang HS, Kim J, Lee JT, Kim K, Park KL, Ahn R, Park SH, Kim SC, Park CH, Lee JH (2012) Korea National Survey for Environmental Pollutants in the Human Body 2008: heavy metals in the blood or urine of the Korean population. Int J Hyg Environ Health 215(4):449–457
He Y, Zhao W, Zhang J, Zhao L, Yang Z, Huo J, Yang L, Wang J, He L, Sun J, Piao J, Yang X, Ge K, Ding G (2019) Data resource profile: China National Nutrition Surveys. Int J Epidemiol 48(2):368–368f
Schulz C, Wilhelm M, Heudorf U, Kolossa-Gehring M, Human Biomonitoring Commission of the German Federal Environment A (2011) Update of the reference and HBM values derived by the German Human Biomonitoring Commission. Int J Hyg Environ Health 215(1):26–35
Taylor CM, Humphriss R, Hall A, Golding J, Emond AM (2015) Balance ability in 7- and 10-year-old children: associations with prenatal lead and cadmium exposure and with blood lead levels in childhood in a prospective birth cohort study. BMJ Open 5(12):e009635
Liao LM, Friesen MC, Xiang YB, Cai H, Koh DH, Ji BT, Yang G, Li HL, Locke SJ, Rothman N, Zheng W, Gao YT, Shu XO, Purdue MP (2016) Occupational lead exposure and associations with selected cancers: the Shanghai Men’s and Women’s Health Study cohorts. Environ Health Perspect 124(1):97–103
Almerud P, Zamaratskaia G, Lindroos AK, Bjermo H, Andersson EM, Lundh T, Ankarberg EH, Lignell S (2021) Cadmium, total mercury, and lead in blood and associations with diet, sociodemographic factors, and smoking in Swedish adolescents. Environ Res 197:110991
Cwielag-Drabek M, Piekut A, Gut K, Grabowski M (2020) Risk of cadmium, lead and zinc exposure from consumption of vegetables produced in areas with mining and smelting past. Sci Rep 10(1):3363
Kelsall LM, de Gooyer TE, Carey M, Vaughan L, Ansari Z (2013) Blood lead levels in the adult Victorian population: results from the Victorian Health Monitor. Aust N Z J Public Health 37(3):233–237
Forte G, Madeddu R, Tolu P, Asara Y, Marchal JA, Bocca B (2011) Reference intervals for blood Cd and Pb in the general population of Sardinia (Italy). Int J Hyg Environ Health 214(2):102–109
Nunes JA, Batista BL, Rodrigues JL, Caldas NM, Neto JA, Barbosa F Jr (2010) A simple method based on ICP-MS for estimation of background levels of arsenic, cadmium, copper, manganese, nickel, lead, and selenium in blood of the Brazilian population. J Toxicol Environ Health A 73(13–14):878–887
Wang S, Jin Y, Chen J, Lu L, Li Y, Zhao Q, Bu S, Geng X, Guan G, Qu W, Zheng Y, Tang J (2021) Blood lead levels of Chinese children from 1991 to 2020: based on Monte Carlo simulation. Environ Pollut 278:116823
Ahn B, Kim SH, Park MJ (2017) Blood cadmium concentrations in Korean adolescents: from the Korea National Health and Nutrition Examination Survey 2010–2013. Int J Hyg Environ Health 220(1):37–42
Olympio KPK, Silva J, Silva ASD, Souza VCO, Buzalaf MAR, Barbosa F Jr, Cardoso MRA (2018) Blood lead and cadmium levels in preschool children and associated risk factors in Sao Paulo, Brazil. Environ Pollut 240:831–838
Burm E, Song I, Ha M, Kim YM, Lee KJ, Kim HC, Lim S, Kim SY, Lee CG, Kim SY, Cheong HK, Sakong J, Kang HT, Son M, Oh GJ, Kim Y, Yang JY, Hong SJ, Seo JH, Kim J, Oh S, Yu J, Chang SS, Kwon HJ, Choi YH, Choi W, Kim S, Yu SD (2016) Representative levels of blood lead, mercury, and urinary cadmium in youth: Korean Environmental Health Survey in Children and Adolescents (KorEHS-C), 2012–2014. Int J Hyg Environ Health 219(4–5):412–418
Alvarez J, Del Rio M, Mayorga T, Dominguez S, Flores-Montoya MG, Sobin C (2018) A comparison of child blood lead levels in urban and rural children ages 5–12 years living in the border region of El Paso. Texas. Arch Environ Contam Toxicol 75(4):503–511
Popovic M, McNeill FE, Chettle DR, Webber CE, Lee CV, Kaye WE (2005) Impact of occupational exposure on lead levels in women. Environ Health Perspect 113(4):478–484
Jarup L, Berglund M, Elinder CG, Nordberg G, Vahter M (1998) Health effects of cadmium exposure–a review of the literature and a risk estimate. Scand J Work Environ Health 24(Suppl 1):1–51
Acknowledgements
We are very grateful to all the team members and participants involved in the China Nutrition and Health Survey 2002 and 2012.
Funding
This study was sponsored by the Danone Nutrition Fund (Grant No. DIC 2017-06) and the Young Scholar Scientific Research Foundation of Chinese Center for Disease Control and Prevention (Grant No. 2018A204).
Author information
Authors and Affiliations
Contributions
Xiaobing Liu and Xiaoguang Yang conceived and designed the conduction of this study; Xiaobing Liu, Huidi Zhang, Yu Zhang, Jun Wang, Hongxing Tan, and Lichen Yang performed the experiment; Xiaobing Liu wrote the manuscript; Xiaoguang Yang and Jianhua Piao reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Liu, X., Zhang, H., Zhang, Y. et al. The Time Trend of Blood Lead and Cadmium Levels in Rural Chinese Children: China Nutrition and Health Survey 2002 and 2012. Biol Trace Elem Res 201, 2162–2169 (2023). https://doi.org/10.1007/s12011-022-03333-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-022-03333-0