
Abstract
Pseudoexfoliation syndrome (PEX), an age-related disorder of the eye, is associated with significant ophthalmic morbidity and can lead to pseudoexfoliation glaucoma (PEG). The etiology of this disorder has not been clearly understood. Trace elements have been suggested to have roles in the pathogenesis of several disorders. This study aimed to determine whether trace element levels have a role in the development of PEX and/or PEG. Levels of zinc (Zn), copper (Cu), selenium (Se), manganese (Mn), chromium (Cr), cobalt (Co), molybdenum (Mo), nickel (Ni), vanadium (V), arsenic (As), aluminum (Al), mercury (Hg), cadmium (Cd), and strontium (Sr) were determined in serum samples of 32 cases of PEX, 30 cases of PEG, and 32 control subjects using inductively coupled plasma–mass spectrometry. Mn, Mo, and Hg concentrations were found to be significantly increased in patients with PEX. Logistic regression revealed Mn and Hg as the strongest determinants of PEX and Mo as the strongest determinant of PEG in the studied Turkish subjects. Levels of Mn, Cr, Co, Mo, Al, Hg, Sr, Ni, V, and As were determined for the first time in these ophthalmological disorders. Increased levels of serum Mn, Mo, and Hg suggest a possible role of these elements in the pathobiology of PEX.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pseudoexfoliation syndrome (PEX) is an age-related systemic disorder which is characterized by accumulation of granular amyloid-like fibrillar extracellular material in anterior structures of the eye. The buildup of abnormal fibrillar material can block normal drainage of the aqueous humor and can cause, in turn, a buildup of pressure leading to glaucoma and loss of vision. PEX can lead to both open-angle glaucoma and angle-closure glaucoma [1]. However, there are persons with PEX without glaucoma [2]. PEX prevalence was found to be 7.2 % among individuals older than 49 years in the Eastern Mediterranean region of Turkey [3].
Despite extensive research, the exact etiology of this disorder remains unknown. Trace elements are often suspected of being the missing link in some of the unexplained human diseases since they have important roles as catalytic and structural components of larger molecules. On the contrary, most of the metals are recognized as being toxic to humans. There is supporting evidence indicating that trace elements have potential roles in the etiology of several diseases including neurodegenerative diseases [4, 5], coronary heart disease [6], and type 2 diabetes [7]. One of the toxic trace elements (cadmium (Cd)) and some of the essential trace elements including zinc (Zn), copper (Cu), and selenium (Se) were analyzed in PEX before [8, 9]. However, knowledge on the role of other essential (manganese (Mn), chromium (Cr), cobalt (Co), molybdenum (Mo)) and toxic (arsenic (As), aluminum (Al), mercury (Hg), Cd, strontium (Sr)) trace elements, as well as potentially beneficial trace elements (nickel (Ni),vanadium (V)) in PEX and/or pseudoexfoliation glaucoma (PEG) is missing.
In the present study, we aimed to clear our understanding of the complex etiology of PEX/PEG. Therefore, we determined the essential, potentially beneficial and toxic trace elements in PEX/PEG patients and control subjects in Turkish population.
Materials and Methods
Patient Selection
This case–control study included 32 patients with PEX (16 males, 16 females), 30 patients with PEG (16 males, 14 females), and 32 control subjects (17 males, 15 females) who were examined at Department of Ophthalmology, Gülhane Military Medical Academy, Turkey. The institutional review board and ethics committee approval was obtained for the study, and written informed consent was obtained from all subjects. The tenets of the Declaration of Helsinki were followed throughout the study.
The diagnosis of PEX was made on slit-lamp examination following mydriasis and included the presence of typical pseudoexfoliation material on the anterior lens capsule and/or the pupillary border. Patients with PEG followed up by our Glaucoma Service were also recruited into the study. PEG patients were diagnosed when anterior segment findings of PEX accompanied an intraocular pressure (IOP) >21 mmHg without treatment, typical optic nerve head changes, and visual field defects. Consecutive age-matched patients with an IOP ≤21 mmHg, a normal optic disk appearance, and no visual field defects were included as controls. Healthy subjects and all patients received a comprehensive ophthalmological examination including best-corrected Snellen visual acuity testing, slit-lamp examination, Goldmann applanation tonometry, gonioscopic evaluation, dilated fundus examination using a 90-dioptre lens, and visual field evaluation using the 30-2 SITA-Standard algorithm (Humphrey Instruments Inc., San Leandro, CA, USA).
Patients with other ophthalmic diseases (uveitis, age-related macular degeneration, etc.), kidney disease, and any central nervous system disease that might have interfered with visual field test were excluded from this study. A detailed medical history was also obtained. All subjects were questioned about smoking and medications (non-steroidal anti-inflammatory drug, supplemental vitamin C and/or vitamin E, diuretics, etc.) and excluded from the study if answered yes. Blood samples were obtained from all the subjects by venipuncture. The blood samples were centrifuged at 2,000×g for 15 min, and the sera were separated and stored at −24 °C until use.
The demographic features of the patients and the controls are given in Table 1. There was no statistically significant difference among groups in terms of age and frequency of males and females.
Determination of the Trace Elements
The concentrations of Zn, Cu, Se, Mn, Cr, Co, Mo, Ni, V, As, Al, Hg, Cd, and Sr in serum samples of all subjects were analyzed by inductively coupled plasma–mass spectrometry (ICP-MS) (Agilent 7500a, Agilent Technologies, USA). A microwave oven (CEM Mars5), equipped with 12 low-volume per uoroalkoxy (PFA) lined vessels (ACV 50) with safety rupture membranes (maximum operation pressure 1,380 kPa), was used for sample digestion. The instrumental operating conditions for ICP-MS are summarized in Table 2.
Statistical Analyses
The categorical variables (sex) were expressed as proportions and compared using the chi-square test. Normality of the sample distribution of each continuous variable was tested with the Kolmogorov–Smirnov test. Normally distributed continuous variables were expressed as mean ± SD and continuous variables which did not follow normal distribution were given in median and range. Differences of continuous variables between two groups were evaluated by the independent samples t test or the Mann–Whitney U test, depending on the normal distribution. One-way analysis of variance (ANOVA) was used for comparing the means of three groups for normally distributed data and Kruskal–Wallis one-way analysis of variance by ranks test for comparing medians of three groups for skewed data. Binary logistic regression analysis with backward selection method was used to determine the effects of trace elements, age, and gender in the prediction of PEX/PEG. Two-tailed probability values with 95 % confidence intervals were estimated for each odds ratio (OR). The Hosmer–Lemeshow goodness of fit test was used for calibration. Statistical Package for Social Sciences version 16.0 (SPSS, Chicago, IL, USA) was used for these statistical analyses. A P value of less than 0.05 was evaluated as statistically significant.
Results
The trace element levels in serum samples of patients with PEX and PEG were compared relative to the controls. We also compared the trace element levels between PEX and PEG patients. In addition, the three groups were compared together. The levels of trace elements in the three groups are given in Table 3 and the significant results were marked.
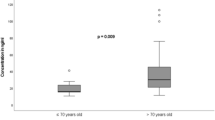
Mn levels of PEX patients were significantly higher compared both to the PEG (P = 0.042) and the control groups (P = 0.002). When the three groups were analyzed together, Mn concentration was significantly different (P = 0.010 by ANOVA). On the other hand, we observed that Mn levels were almost the same in the PEG and the control groups. Mo and Hg concentrations were significantly higher in PEX patients compared to controls. The levels of these two elements were also higher in PEG group compared to the controls; however, the differences were not significant. Hg concentrations showed significant variation among the three study groups (P = 0.003 by ANOVA).
Levels of Zn, Cu, Se, Al, Cr, Ni, and As were not widely different in the patients compared to the controls. Co, V, Sr, and Cd levels were less than 0.5 μg/L for all the subjects (Table 3). All of the elements fell into the respective reference interval, except for the Mn level of PEX patients, which was slightly above the upper limit for Mn [10].
Logistic regression analysis revealed Mn (OR = 3.686, 95 % CI = 1.272–10.687, P = 0.016) and Hg (OR = 2.686, 95 % CI = 1.114–6.476, P = 0.028) to be significantly associated with PEX and Mo to be significantly associated with PEG (OR = 3.685, 95 % CI = 1.079–12.585, P = 0.037). Age and sex were not associated with the risk of PEX or PEG (results not given in a table). Calibration of the logistic regression models turned out to be satisfactory (chi-square = 7.791 for PEX; 8.977 for PEG; 8 degrees of freedom for both analyses; P = 0.454 for PEX and P = 0.344 for PEG). The models predicted 74.1 % of cases correctly in PEX and 61.1 % for PEG.
Discussion
In the present study, we hypothesized that a number of essential and/or toxic trace elements might have a role in the development of pseudoexfoliation syndrome, one of the most important age-related ophthalmological diseases with an unexplained pathology, as well as pseudoexfoliation glaucoma, which can lead to a loss of vision.
Essential trace elements such as Zn, Cu, Se, Mn, Cr, Co, and Mo act as cofactors or prosthetic groups of several enzymes including alcohol dehydrogenase, superoxide dismutase (SOD) and carbonic anhydrase (Zn), cytochrome oxidase and SOD (Cu), glutathione peroxidase (Se), arginase (Mn), sulfite oxidase, xanthine oxidoreductase, and aldehyde oxidase (Mo) which participate in various enzymatic reactions indispensible for human metabolism.
Zn is found in almost all tissues, although the highest concentration of this trace element is detected in the eye. Zn is essential in the retina, choroid, cornea, and lens [11]. Zn and Cu are generally considered to have antioxidant roles in the human metabolism, as these metals are involved in the process of elimination of superoxide radicals by the SOD enzyme. Decreased levels of Cu and Zn not only lead to inadequate antioxidant defense mechanism due to a reduction of Mn/Zn-SOD but also cause an increase in body iron stores due to the antagonistic relationship between these two elements and iron [12]. Iron is a strong oxidant that catalyzes the oxidation of LDL in vitro. Furthermore, 90 % of Cu is bound to ceruloplasmin, an iron oxidase and an acute phase reactant, as well as an antioxidant protein found in plasma. Therefore, reduced level of Cu is expected to be associated with increased oxidative stress.
However, it is also known that Cu is a transition metal and can potentially induce catalysis of the oxidation of lipoproteins. Cu was indeed shown to be involved in ocular inflammation [13]. Several lines of evidence indicate that oxidative stress constitutes a major mechanisms involved in the pathobiology of PEX syndrome [14–16]. Cu level was found to be lower in patients with cataract [17]. Zn concentrations were also considerably lower in cataract [17] and age-related macular degeneration [18].
Therefore, we suspected that Zn and Cu might have a role in the development of PEX and/or PEG. We found slightly lower serum concentrations of Zn and Cu in patients with PEX. Similarly, in a study on Turkish subjects, Zn level in serum displayed no significant difference between PEX patients and the controls [19]. Zn content of lenses also did not differ enormously between the two groups. However, in aqueous humor, markedly higher Zn and Cu levels in PEX group were found. Levels of Cu in serum and lens tissue were also dramatically increased in PEX group compared to the control group [19]. A more recent study was also in accordance with our findings; Zn and Cu concentrations in the aqueous humor did not show statistically significant difference in cataract patients with and without PEX [20]. In contrast, the work undertaken by Yildirim et al. [8] reported significantly lower Zn concentration in lens tissues of cataract patients with PEX. The level of Cu in the lens from patients with PEX and without PEX was, however, not statistically different [8].
Se is an essential mineral that is incorporated into at least 25 distinct proteins mainly as selenocysteine residue. These proteins include glutathione peroxidases (GPx), iodothyronine deiodinases, and thioredoxin reductases. Se is best known for its crucial role in the GPx enzyme system, which is accepted as the major antioxidant defense system within the body. However, it was also found that high-plasma Se was associated with glaucoma [21]. In our study, we observed slightly higher levels of Se in PEG patients as compared to the controls and PEX patients. On the other hand, PEX patients had slightly lower Se concentration relative to the controls. There are only two previous studies considering Se levels in PEX. In the first one, serum and lens concentrations of Se were reported to be far lower in patients with PEX [9]. In the second study, Yilmaz et al. [22] determined significantly decreased Se levels in the aqueous humor and conjunctival specimens of Turkish patients with PEX syndrome compared to controls. Mean Se levels in serum were not significantly different between patients and the controls, but slightly lower in PEX patients, as in our study. Apart from PEX, serum Se level was measured in age-related macular degeneration and found to be much lower in patients [18].
Mn is a nutritionally essential metal because it acts as an activator and constituent of many enzymes such as MnSOD. However, Mn levels were reported to be elevated in several diseases including congestive heart failure, hypertension, diabetes, infection, chronic obstructive pulmonary disease, and psychoses [23]. As stated by Paracelsus (1493–1541), everything is toxic; it is just a matter of dose that differentiates a remedy and a poison. Essential elements can also be toxic if excessive amounts are ingested. As such, Mn, an essential trace mineral, has also been known as neurotoxic, as overexposure can cause manganism, a neurological syndrome that is similar to Parkinson’s disease [5]. Mn is a redox-active metal and has the ability to promote free radical formation that leads to oxidative stress. It was suggested that Mn-induced neurotoxicity includes NF-κB induction and the activation of nitric oxide synthase through reactive oxygen species [24]. Considerable evidence implicates crucial roles of oxidative stress in the pathogenesis of PEX and/or PEG [14–16]. In our study, we observed that patients with PEX had significantly higher serum Mn when compared to both the PEG and the control groups. Increased Mn levels in PEX patients could have led to disturbance of oxidative balance in the eye, which in turn could have paved the way to the development of PEX in the Turkish population studied. There are no other studies in the literature determining Mn levels in PEX/PEG. Khosla et al. [25] have studied the effect of Mn on rabbit retina and found that it is potentially retinotoxic, having a selective effect on photoreceptors and ganglion cells.
Mo functions as a cofactor for three enzymes, namely sulfite oxidase, xanthine oxidase, and aldehyde oxidase [26]. Adverse effects of Mo intake was linked to impaired utilization of Cu in ruminants [27] and was suggested to be due to the interaction among Mo, Cu, and sulfur that occurs in ruminants, but not in humans. Elevations in blood Mo concentrations were accompanied by decreases in blood Cu concentrations [26]. In addition, a gout-like syndrome and pneumoconiosis have been associated with excessive concentrations of Mo [28]. In their study with trace elements, Khosla et al. [25] have also tested the effect of Mo, in addition to Mn, on rabbit retina. They concluded that Mo was the most toxic among the elements studied. In our study, we found prominently increased levels of Mo in PEX patients compared to the controls, as well as slightly lower Cu levels in the patient groups. This finding could point to a potential role of Mo in the pathogenesis of PEX and/or PEG; however, further more detailed studies are required to better understand the role of Mo in these disorders. To the best of our knowledge, this is the first study that analyzes Mo levels in PEX/PEG.
Cr is now considered as an essential trace element since it takes role in the metabolism of glucose, insulin, and fatty acids [29]. In the present study, we did not find significant differences in the concentrations of Cr among the groups. Co is another essential trace element as it is a component of vitamin B12, the coenzyme for methyl transferase that is necessary for thymidine synthesis and, ultimately, DNA biosynthesis and the transcription process itself. Excess levels of Co is toxic; however, it is not a cumulative toxin and is mainly excreted in urine and to a lesser extent via feces. It does not circulate freely in the plasma; that is probably why all the subjects had Co levels less than 0.5 μg in this study. We are not aware of any studies analyzing the roles of Mn, Cr, Co, or Mo in PEX and/or PEG.
There are a group of metals which are not proven to be essential to humans but may have some beneficial effects at low levels of exposure. Also called ultratrace elements, this group consists of Ni, V, boron, and silicon. Some authors also include arsenic in this group. As will be expected, these elements are toxic at higher levels [30]. There are no studies in the literature searching for the role of Ni, V, and As in any ophthalmological disorders including PEX and PEG. We did not find significant differences among the groups studied in terms of levels of Ni, V, and As.
In addition to the essential and possibly beneficial elements, we were also interested in the levels of metals with no known beneficial effects, such as Al, Hg, Cd, and Sr, which are known to interfere with vital processes in the body. To the best of our knowledge, this is the first study investigating the roles of Al, Hg, and Sr in the pathobiology of PEX and/or PEG.
Al is neurotoxic and has been implicated in the pathogenesis of Alzheimer’s disease [31]. Al may contribute to some specific diseases, most of which related with aging [32]. Al levels were within normal ranges and slightly higher in patients with PEX and PEG compared to the controls in this study.
Hg is a heavy metal occurring in several forms, all of which can produce toxic effects in high enough doses. Hg toxicity mechanism depends on inhibition of selenoenzymes irreversibly. Thioredoxin reductase, a selenoenzyme, restores vitamins C and E, back into their reduced forms, enabling them to counteract oxidative damage within body cells [33]. The toxic effects include pathological disturbances in the brain, lungs, and kidney [34]. People are mainly exposed to methylmercury, the organic species of Hg, when they digest fish and shellfish. Methylmercury is highly toxic to neurological development in utero at very low levels of exposure. Children with autism were found to have significantly greater in-hair concentration levels of Pb, Hg, and uranium. In the present study, Hg concentrations were considerably elevated in patients with PEX as compared to the controls, even though within the reference interval in both groups. Therefore, we can suggest that mercury, even below its toxic level, may have a role in the processes leading to the formation of pseudoexfoliative material, probably due to reduction of antioxidants in this tissue.
Cd is a toxic metal and can induce several diseases in humans, especially cancer, as well as aging diseases, kidney, and bone diseases. Sr was indicated in bone formation and resorption in the mouse [35]; however, a role for this trace element in human metabolism has not been reported to date. In our study, we did not determine Cd and Sr to be important in PEX and/or PEG, as the concentrations of these metals were less than 0.5 μg/L in all the subjects. In a recent study, Cd was detected in a small number of aqueous humor samples, without however statistical differences between PEX and control groups [20].
When the effects of all parameters were taken into account in a logistic regression analysis, Mn and Hg came out to be the strongest determinants of PEX and Mo was the strongest determinant of PEG in the Turkish subjects studied. Limitations of this study include number of the subjects; however, it should be stated that the sample is clinically well defined and strictly selected. We also did not have a chance to obtain lens tissue or aqueous humor from the subjects. It is informative to determine the essential and toxic trace element concentrations in biological samples; however, at present, the practical implications in terms of diagnosis and clinical management are limited.
In conclusion, the main findings in the present study were the prominently increased levels of Mn, Mo, and Hg in patients with PEX. To the best of our knowledge, this is the first time Mn and Hg are found as significant determinants of PEX and Mo as the significant determinant of PEG. We are not aware of any studies analyzing the roles of Mn, Cr, Co, Mo, Al, Hg, Sr, Ni, V, and As in the pathobiology of these ophthalmological disorders. The exact roles of these elements in the pathogenesis of PEX and/or PEG could be better understood through further detailed studies.
Abbreviations
- Al:
-
Aluminum
- As:
-
Arsenic
- Cd:
-
Cadmium
- Cr:
-
Chromium
- Co:
-
Cobalt
- Cu:
-
Copper
- Hg:
-
Mercury
- Mn:
-
Manganese
- Mo:
-
Molybdenum
- Ni:
-
Nickel
- PEX:
-
Pseudoexfoliation syndrome
- PEG:
-
Pseudoexfoliation glaucoma
- Se:
-
Selenium
- Sr:
-
Strontium
- V:
-
Vanadium
- Zn:
-
Zinc
References
Bhat S (2010) Pseudoexfoliation syndrome: an identifiable cause of open angle glaucoma. KJO 22(4):330–335
Pons ME. Pseudoexfoliation Glaucoma. In: Hampton R (ed) Medscape. http://emedicine.medscape.com/article/1206366-overview. Accessed 15 Dec 2011
Yalaz M, Othman I, Nas K, Eroğlu A, Homurlu D, Cikintas Z et al (1992) The frequency of pseudoexfoliation syndrome in the eastern Mediterranean area of Turkey. Acta Ophthalmol (Copenh) 70(2):209–213
Sayre LM, Perry G, Atwood CS, Smith MA (2000) The role of metals in neurodegenerative diseases. Cell Mol Biol 46:731–741
Zatta P, Lucchini R, van Rensburg SJ, Taylor A (2003) The role of metals in neurodegenerative processes: aluminum, manganese, and zinc. Brain Res Bull 62:15–28
Fields M (1999) Role of trace elements in coronary heart disease. Br J Nutr 81:85–86
Chaudhary DP, Sharma R, Bansal DD (2010) Implications of magnesium deficiency in type 2 diabetes: a review. Biol Trace Elem Res 134:119–129
Yildirim Z, Uçgun NI, Kiliç N, Gürsel E, Sepici-Dinçel A (2007) Pseudoexfoliation syndrome and trace elements. Ann N Y Acad Sci 1100:207–212
Laganovska G, Martinsons A, Pitrans B, Widner B, Fuchs D (2003) Kynurenine and neopterin in the aqueous humor of the anterior chamber of the eye and in serum of cataract patients. Adv Exp Med Biol 527:367–374
Wu AHB (2006) Tietz clinical guide to laboratory tests, 4th edn. Saunders/Elsevier, St. Louis
Karcioglu ZA (1982) Zinc in the eye. Surv Ophthalmol 27(2):114–122
Owen CA Jr (1978) Effects of iron on copper metabolism and copper on iron metabolism in rats. Am J Physiol 224:514–518
McGahan MC, Bito LZ. (1982–1983) The pathophysiology of the ocular microenvironment. I. Preliminary report on the possible involvement of copper in ocular inflammation. Curr Eye Res 2(12):883–5
Haung W, Koralewska-Makár A, Bauer B, Akesson B (1997) Extracellular glutathione peroxidase and ascorbic acid in aqueous humor and serum of patients operated on for cataract. Clin Chim Acta 261:117–130
Jacques PF, Chylack LT Jr, McGandy RB, Hartz SC (1988) Antioxidant status in persons with and without senile cataract. Arch Ophthalmol 106:337–340
Zoric L, Miric D, Milenkovic S, Jovanovic P, Trajkovic G (2006) Pseudoexfoliation syndrome and its antioxidative protection deficiency as risk factors for age-related cataract. Eur J Ophthalmol 16:268–273
Bhat KS (1988) Plasma calcium and trace elements in human subjects with mature cataract. Nutr Rep Int 37:157–163
Öztürk F, Bayraktar Z, Aydın A, Abbanoğlu F, Koç B, Işımer A (1993) Age-related macular degeneration. Ret-Vit 1(2):148–151
Cumurcu T, Mendil D, Etikan I (2006) Levels of zinc, iron, and copper in patients with pseudoexfoliative cataract. Eur J Ophthalmol 16(4):548–553
Panteli VS, Kanellopoulou DG, Gartaganis SP, Koutsoukos PG (2009) Application of anodic stripping voltammetry for zinc, copper, and cadmium quantification in the aqueous humor: implications of pseudoexfoliation syndrome. Biol Trace Elem Res 132(1–3):9–18
Bruhn RL, Stamer WD, Herrygers LA, Levine JM, Noecker RJ (2009) Relationship between glaucoma and selenium levels in plasma and aqueous humour. Br J Ophthalmol 93:1155–1158
Yilmaz A, Ayaz L, Tamer L (2011) Selenium and pseudoexfoliation syndrome. Am J Ophthalmol 151(2):272–276
Sullivan JF, Blotcky AJ, Jetton MM, Hahn HK, Burch RE (1979) Serum levels of selenium, calcium, copper, magnesium, manganese and zinc in various human diseases. J Nutr 109(8):1432–1437
Prabhakaran K, Ghosh D, Chapman GD, Gunasekar PG (2008) Molecular mechanism of manganese exposure-induced dopaminergic toxicity. Brain Res Bull 76(4):361–367
Khosla PK, Karki DB, Gahlot DK (1983) Retinotoxic effect of zinc, manganese and molybdenum on rabbit retina (an experimental study). Indian J Ophthalmol 31:545–547
IOM (Institute of Medicine). Dietary reference intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. pp. 420–441. Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Panel on Micronutrients, Food and Nutrition Board, Institute of Medicine: Washington, DC. ISBN 0-309-7279-4 2001. http://www.nap.edu/catalog/10026.html. Accessed 20 Feb 2012
Mills CF, Davis GK (1987) Molybdenum. In: Mertz W (ed) Trace elements in human and animal nutrition, 5th edn. Academic, New York, pp 429–463
Barceloux DG (1999) Molybdenum. J Toxicol Clin Toxicol 37(2):231–237
Stearns DM (2000) Is chromium a trace essential metal? Biofactors 11(3):149–162
Goyer R (2004) Issue paper on the human health effects of metals. U.S. Environmental Protection Agency Risk Assessment Forum. http://www.epa.gov/raf/metalsframework/pdfs/metals-risk-assessment-final.pdf. Accessed 20 Nov 2012
Crapper DR, Krishnan SS, Dalton AJ (1973) Brain aluminum distribution in Alzheimer’s disease and experimental neurofibrillary degeneration. Science 180:511–513
Ganrot PO (1986) Metabolism and possible health effects of aluminum. Environ Health Perspect 65:363–441
Carvalho CML, Hashemy SI, Lu J, Holmgren A (2008) Inhibition of the human thioredoxin system: a molecular mechanism of mercury toxicity. J Biol Chem 283(18):11913–11923
Clifton JC II (2007) Mercury exposure and public health. Pediatr Clin North Am 54(2):237–269
Marie PJ, Hott M (1986) Short-term effects of fluoride and strontium on bone formation and resorption in the mouse. Metabolism 35(6):547–551
Acknowledgments
The authors thank to the participants of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ceylan, O.M., Can Demirdöğen, B., Mumcuoğlu, T. et al. Evaluation of Essential and Toxic Trace Elements in Pseudoexfoliation Syndrome and Pseudoexfoliation Glaucoma. Biol Trace Elem Res 153, 28–34 (2013). https://doi.org/10.1007/s12011-013-9644-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-013-9644-5