
Abstract
The possible mechanism of adriamycin (ADR) and/or selenium (Se) deficiency-induced cardiac dysfunction, and cardioprotective effects of Se against ADR-induced cardiac toxicity were investigated in this study. Cardiac function was evaluated by plasma brain natriuretic peptide level and echocardiographic and hemodynamic parameters. Cardiac glutathione peroxidase (GPx) activity was assessed spectrophotometrically. Expression of ATP-sensitive potassium channels (KATP) subunits—SUR2A and Kir6.2—were examined by real-time PCR and Western blotting. The results showed that cardiac function and cardiac GPx activity decreased remarkably after administration of ADR or Se deficiency; more dramatic impairment of cardiac function and cardiac GPx activity were observed after co-administration of ADR and Se deficiency. Mechanically, it is novel for us to find down-regulation of KATP subunits gene expression in cardiac tissue after administration of ADR or Se deficiency, and more significant inhibition of cardiac KATP gene expression was identified after co-administration of ADR and Se deficiency. Furthermore, cardiac toxicity of ADR was found alleviated by Se supplementation, accompanied by restoring of cardiac GPx activity and cardiac KATP gene expression. These results indicate that decreased expression of cardiac KATP is involved in adriamycin and/or Se deficiency-induced cardiac dysfunction; Se deficiency exacerbates adriamycin-induced cardiac dysfunction by future inhibition of KATP expression; Se supplementation seems to protect against adriamycin-induced cardiac dysfunction via restoring KATP expression, showing potential clinical application in cancer chemotherapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chemotherapy is now a major regimen of cancer for its effectiveness which significantly increases survival rate in patients with cancer. However, the cardiotoxicity after chemotherapy administrations which is presented as cardiac dysfunctions draws our attention. Both early diastolic and later systolic cardiac dysfunction were observed in clinical practice and animal models [1]. Pathologically, sacroplasmic reticulum injury, mitochondrial damage, and perimyocytic matrix loss were observed in heart after chemotherapy administrations [2].
It is suggested that heart failure is associated with lower circulating selenium (Se) level. Se deficiency is believed as an admitted cause of reversible heart failure such as Keshan Disease [3]. Epidemiological data showed that low Se concentration was associated with cardiovascular death in patients with acute coronary disease [4]. Lowered circulating Se level has been recognized as an indicator of increasing risk of cardiovascular diseases [5]. Thus, patients with low Se status may have already suffered from potential or subclinical cardiovascular diseases before observation of marked cardiac dysfunction. As an antioxidant inducer, the cardiac protective role of Se has been described in previous studies [6, 7]. It is interesting for us to investigate whether the low Se status exacerbates cardiac dysfunction on one hand, and on the other hand, if Se supplement attenuates cardiac dysfunction during chemotherapy administration.
Expression of inward rectifier K+ channels (KATP) has been indentified in cardiac muscle at high density [8]. Cardiac KATP is described molecularly composed of two subunits: regulatory sulfonylurea receptors 2A (SUR2A) and inward rectifying K+ channel 6.2 (Kir6.2), which locate on intracellular membranes of cardiomyocytes [9]. As a metabolism activity-gated biological sensor [10], the most important role of KATP is to adjust potential-dependent functions to accommodate cell energy demand under physiological and pathological conditions [11]. There are immediate and delayed regulations of KATP channels. The former means temporal regulation of channel activities after instant metabolic changes [12], while the later means postponed but more profound regulation of KATP channels by modulating the gene expressions [13]. Activation and up-regulated expression of KATP were described cardioprotective in previous studies [14, 15].
Thus, mechanically, it is logical for us to assume that the regulation of KATP channels may be involved in chemotherapy and/or low-selenium-induced cardiac dysfunction; and supplementation of Se could attenuate chemotherapy-induced cardiac dysfunction via modulating expression of KATP channel. In order to demonstrate this hypothesis, the present study employed adriamycin and/or low-selenium-induced cardiac dysfunction animal models. Cardiac function and expression of KATP channel were assessed before and after supplementation of Se in animals.
Materials and Methods
Animals
Fifty-one male weaning (3-week-old) Sprague–Dawley rats (SPF class, body weight 75 ± 10 g) were raised in ten polypropylene cages under controlled environment conditions (12-h light–dark cycle, temperature 25 ± 1 °C, humidity 65 ± 4 %). Standard diet (containing 0.2 mg selenium/kg food) [16] was produced by Animal Experimental Center of Xi’an Jiaotong University and low-selenium diet (<0.02 mg selenium/kg food) was produced by Trophic Animal Feed High-tech Co. (Jiangsu, China) according to AIN-93M formula. Diets were stored at 4 °C and fresh tap water was allocated continuously. All animal experimental procedures followed protocols approved by Medical Animal Research Ethics Committee at Xi’an Jiaotong University.
Groups and Treatments
Animals were assigned randomly into five groups: control (n = 10), ADR (n = 10), LS (n = 10), LS + ADR (n = 11), and ADR + SS (n = 10). In control, animals were fed with standard diet for 14 weeks and then treated by intraperitoneal injection of physiological saline everyday for 21 days. In ADR, animals were fed with standard diet for 14 weeks and then treated by four equal intraperitoneal injections of adriamycin (Pharmacia & Upjohn, UK) once a week during 4 weeks. Each injection contained 4 mg/kg bodyweight adriamycin, for a total dose of 16 mg/kg bodyweight (modified from previous studies [17]). In LS, animals were fed with low-selenium diet for 14 weeks and then treated by intraperitoneal injection of physiological saline every day for 21 days. In ADR + LS, animals were fed with low-selenium diet for 14 weeks and then treated by four equal intraperitoneal injections of adriamycin (4 mg/kg bodyweight) once a week during 4 weeks; In ADR + SS, animals fed with standard diet for 14 weeks and then treated by four equal intraperitoneal injections of adriamycin (4 mg/kg bodyweight) once a week during 4 weeks, then intraperitoneal injection of sodium selenite (0.05 mg/kg bodyweight; Sigma-Aldrich, USA) was administrated as selenium supplementation every day for 21 days [18].
Echocardiographic and Hemodynamic Parameters
Echocardiography
Echocardiographic tests were performed according to protocols described in other previous studies [19, 20]. Animals were anesthetized with chloral hydrate (10 %, 0.03 ml/kg bodyweight) intraperitoneally 10 min before imaging. In order to maintain an optimal image quality, the hair of anterior chest wall was removed by 7 % sodium sulfite solution and rats were placed left laterally. Vivid 7 dimension (GE Healthcare, USA) with probe (12L) working at 10 MHz was utilized. The probe was placed parallel to left margin of sternum, adjusting image depth ranging from 2.0 to 4.0 cm. Regurgitant jets were assessed by two-dimensional color and continuous Doppler. M-mode tracings were applied to determine left ventricular end-systole diameter (LVESD) and left ventricular end-diastole diameter (LVEDD). At last, functional parameters such as left ventricular fractional shortening (LVFS%) which stands for percentage of blood ejected by left ventricle each heart beat and left ventricular ejection fraction (LVEF%) which measures the change of left ventricular diameter from each diastole to systole were calculated respectively: LVFS% = [(LVEDD−LVESD)/LVEDD]%; LVEF% = [(LVEDV−LVESV)/LVEDV]%.
Hemodynamic Parameters
According to methods described in a previous study [21], hemodynamic determination was conducted. Animals were anesthetized with chloral hydrate (10 %, 0.03 mL/kg bodyweight) intraperitoneally. A catheter connected to Powerlab 4/25 biological analysis system (AD Instrument, Australia) was intubated from right carotid artery into left ventricle. Left ventricular systolic pressure (LVSP) and left ventricular end-diastolic pressure (LVEDP) were measured. Left ventricular developed pressure (LVDP) was calculated by subtracting LVEDP from LVSP (LVDP = LVSP−LVEDP). Heart rate (HR) was measured by electrocardiogram connected to Powerlab 4/25 biological analysis system.
Selenium Concentration Detection
Samples of whole blood and hearts harvested from rats were wet-washed by mixed acids (nitric acid and perchloric acid) in borosilicate reaction tubes. After removal of excess acids, samples were titrated to 10 ml by ultra pure water (Aqulix 5 water purification system, Merck Millipore, USA). Selenium concentration was then determined by flameless atomic absorption spectrophotometry method using Z-5000 spectrophotometer (Hitachi, Japan) with cathode lamp of Se (resonance line, 196.0 nm; Photron, Australia). Standard selenium solutions were used to calibrate the results.
Plasma BNP Assay
After femoral artery puncture, whole blood samples were collected using EDTA-Na2 vacuum blood collection tubes. Supernatant was collected after centrifuged at 1,500 rpm for 20 min. Samples were processed by Triage brain natriuretic peptide (BNP) assay (Biosite, USA) within 1 h after collection at room temperature according to the manufacturer’s instructions.
Tissue Preparation
Heart was removed immediately after sacrifice, trimmed on ice, then transferred to −80 °C refrigerator after flash-frozen in liquid nitrogen. Collected tissue was then processed for real-time PCR and Western blotting.
Real-Time PCR
According to manufacturer’s instructions, total RNA was extracted from tissue using RNAfast 200 Kit (Fastagen, Shanghai, China). Reverse transcription was performed by using PrimeScript RT Master Mix (TaKaRa, Japan). SYBR Premix Ex TaqTMII (TaKaRa, Japan) was employed to perform real-time PCR, using oligonucleotide primers for SUR2A and Kir6.2 [6] (Table 1). Relative expression of mRNA was analyzed and compared using Bio-Rad IQ5 software (Version 2.0, BioRad, USA). △cycle threshold (△Ct = CtTarget−Ctβ-actin) was employed when β-actin expression was introduced as endogenous reference gene to normalize mRNA expression of SUR2A and Kir6.2.
Western Blotting
Frozen cardiac tissue was homogenized in RIPA lysis buffer system (Santa Cruz, USA) with PMSF (Santa Cruz, USA). All procedures followed manufacturer’s instructions. Sample protein concentration was detected by using BCA protein assay kit (Santa Cruz, USA). Sample protein was boiled in 1× SDS-PAGE loading buffer and separated by electrophoresis in 10 % SDS–polyacrylamide gel, then transferred to a PVDF membrane. Antibodies against Kir6.2 (ab79171, Abcam, USA) and SUR2A (ab84229, Abcam, USA) were applied to incubate the bolts at 4 °C overnight. Tris-buffered saline (containing 0.02 % Tween 20) was used to wash the membranes which were then incubated with goat polyclonal secondary antibody to rabbit IgG conjugated to HRP (ab6721, Abcam, USA). Membranes were developed using Super Signal West Pico chemiluminescence reagent (Thermo Scientific, USA) and then visualized on X-ray films.
Cardiac Tissue Glutathione Peroxidase Activity Assay
GPx activity in heart extract was assessed by spectrophotometrical method using Glutathione Peroxidase Cellular Activity Assay Kit (Sigma-Aldrich, USA), following the manufacturer’s instructions. The assay is based on the reaction in which oxidation of glutathione (GSH) to oxidized glutathione (GSSG) is catalyzed by GPx. As NADPH is consumed when GSSG is recycled back to GSH, the decrease in NADPH absorbance at 340 nm (Tecan Sunrise Absorbance Reader, Tecan, Austria) could be utilized to calculate the activity of GPx indirectly.
Statistical Analysis
Data obtained was input into Excel (version 12.0, Microsoft, USA) and analyzed by SPSS (version 17.0, SPSS, USA). Results were presented as (mean ± SD). Among groups, comparisons of differences were analyzed by one-way ANOVA, and then a LSD test was carried out. P < 0.05 was considered statistically significant.
Results
Se Concentration in Cardiac Tissue and Blood Samples
Se concentration in cardiac tissue and blood is shown in Table 2. Significant changes of Se concentration were observed in low-Se dietary and/or Se intraperitoneal injection-treated animals. Compared with control, Se concentration in blood and/or cardiac tissue decreased significantly in LS and ADR + LS groups. Se intraperitoneal injection was proved to increase Se concentration in blood and cardiac tissue in ADR + SS group compared with ADR group.
Effects of Se Deficiency and/or Se Supplementation on ADR-Induced Cardiac Dysfunctions
Plasma BNP
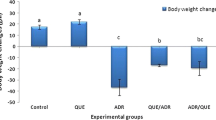
As demonstrated in Fig. 1, it was showed by Triage BNP assay that plasma BNP level increased significantly in LS or ADR group compared with control. A more dramatic increase of plasma BNP was found in ADR + LS group. After Se supplementation by intraperitoneal injections, a drop of plasma BNP level in ADR + SS group was indentified compared with ADR.

Effects of Se deficiency/supplementation and/or adriamycin on plasma BNP level. Plasma BNP concentration (pg/ml) was examined by Triage BNP Assay. Columns indicate BNP concentrations in control, LS, ADR, ADR + LS, and ADR + SS, respectively. Values are presented as mean ± SD. a Values are significantly different from control; b value is significantly different from LS (P < 0.01); c value is significantly different from ADR [*P < 0.05; **P < 0.01; #P < 0.001]
Echocardiographic and Hemodynamic Determination
Echocardiographic and hemodynamic parameters including LVEDD, LVESD, LVEF, LVFS, LVSP, LVDP, and HR were detected and calculated in this study as shown in Tables 3 and 4. An overall increase of LVEDD, LVESD, and LVDP accompanied by an overall decrease of LVEF, LVFS, LVSP, and HR were found in LS, ADR, and ADR + LS groups. However, it appeared to be more significant increase of LVEDD, LVESD, and LVDP, decrease of LVEF, LVFS, LVSP, and HR in ADR + LS group compared with LS or ADR groups. Significant recovery of cardiac function marked by echocardiographic and hemodynamic parameters was found in ADR + SS group compared with ADR group, which was evidenced by restoring of LVEDD, LVESD, LVEF, LVFS, LVSP, LVDP, and HR after Se supplementation.
Effects of ADR, Se Deficiency, and Se Supplementation on Expression of KATP Subunits
Real-time PCR and Western blotting were employed to detect the changes of expression of Kir6.2 and SUR2A in the present study. As shown in Figs. 2a and 3a, mRNA and protein expression of SUR2A in cardiac tissue was impaired by treatment of Se deficiency and/or adriamycin in LS, ADR, and ADR + LS groups. Co-administration of Se deficiency and ADR resulted in more dramatic decrease of SUR2A gene expression in ADR + LS group compared with LS or ADR group. mRNA and protein levels in cardiac tissue of rats received injection of Se in ADR + SS group were significantly recovered compared with those in ADR group. Similarly, as demonstrated in Figs. 2b and 3b, expression at transcriptional and translational levels of another subunit of cardiac KATP, Kir6.2, decreased significantly in LS, ADR, and ADR + LS groups compared with control group. Decreasing expression of Kir6.2 in ADR + LS group was enhanced by co-administration of Se deficiency and adriamycin compared with ADR or LS group. However, it seemed that supplementation of Se reversed the decreasing expression of Kir6.2 in ADR + SS group compared with ADR group.

Effects of Se deficiency/supplementation and/or adriamycin on mRNA expression of KATP subunits in cardiac tissue. Total mRNA was extracted from cardiac tissue and then detected by real-time PCR with designed primers for KATP subunits SUR2A and Kir6.2 in Table 1. mRNA expression of β-actin was introduced to normalize mRNA expression of SUR2A and Kir6.2. a Analysis of expression of SUR2A normalized by β-actin. Columns in graph present the ratio of SUR2A/β-actin as mean ± SD (n = 6) of control, LS, ADR, ADR + LS, and ADR + SS, respectively. b Analysis of expression of Kir6.2 normalized by β-actin. Columns in graph present the ratio of Kir6.2/β-actin as mean ± SD (n = 6) of control, LS, ADR, ADR + LS, and ADR + SS, respectively. a Indicates significant differences when compared with control; b indicates significant differences when compared with LS; c indicates significant differences when compared with ADR [*P < 0.05; **P < 0.01; #P < 0.001]

Effects of Se deficiency/supplementation and/or adriamycin on protein expression of KATP subunits in cardiac tissue. Sample protein was extracted, separated, and detected by specific antibodies against KATP subunits SUR2A and Kir6.2. The expression of SUR2A and Kir6.2 was normalized by β-actin in the same sample. Darkness of immunoblots stands for expression level of protein. a Western blotting of SUR2A. Immunoblots stands for control, LS, ADR, ADR + LS, and ADR + SS from left side to right side, respectively. b Western blotting of Kir6.2. Immunoblots stands for control, LS, ADR, ADR + LS, and ADR + SS from left side to right side, respectively
Effects of ADR, Se Deficiency, and Se Supplementation on GPx Activity
As shown in Fig. 4, activity of GPx in LS, ADR, and ADR + LS group decreased significantly compared with control. It was observed that in ADR + LS group, activity of GPx dropped more apparently compared with LS or ADR group. However, a noticeable recovery of GPx activity in ADR + SS group was confirmed by GPx activity assay when compared with ADR group.

Effects of Se deficiency/supplementation and/or adriamycin on GPx activity in cardiac tissue. Spectrophotometrical method was utilized to examine the activity of GPx in cardiac tissue. Values indicated by columns in graph are presented as mean ± SD (n = 6). Columns from left side to right side stand for control, LS, ADR, ADR + LS, and ADR + SS, respectively. a Indicates significant differences when compared with control; b indicates significant differences when compared with LS; c indicates significant differences when compared with ADR [*P < 0.05; **P < 0.01; #P < 0.001]
Discussion
As a widely used chemotherapy agent, ADR is also well-known for its cardiac toxicity [22]. In this study, impaired cardiac function was confirmed in ADR-treated rats. Se deficiency is considered as an indicator for cardiovascular diseases [23]; measurements performed in the present study revealed cardiac dysfunctions in rats fed with low-Se diet. Considering these two cardiac harmful factors together, it motivated us to investigate whether heart is more susceptible to ADR-induced damage during Se deficiency, and if Se supplementation which plays a role in cardiac protection [24] alleviates ADR-induced cardiac toxicity. Mechanically, KATP has been proved cardioprotective in KATP disrupted animals [25], so it is logical for us to speculate that down-regulation of KATP maybe accounted for impaired cardiac function in Se deficiency and/or ADR-treated rats, and correspondingly, up-regulation of KATP may be the mechanism of recovery of cardiac function after Se supplementation.
In this study, cardiac function was measured by echocardiographic and hemodynamic determination. An overall increase of LVEDD, LVESD, and LVDP accompanied by an overall decrease of LVEF, LVFS, LVSP, and HR indicate that both left ventricular systolic and diastolic functions are impaired in rats [21]. In response to pressure overload and/or volume expansion stimulation, BNP is released from cardiac ventricles dramatically. In patients with left ventricular dysfunction, elevation of plasma BNP level is usually used to evaluate the severity and clinical prognosis [26]. It is considered that plasma BNP level is reliable in monitoring cardiac function [27].
Adriamycin (doxorubicin) which belongs to anthracycline drug family has been shown to be an effective antitumor chemotherapeutic agent [28]. Even nowadays, adriamycin is still being widely used in treatment of many kinds of hematologic malignancies and solid tumors such as leukemia, multiple myeloma, breast cancer, lung cancer, and so on. Though adriamycin’s strong anti-tumor therapeutic effects have been confirmed, it was described early in clinical practice that cardiac dysfunction was one of the complications after administration of adriamycin [29]. In 1,697 patients with non-Hodgkin’s lymphomas, 147 (3.2 %) patients who received an adriamycin-based treatment developed acute cardiac complications, including acute heart failure, myocardial infarction, atrial fibrillation, and myocarditis [30]. In the present study, after intrapertoneal injection of adriamycin, measurements confirmed adriamycin-induced cardiac dysfunction in ADR group. While adriamycin binds to DNA, released electrons convert the drug from quinone from to semiquinone from. During the reaction, superoxide anions are produced, which induce further reactive oxygen species (ROS) generation [31]. It is proposed that formation of ROS is responsible for cardiac injury during chemotherapy [32]. As a major peroxide scavenging enzyme, decreased GPx activity has been described under condition of oxidative stress [33]. In the present study, GPx activity in cardiac tissue treated by adriamycin decreased significantly, indicating that adriamycin-induced cardiac dysfunction was associated with oxidative stress.
In this study, we demonstrated decreased cardiac function in rats received low-Se diet by plasma BNP and echocardiographic and hemodynamic determinations. Se deficiency or low Se status is always mentioned crucial in development of heart diseases. Early population-based clinical study showed that low selenium level was associated with cardiovascular outcomes [34]. Low selenium status, which existed before observation of clinical cardiac events, was amplified by acute coronary syndrome [35]. In a recent prospective cohort study of patients with coronary artery disease, individual baseline serum selenium concentration was inversely associated with mortality of acute coronary syndrome. Low serum selenium was considered independent of classic risk factors including biomarkers of necrosis, LVEF, and so on of acute coronary syndrome [4]. In an animal study, Se deficiency was proved associated with pronounced worsening of cardiac functional parameters and cardiac hypertrophy, associated with remarkable decrease of GPx activity in cardiac tissue [36]. These results are in accordance with ours: increasing serum BNP level, LVEDD, LVESD, and LVDP, decreasing LVEF, LVFS, LVSP, and HR accompanied by decreasing GPx activity was found in low-Se-diet-treated rats.
It seems that administration of low-Se diet and adriamycin share the same pathway of impairment of GPx activity in worsening cardiac functions. On one hand, cancer patients are found lack of micronutrients including Se. It was mentioned that the serum Se concentration in patients with urinary or larynx cancer was lower than normal control [37]. On the other hand, low serum Se concentration is an independent risk factor for coronary artery disease [4]. Thus, it is interesting and of clinical significance to investigate whether chemotherapy exacerbates cardiac function in patients with low Se status which indicates potential or existing heart diseases. In this study, co-administration of low-Se diet and intraperitoneal injections of adriamycin was applied to rats to mimic such certain clinical situation. Results in this study showed a more significant worsening of cardiac function in ADR + LS than in ADR or LS. Further, GPx activity assay confirmed more significant impairment of GPx activity after co-administration of adriamycin and low-Se diet, proposing that stimulated oxidative stress which depresses GPx activity was exerted by both Se deficiency and adriamycin. These results indicate that Se-deficient rats are more sensitive to cardiac toxicity of adriamycin, suggesting when cardiac toxic chemotherapy agents are employed, cancer patients with low Se status should be treated more cautiously.
As a regimen, intraperitoneal administration of Se was applied to rats receiving treatment of adriamycin which was proved cardiac toxic in ADR group in the present study. Cardiac function examination of BNP and echocardiographic and hemodynamic parameters showed that the adriamycin-induced cardiac dysfunction was attenuated significantly by supplementation of Se. And simultaneously, decreased GPx activity was restored by supplementation of Se, indicating that Se alleviated cardiac dysfunction by increasing activity of GPx which was one of the major ROS scavengers [38]. This result is coincided with previous studies on association between Se and cardiac dysfunctions [6, 24, 36, 39, 40]. Se is essential in biosynthesis of selenoenzymes including six groups of GPx (GPx 1–6), which play an important role in protecting cells against oxidative injury caused by ROS in certain pathological conditions [41]. Se supplementation may promote GPx activity by providing substrate for synthesis of GPx. Therefore, in chemotherapy of patients with cancer, Se containing drugs or compounds may be able to be used to enhance resistance to chemotherapy-induced cardiac toxicity.
Furthermore, this study explored possible mechanism of cardiac dysfunction induced by adriamycin and/or low-Se diet. Molecularly, KATP expressed in cardiomyocytes is a heteromultimer with octameric conformation. Data from animal models have indentified cardiac KATP is composed of tow subunits—Kir6.2 (encoded by KCNJ11) and SUR2A (encoded by ABBC9) [42, 43]. Generally, it is well accepted that KATP has a cardioprotective property in certain pathological conditions such as myocardial ischemia [44]. 5-HD, a KATP channel blocker, was applied in a number of studies to testify the role of KATP in ischemic cardiac dysfunctions. These studies showed that the cardiac protective effects were inhibited after administration of 5-HD [45]. Decreased expression of cardiac KATP was proposed as one of the mechanisms for cardiac dysfunction in diabetic rats. Similar down-regulation of KATP expression was indentified in high-glucose incubated myocytes in the same study [46]. In the present study, decreasing expression of Kir6.2 and SUR2A were detected by real-time PCR and Western blotting in cardiac tissue from rats received treatment of adriamycin and/or Se deficiency. Therefore, our results suggest that decreased expression of cardiac KATP impairs cardioprotective effects against adriamycin and/or Se deficiency, leading to cardiac dysfunction.
Interestingly, whether in myocardial ischemia, hyperglycemia, adriamycin-, or Se-deficiency-induced cardiac dysfunction, oxidative stress always plays an important part. Studies have revealed malfunctions of ion channels in status of oxidative stress. Administration of H2O2 which is a strong oxidant-induced cytosolic Ca2+ influx in neuronal PC12 cells [47] and TRPM2 (transient receptor potential melastain 2) current in ovary cells [48]. In high-glucose-treated myocytes, previous study has illustrated that cardiac injury is caused by excessively increasing production of ROS [49]. Clearing of ROS is seemed to protect cell from injury, especially for myocyte which is more susceptible to oxidative stress. After application of Se as a free radical scavenger, this study demonstrated that the activity of GPx elevated significantly, indicating that supplement of Se inhibited oxidative stress in myocytes; we also found that the expression of Kir6.2 and SUR2A was restored to perform cardioprotective effects in adriamycin-treated rats after supplementation of Se. These results suggest that Se attenuates adriamycin-induced cardiac dysfunction by restoring expression of KATP via elevating activity of GPx to depress ROS generation. However, the specific mechanism(s) of inhibiting KATP expression by ROS and induction of KATP expression by Se (or other anti-oxidants) is still unclear. More studies are necessary to illustrate the change of KATP currents, structure, and signal transduction in cardiac dysfunction in the very near future.
Conclusions
This study may provide a new recognition of possible mechanism of Se deficiency and/or adriamycin-induced cardiac dysfunction and cardiac protective effects of Se supplementation:
-
1.
Decreased expression of KATP is involved in adriamycin- and/or Se-deficiency-induced cardiac dysfunction.
-
2.
Se deficiency exacerbates adriamycin-induced cardiac dysfunction by future inhibition of KATP expression.
-
3.
Se supplementation seems to protect against adriamycin-induced cardiac dysfunction via restoring KATP expression.
References
Singal PK, Iliskovic N (1998) Doxorubicin-induced cardiomyopathy. N Engl J Med 339(13):900–905. doi:10.1056/NEJM199809243391307
Shan K, Lincoff AM, Young JB (1996) Anthracycline-induced cardiotoxicity. Ann Intern Med 125(1):47–58
Yang J, Wang T, Wu C, Liu C (2010) Selenium level surveillance for the year 2007 of Keshan disease in endemic areas and analysis on surveillance results between 2003 and 2007. Biol Trace Elem Res 138(1–3):53–59. doi:10.1007/s12011-010-8609-1
Lubos E, Sinning CR, Schnabel RB, Wild PS, Zeller T, Rupprecht HJ, Bickel C, Lackner KJ, Peetz D, Loscalzo J, Munzel T, Blankenberg S (2010) Serum selenium and prognosis in cardiovascular disease: results from the AtheroGene study. Atherosclerosis 209(1):271–277. doi:10.1016/j.atherosclerosis.2009.09.008
Krim SR, Campbell P, Lavie CJ, Ventura H (2012) Micronutrients in chronic heart failure. Curr Heart Fail Rep. doi:10.1007/s11897-012-0118-4
Venardos K, Harrison G, Headrick J, Perkins A (2004) Effects of dietary selenium on glutathione peroxidase and thioredoxin reductase activity and recovery from cardiac ischemia-reperfusion. J Trace Elem Med Biol 18(1):81–88. doi:10.1016/j.jtemb.2004.01.001
Manati W, Vaillant F, Bost M, Maffre V, Belhani D, Descotes J, Tabib A, Bui-Xuan B, Hamdan L, Timour Q (2009) Protective role of selenium supplementation against cardiac lesions induced by the combination of levomepromazine and risperidone in the rabbit. Hum Exp Toxicol 28(8):461–467. doi:10.1177/0960327109106968
Miki T, Seino S (2005) Roles of KATP channels as metabolic sensors in acute metabolic changes. J Mol Cell Cardiol 38(6):917–925. doi:10.1016/j.yjmcc.2004.11.019
Kurachi Y, Yamada M (2005) Relationship between function and structure of ATP-sensitive K+ (KATP) channels. Nihon Yakurigaku Zasshi 126(5):311–316
Zingman LV, Alekseev AE, Hodgson-Zingman DM, Terzic A (2007) ATP-sensitive potassium channels: metabolic sensing and cardioprotection. J Appl Physiol 103(5):1888–1893. doi:10.1152/japplphysiol.00747.2007
Terzic A, Jahangir A, Kurachi Y (1995) Cardiac ATP-sensitive K+ channels: regulation by intracellular nucleotides and K+ channel-opening drugs. Am J Physiol 269(3 Pt 1):C525–C545
Tanner GR, Lutas A, Martinez-Francois JR, Yellen G (2011) Single K ATP channel opening in response to action potential firing in mouse dentate granule neurons. J Neurosci 31(23):8689–8696. doi:10.1523/jneurosci.5951-10.2011
Philip-Couderc P, Tavares NI, Roatti A, Lerch R, Montessuit C, Baertschi AJ (2008) Forkhead transcription factors coordinate expression of myocardial KATP channel subunits and energy metabolism. Circ Res 102(2):e20–e35. doi:10.1161/CIRCRESAHA.107.166744
Maack C, Dabew ER, Hohl M, Schafers HJ, Bohm M (2009) Endogenous activation of mitochondrial KATP channels protects human failing myocardium from hydroxyl radical-induced stunning. Circ Res 105(8):811–817. doi:10.1161/CIRCRESAHA.109.206359
Kramer PR, Wray S (2002) 17-Beta-estradiol regulates expression of genes that function in macrophage activation and cholesterol homeostasis. J Steroid Biochem Mol Biol 81(3):203–216
Tanguy S, Grauzam S, de Leiris J, Boucher F (2012) Impact of dietary selenium intake on cardiac health: experimental approaches and human studies. Mol Nutr Food Res 56(7):1106–1121. doi:10.1002/mnfr.201100766
Xin YF, Zhou GL, Deng ZY, Chen YX, Wu YG, Xu PS, Xuan YX (2007) Protective effect of Lycium barbarum on doxorubicin-induced cardiotoxicity. Phytother Res 21(11):1020–1024. doi:10.1002/ptr.2186
Dursun N, Taskin E, Yerer Aycan MB, Sahin L (2011) Selenium-mediated cardioprotection against adriamycin-induced mitochondrial damage. Drug Chem Toxicol 34(2):199–207. doi:10.3109/01480545.2010.538693
Gu L, Pandey V, Geenen DL, Chowdhury SA, Piano MR (2008) Cigarette smoke-induced left ventricular remodelling is associated with activation of mitogen-activated protein kinases. Eur J Heart Fail 10(11):1057–1064. doi:10.1016/j.ejheart.2008.08.009
Ma J, Qian J, Ge J, Zeng X, Sun A, Chang S, Chen Z, Zou Y (2012) Changes in left ventricular ejection fraction and coronary flow reserve after coronary microembolization. Arch Med Sci 8(1):63–69. doi:10.5114/aoms.2012.27283
Jiang K, Shui Q, Xia Z, Yu Z (2004) Changes in the gene and protein expression of K(ATP) channel subunits in the hippocampus of rats subjected to picrotoxin-induced kindling. Brain Res Mol Brain Res 128(1):83–89. doi:10.1016/j.molbrainres.2004.06.005
Cui Y, Piao CS, Ha KC, Kim DS, Lee GH, Kim HK, Chae SW, Lee YC, Park SJ, Yoo WH, Kim HR, Chae HJ (2010) Measuring adriamycin-induced cardiac hemodynamic dysfunction with a proteomics approach. Immunopharmacol Immunotoxicol 32(3):376–386. doi:10.3109/08923970903440168
McKeag NA, McKinley MC, Woodside JV, Harbinson MT, McKeown PP (2012) The role of micronutrients in heart failure. J Acad Nutr Diet 112(6):870–886. doi:10.1016/j.jand.2012.01.016
Danesi F, Malaguti M, Nunzio MD, Maranesi M, Biagi PL, Bordoni A (2006) Counteraction of adriamycin-induced oxidative damage in rat heart by selenium dietary supplementation. J Agric Food Chem 54(4):1203–1208. doi:10.1021/jf0518002
Hu X, Xu X, Huang Y, Fassett J, Flagg TP, Zhang Y, Nichols CG, Bache RJ, Chen Y (2008) Disruption of sarcolemmal ATP-sensitive potassium channel activity impairs the cardiac response to systolic overload. Circ Res 103(9):1009–1017. doi:10.1161/CIRCRESAHA.107.170795
Gaggin HK, Januzzi JL Jr (2013) Biomarkers and diagnostics in heart failure. Biochim Biophys Acta. doi:10.1016/j.bbadis.2012.12.014
Jourdain P, Jondeau G, Funck F, Gueffet P, Le Helloco A, Donal E, Aupetit JF, Aumont MC, Galinier M, Eicher JC, Cohen-Solal A, Juilliere Y (2007) Plasma brain natriuretic peptide-guided therapy to improve outcome in heart failure: the STARS-BNP Multicenter Study. J Am Coll Cardiol 49(16):1733–1739. doi:10.1016/j.jacc.2006.10.081
Tacar O, Sriamornsak P, Dass CR (2013) Doxorubicin: an update on anticancer molecular action, toxicity and novel drug delivery systems. J Pharm Pharmacol 65(2):157–170. doi:10.1111/j.2042-7158.2012.01567.x
Lefrak EA, Pitha J, Rosenheim S, Gottlieb JA (1973) A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer 32(2):302–314
Wojnowski L, Kulle B, Schirmer M, Schluter G, Schmidt A, Rosenberger A, Vonhof S, Bickeboller H, Toliat MR, Suk EK, Tzvetkov M, Kruger A, Seifert S, Kloess M, Hahn H, Loeffler M, Nurnberg P, Pfreundschuh M, Trumper L, Brockmoller J, Hasenfuss G (2005) NAD(P)H oxidase and multidrug resistance protein genetic polymorphisms are associated with doxorubicin-induced cardiotoxicity. Circulation 112(24):3754–3762. doi:10.1161/circulationaha.105.576850
Zhang YW, Shi J, Li YJ, Wei L (2009) Cardiomyocyte death in doxorubicin-induced cardiotoxicity. Arch Immunol Ther Exp (Warsz) 57(6):435–445. doi:10.1007/s00005-009-0051-8
Zhang S, Liu X, Bawa-Khalfe T, Lu LS, Lyu YL, Liu LF, Yeh ET (2012) Identification of the molecular basis of doxorubicin-induced cardiotoxicity. Nat Med 18(11):1639–1642. doi:10.1038/nm.2919
Miyamoto Y, Koh YH, Park YS, Fujiwara N, Sakiyama H, Misonou Y, Ookawara T, Suzuki K, Honke K, Taniguchi N (2003) Oxidative stress caused by inactivation of glutathione peroxidase and adaptive responses. Biol Chem 384(4):567–574. doi:10.1515/BC.2003.064
Salonen JT, Alfthan G, Huttunen JK, Pikkarainen J, Puska P (1982) Association between cardiovascular death and myocardial infarction and serum selenium in a matched-pair longitudinal study. Lancet 2(8291):175–179
Kok FJ, Hofman A, Witteman JC, de Bruijn AM, Kruyssen DH, de Bruin M, Valkenburg HA (1989) Decreased selenium levels in acute myocardial infarction. JAMA 261(8):1161–1164
Lymbury RS, Marino MJ, Perkins AV (2010) Effect of dietary selenium on the progression of heart failure in the ageing spontaneously hypertensive rat. Mol Nutr Food Res 54(10):1436–1444. doi:10.1002/mnfr.201000012
Borawska MH, Socha K, Lazarczyk B, Czyzewska E, Markiewicz R, Darewicz B (2009) The effects of diet on selenium concentration in serum in patients with cancer. Nutr Cancer 61(5):629–633. doi:10.1080/01635580902825555
Dokic I, Hartmann C, Herold-Mende C, Regnier-Vigouroux A (2012) Glutathione peroxidase 1 activity dictates the sensitivity of glioblastoma cells to oxidative stress. Glia 60(11):1785–1800. doi:10.1002/glia.22397
Bordoni A, Biagi PL, Angeloni C, Leoncini E, Danesi F, Hrelia S (2005) Susceptibility to hypoxia/reoxygenation of aged rat cardiomyocytes and its modulation by selenium supplementation. J Agric Food Chem 53(2):490–494. doi:10.1021/jf049426d
Yu H, Liu J, Li J, Zang T, Luo G, Shen J (2005) Protection of mitochondrial integrity from oxidative stress by selenium-containing glutathione transferase. Appl Biochem Biotechnol 127(2):133–142
Tinggi U (2008) Selenium: its role as antioxidant in human health. Environ Health Prev Med 13(2):102–108. doi:10.1007/s12199-007-0019-4
Quindry JC, Miller L, McGinnis G, Kliszczewicz B, Irwin JM, Landram M, Urbiztondo Z, Nanayakkara G, Amin R (2012) Ischemia reperfusion injury, KATP channels, and exercise-induced cardioprotection against apoptosis. J Appl Physiol 113(3):498–506. doi:10.1152/japplphysiol.00957.2011
Ponce-Balbuena D, Rodriguez-Menchaca AA, Lopez-Izquierdo A, Ferrer T, Kurata HT, Nichols CG, Sanchez-Chapula JA (2012) Molecular mechanisms of chloroquine inhibition of heterologously expressed Kir6.2/SUR2A channels. Mol Pharmacol 82(5):803–813. doi:10.1124/mol.112.079152
Hsu CY, Fang SY, Chen YZ, Roan JN, Chang SW, Huang CC, Liu YC, Lam CF, Tsai YC (2012) Cardiovascular protection of activating KATP channel during ischemia-reperfusion acidosis. Shock 37(6):653–658. doi:10.1097/SHK.0b013e318252caf6
Wang ZF, Wang NP, Harmouche S, Philip T, Pang XF, Bai F, Zhao ZQ (2013) Postconditioning promotes the cardiac repair through balancing collagen degradation and synthesis after myocardial infarction in rats. Basic Res Cardiol 108(1):318. doi:10.1007/s00395-012-0318-9
Chen ZC, Cheng YZ, Chen LJ, Cheng KC, Li Y, Cheng J (2012) Increase of ATP-sensitive potassium (K(ATP)) channels in the heart of type-1 diabetic rats. Cardiovasc Diabetol 11:8. doi:10.1186/1475-2840-11-8
Demirci S, Kutluhan S, Naziroglu M, Uguz AC, Yurekli VA, Demirci K (2013) Effects of selenium and topiramate on cytosolic ca(2+) influx and oxidative stress in neuronal PC12 cells. Neurochem Res 38(1):90–97. doi:10.1007/s11064-012-0893-z
Naziroglu M, Ozgul C, Kucukayaz M, Cig B, Hebeisen S, Bal R (2013) Selenium modulates oxidative stress-induced TRPM2 cation channel currents in transfected Chinese hamster ovary cells. Basic Clin Pharmacol Toxicol 112(2):96–102. doi:10.1111/j.1742-7843.2012.00934.x
Younce C, Burmeister MA, Ayala JE (2013) Exendin-4 attenuates high glucose-induced cardiomyocyte apoptosis via inhibition of endoplasmic reticulum stress and activation of SERCA2a. Am J Physiol Cell Physiol. doi:10.1152/ajpcell.00248.2012
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liu, ZW., Niu, XL., Chen, KL. et al. Selenium Attenuates Adriamycin-Induced Cardiac Dysfunction via Restoring Expression of ATP-Sensitive Potassium Channels in Rats. Biol Trace Elem Res 153, 220–228 (2013). https://doi.org/10.1007/s12011-013-9641-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-013-9641-8