
Abstract
Background
Acetabular revision THA with use of a large (jumbo) cup is an effective treatment for many cavitary and segmental peripheral bone defects. However, the jumbo cup may result in elevation of the hip center and protrusion through the anterior acetabular wall as a result of the oversized geometry of the jumbo cup compared with the physiologic acetabulum.
Questions/purposes
The purpose of this computer simulation was to determine how much elevation of the hip center and anterior wall protrusion occurs in revision THA with use of a jumbo cup technique in which the inferior edge of the jumbo cup is placed at the inferior acetabular rim and the superior edge of the jumbo cup is placed against host bone at the superior margin of a posterosuperior bone defect.
Methods
Two hundred sixty-five pelvic CT scans were analyzed by custom CT analytical software. The computer simulated oversized reaming. The vertical and anterior reamer center shifts were measured, and anterior column bone removal was determined.
Results
The computer simulation demonstrated that the hip center shifted 0.27 mm superiorly and 0.02 mm anteriorly, and anterior column bone removal increased 0.86 mm for every 1-mm increase in reamer diameter.
Conclusions
Our results indicate that the jumbo cup technique results in hip center elevation despite placement of the cup adjacent to the inferior acetabulum. For a hypothetical increase from a 54-mm socket to a 72-mm socket, as one might see in the context of the revision of a failed THA, our model would predict an elevation of the hip center of approximately 5 mm and loss of approximately 15 mm of anterior column bone. This suggests that an increase in femoral head length may be needed to compensate for the hip center elevation caused by the use of a large jumbo cup in revision THA. A jumbo cup may also result in protrusion through the anterior wall.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The durability and versatility of jumbo, hemispherical, cementless, acetabular cups in managing cavitary and segmental bone defects in the revision THA setting are well documented [3, 10, 11, 15, 18]. Jumbo cups offer several advantages over other methods of acetabular revision. First, they provide a large amount of contact area of host bone with the porous implant surface facilitating reliable biological fixation [12]. Additionally, this method allows for a surgical technique with use of hemispherical reamers and screw fixation, which is similar to that used for primary THA. Furthermore, many commonly encountered bone deficiencies can be filled by the large size of the jumbo shell and cancellous graft, oftentimes eliminating the need for bulk allograft or augments. The jumbo cup that fills the gap from the superior bone defect to the inferior acetabulum provides an alternative to placing a cup into the superior defect (high hip center) or use of an augment above a component placed in the anatomic acetabulum [2].
However, use of the jumbo cup technique requires reaming and preparation of the acetabular surface to fit an implant that is often much larger than the native acetabulum. The increased diameter of the jumbo cup relative to the native acetabulum may result in elevation of the hip center, which has been associated with altered hip biomechanics and hip instability [4, 16, 17].
At revision, most segmental acetabular bone defects are located superiorly and posteriorly. When reaming the acetabulum with these defects into a hemispherical shape, the large diameter required to span the distance from the superior defect to the inferior acetabulum results in an equal AP reaming dimension. Reaming through the medial wall and placement of a cup medial to Kohler’s line to gain better superior coverage has been advocated in the treatment of hip dysplasia and revision THA without adverse consequences [6, 7, 9]. However, reaming through the anterior wall should be avoided because this can result in impingement between the anterior cup edge and iliopsoas tendon [5, 14]. We therefore used a computer model to test the following questions: (1) does revision THA with a jumbo cup result in elevation of the hip center with use of a surgical technique in which the goal is to avoid superior placement of the cup and, if so, by how much; and (2) how much anterior column bone loss is caused by progressive reaming for a jumbo cup while preserving the integrity of the posterior acetabular wall?
Patients and Methods
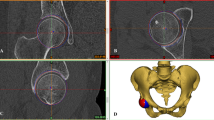
To conduct the computer simulation, 265 pelvic CT scans consisting of 158 males and 107 females were converted to virtual three-dimensional bones. The average native acetabular diameter was 52.0 mm (SD = 4.0 mm; 52.4 mm in males, SD = 2.8 mm and 46.4 mm, SD = 2.6 mm in females). All the source CT scans were obtained from a skeletally mature white population. The mean age of the patients was 65 years (range, 30–93 years; mean male, 65 years; mean female, 66 years). These images were analyzed by custom CT analytical software (SOMATM Version 3.2; Stryker, Mahwah, NJ, USA). Using this software, we were able to simulate oversized reaming. Four distinct points, located in and around the acetabular margins, were used to determine the reamer sphere. Points 1 to 3 were located at the inferior and inferomedial acetabular margins, and Point 4 was located superiorly and posteriorly in the acetabulum to simulate a bony defect in this location (Fig. 1). Point 4 was placed at 10%, 20%, 30%, 40%, 50%, and 60% of the distance from the superoposterior margin of the acetabular rim to the sciatic notch to simulate bony defects of increasing size. Using this computerized model, we simulated progressively oversized reaming without violating the inferior wall and significant parts of medial acetabular wall.

The computer simulation of jumbo cup acetabular reaming was constructed from a sphere containing three fixed points along the inferior acetabulum and a fourth point that represented the extent of a posterosuperior segmental bone defect. The posterosuperior point was placed at 10%, 20%, 30%, 40%, 50%, and 60% of the distance from the superoposterior margin of the acetabular rim to the sciatic notch to simulate bony defects of increasing size.
Translations in the center of the reamer in the vertical and AP planes with progressive reaming were measured. The vertical reamer center shift was measured from the frontal plane, whereas the AP shift was measured from the sagittal plane. The amount of anterior column bone removal was estimated by finding the difference between the radius of the reamer sphere (measured from the center of the reamer sphere to its anterior edge) and the distance from the hip center to the anteroinferior iliac spine. Student’s t-tests were performed to evaluate sex differences in vertical and anterior shifts with increased reaming and to evaluate sex differences in anterior column bone removal.
Results
Results from the computer simulation demonstrated that the jumbo cup technique can result in elevation of the hip center. The average pelvic size in the computer simulation had a mean native acetabular diameter in males of 52.4 mm and 46.4 mm in females (p = 1.8E−47). The computer simulation predicted that the hip center shifted both superiorly and anteriorly as the reamer size increased, and there were statistically significant differences between males and females (Fig. 2). The hip center shifted superiorly by 0.28 mm for every 1-mm increase in reamer size with a more pronounced difference in women than men (male = 0.27 mm, female = 0.29 mm; p = 0.0098).

Graph illustrating the average jumbo cup hip center shift superiorly and anteriorly in male and females hips as a function of increasing reamer diameter. HC = hip center.
The hip center also shifted anteriorly by 0.028 mm for every 1-mm increase in reamer size (male = 0.013 mm, female = 0.042 mm; p = 2.36E−9). Based on the computer simulation, every 1-mm increase in the size of the reamer corresponded to an average of 0.82 mm of anterior column bone removal (male = 0.82 mm, female = 0.82 mm; p = 0.269) (Fig. 3).

Graph illustrating the average anterior column bone removal (y) as a function of increasing reamer diameter.
Discussion
Several studies have shown the jumbo cementless acetabular cup to be a durable and versatile choice for the management of bony acetabular defects in revision THA [3, 10, 11, 15, 18]. Jumbo cups offer several advantages over other methods of acetabular revision. They provide a maximal area of contact between host bone and the porous implant surface facilitating reliable biological fixation [12] and they allow for a relatively straightforward and reproducible surgical technique of hemispherical reaming and screw fixation of the implant. The large size of the jumbo shell can also compensate for areas of bone loss often eliminating the need for bulk allograft or metal augments. However, the jumbo cup technique requires preparation of the acetabular surface to fit a hemispherical implant, which is larger in diameter than the native acetabulum. We asked whether the use of a jumbo cup would result in hip center elevation in revision THA. Reaming in a superior direction may result in placement of the cup above the anatomic acetabulum and result in elevation of the hip center. Additionally, the use of a large acetabular cup alone may result in elevation of the hip center resulting from the increased radius of the jumbo cup. The computer simulation, which maintained positioning of the revision cup along the inferior and posterior acetabulum, demonstrated an anterior, superior, and lateral hip center shift as reamer size increased.
This study has several limitations. First, the model is based on average pelvic and acetabular anatomy obtained from a database of pelvic CT scans and may not represent the variation in individual anatomy encountered in different THA revision settings. For example, in our model we maintain positioning of the revision cup along the inferior acetabulum, although medialization or high placement of the cup are techniques that are often necessary in the clinical setting. Second, our model does not account for how various other characteristics of the revision such as cup orientation or liner offset will affect the measured variables. Third, the results of this computer simulation are not validated by radiographic data, so caution should be taken when translating our findings directly to the clinical setting. However, our model was intended to provide quantitative measurements about the relative hip center elevation and anterior bone loss with placement of the inferior cup against the inferior acetabular rim in an effort to help guide intraoperative decision-making in revision THA. For example, when using a jumbo cup 10 mm larger in diameter than the native acetabulum, the surgeon may choose to add one head length (4 mm) to compensate for the head center elevation or when a jumbo cup more than 15 mm larger than the native acetabulum is required, the surgeon may choose to use a superior augment above a cup the size of the native acetabulum or higher hip center to avoid reaming through the anterior wall.
The hip center shift may result in altered hip biomechanics and soft tissue laxity. A retrospective study involving 79 THA revisions by Dou et al. [8] reported that the acetabular side significantly contributes to hip center elevation and leg length discrepancies after revision THA. In addition to its role in leg length changes, an elevated hip center also results in suboptimum biomechanics of the hip [4, 17]. Delp et al. [4] showed that superolateral placement of the hip center (2 cm superior and 2 cm lateral) decreases the moment arm of the hip abductors by an average of 28%, thus reducing force generating capacity. Lachiewicz and Soileau [13] reported a dislocation rate of 10% after jumbo cup revision THA, which was the most common complication observed in their series. Given the results of our computer simulation, and established data that point to hip center shifts as contributors to suboptimal hip biomechanics, it is plausible that shifts in the hip center may have contributed to the incidence of dislocation in jumbo cup revision THA seen in the Lachiewecz and Soileu series [13]. However, multiple factors can contribute to hip dislocation and further clinical studies need to be undertaken to determine the effect of hip center elevation on instability. Increased femoral head length, polyethylene liner exchange, or use of modular systems may all be helpful to compensate for the elevated hip center.
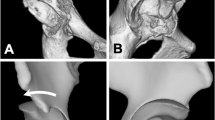
Another potential consequence of the use of a jumbo cup is that, secondary to its size, it may protrude through the anterior wall of the acetabulum and lead to problems stemming from soft tissue impingements such as iliopsoas tendonitis [5, 14]. Iliopsoas tendonitis has been associated with inadequate anteversion of the cup in THA resulting in prominence of the anterior cup edge, which impinges against the iliopsoas tendon causing groin pain. The incidence of iliopsoas impingement after THA has been reported to be as high as 4.3% [1]. One purpose of this investigation was to use a computer simulation in which the medial wall of the acetabulum was not violated to investigate whether the jumbo cup technique for revision THA resulted in protrusion through the anterior acetabular wall and to measure the degree of anterior column bone loss caused by progressive reaming for an oversized cup. Our results indicate that anterior bone loss and protrusion of the anterior edge of the jumbo cup through the anterior wall can occur when the inferior edge of the jumbo cup is positioned against the inferior acetabulum. To preserve the anterior wall, other techniques such as higher placement of a smaller cup or use of a superior augment above an anatomically positioned cup can be used. Reaming medially through the medial wall to gain better superior coverage has also been used successfully as an alternative to a superior augment or bone graft [6, 7, 9]. The final decision of which technique to use is made intraoperatively based on a direct assessment of the remaining bone and acetabular anatomy. Our data on the effect of head center shift and anterior bone loss with increasing reamer size are intended to provide quantitative information, which may be helpful in the intraoperative decision-making process during revision THA.
References
Bricteux S, Beguin L, Fessy MH. [Iliopsoas impingement in 12 patients with a total hip arthroplasty] [in French]. Rev Chir Orthop Reparatrice Appar Mot. 2001;87:820–825.
Brooks PJ. The jumbo cup: the 95% solution. Orthopedics. 2008;31:913, 915.
Dearborn JT, Harris WH. Acetabular revision arthroplasty using so-called jumbo cementless components: an average 7-year follow-up study. J Arthroplasty. 2000;15:8–15.
Delp SL, Wixson RL, Komattu AV, Kocmond JH. How superior placement of the joint center in hip arthroplasty affects the abductor muscles. Clin Orthop Relat Res. 1996;328:137–146.
Dora C, Houweling M, Koch P, Sierra RJ. Iliopsoas impingement after total hip replacement: the results of non-operative management, tenotomy or acetabular revision. J Bone Joint Surg Br. 2007;89:1031–1035.
Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z. Medial protrusio technique for placement of a porous-coated hemispherical acetabular component without cement in total hip arthroplasty patients who have acetabular dysplasia. J Bone Joint Surg Am. 1999;81:83–92.
Dorr LD, Wan Z. Ten years of experience with porous acetabular components for revision surgery. Clin Orthop Relat Res. 1995;319:191–200.
Dou Y, Zhou Y, Tang Q, Yang D, Liu J. Leg-length discrepancy after revision hip arthroplasty: are modular stems superior? J Arthroplasty. 2013;28:676–679.
Fabi D, Gonzalez M, Goldstein W, Ahmed M. Acetabular cup revision with the use of the medial protrusio technique at an average follow-up of 6.6 years. J Arthroplasty. 2010;25:197–202.
Fan CY, Chen WM, Lee OK, Huang CK, Chiang CC, Chen TH. Acetabular revision arthroplasty using jumbo cups: an experience in Asia. Arch Orthop Trauma Surg. 2008;128:809–813.
Gustke KA. Jumbo cup or high hip center: is bigger better? J Arthroplasty. 2004;19(Suppl 1):120–123.
Jasty M. Jumbo cups and morsalized graft. Orthop Clin North Am. 1998;29:249–254.
Lachiewicz PF, Soileau ES. Fixation, survival, and dislocation of jumbo acetabular components in revision hip arthroplasty. J Bone Joint Surg Am. 2013;95:543–548.
O’Sullivan M, Tai CC, Richards S, Skyrme AD, Walter WL, Walter WK. Iliopsoas tendonitis a complication after total hip arthroplasty. J Arthroplasty. 2007;22:166–170.
Patel JV, Masonis JL, Bourne RB, Rorabeck CH. The fate of cementless jumbo cups in revision hip arthroplasty. J Arthroplasty. 2003;18:129–133.
Tanzer M. Role and results of the high hip center. Orthop Clin North Am. 1998;29:241–247.
Vasavada AN, Delp SL, Maloney WJ, Schurman DJ, Zajac FE. Compensating for changes in muscle length in total hip arthroplasty. Effects on the moment generating capacity of the muscles. Clin Orthop Relat Res. 1994;302:121–133.
Whaley AL, Berry DJ, Harmsen WS. Extra-large uncemented hemispherical acetabular components for revision total hip arthroplasty. J Bone Joint Surg Am. 2001;83:1352–1357.
Author information
Authors and Affiliations
Corresponding author
Additional information
Two authors (NND, CDH) are employees of Stryker Orthopaedics Inc. (Mahwah, NJ, USA). The remaining authors (CN, MDR) certify that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Nwankwo, C., Dong, N.N., Heffernan, C.D. et al. Do Jumbo Cups Cause Hip Center Elevation in Revision THA? A Computer Simulation. Clin Orthop Relat Res 472, 572–576 (2014). https://doi.org/10.1007/s11999-013-3169-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-3169-2