
Abstract
Background
Bone grafts are frequently used to supplement bone stock and to establish structural stability. However, graft-associated infection represents a challenging complication leading to increased patient morbidity and healthcare costs.
Questions/purposes
We therefore designed this study to (1) determine if increasing initial S. aureus inoculation of bone allograft results in a proportionate increase in colonization; (2) assess if antibiotics decrease colonization and if antibiotic tethering to allograft alters its ability to prevent bacterial colonization; and (3) determine if covalent modification alters the allograft topography or its biological properties.
Methods
Allograft bone and vancomycin-modified bone (VAN-bone) was challenged with different doses of S. aureus for times out to 24 hours in the presence or absence of solution vancomycin. Bacterial colonization was assessed by fluorescence, scanning electron microscopy (SEM), and by direct colony counting. Cell density and distribution of osteoblast-like cells on control and modified allograft were then compared.
Results
Bacterial attachment was apparent within 6 hours with colonization and biofilm formation increasing with time and dose. Solution vancomycin failed to prevent bacterial attachment whereas VAN-bone successfully resisted colonization. The allograft modification did not affect the attachment and distribution of osteoblast-like cells.
Conclusions
Allograft bone was readily colonized by S. aureus and covered by a biofilm with especially florid growth in natural topographic niches. Using a novel covalent modification, allograft bone was able to resist colonization by organisms while retaining the ability to allow adhesion of osteoblastic cells.
Clinical Relevance
Generation of allograft bone that can resist infection in vivo would be important in addressing one of the most challenging problems associated with the use of allograft, namely infection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Surgeons are frequently faced with reconstruction challenges caused by bone loss [30]. Although autologous bone is the gold standard for bone restoration, donor site morbidity and limited bone volume [1, 6] have led to increased utilization of allograft bone. Approximately 800,000 bone allograft transplantations are performed yearly in the United States, making bone the second most commonly transplanted tissue [7] (exceeded only by blood). Unfortunately, after more than 50 years of research into synthetic tissue substitutes, none of these bone substitutes yet match the unique fibrous and mineral composition of bone [13].
Although bone allograft generally restores bone mass [19], complications such as graft-host nonunion, fracture, and graft infection [5] are not infrequent. Allograft-associated infection often requires removal of infected bone and extensive débridement of the affected site [32], with substantial patient morbidity. Most of these allograft-associated infections occur early (within 4 months) [29, 37], and despite extended antibiotic prophylaxis [31], the reported incidence remains at 4% to 12% [29]. Like metallic implants, allografts act as highly porous, noncellular, and avascular foreign bodies that are prone to bacterial adhesion. Once bacteria attach, they secrete a thick glycocalyx matrix rendering them inaccessible to immune surveillance and local cellular defense mechanisms [39].
To better understand bacterial colonization of bone grafts, we determined whether (1) increasing initial S. aureus inoculation of bone allograft results in a proportionate increase in colonization; (2) addition of antibiotics to solution decreases allograft colonization; and (3) covalent tethering of antibiotic to allograft alters its ability to prevent bacterial colonization; (4) covalent modification altered the topography of the allograft or its biological properties in allowing osteoblast-like cell adhesion.
Materials and Methods
The experimental design was performed three independent times (Fig. 1). Briefly, in order to characterize bacterial colonization of allograft, morselized bone was challenged with S. aureus (Ci = 102–105 cfu) for 6 hours, and sonicated to suspend adherent bacteria that were then plated and counted. We then asked if adding antibiotics to the solution would eradicate adherent S. aureus colonization. Morselized bone was challenged with S. aureus in (1) trypticase soy broth (TSB) alone; (2) TSB followed by addition of vancomycin (VAN) at 12 hours; or (3) TSB in the presence of VAN, and adherent bacteria were counted. The progression of bacterial attachment was also directly visualized on cortical bone stubs in the presence of TSB (control) or TSB + VAN. Control and vancomycin-modified bone (VAN-bone), were examined by SEM to allow assessment of any gross morphological changes in surface topography associated with the chemical modification process. The efficacy of VAN-bone to resist colonization was evaluated by challenging both control and VAN-bone with S. aureus for 12 hours and visualization by confocal laser scanning microscopy after staining with the Live/Dead BacLight™ kit (Invitrogen, Carlsbad, CA); or by SEM following fixing. Finally, the distribution of human fetal osteoblastic cells (hFOBs) that had been cultured on control and VAN-bone cortical squares for 48 hours were examined by confocal microscopy as a preliminary indication of toxicity/biocompatibility of the surfaces.

The experimental flow diagram is shown. A total of 21 morselized bone samples were used to quantitatively assess bacterial growth on bone as it varies with initial bacterial dose (12 samples) and addition of solution antibiotics (nine samples). Sixteen (16) cortical bone samples were then used to qualitatively assess the temporal colonization of bone surfaces in the presence or absence of solution antibiotics (six samples). Half of the remaining 10 samples were modified with vancomycin and half were used as controls for morphological assessment, visualization of SA colonization by SEM and fluorescence and toxicity determination by mammalian cell culture. All experiments were repeated at least three independent times. SA = Staphylococcus aureus.
Three cortical stubs or morselized human allograft bone were obtained from the Musculoskeletal Transplant Foundation. Cortical bone was cut into 1 × 1-cm squares using a high-speed cutter (Dremel: Racine, WI), washed, and sonicated with dH2O until washings were clear. Samples were partially demineralized by incubation with 12.5% EDTA, pH 7, 37°C for 3 days with shaking; EDTA was replaced daily. Before synthesis, all samples were washed with dH2O and sonicated twice for 30 minutes in dimethylformamide (DMF; Acros Organics, Morris Plains, NJ).
Washed cortical bone stubs were coupled twice with 10 mg/mL Fmoc-[2-(2-amino-ethoxy)-ethoxy]-acetic acid (Fmoc-AEEA) followed by chemical coupling with 10 mg/mL clinical grade VAN (American Pharmaceutical Partners, Inc, Schaumburg, IL) as described previously for bone (Ketonis et al., manuscript under review) and metal alloys [3, 16, 25]. The modified bone was washed extensively with DMF and incubated in dH2O for at least 5 days before use. Presence of VAN was confirmed by reaction with a specific anti-VAN antibody (US Biologicals, Swampscott, MA).
Control or VAN-bone was sterilized with 70% ethanol for 15 minutes and washed three times with PBS and three times with TSB. S. aureus (Xen36 derived from ATCC 49525; Caliper Life Science, Hopkinton, MA) were cultured in TSB, 250 rpm, 37ºC, 12 to 14 hours (overnight culture), followed by dilution using a 0.5 McFarland (a turbidity standard with approximately 1 × 108 cfu/mL when A600 = 0.10). Bacteria were incubated with the sterilized samples in TSB, 37°C, under static conditions for 6 to 24 hours.
To determine colonization as a function of bacterial dose, sterilized morselized bone (10 mg) was incubated with bacteria (Ci = 102, 103, 104 or 105 cfu) for 6 hours in TSB, 37°C, under static conditions. Samples were washed three times with PBS, transferred to Eppendorf tubes, briefly vortexed, and washed three more times with PBS to remove nonadherent bacteria. To suspend the adherent bacteria, samples were sonicated in 0.3% Tween-80, 5 minutes, and after serial dilution, plated on 3 M® Petrifilms (St. Paul, MN) and incubated overnight at 37°C. Films were digitally counted using a macro in Adobe Photoshop CS3 (San Jose, CA).
To test the efficacy of solution antibiotic in preventing bacterial colonization, 1 × 104 cfu S. aureus were incubated with (1) TSB, 12 hours, TSB 4 hours; (2) TSB, 12 hours, TSB + 10 μg/mL VAN, 4 hours; (3) TSB + 10 μg/mL VAN, 12 hours, TSB, 4 hours. Adherent bacteria were plated or imaged. Imaging of cortical stubs was performed on bone squares that had been challenged with S. aureus for 6, 12, or 24 hours in TSB, 37ºC, washed thoroughly to remove nonadherent bacteria, and reincubated in a fresh plate containing either TSB (control) or TSB + VAN. After 3 hours, samples were thoroughly washed with PBS to remove nonadherent bacteria and were either stained with the Live/Dead BacLight™ Kit (Invitrogen, Carlsbad, CA; 20 minutes, room temperature) and visualized with confocal laser microscopy or prepared for visualization by SEM. Areas of surface colonization were determined from multiple fluorescent images analyzed using ImagePro (Media Cybernetics, Inc, Bethesda, MD).
Control and VAN-modified cortical bone squares (1 cm × 1 cm) were sterilized with 70% ethanol, rinsed three times with PBS, three times with DMEM/F-12 containing 10% FBS (full media), and exposed to ultraviolet radiation for 10 minutes. The sterilized samples were incubated with 1 mL of 5 × 104 cells/mL hFOBs [22] in full media for 48 hours, stained with CellTracker (Invitrogen, Carlsbad, CA; 1 μM, 30 minutes) and visualized using confocal laser microscopy.
Bacterially-colonized control or VAN-modified cortical bone squares (1 cm × 1 cm) were thoroughly washed with dH2O and fixed for 1 hour with 4% paraformaldehyde. Samples were sequentially dried with a graded ethanol series, incubated in Freon, and vacuum-dried overnight. Samples were then affixed onto a metal plate, sputter-coated with gold, and visualized using a Hitachi TM-1000 SEM (Ibaraki, Japan).
All experiments (Fig. 1) were performed independently at least three times. Data are presented as means ± standard errors. All statistical analyses were performed on normal equally variant data using a one or two-way analysis of variance (ANOVA) with a Tukey multiple comparison procedure.
Results
Increasing inocula resulted in increased colonization, with no apparent plateau under our study conditions. Bacteria added to solution proliferated over time so that an initial inoculate of 1 × 102 cfu yielded approximately 4 × 104 cfu after 6 hours incubation, whereas 1 × 105 cfu resulted in yield of approximately 7.6 × 106 cfu, an almost 200-fold increase (Fig. 2).

The colonization of allograft by Staphylococcus aureus is shown. Morselized bone squares were challenged with increasing numbers of S. aureus for 6 hours. Small increases in initial bacterial inoculates resulted in a much more robust colonization at the end of the incubation period. Numbers of colonizing bacteria are expressed as fold change relative to the 102 inoculum.
Addition of VAN to solution only partially prevented bacterial proliferation. Addition of VAN for 4 hours following bacterial attachment on the bone morsels, resulted in a marginal reduction in colonization as compared to control samples without VAN. Bacterial colonization, though reduced, still occurred even when VAN was added concurrently with the bacterial inoculum (Fig. 3). By microscopy, individual bacteria as well as biofilm formation were evident on the surface of the cortical bone squares at 6 hours (Fig. 4A), which progressed to bacterial aggregates (Fig. 4B) consequently to mature biofilm with its characteristic reticulate honeycomb appearance (Fig. 4C). When incubated for an additional 3 hours in the presence of 10 μg/mL VAN (~5–10 times the MIC), bacterial colonization was still abundant on the bone surface at all time points (Fig. 4D–F: 6–24 hrs). By SEM, these VAN-treated, colonized surfaces showed individual grape-like clusters of bacteria (Fig. 4D–F, arrows) as well as mature biofilms (Fig. 4E–F, asterisks) that formed despite the presence of VAN in solution.

Effects of the addition of 10 μg/mL vancomycin (VAN) on bacterial colonization are illustrated. Morselized bone was colonized with trypticase soy broth (TSB) ± VAN using the schedule indicated under the bars showing that only a small reduction is achieved in colonization by solution antibiotics. Error bars = Standard error.

Surface colonization by S. aureus is shown. (A) Control cortical allograft was challenged for 6 to 24 hours with S. aureus and reincubated in TSB (A–C) or TSB in the presence of 10 μg/mL VAN (D–F) for an additional 3 hours. The micrographs show a gradual increase in biofilm generation and how it matures over time. Note the reticulate and characteristic honeycomb appearance entrenching most of the bacteria present and protecting them from solution antibiotics. Scale bar: 10 μm; arrows = bacterial clusters; asterisks = biofilm.
The endosteal surface of the bone pieces from the cortical stub squares was sanded until flat and VAN linked to the primary amines displayed on the ECM proteins of bone allograft (Fig. 5A–B). Covalent tethering of VAN to allograft did not alter the surface topography as seen by SEM (Fig. 5C–D). The microarchitecture of modified and control bone appeared similar by containing a dense collagen fiber meshwork, osteocytic lacunae with the Haversian and Volkmann’s canals being preserved.

Preparation of bone squares is illustrated. (A) Cortical stubs from human cadaveric tibias were supplied by the Musculoskeletal Transplant Foundation, washed, and marked into squares measuring 1 × 1 cm. Each cortical stub yielded between approximately 20 and 30 squares. (B) A high-speed cutter (Dremel) was used to cut the marked tibias into individual 1 × 1-cm squares that were further washed and processed. The endosteal surface of the bone pieces was sanded until flat making the thickness of each piece approximately 2 to 3 mm; a cartoon is shown of the synthetic scheme for attachment of vancomycin (VAN) (through two aminoethoxyethylacetate [AEEA] linkers) to the primary amines displayed on the ECM proteins of bone allograft. (C–D) Scanning electron microscopy analysis of bone following VAN coupling is shown. Note that the gross topography was unchanged between control (C) and modified bone (D) with preservation of the collagenous meshwork and the natural crevices and capillary canals. Scale bar: 10 μm.
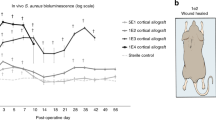
S. aureus readily colonized control bone (Ci = 104 cfu, 12hrs), as evidenced by multiple green foci (Live/Dead stain, live bacteria fluoresce green), with patchy areas of abundant stain uptake indicative of biofilm. Using the same conditions, VAN-bone showed little evidence of microcolony formation; a few fluorescent green trails were apparent that are likely the result of stain trapping in the crevices of the bone surface (Fig. 6A). Morphometric analysis of multiple such images revealed that bacterial coverage on VAN-allograft surfaces was less (p < 0.001) than that of controls (0.8% of controls) (Fig. 6B).

VAN-bone prevents bacterial colonization. (A) After 12 hours incubation with S. aureus, control bone (Con) shows green punctate staining (adherent bacteria), with larger areas of intense staining indicating biofilm presence. Note that minimal staining was seen on the VAN allograft with only occasional trails of stain trapped in the underlying crevices of the bone. Scale bar: 100 μm. (B) Morphometric analysis shows that the total area covered on VAN-bone is smaller. Total colonized area is expressed as a percentage of controls. (* = p < 0.001)
By SEM, control bone surfaces were covered with multiple colonies of S. aureus (Fig. 7A, control). At higher magnifications, these colonies organized into grape-like clusters (Fig. 7B–C). Planar surfaces were also covered with a slimy material characteristic of biofilm (Fig. 7D). Within this biofilm, multiple small spherical bacteria (diameter 0.3–1 μm) can be distinguished, representing entrenched S. aureus. At higher magnification, in areas where the biofilm was more mature, biofilm budding was seen as bright white features [20] (Fig. 7E–F). Natural topographic niches such as Haversian and Volkmann’s canals seemed to be a nidus for bacterial aggregation, and examination of these structures at higher magnification showed that they were consistently populated with S. aureus colonies that extended into the canals (Fig. 7G–I). In contrast, the surface of the VAN-bone appeared free of bacterial colonies even within Haversian/Volkmann’s canals (Fig. 7J–L).

SEM assessment of colonization is shown. Control surfaces were abundantly colonized with bacteria (CONTROL) after 12 hours. At low magnification on the planar surfaces (A), small white dots are evident that, at higher magnifications (B–C), resolve into multiple colonies of bacteria that populate the surface in grape-like clusters. On other areas, reticulated biofilm (D) is evident which at higher magnification (E–F) can be distinguished as a thick layer of slimy material with multiple small spherical bacteria (diameter 0.3–1 μm) representing biofilm entrenched S. aureus colonies. Natural topographic niches such as Haversian and Volkmann’s canals (G) at low magnifications showed no apparent colonization. However, at higher magnifications, they were consistently filled with S. aureus (H) that at 3000x (I) were seen deep into these canals. The surface of the VAN-allograft appeared free of bacterial colonies on all surfaces at any magnification (J–L). Scale bars: A, D, G, J = 200 μm; B, E, H, K = 50 μm; C, F, I, L = 30 μm.
Human fetal osteoblast-like cell cultured on VAN-allograft (48 hrs) retained normal morphology and distribution. Cell shape and distribution were very similar between the control and VAN-modified allograft with cells appearing to align along the underlying collagenous matrix (Fig. 8). Cell density appeared similar on both the control and VAN-bone, suggesting the VAN-bone is sufficiently like the parent bone substrate to support bone ingrowth.

Cell morphology on control and vancomycin (VAN)-bone surfaces. Human fetal osteoblastic (hFOBs) cells were stained with CellTracker Green after culturing for 48 hours on control and VAN-bone. Abundant hFOBs attached to both control (A) and VAN-bone (B) surfaces showed normal morphology and exhibited a similar distribution and density. Scale bar: 400 μm.
Discussion
Allograft bone is used frequently to replenish bone loss that may be encountered during revision joint arthroplasty [30]. With the rise in the number of complex revision arthroplasty cases and the increase of aging population, the demand for bone grafts will continue. Worldwide, bone grafts are used in approximately 2.2 million orthopaedic procedures annually, generating a $2.5 billion per year industry [14]. Unfortunately, the prevalence of allograft-related infection rates remains relatively high with a reported incidence of 4% to 12% compared to periprosthetic joint infection rates of 1% to 3% [11, 26, 41]. This study was designed to investigate the phenomenon of allograft infection by conducting a series of experiments. We determined if (1) increasing initial S. aureus inoculation of bone allograft resulted in a proportionate increase in colonization; (2) addition of antibiotics to solution could decrease allograft colonization; (3) covalent tethering of antibiotic to allograft altered its ability to prevent bacterial colonization; and (4) covalent modification altered the topography of the allograft or its biological properties in allowing osteoblast-like cell adhesion.
The most important limitation of this study is that it is an in vitro attempt to describe an in vivo phenomenon. As a result, it necessarily deals with the time frames and ideal environment associated with bacterial colonization under laboratory conditions. Second, much of the data that we present depends on visual assessment of bacterial colonization on surfaces. With the special properties of adherent/biofilm bacteria, detection of these bacteria using the stains and SEM, as we have described, are methods that circumvent the need for biofilm dissolution and bacterial detachment required for accurate counts and are thus, of necessity, observational. However, these methods can only sample limited areas on the surface and hence cannot offer the assurance that there are not pockets of allograft that appear different. Unfortunately, currently available more quantitative methods, ie, resuspension of adherent bacteria and subsequent plating are plagued by problems such as poor recovery of bacteria [34]. Third, we assessed colonization by one organism and one antibiotic construct. In a situation where infection is establishing, it may not be rare to find multiple microorganisms. We limited the experimental design to the most common infecting organism, namely Staphylococcus aureus, which we believe represents a “model organism” for allograft associated infections. However, we acknowledge other organisms may behave differently. Fourth, the concentrations of vancomycin used for addition to solution was based on our experience with these experiments over the past few years and appears to be ~10X the MIC for the planktonic S. aureus. It was our aim to stay within clinically useful levels while avoiding concentrations that could become toxic to mammalian cells.
We found small increases in initial bacterial inoculate resulted in a disproportionately large increase in bacterial colonization of allograft surfaces. The bacteria readily attached to, and colonized, cortical allografts in vitro. From our subsequent electromicrograph analysis, it appears that bacterial colonization was potentiated by the porous nature of bone that provides bacteria with topographically protected niches where they can attach, proliferate, and form a mature biofilm. Successful bacterial colonization can be achieved with very small inoculate sizes when foreign bodies are present [23]. For example, the initial inoculate of bacteria required to infect an incision site decreases by 4 logs when sutures are in place [17]. In our experiments, colonization was achieved on bone with the lowest inoculate tested (100 cfu) and the attached bacteria harvested dramatically increased for every subsequent 10-fold increase in dose. However, a much higher inoculum of 104 cfu was chosen to challenge the modified allograft in order to capture the clinical scenario when larger number of bacteria may be present.
Systemic or local antibiotics alone are unlikely to eradicate an established infection around a prosthesis or an allograft [12]. We attempted to recapitulate this situation through introduction of antibiotics after establishment of bacterial colonization on the allograft. As observed clinically, these bathing antibiotics, while clearing the nonadherent bacteria, were unable to affect the adherent bacteria, much of which remained encased in a biofilm slime. Importantly, bacteria were able to attach to bone surfaces even when inoculated in an antibiotic-rich medium. Electron microscopy demonstrated that S. aureus attached and initiated biofilm formation on cortical allografts within 6 hours. By 12 and 24 hours, the surface was covered with the thick biofilm glycocalyx, entrenching and protecting the underlying bacteria from environmental challenges including solution antibiotics [21, 33, 35]. We suggest in vivo colonization of allografts during establishment of infection can occur preferentially in protected niches, although the timeframe of these events is likely to be longer than what we describe here. To prevent establishment of infection during the immediate postsurgical period, prophylactic antibiotic regimens have been adopted that involve the administration of antibiotics intravenously for 2 to 14 days and orally for up to 16 weeks [15, 24, 29]. Similarly, to prevent initial infection, physicians have empirically impregnated bone allografts with antibiotics before implantation, achieving high local concentrations of antibiotic during the initial elution [8]. Our in vitro data support these processes, and even though they are important means to prevent establishment of infection, they are imperfect. Unfortunately, as with supplementation of PMMA cement with antibiotics, elution kinetics from allograft are largely variable, in which high local antibiotic concentrations can have deleterious effects on host cells thereby retarding graft incorporation. Additionally, once antibiotic is depleted, the graft is again susceptible to bacterial colonization. Therefore, although use of allograft has yielded excellent results, its use in cases of infection has been controversial as a result of the possible increased risk of reinfection [8, 9, 18].
In an attempt to address these problems, we turned to an antibiotic-modified cortical allograft as an approach to providing an antibacterial surface that would effectively resist infection. Despite subjecting the modified allograft to bacterial inoculate three to four orders of magnitude higher than what one expects to encounter in a clinical scenario [4, 17], the allograft exhibited excellent efficacy in preventing colonization by S. aureus. The process of modification did not appear to affect the microarchitecture of bone or its biological activity, at least based on limited cellular adhesion studies that were performed here. The surface demineralization that we used is not uncommon in allograft preparations and reportedly enhances bone incorporation and ingrowth [27, 28]. The solvents used during the chemical modification also appeared to access the niches and allow coupling of allograft throughout.
The observation that osteoblast-like cells were able to adhere to the surface of the modified allograft as readily as the control allograft is encouraging. Previous experiments in our laboratory and those of others have shown antibiotics in higher concentrations can have deleterious effects on mammalian cells [2, 40]. Therefore, toxicity studies must be performed with the introduction of any novel bioactive construct or drug delivery system [10, 36, 38]. When the cells on our antibiotic-laden construct were visualized, careful observations failed to identify any differences among their density, morphology, distribution, and cell–cell associations on either control or VAN-modified allograft. Although a detailed assessment of biocompatibility, including measurements of osteoblastic maturation, is required to fully characterize the effect of the VAN-surface on osteoblastic function, these initial findings are suggestive that the VAN-bone should be biocompatible. Furthermore, because the antibiotic is permanently bonded to the surface of the allograft, no systemic toxicity is expected in vivo.
References
Ahlmann E, Patzakis M, Roidis N, Shepherd L, Holtom P. Comparison of anterior and posterior iliac crest bone grafts in terms of harvest-site morbidity and functional outcomes. J Bone Joint Surg Am. 2002;84:716–720.
Antoci V, Adams CS, Hickok NJ, Shapiro IM, Parvizi J. Antibiotics for local delivery systems cause skeletal cell toxicity in vitro. Clin Orthop Relat Res. 2007;462:200–206.
Antoci V, Adams CS, Parvizi J, Ducheyne P, Shapiro IM, Hickok NJ. Covalently attached vancomycin provides a nanoscale antibacterial surface. Clin Orthop Relat Res. 2007;461:81–87.
Arbeit RD, Dunn RM. Expression of capsular polysaccharide during experimental focal infection with Staphylococcus aureus. J Infect Dis. 1987;156:947–952.
Aro HT, Aho AJ. Clinical use of bone allografts. Ann Med. 1993;25:403–412.
Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA. Complications of iliac crest bone graft harvesting. Clin Orthop Relat Res. 1996;329:300–309.
Boyce T, Edwards J, Scarborough N. Allograft bone. The influence of processing on safety and performance. Orthop Clin North Am. 1999;30:571–581.
Buttaro M, Comba F, Piccaluga F. Vancomycin-supplemented cancellous bone allografts in hip revision surgery. Clin Orthop Relat Res. 2007;461:74–80.
Buttaro MA, Morandi A, Rivello HG, Piccaluga F. Histology of vancomycin-supplemented impacted bone allografts in revision total hip arthroplasty. J Bone Joint Surg Br. 2005;87:1684–1687.
Cleary J, Rogers P, Chapman S. Variability in polyene content and cellular toxicity among deoxycholate amphotericin B formulations. Pharmacotherapy. 2003;23:572–578.
Darouiche RO. Treatment of infections associated with surgical implants. N Engl J Med. 2004;350:1422–1429.
Day RE, Megson S, Wood D. Iontophoresis as a means of delivering antibiotics into allograft bone. J Bone Joint Surg Br. 2005;87:1568–1574.
Delloye C, Cornu O, Druez V, Barbier O. Bone allografts: what they can offer and what they cannot. J Bone Joint Surg Br. 2007;89:574–579.
Desai BM. Osteobiologics. Am J Orthop. 2007;36(Suppl):8–11.
Dick HM, Strauch RJ. Infection of massive bone allografts. Clin Orthop Relat Res. 1994;306:46–53.
Edupuganti OP, Antoci V, King SB, Jose B, Adams CS. Covalent bonding of vancomycin to Ti6Al4V alloy pins provides long-term inhibition of Staphylococcus aureus colonization. Bioorg Med Chem Lett. 2007;17:2692–2696.
Elek SD, Conen PE. The virulence of Staphylococcus pyogenes for man: a study of the problems of wound infection. Br J Exp Pathol. 1957;38:573–586.
Farfalli GL, Buttaro MA, Piccaluga F. Femoral fractures in revision hip surgeries with impacted bone allograft. Clin Orthop Relat Res. 2007;462:130–136.
Finkemeier CG. Bone-grafting and bone-graft substitutes. J Bone Joint Surg Am. 2002;84:454–464.
Fux CA, Stoodley P, Hall-Stoodley L, Costerton JW. Bacterial biofilms: a diagnostic and therapeutic challenge. Expert Rev Anti Infect Ther. 2003;1:667–683.
Hall-Stoodley L, Costerton JW, Stoodley P. Bacterial biofilms: from the natural environment to infectious diseases. Nat Rev Microbiol. 2004;2:95–108.
Hicok KC, Thomas T, Gori F, Rickard DJ, Spelsberg TC, Riggs BL. Development and characterization of conditionally immortalized osteoblast precursor cell lines from human bone marrow stroma. J Bone Miner Res. 1998;13:205–217.
James RC, MacLeod CJ. Induction of staphylococcal infections in mice with small inocula introduced on sutures. Br J Exp Pathol. 1961;42:266–277.
Jofe MH, Gebhardt MC, Tomford WW, Mankin HJ. Reconstruction for defects of the proximal part of the femur using allograft arthroplasty. J Bone Joint Surg Am. 1988;70:507–516.
Ketonis C, Parvizi J, Adams CS, Shapiro IM, Hickok NJ. Topographic features retained after antibiotic modification of Ti alloy surfaces: retention of topography with attachment of antibiotics. Clin Orthop Relat Res. 2009;467:1678–1687.
Lentino JR. Prosthetic joint infections: bane of orthopedists, challenge for infectious disease specialists. Clin Infect Dis. 2003;36:1157–1161.
Lewandrowski KU, Schollmeier G, Ekkemkamp A, Uhthoff HK, Tomford WW. Incorporation of perforated and demineralized cortical bone allografts. Part I: radiographic and histologic evaluation. Biomed Mater Eng. 2001;11:197–207.
Lewandrowski KU, Tomford WW, Schomacker KT, Deutsch TF, Mankin HJ. Improved osteoinduction of cortical bone allografts: a study of the effects of laser perforation and partial demineralization. J Orthop Res. 1997;15:748–756.
Lord CF, Gebhardt MC, Tomford WW, Mankin HJ. Infection in bone allografts. Incidence, nature, and treatment. J Bone Joint Surg Am. 1988;70:369–376.
Ma T, Gutnick J, Salazar B, Larsen MD, Suenaga E, Zilber S, Huang Z, Huddleston J, Smith RL, Goodman S. Modulation of allograft incorporation by continuous infusion of growth factors over a prolonged duration in vivo. Bone. 2007;41:386–392.
Mankin HJ, Hornicek FJ, Raskin KA. Infection in massive bone allografts. Clin Orthop Relat Res. 2005;432:210–216.
Muscolo DL, Ayerza MA, Calabrese ME, Gruenberg M. The use of a bone allograft for reconstruction after resection of giant-cell tumor close to the knee. J Bone Joint Surg Am. 1993;75:1656–1662.
Percival SL, Kite P. Intravascular catheters and biofilm control. J Vasc Access. 2007;8:69–80.
Sanford BA, de Feijter AW, Wade MH, Thomas VL. A dual fluorescence technique for visualization of Staphylococcus epidermidis biofilm using scanning confocal laser microscopy. J Ind Microbiol. 1996;16:48–56.
Stamm WE. Catheter-associated urinary tract infections: epidemiology, pathogenesis, and prevention. Am J Med. 1991;91:65S–71S.
Thimm B, Unger R, Neumann H, Kirkpatrick C. Biocompatibility studies of endothelial cells on a novel calcium phosphate/SiO2-xerogel composite for bone tissue engineering. Biomed. Mater. 2008;3:15007.
Tomford WW, Thongphasuk J, Mankin HJ, Ferraro MJ. Frozen musculoskeletal allografts. A study of the clinical incidence and causes of infection associated with their use. J Bone Joint Surg Am. 1990;72:1137–1143.
Udipi K, Chen M, Cheng P, Jiang K, Judd D, Caceres A, Melder RJ, Wilcox JN. Development of a novel biocompatible polymer system for extended drug release in a next-generation drug-eluting stent. J Biomed Mater Res Part A. 2008;85:1064–1071.
Witsø E, Persen L, Benum P, Bergh K. Cortical allograft as a vehicle for antibiotic delivery. Acta Orthop. 2005;76:481–486.
Witsø E, Persen L, Løseth K, Bergh K. Adsorption and release of antibiotics from morselized cancellous bone. In vitro studies of 8 antibiotics. Acta Orthop. 1999 Jun 1;70(3):298–304.
Zimmerli W. Prosthetic-joint-associated infections. Best Pract Res Clin Rheumatol. 2006;20:1045–1063.
Acknowledgments
We thank the Musculoskeletal Transplant Foundation for providing samples for this work as well as for their generous support of these studies.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Ketonis, C., Barr, S., Adams, C.S. et al. Bacterial Colonization of Bone Allografts: Establishment and Effects of Antibiotics. Clin Orthop Relat Res 468, 2113–2121 (2010). https://doi.org/10.1007/s11999-010-1322-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-010-1322-8