
Abstract
Acetabular revision of failed cages or rings may be facilitated by previously placed bone graft, enabling the use of highly porous cementless hemispheric cups. We retrospectively reviewed all 15 patients who had conversion of failed antiprotrusion cages (10 patients) or roof rings (five patients) to cementless cups. All patients had restoration of bone stock (three major column, eight morselized, four combined bone grafts) performed in conjunction with their index cage or ring reconstruction arthroplasty. The minimum followup was 24 months (average, 48.3 months; range, 24–72 months). Failure was defined as radiographic cup migration. In 12 of the 15 patients, there was no radiographic change in cup position at the last followup or symptoms indicative of loosening. The average Harris hip scores improved from 31 (range, 15–48) to 69 (range, 56–87) at latest followup. Cup failure occurred in three patients. In two patients, the failed cups were revised; the third patient refused additional surgery. Our experience suggests treatment of failed cages by highly porous cementless cups is a reasonable option. However, we recommend patients be followed closely to detect cup migration, which can occur until satisfactory bony ingrowth occurs.
Level of Evidence: Level IV, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acetabular reinforcement rings, also known as roof rings and antiprotrusion cages, have been used for approximately 30 years in the management of severe acetabular bone loss in revision THA [7, 9–11, 19, 27]. Roof rings are a metallic device with a superior flange for the placement of multiple screws for additional fixation. These implants are generally used to protect morselized cancellous bone grafts in minor acetabular dome or medial wall defects and are in contact with host bone superiorly and inferomedially. In contrast, antiprotrusion cages are larger metallic implants that span the entire acetabulum from the ilium to the ischium. Antiprotrusion cages gain supplementary purchase through a superior flange fixed with multiple screws onto the ilium and a lower flange inserted through a slot into the ischium. These cages are used for more extensive bone defects, including uncontained defects of the acetabular columns and dome when contact with native bleeding bone is marginal for bone ingrowth to allow long-term fixation of cementless cups [2, 19, 23, 26, 33, 34]. They protect the extensively grafted acetabular bed, often by major column grafts, by transferring some of the load from the acetabular bed to the ilium and the ischium.
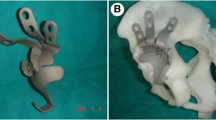
Because there is no bone ingrowth into the cages, they have reported failure rates defined as aseptic loosening and cage migration ranging from 0% to 25% at midterm as a result of hardware failure of the screws or flanges [9, 32, 34]. Screws may eventually break, whereas the ischial flanges can either break or loosen, leading to cage migration (Fig. 1). Management of failed acetabular cage reconstruction (reinforcement rings or antiprotrusion cages) may require a repeated attempt at cage reconstruction [19].

A 76-year-old patient presented with a failed antiprotrusion cage. Note the broken hardware and a distorted ischium.
However, bone graft implanted during the index cage reconstruction may provide satisfactory bone stock to allow coverage for a cementless hemispheric cup fixed by multiple screws and simplifying the surgical procedure [2, 4, 5]. Trabecular metal cups provide reliable bone ingrowth and durability even under less favorable conditions such as pelvic discontinuity [28, 29].
Our study had several objectives: (1) to determine the rates of cup migration or presence of radiolucent lines after conversion of failed cages to trabecular metal (TM) cups without ancillary buttressing of a metallic augment or structural bone graft; and (2) to evaluate the Harris hip scores (HHSs) and use of walking aids for ambulation.
Materials and Methods
We retrospectively reviewed all 15 patients (nine women, six men) who had a failed cage reconstruction with bone grafting and who were converted to TM hemispheric cups (Zimmer, Warsaw, IN) (Figs. 2, 3). The indication for all revisions was aseptic loosening and cage migration. The mean age at the time of surgery was 67 years (range, 34–89 years). Average time to cage failure, defined as cage migration resulting from loosening, hardware breakage, or ischial flange escape, was 75 months (range, 22–123 months; median, 72 months; Table 1), which corresponds to the reported time to failure of acetabular cages in previous studies [9, 33]. The only patient with a cage survival shorter than 50 months was referred to our institution as a result of a technically malpositioned cage. Apart from this patient, all index cage reconstructions were performed by the senior author (AEG). Minimum followup was 24 months (average, 48.3 months; range, 24–72 months). One patient died 36 months postsurgery; at her last followup, 3 years postsurgery, there was no evidence of cup migration or loosening. None of the patients was lost to followup. We had prior approval of our Institutional Review Board.

Postoperative radiographs of the patient at 6 weeks postconversion from a failed antiprotrusion cage to trabecular metal cup. Note that the broken screws did not require removal and were left in situ.

Postoperative radiographs of the patient at 2 years postconversion from failed cage to trabecular metal cup. There is no change in cup position or presence of radiolucent lines.
All patients had bone grafting (three structural, eight morsellized, four combined bone grafts) performed in conjunction with the initial cage or ring reconstruction (Table 1). Ten of the cages were antiprotrusion cages and five were reinforcement rings. In six of the 10 antiprotrusion cages, structural bone grafts were used either in combination with morsellized bone graft (three patients) or alone (three patients). In the remaining four patients, bone stock was restored solely by morsellized bone graft. Conversely, morsellized bone grafts were used in four of the five patients with failed reinforcement rings, whereas a combined morsellized and major column bone graft was used in one patient.
In each patient, we documented the number of previous arthroplasties as well as surgical approach, acetabular and femoral head sizes, type of liner, number of screws used to fix the cup, and use of morsellized fresh frozen bone allograft (Table 1). In six of the 15 patients, we inserted a constrained liner at the time the failed acetabular cage was converted to a TM cup to enhance hip stability. In four of these patients, cage failure was accompanied by dislocation, whereas another patient had a history of dislocations and was already treated by a constrained liner before his cage failure. The remaining patient had severely compromised abductor function.
The senior author used revision model 00-7000-056-20 (Zimmer) TM cups for all of these complex revision arthroplasties because they allow bone ingrowth even with limited bleeding bone. If necessary, new drill holes can be drilled by the surgeon into the TM cups for enhanced initial cup fixation by appropriately placed screws into the ilium [14, 21, 22]. Drilling the TM cup is approved by the manufacturer only in the revision model. The quality of screw purchase was assessed by the senior author (AEG) on a rough estimate scale of 1 to 10 with the aim to have at least two screws with good purchase (8 and above) [4]. Subsequently, an average of four screws (range, 2–6; median, 4) (Table 1) was used.
We performed a trochanteric sliding or extended trochanteric osteotomy in all patients [9]. Extended trochanteric osteotomy was used in two patients with loose femoral components that were revised to a cementless modular stem (ZMR; Zimmer) in conjunction with the cage conversion. In cases in which there was a previous fibrous union after a previous arthroplasty, the greater trochanter bony shell was preserved, maintaining vastus lateralis-abductor continuity, and was secured at the end of the revision to the proximal femur. The loose cage was removed carefully to prevent unnecessary damage to the acetabular bone stock and soft tissues, especially at the vicinity of the sciatic notch. The acetabulum was cleared from residual cement and soft tissue typically present at the backside of the cup. The acetabulum was initially assessed for segmental as well as cavitary defects and was reamed until good contact was reached with bleeding host bone. The most superficial layer of the acetabular bone graft implanted during the cage reconstruction was sclerotic [21]. A deeper layer was transitional and has few islands of bleeding bone. It was necessary to ream beyond this layer to reveal the deepest layer of the bone graft that has superior vascularity with more abundant bleeding bone, allowing improved biologic conditions for bony ingrowth. Once reaming of the acetabulum was completed, we examined the acetabular bed to evaluate bone defects and to determine if its bone stock could provide adequate mechanical support for the cup. In all the patients included in the study, the acetabular bed allowed a reasonable press fit of the cup for primary fixation [2, 5, 21]. At the time of conversion to TM cups, we encountered cavitary (Type II) defects in 10 of the 15 patients [3, 25] that were filled with packed fresh-frozen morselized bone allograft. No segmental acetabular defects were encountered; thus, none of the patients in the study had ancillary buttressing by a structural bone graft or a metallic augment. A touch weightbearing protocol was applied to all patients postoperatively for a period of 6 weeks with a gradual return to full weightbearing over 2 weeks thereafter.
We clinically evaluated each patient at 6 weeks, 6 months postsurgery, and at annual followup visits. The evaluation included HHSs (which had also been obtained preoperatively) [13]. In addition, we recorded data regarding patients’ use of walking aids preoperatively and postoperatively (Table 2).
Radiographic evaluation included routine hip radiographs (anteroposterior view of the pelvis as well as anteroposterior and lateral views of the affected hip) performed preoperatively and at 6 weeks, 6 months, and annually postsurgery (Figs. 2, 3). Radiographs performed at 6 weeks postsurgery served as the baseline to which subsequent followup radiographs were compared. The senior author (AEG) examined acetabular cup fixation according to published criteria for cup migration as well as for presence of radiolucent lines [20]. In each patient, cup inclination angles and the vertical distance of the hip center of rotation from the inter ischial line as well as the horizontal distance from the hip center of rotation to the ipsilateral teardrop were determined. If the teardrop of the involved side was deformed after cage reconstruction, the contralateral teardrop served as the reference point for these measurements. Cup failure was defined if horizontal or vertical acetabular component migration greater than 5 mm was observed or if radiographs demonstrated circumferential radiolucent lines, including in the area around the screws [20].
Results
In 12 of the 15 patients, there was no change in cup position or radiolucent lines on followup radiographs at latest followup. None of these patients reported symptoms indicative of loosening. In three patients, we identified cup at 6 months, 1 year, and 3 years postsurgery, respectively. In the first patient, the cup was replaced by an antiprotrusion cage and the patient is doing well with HHS of 62 at 3 years followup. The second patient refused any additional surgical intervention and ambulates with a walker. In the third patient, the cup was changed to a larger TM cup (74–78 mm diameter) that was protected by an antiprotrusion cage (cup-cage technique). He is doing well at 6-month followup and ambulates with a walker. The cup migrated in two of the six patients who were treated by a constrained liner compared with only one of the remaining nine patients treated by unconstrained liners at their index conversion arthroplasty from failed cages to cups.
The average HHS improved from 31 (range, 15–48; median, 27) preoperatively to 69 (range, 56–87; median, 65) at latest followup. Two patients did not use external walking aids, four patients used a single cane, two patients used two canes, and four patients used a walker (Table 2). One patient, who had a hip dislocation after conversion from a failed cage to a TM cup, was treated by revision of his femoral component and changing his liner to a constrained one without changing the TM shell. No infections, vascular or neurologic injuries were encountered.
Discussion
Clinical outcomes of acetabular reconstructions by cages combined with allogeneic bone graft have been well documented [1, 2, 7–11, 23–27, 34] with a reported failure rate reaching up to 25% at 5 years [9]. However, to the best knowledge of the authors, there are no data in the literature regarding the outcomes of repeated acetabular reconstructions after such failures. During the timeframe from reconstruction with a cage to implant failure, the bone graft implanted in conjunction with the cage reconstruction may undergo remodeling and restore the acetabular bone stock [21]. In some cases, this may provide adequate bone stock for reconstruction with a cementless hemispheric cup without structural support instead of repeated reconstruction by a cage [4]. Consequently, the acetabular reconstruction will not involve extra acetabular exploration of the ischium and ilium that is required for repeated reconstruction by a cage. Thus, the potential for sciatic nerve as well as the superior gluteal nerve and artery injury may be reduced [14]. We report on the radiographic outcomes, including rates of cup failure and presence of radiolucent lines as well clinical outcomes using HHS and use of walking aids, in 15 patients with failed acetabular cages managed by nonbuttressed TM cups at a mean of 4 years.
Our study has certain limitations. First, the number of patients was limited despite the high-volume referral base and catchments area of our institution. Given there was no control group, the lack of published data in the literature specific for outcomes after repeated acetabular reconstructions after failed cages did not allow for a ready comparison. Second, the followup review of the patients was not blinded. Third, because this was not a randomized study, selection bias and confounders could not be controlled. In addition, the decision whether a nonbuttressed cup is appropriate can be taken only after removal of the old component and reaming the socket. This decision is based on the type of the acetabular defects, quality of fixation achieved, and amount of bleeding bone from the restored bone stock. Consequently, the decision may not be reproduced by an unbiased observer [25]. However, none of the patients was lost to followup and we analyzed a uniform acetabular reconstruction technique by a single surgeon decreasing the heterogeneity of the study group, allowing some conclusions regarding the usefulness of such reconstructions.
Several series have reported promising preliminary outcomes of acetabular reconstructions in patients with combined cavitary and segmental defects treated with TM cups and metallic augments with mechanical failure rates ranging from 0% to 6% [12, 29–31]. Although mechanical buttressing with metallic augments can provide ancillary primary fixation to the cup, they are indicated for segmental rather than cavitary acetabular defects [17, 29]. Outcomes of impaction bone grafting and cemented cups are variable and require careful execution to achieve reliable long-term results [16, 28]. More recent series indicated large cavitary defects can be reliably treated by TM cups even in the face of limited contact with bleeding bone [15]. TM is 80% porous with a microstructure similar to bone and a modulus of elasticity between that of cortical and cancellous bones. Moreover, it has a high coefficient of friction [1, 6, 12]. These improved material characteristics provide a favorable environment for bone ingrowth, bone graft remodeling, and better initial stability. TM cups for salvage of failed acetabular cages with cavitary defects had a radiographic failure rate of 20% at an average 4-year followup and compared favorably with reconstruction by antiprotrusion cages. Repeated reconstruction of an antiprotrusion cage can be technically difficult and entail a substantial risk for neurovascular injury in the face of a distorted ischium, which is often the case after cage failure [14]. Two of the three failures in our study occurred in patients who were treated with constrained liners as a result of abductor weakness and instability. Under these borderline mechanical and biologic conditions for cup fixation and bone ingrowth, constrained liners may be prone to early failure [18, 35] and should be avoided whenever possible.
Use of nonbuttressed TM cups substantially simplified the acetabular reconstruction and allowed substantial functional improvement in 12 of the 15 patients. None of these patients who returned to ambulate with various degrees of walking aids reported symptoms suggestive of loosening at the latest followup. Although longer followup is required, our preliminary results suggest treatment of failed cages by nonbuttressed cups is a viable option when bone stock has been adequately restored. Patients should be followed closely to detect cup migration, which can occur until satisfactory bony ingrowth takes place.
References
Boscainos PJ, Kellett CF, Maury AC, Backstein D, Gross AE. Management of periacetabular bone loss in revision hip arthroplasty. Clin Orthop Relat Res. 2007;465:159–165.
Cabanela ME. Reconstruction rings and bone graft in total hip revision surgery. Orthop Clin North Am. 1998;29:255–262.
D’Antonio JA, Capello WN, Borden LS, Bargar WL, Bierbaum BF, Boettcher WG, Steinberg ME, Stulberg SD, Wedge JH. Classification and management of acetabular abnormalities in total hip arthroplasty. Clin Orthop Relat Res. 1989;243:126–137.
Della Valle CJ. Cementless acetabular reconstruction in revision total hip arthroplasty. Clin Orthop Relat Res. 2004;420:96–100.
Etienne G, Bezwada HP, Hungerford DS, Mont MA. The incorporation of morsellized bone grafts in cementless acetabular revisions. Clin Orthop Relat Res. 2004;428:241–246.
Flecher X, Sporer S, Paprosky W. Management of severe bone loss in acetabular revision using a trabecular metal shell. J Arthroplasty. 2008;23:949–955.
Gill TJ, Sledge JB, Müller ME. The management of severe acetabular bone loss using structural allograft and acetabular reinforcement devices. J Arthroplasty. 2000;15:1–7.
Goodman S, Pressman A, Saastamoinen H, Gross A. Modified sliding trochanteric osteotomy in revision total hip arthroplasty. J Arthroplasty. 2004;19:1039–1041.
Goodman S, Saastamoinen H, Shasha N, Gross A. Complications of ilioischial reconstruction rings in revision total hip arthroplasty. J Arthroplasty. 2004;19:436–446.
Gross AE. Revision arthroplasty of the acetabulum with restoration of bone stock. Clin Orthop Relat Res. 1999;369:198–207.
Gross AE. Grafts and cages: managing massive bone loss. Orthopedics. 2000;23:973–974.
Gruen TA, Poggie RA, Lewallen DG, Hanssen AD, Lewis RJ, O’Keefe TJ, Stulberg SD, Sutherland CJ. Radiographic evaluation of a monoblock acetabular component: a multicenter study with 2- to 5-year results. J Arthroplasty. 2005;20:369–378.
Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51:737–755.
Issack PS, Beksac B, Helfet DL, Buly RL, Sculco TP. Reconstruction of the failed acetabular component using cemented shells and impaction grafting in revision hip arthroplasty. Am J Orthop. 2008;37:510–512.
Lakstein D, Backstein D, Safir O, Kosashvili Y, Gross AE. Trabecular metal cups for acetabular defects with 50% or less host bone contact. Clin Orthop Relat Res. 2009 Mar 10 [Epub ahead of print].
Lavernia CJ, Cook CC, Hernandez RA, Sierra RJ, Rossi MD. Neurovascular injuries in acetabular reconstruction cage surgery: an anatomical study. J Arthroplasty. 2007;22:124–132.
Levine B, Della Valle CJ, Jacobs JJ. Applications of porous tantalum in total hip arthroplasty. J Am Acad Orthop Surg. 2006;14:646–655.
Lombardi AV Jr. Constrained liners in revision: total hip arthroplasty an overuse syndrome: in opposition. J Arthroplasty. 2006;21(Suppl 1):126–130.
Markovich GD. Acetabular reconstruction in revision total hip arthroplasty: a review of options. Am J Orthop. 1998;27:662–670.
Massin P, Schmidt L, Engh CA. Evaluation of cementless acetabular component migration. An experimental study. J Arthroplasty. 1989;4:245–251.
Oakes DA, Cabanela ME. Impaction bone grafting for revision hip arthroplasty: biology and clinical applications. J Am Acad Orthop Surg. 2006;14:620–628.
Paprosky WG, O’Rourke M, Sporer SM. The treatment of acetabular bone defects with an associated pelvic discontinuity. Clin Orthop Relat Res. 2005;441:216–220.
Perka C, Ludwig R. Reconstruction of segmental defects during revision procedures of the acetabulum with the Burch-Schneider anti-protrusio cage. J Arthroplasty. 2001;16:568–574.
Peters CL, Curtain M, Samuelson KM. Acetabular revision with the Burch-Schnieder antiprotrusio cage and cancellous allograft bone. J Arthroplasty. 1995;10:307–312.
Saleh KJ, Holtzman J, Gafni A, Saleh L, Davis A, Resig S, Gross AE. Reliability and intraoperative validity of preoperative assessment of standardized plain radiographs in predicting bone loss at revision hip surgery. J Bone Joint Surg Am. 2001;83:1040–1046.
Saleh KJ, Jaroszynski G, Woodgate I, Saleh L, Gross AE. Revision total hip arthroplasty with the use of structural acetabular allograft and reconstruction ring: a case series with a 10-year average follow-up. J Arthroplasty. 2000;15:951–958.
Schatzker J, Wong MK. Acetabular revision. The role of rings and cages. Clin Orthop Relat Res. 1999;369:187–197.
Schreurs BW, Luttjeboer J, Thien TM, de Waal Malefijt MC, Buma P, Veth RP, Slooff TJ. Acetabular revision with impacted morsellized cancellous bone graft and a cemented cup in patients with rheumatoid arthritis. A concise follow-up, at eight to nineteen years, of a previous report. J Bone Joint Surg Am. 2009;91:646–651.
Siegmeth A, Duncan CP, Masri BA, Kim WY, Garbuz DS. Modular tantalum augments for acetabular defects in revision hip arthroplasty. Clin Orthop Relat Res. 2009;467:199–205.
Sporer SM, O’Rourke M, Paprosky WG. The treatment of pelvic discontinuity during acetabular revision. J Arthroplasty. 2005;20:79–84.
Sporer SM, Paprosky WG. Acetabular revision using a trabecular metal acetabular component for severe acetabular bone loss associated with a pelvic discontinuity. J Arthroplasty. 2006;21:87–90.
Udomkiat P, Dorr LD, Won YY, Longjohn D, Wan Z. Technical factors for success with metal ring acetabular reconstruction. J Arthroplasty. 2001;16:961–969.
Wachtl SW, Jung M, Jakob RP, Gautier E. The Burch-Schneider antiprotrusio cage in acetabular revision surgery: a mean follow-up of 12 years. J Arthroplasty. 2000;15:959–963.
Winter E, Piert M, Volkmann R, Maurer F, Eingartner C, Weise K, Weller S. Allogeneic cancellous bone graft and a Burch-Schneider ring for acetabular reconstruction in revision hip arthroplasty. J Bone Joint Surg Am. 2001;83:862–867.
Yun AG, Padgett D, Pellicci P, Dorr LD. Constrained acetabular liners: mechanisms of failure. J Arthroplasty. 2005;20:536–541.
Acknowledgments
We thank Dr Muheddine Al-Taki, and Matthew MacDonald for their assistance with the data processing and statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
The senior author (AEG) is a consultant for Zimmer (Warsaw, IN). All other authors certify that they do not have commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution has approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
About this article
Cite this article
Kosashvili, Y., Safir, O., Backstein, D. et al. Salvage of Failed Acetabular Cages by Nonbuttressed Trabecular Metal Cups. Clin Orthop Relat Res 468, 466–471 (2010). https://doi.org/10.1007/s11999-009-0935-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-009-0935-2