
Abstract
Metal-on-metal total hip resurfacing arthroplasty has had excellent reported results at early to midterm followup, and some studies suggest that outcomes are comparable to conventional THA. We compared the clinical and radiographic outcomes of two closely matched groups of 54 patients who underwent resurfacing and conventional THA, respectively. Each group consisted of 36 men and 18 women who had a mean age of 52 years and a mean body mass index of 29 kg/m2. At a minimum followup of 24 months (mean, 40 months; range, 24–60 months), the mean Harris hip scores increased similarly in both groups (from 52 to 90 points and from 50 to 91 points for the resurfacing and conventional groups, respectively). Radiographic outcomes, revision rates, complications, pain scores, and satisfaction ratings of the two groups were similar. The patients who underwent resurfacing had higher postoperative weighted activity scores than the patients who underwent conventional THA, although they had higher preoperative weighted activity scores as well. The early outcomes of resurfacing are comparable to those of conventional THA.
Level of Evidence: Level III, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With recent improvements in metal-on-metal bearing designs, total hip resurfacing arthroplasty has grown in popularity as a treatment for symptomatic arthritic hips. Clinical success has been reported in 94% to 100% of patients who underwent resurfacing at short- to midterm followup [1, 6, 11, 12, 14–16]. Survival rates have improved as surgeons have moved beyond their learning curves and refined their techniques [8, 10], so resurfacing may provide comparable results to conventional THA.
Two published reports of small patient groups have directly compared total hip resurfacing arthroplasties with conventional THAs. Vail et al. [16] compared 2-year followup results of 57 resurfaced hips with 93 conventional THAs and reported that functional scores of the two groups were similar, but activity and range of motion scores were greater in the patients who underwent resurfacing. Similarly, Pollard et al. [12] compared two matched groups of 54 patients at followup times of 5 to 7 years and reported similar hip function scores, but the patients who underwent resurfacing had higher activity and quality of life scores. These studies had potential confounding factors, including the learning curves of the procedures, varied followup times, diverse indications for the procedure, medical comorbidities, and unreported preoperative hip scores.
We compared the short-term outcomes of hip resurfacing with conventional THA in two closely matched patient cohorts while addressing the limitations of the previous reports. We specifically assessed satisfaction, pain, weighted activity and Harris hip scores, in addition to complications, revision rates, and radiographic outcomes.
Materials and Methods
We compared 54 patients (54 hips) who were treated with metal-on-metal total hip resurfacing arthroplasties with a group of 54 patients (54 hips) who received conventional THAs during the same time period (November 1, 2002, to January 1, 2005). Both groups of patients had been separately prospectively followed before the retrospective matching was performed. The patients who underwent resurfacing were part of the US Food and Drug Administration multicenter investigational device exemption (IDE) study of the Conserve Plus™ prosthesis (Wright Medical Technology, Arlington, TN). During this time period, the surgeon performed 250 conventional THAs. The indications for both procedures were osteoarthritis, osteonecrosis, or hip dysplasia in patients who had failed nonoperative treatment. We excluded patients who were pregnant, and those who had active human immunodeficiency virus or hepatitis infection, documented allergy to cobalt, chromium, or molybdenum; or a neurologic deficit that might adversely affect gait or weightbearing. The patients who underwent resurfacing came to our institution to request that procedure and were assessed for femoral and acetabular bone quality. If they had no contraindications for resurfacing, including large femoral neck cysts (greater than 2 cm), insufficient femoral head remaining, or osteopenia, they underwent the procedure. The patients who underwent THA chose that procedure for personal reasons or because their insurance required it. Some patients who originally requested resurfacing ended up receiving a THA because of poor bone quality, but those patients were not included in the matched group of this study. A power analysis was performed with the postoperative Harris hip score as the primary outcome, a difference in means of 3 points, and a standard deviation of the difference of 5 points. At an alpha level of 0.01, the sample size of 54 patients was associated with a power of 0.955. We received Institutional Review Board approval to compare the functional and radiographic outcomes of these patients.
To match the patient groups, we identified consecutive groups of patients who underwent resurfacing and conventional THA during the specified time period. Each patient who underwent resurfacing was matched to a patient who underwent THA by gender (exact match), diagnosis (exact match), age (within 3 years), body mass index (within 3 kg/m2), American Society of Anesthesiologists score [13] (exact score), preoperative Harris hip score (within 5 points), and length of followup (within 6 months). Fifty-four of the patients who underwent resurfacing were matched to patients who underwent THA through this process. None of the patients who were selected and matched for this study were lost to followup. Because it is possible there were more complex cases in the conventional THA group, we analyzed the difficulty based on surgical time. No standard cases took longer than 95 minutes (mean, 58 minutes; range, 38–95 minutes), which was similar to the mean of 68 minutes for the resurfacing group (range, 42–100 minutes). The mean surface arthroplasty risk indices (SARI) [2] were 2.4 and 2.6 points for the resurfacing and THA groups, respectively (p = 0.508). Because the surgical times and SARI scores were similar, we believe the groups were well-matched based on complexity.
Each group consisted of 36 men and 18 women who had a mean age of 55 years (range, 35–79 years) (Table 1). The mean preoperative Harris hip scores of the resurfacing and conventional THA cohorts were 52 points (range, 28–71 points) and 50 points (range, 20–73 points), respectively, which were similar (p = 0.107). The mean body mass indices and medical comorbidities of the two groups were also similar. Patients were followed both clinically and radiographically for a minimum of 2 years (mean, 40 months; range, 24–60 months).
All hip resurfacings were performed using an anterolateral approach by the senior author (MAM). The surgeon had performed more than 300 resurfacings before the patient selection process was started to avoid any possible learning curve biases. The Conserve Plus™ hip resurfacing system (Wright Medical Technologies, Arlington, Virginia) was used for all of the procedures. The femoral head component sizes ranged from 38 to 52 mm. The acetabular components were inserted in a press-fit manner after underreaming by 1 mm and all femoral components were cemented. All conventional THAs were performed by the senior author (MAM) using the Stryker Howmedica Osteonics™ Trident® cup with an Accolade™ femoral component (Stryker Orthopaedics, Mahwah, NJ). Femoral head sizes ranged from 22 to 32 mm. Acetabular cups were inserted in a press-fit manner after underreaming by 1 mm and ceramic or standard cobalt chrome alloy femoral heads were used in conjunction with polyethylene liners.
Postoperative rehabilitation was slightly different for the two cohorts. The patients who underwent resurfacing followed the protocol that was put in place for the IDE study: 20% weightbearing for the first 5 to 6 weeks using crutches or a walker followed by 50% weightbearing using a cane or crutch in the contralateral hand until 10 weeks, at which time full weightbearing was allowed. Of note, we presently allow 50% weightbearing initially with progression to full weightbearing at 5 weeks. The patients who received conventional THAs were kept at 50% weightbearing for the first 5 weeks and then advanced to full weightbearing after that time. Otherwise, intraoperative and perioperative management as well as early rehabilitation of both patient groups were the same.
We (MAM, MSM, DRM) examined patients postoperatively, at 6 months, 1 year, and annually thereafter for a minimum of 2 years. Harris hip scores [5] were determined preoperatively and at the followup visits. Additionally, patients were carefully assessed for any perioperative or postoperative complications. Finally, patients were asked to use an 11-point Likert scale [7] to quantify their pain levels and overall levels of satisfaction with the procedure. The pain scale ranged from 0 to 10 points with 0 points indicating no pain and 10 points indicating the worst pain imaginable. For the satisfaction scale, 0 points indicated complete dissatisfaction and 10 points indicated complete satisfaction with the procedure.
We (MAM, MSM) assessed anteroposterior and lateral radiographs of the affected hips at followup visits for any progressive radiolucencies using the zonal analysis of DeLee and Charnley [3] for the acetabulum and Gruen zones [4] for the femoral components of the conventional THAs. For the resurfacing, a similar evaluation was performed on the acetabular cup, and the femoral component was divided into three zones as described by Beaulé et al. [2] for evaluation of radiolucencies. Radiographs were also examined for alignment postoperatively and at followup visits.
In addition to the other outcome variables, we wanted to evaluate whether patients who had undergone resurfacing experienced more active lifestyles postoperatively than the patients who underwent conventional THAs. Preoperative and postoperative weighted activity scores had been collected and recorded for all patients as part of a prospective database. After the patients had been matched and the results had been compiled, the weighted activity scores were reviewed retrospectively. The weighted activity scores were determined by adapting, for THAs, a scoring system that had been previously used for TKAs [9]. At the preoperative and followup visits, each patient answered a questionnaire that asked about the frequency, duration, and competitiveness of the physical activities in which he or she regularly participated. The activities were assigned weighted points based on their levels of exertion and impact. The weighted points ranged from 1 for a low-impact activity such as walking to 3 for a high-impact activity such as basketball. The weighted activity score was calculated by multiplying the frequency (per week), the duration in hours, and the weighted activity points for each activity and summing the products for all the activities (Table 2). Scores ranging from 0 to 8 points indicated low-activity patients and scores of 9 points or higher indicated high-activity patients.
Demographic and outcome variables of the two groups were compared using paired Student’s t tests. All data were analyzed using SPSS software, Version 13.0 (SPSS Inc, Chicago, IL).
Results
At final followup, the mean Harris hip scores of the two patient cohorts were similar (p = 0.771) with a mean scores of 90 points (range, 50–100 points) and 91 points (range, 62–100 points) for the resurfacing and conventional groups, respectively. Patient satisfaction scores were also similar (p = 0.403) with patients undergoing resurfacing reporting a mean score of 9.2 points (range, 2–10 points) and patients undergoing conventional THA reporting a mean score of 8.8 points (range, 0–10 points). Forty-eight of 50 patients who underwent resurfacing (96%) and 46 of 50 patients who received conventional THAs (92%) reported satisfaction scores of 7 points or higher.
Assessment of radiographs revealed all components were well-fixed, except for one shifted acetabular cup in the resurfacing group and one acetabular loosening in the THA group, which are discussed in detail in a subsequent paragraph. The mean femoral component shaft angles in the resurfacing group were 140° (range, 126°–155°) and 166° (range, 145°–182°) on the anteroposterior and lateral views, respectively. The mean cup inclination angle was 38° (range, 25°–60°).
The mean weighted activity score increased from 3 points (range, 0–15 points) preoperatively to 11.5 points (range, 0–32 points) at final followup for the patients who underwent resurfacing and increased from 2 points (range, 0–6 points) preoperatively to 7 points (range, 0–20 points) at final followup for the patients who received conventional THAs. The final mean activity score of the patients who underwent resurfacing was higher (p = 0.0004) than the final mean score of the patients who received conventional THAs. However, the preoperative activity levels of the patients who had surface replacements were also higher (p = 0.01). The mean differences between preoperative and postoperative weighted activity scores for the resurfacing and conventional THA cohorts were 8 points (range, 0–17 points) and 5 points (range, 0–15 points), respectively (p = 0.0004).
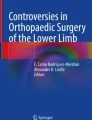
There were two reoperations in each cohort. In the resurfacing group, a 35-year-old man experienced a femoral neck fracture after falling during a soccer game 1 year after his procedure and was revised to a conventional THA. His Harris hip score before the fracture was 100 points and was 95 points at final followup, 3 years after the revision. The other patient who had undergone resurfacing who required a reoperation was a 61-year-old man whose acetabular cup had shifted horizontally on a routine postoperative radiograph that was taken in the recovery room. He was taken back to the operating room, where an inserter was used to reposition the cup and press it into a more secure position (Fig. 1). This patient is now doing well with a Harris hip score of 96 points at a followup time of 3 years after the revision. In the conventional THA cohort, a 51-year-old man had progressive acetabular radiolucencies on radiographs and had a loose acetabular cup. The cup was removed and a new one was placed with screw fixation (Fig. 2). At final followup, 3 years after revision, his Harris hip score was 97 points. Another patient, a 50-year-old man, developed a postoperative infection and underwent a two-stage revision. He now has a Harris hip score of 83 points 2 years after revision. Additionally, one patient from each cohort reported painless decreased range of motion, presumably secondary to excess heterotopic bone formation (Brooker Class II in both patients; Fig. 3). On radiographic analysis, no other patients exhibited any changes in the alignments of their prostheses or any progressive radiolucencies.

Anteroposterior radiographs show the left hip of a 61-year-old man who underwent resurfacing for osteoarthritis. (A) A routine radiograph in the recovery room showed his acetabular cup had shifted, so (B) he was taken back to the operating room where an inserter was used to reposition the cup. (C) It was well-fixed at the 2-year followup.

Anteroposterior (A) and lateral (B) radiographs show the right hip of a 51-year-old man who had progressive radiolucencies around his acetabular cup. (C) A new cup was placed with screw fixation.

Anteroposterior radiographs show the right hips of a 61-year-old man who underwent resurfacing (A) and a 49-year-old man who underwent THA (B). Both of these patients developed painless heterotopic ossification (Brooker Type II).
Discussion
Metal-on-metal total hip resurfacing arthroplasty has grown in popularity and has received much media and international attention. Surgeons who recommend this procedure for young, active patients are often sought out by these patients to perform the procedure as a possible conservative approach to conventional THA. Only two direct comparisons of the two procedures have been published [12, 16], and they had various limitations, which prompted us to perform the present study. This study attempted to address the limitations of the previous studies by matching the patient cohorts according to seven preoperative factors and trying to eliminate the learning curve. The variables that were assessed in this study included postoperative satisfaction, pain, Harris hip and weighted activity scores as well as complications, revision rates, and radiographic outcomes.
There were a number of limitations in the present study. One limitation was the fact that the two groups were not matched for preoperative activity levels, and some selection bias may be present in the final weighted activity scores, because higher-activity patients may have been more likely to request resurfacing procedures. Also, the methodology of the weighted activity score has not yet been validated, although a separate study with this aim is currently in progress. Other limitations include the small number of patients in each group, which restricts full comparison, and the short mean followup duration of 40 months. Nevertheless, the two groups were carefully matched for various demographic factors, preoperative scores, medical comorbidities, and followup times, which reduced many confounding factors. The similar surgical times and SARI scores for the two groups also confirmed the uniformity of the case complexity. We believe the close matching of patient cohorts and the high statistical power of the study make the comparison groups valid. Additionally, because of numerous factors, including patient demand and insurance coverage, it would be very difficult to perform a true randomized prospective study comparing the two procedures.
Our data support recent studies reporting similar short- and midterm results of resurfacing compared with conventional THA. Vail et al. [16] retrospectively compared 57 patients who underwent metal-on-metal total hip resurfacing arthroplasties with 93 who underwent conventional metal-on-polyethylene primary THAs during the same time period. After controlling for age, gender, and preoperative data, they found comparable pain and Harris hip scores between the two cohorts. However, the activity and range of motion components of the Harris hip scores were higher in the resurfacing group. Pollard et al. [12] compared resurfacing and conventional THA by evaluating two groups of 54 patients who were matched by gender, age, body mass index, and preoperative activity levels. At followup times of 5 to 7 years, the Oxford hip scores and complication rates of both groups were similar, but the patients who underwent resurfacing had higher EuroQol quality of life scores and University of California at Los Angeles activity scores. The revision rates were 8% in the conventional THA group and 6% in the resurfacing group. Both of those studies were limited in that they did not evaluate preoperative hip scores, medical comorbidities, indications for the procedures, or learning curves, and they did not match the followup times of the two patient groups. The present study attempted to correct for those factors and found postoperative hip scores and radiographic outcomes were similar for the two procedures.
The present study confirms high activity levels and similar hip scores as well as radiographic outcomes of patients who received resurfacing arthroplasties when compared with closely matched patients who received conventional THAs. It also found similar pain and satisfaction scores. We await longer-term results to further evaluate the efficacy of resurfacing procedures. Additionally, preoperative stratification by activity levels will be conducted in the future in an attempt to further minimize bias.
References
Amstutz HC, Ball ST, Le Duff MJ, Dorey FJ. Resurfacing THA for patients younger than 50 year: results of 2- to 9-year followup. Clin Orthop Relat Res. 2007;460:159–164.
Beaulé PE, Dorey FJ, LeDuff M, Gruen T, Amstutz HC. Risk factors affecting outcome of metal-on-metal surface arthroplasty of the hip. Clin Orthop Relat Res. 2004;418:87–93.
DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976;121:20–32.
Gruen TA, McNeice GM, Amstutz HC. ‘Modes of failure’ of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res. 1979;141:17–27.
Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51:737–755.
Hing CB, Back DL, Bailey M, Young DA, Dalziel RE, Shimmin AJ. The results of primary Birmingham hip resurfacings at a mean of five years. An independent prospective review of the first 230 hips. J Bone Joint Surg Br. 2007;89:1431–1438.
Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932;140:1–55.
Marker DR, Seyler TM, Jinnah RH, Delanois RE, Ulrich SD, Mont MA. Femoral neck fractures after metal-on-metal total hip resurfacing: a prospective cohort study. J Arthroplasty. 2007;22:66–71.
Mont MA, Marker DR, Seyler TM, Gordon N, Hungerford DS, Jones LC. Knee arthroplasties have similar results in high- and low-activity patients. Clin Orthop Relat Res. 2007;460:165–173.
Mont MA, Seyler TM, Ulrich SD, Beaule PE, Boyd HS, Grecula MJ, Goldberg VM, Kennedy WR, Marker DR, Schmalzried TP, Sparling EA, Vail TP, Amstutz HC. Effect of changing indications and techniques on total hip resurfacing. Clin Orthop Relat Res. 2007;465:63–70.
Nishii T, Sugano N, Miki H, Takao M, Koyama T, Yoshikawa H. Five-year results of metal-on-metal resurfacing arthroplasty in Asian patients. J Arthroplasty. 2007;22:176–183.
Pollard TC, Baker RP, Eastaugh-Waring SJ, Bannister GC. Treatment of the young active patient with osteoarthritis of the hip. A five- to seven-year comparison of hybrid total hip arthroplasty and metal-on-metal resurfacing. J Bone Joint Surg Br. 2006;88:592–600.
Saklad M. Grading of patients for surgical procedures. Anesthesiology. 1941;2:281–284.
Schmalzried TP, Silva M, de la Rosa MA, Choi ES, Fowble VA. Optimizing patient selection and outcomes with total hip resurfacing. Clin Orthop Relat Res. 2005;441:200–204.
Treacy RB, McBryde CW, Pynsent PB. Birmingham hip resurfacing arthroplasty. A minimum follow-up of five years. J Bone Joint Surg Br. 2005;87:167–170.
Vail TP, Mina CA, Yergler JD, Pietrobon R. Metal-on-metal hip resurfacing compares favorably with THA at 2 years followup. Clin Orthop Relat Res. 2006;453:123–131.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (MAM) is a consultant for and has received funding from Stryker Orthopaedics (Mahwah, NJ) and Wright Medical Technology (Arlington, TN).
Each author certifies that his institution has approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
About this article
Cite this article
Mont, M.A., Marker, D.R., Smith, J.M. et al. Resurfacing is Comparable to Total Hip Arthroplasty at Short-term Followup. Clin Orthop Relat Res 467, 66–71 (2009). https://doi.org/10.1007/s11999-008-0465-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-008-0465-3