
Abstract
The advantages of sonographic examination are well known, but its main disadvantage is that it might lead to overdiagnosis, which might cause overtreatment. Variations in the incidence of developmental dysplasia of the hip are well known. We ascertained the incidence of neonatal sonographic developmental dysplasia of the hip without considering the development of those joints during followup. All 45,497 neonates (90,994 hips) born in our institute between January 1992 and December 2001 were examined clinically and sonographically during the first 48 hours of life. Sonography was performed according to Graf’s method, which considers mild hip sonographic abnormalities as Type IIa. We evaluated the different severity type incidence pattern and its influence on the total incidence during and between the investigated years. According to our study, sonographic Type IIa has major effects on the incidence of overall developmental dysplasia of the hip with a correlation coefficient of 0.95, whereas more severe sonographic abnormalities show relatively stable incidence patterns.
Level of Evidence: Level I, prognostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Developmental dysplasia of the hip (DDH) is one of the most widely discussed abnormalities in neonates. Previously termed congenital dislocation of the hip, DDH encompasses a group of related pediatric hip disorders, including clinical instability of the hip (neonatal or early postnatal), with or without anatomic dysplasia, subluxation, or dislocation. The definition of DDH is a complex and difficult issue. The question is whether all neonates with slight hip abnormalities can be considered as having DDH or does it apply only to those hips that will remain pathologic if not treated. DDH etiology is obscure and seems multifactorial. DDH is associated with genetics, family history, female gender, skeletal abnormalities, and hormonal and environmental factors, making the definition of the problem difficult. Determining the incidence of DDH based on an uncertain definition is even more difficult, and data on the subject in the literature vary widely [15, 16, 26, 28, 29, 31].
The literature on DDH incidence and the way it is diagnosed has changed over the years [4, 6, 27]. At the beginning, before the introduction of routine screening programs for detecting DDH, incidence was estimated at 0% to 40%. Until the 1980s when routine screening for DDH was performed clinically, incidence was 0.41% to 16.8%. Since the 1980s, after the introduction of sonographic techniques for investigation of pediatric hip and neonatal screening, incidence rose to 4.4% to 52%. This wide range of numbers is, as suggested earlier, in part attributable to the varying definitions and diversity between inclusion and exclusion criteria in the protocols used by various authors.
It is now widely accepted ultrasound is the most sensitive method to evaluate infant hips and is sometimes even too sensitive [4, 10, 25]. It is an excellent tool for evaluating acetabular development and for followup during and after treatment. On the other hand, it is well known that sonographic screening of the neonatal hip, combined with clinical examination, can lead to overdiagnosis followed by overtreatment when not used properly [4, 10, 25]. Two principal methods for examining the infant hip by means of sonography have been used recently. The method of Graf [10] is more static but describes the exact anatomic structures of the hip. The method of Harcke et al. [13] is more dynamic, resembling clinical examination under sonographic control. Patel et al. [20] reported most infants with DDH have no risk factors and selective ultrasound screening failed to show benefit.
We believe all neonates should be screened sonographically and clinically examined. In the first 2-year period of this program, we reported a sonographic incidence of DDH of 5.5% [4]. We suggested calling those hips that underwent subsequent treatment “true DDH” and this decreased the incidence to 0.5% [4].
We assessed 10 years of experience with clinical-sonographic neonatal screening for DDH within the first 48 hours of life, without considering the development of those joints in the following years.
Materials and Methods
Since January 1992, each neonate born at our hospital was routinely examined clinically and sonographically for hip abnormality within the first 48 hours of life by experienced neonatologists (clinically) and pediatric orthopaedic surgeons (VB, ME) (sonographically) working independently. From January 1993 until the end of 2001, we examined 45,497 neonates (90,994 hips) clinically and sonographically (Table 1). For this report we excluded 4620 patients (9240 hips) in the first year we started using sonography (1992), because some data were missing from our records (Table 1). No other neonates were included in the study.
The sonographic investigation was performed by the senior author (VB) or under his supervision. Since January 2000, another senior pediatric orthopaedic surgeon (ME) performed the sonographic examinations, first under the supervision of the senior author and later independently. The clinical examination by the pediatric orthopaedic surgeon was performed only when the sonographic examination revealed hip abnormality. We performed the clinical examination as instituted by Ortolani [19] and Barlow [1]. and the sonographic investigation with Graf’s method [10, 11] using a 7.5-MHz transducer. Data on family history, gender, other skeletal abnormalities, and so on, were not evaluated, because this was not an epidemiologic study.
The sonographically abnormal hips were classified by Graf’s classification [10, 11]. Graf’s method is based on an exact anatomic description of the infant hip using sonography and is divided into four major types (Types I–IV). We considered Graf’s Types Ia and Ib as mature joints and Type IIa as physiologically immature. For statistical purposes, we considered Type IIa hips as “pathologic,” because they were not fully mature hips, progressing (at least theoretically) to Type IIb or worse.
We first determined the yearly incidences of the different DDH types per year. We evaluated the pattern of total DDH incidence consisting of all the sonographically pathologic hips during the investigated years. The incidence pattern of each type was compared between the years as was the relation and influence of each type on the total incidence. We compared Type IIa with the other severity types (Types IIc, D, III, IV) and their patterns through the years.
Statistical evaluation was with a “crosstabs” chi square. The Pearson correlation coefficient was calculated.
Results
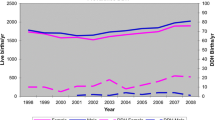
In 1993, the total neonatal incidence of DDH, including Graf Type IIa, was 5.26%, changing and decreasing gradually (p < 0.001) until it reached 3.41% in 1999 (Table 2). It increased (p = 0.08) again to 4.51% in 2001, still lower (p < 0.001) than it was in 1993. Assessing Graf Type IIa separately, the incidence changed similarly, from 2.45% in 1993 decreasing (p = 0.01) to 1.48% in 1997 and continuing to decrease (p = 0.003) to 1.03% in 1999. In 2000 and 2001, Type IIa incidence increased again, in keeping with the total incidence. Nevertheless, Type IIa incidence was still less than it was in 1993 (p < 0.001). The decrease in Type IIa incidence (p < 0.001) over the years is expressed by a linear regression line slope (Fig. 1). Sonographic abnormalities other than Type IIa were stable and did not change. Concerning Type IIa, the mean incidence between 1993 and 1996 was 2.63%, decreasing (p < 0.001) to 1.31% in the second period. We found no changes between the successive years except between 1996 and 1997 (p < 0.013) and between 1998 and 1999 (p < 0.003). The pattern of incidence changed when comparing all neonatal DDH with Type IIa during the investigated period (Fig. 2). The constantly changing Type IIa incidence had a major influence on the overall results, whereas Type IIc and more severe sonographic hip abnormalities had relatively stable patterns of incidence. We observed a correlation (r = 0.95) between total incidence and Type IIa.

Sonographic incidence of Type IIa developmental dysplasia of the hip is compared with other hip abnormalities in the assessed period adding the regression lines, which demonstrate the pattern of the incidence changes during the reported years.

The incidence of total developmental dysplasia of the hip is compared with the incidence of Type IIa developmental dysplasia of the hip per year adding their regression lines showing the pattern of the changes during the reported years.
Discussion
This study was constructed to ascertain sonographic DDH incidence over a long period of time without considering the later development and treatment of these hips or epidemiologic, demographic, or other factors. Sonography of the pediatric hip is highly sensitive but can lead to overdiagnosis. Using Graf’s method of sonography, even minimal anatomic abnormalities can be detected, most of which will not affect the later development of the hip, which will go on to become normal. In a previous study, we suggested overtreatment can be avoided with correct use [4].
The study was limited to assessing incidence only. We did not ascertain any factors that might have influenced the overall incidence of DDH or the relative incidences of the various Graf types (eg, gender, presentation at delivery). We have no formal study to examine learning curves, although we believe the data reflect in part a learning curve.
Sonographic DDH incidence using Graf’s method as reported in the literature varies between 4.44% and 51.8% (Table 3) [2–5, 7–9, 14, 17, 18, 21–24, 27, 30]. Such incidence rates differ from those reported in previous estimated and clinical screening periods [2–5, 7–9, 14, 17, 18, 21–24, 27, 30]. and are essentially higher than what we call the true incidence of DDH. In a previous study, we reported an overall sonographic incidence of DDH as high as 5.51%. From these, only 0.5% abnormal hips with sonographic DDH did not progress to normal and needed treatment; these were defined as “true DDH” [4]. These data confirm Barlow’s statement, suggesting 88% of unstable hips will eventually become normal without treatment [1].
In 2000, another senior pediatric orthopaedic surgeon (ME) joined our unit, and he performed the neonatal hip screening, first under the supervision of the senior author. At the beginning of 2001, he started to investigate neonatal hip sonography independently and, to be on the safe side, considered Type Ib hips as Type IIa. This, in our opinion, explains the increased incidence pattern of DDH from 3.53% to 4.51% in this period based mainly on Type IIa hip incidence changes. Our results are very similar to those published by Toma et al. [29] describing the incidence of DDH according to US investigations as 4.7% and Type IIa incidence as 3.36%.
Our continuing study confirms our earlier contention that the diagnosis of neonatal hip abnormalities carried out during the first days of life are different from true DDH incidence. They are higher but can serve as a baseline for further followup until repeated clinical-sonographic investigation shows a necessity for treatment.
Our data suggest the differences in the incidence pattern of DDH during the years studied were influenced by Type IIa and not by “changing” of the incidence itself. Sonographic incidence of all types except Graf’s Type IIa did not change and is close to that reported previously [4, 12]. It is well known that ultrasonographic investigation depends on the examiner’s skill and equipment quality. We believe the difficulties are mainly with hips associated with mild or very mild sonographic abnormalities, defined as Type IIa according to Graf’s classification. More severe sonographic hip abnormalities are recognized more easily, even by the less experienced investigator. We believe the data suggest an understanding of mild hip sonographic abnormality (Type IIa hips) needs a longer period of training until the investigator achieves enough experience in performing neonatal hip sonography.
References
Barlow TG. Early diagnosis and treatment of congenital dislocation of the hip. J Bone Joint Surg Br. 1962;44:292–301.
Baronciani D, Atti G, Andiloro F, Bartesaghi A, Gagliardi L, Passamonti C, Petrone M. Screening for developmental dysplasia of the hip: from theory to practice. Collaborative Group DDH Project. Pediatrics. 1997;99:E5.
Bialik V, Berant M. ‘Immunity’ of Ethiopian Jews to developmental dysplasia of the hip: a preliminary sonographic study. J Pediatr Orthop B. 1997;6:253–254.
Bialik V, Bialik GM, Blazer S, Sujov P, Wiener F, Berant M. Developmental dysplasia of the hip: a new approach to incidence. Pediatrics. 1999;103:93–99.
Dorn U, Hattwich M. Initial experience using routine hip sonography in newborn infants [in German]. Wien Klin Wochenschr. 1987;99:92–95.
Edelstein J. Congenital dislocation of the hip in Bantu. J Bone Joint Surg Br. 1966;48:397.
Exner GU. Ultrasound screening for hip dysplasia in neonates. J Pediatr Orthop. 1988;8:656–660.
Falliner A, Hahne HJ, Hassenpflug J. Ultrasound screening of neonatal hips. Monatsschr Kinderheilkd. 1996;144:1223–1229.
Ganger R, Grill F, Leodolter S. Ultrasound screening of the hip in newborns: results and experience. J Pediatr Orthop. 1988;8:12–16.
Graf R. Guide to Sonography of the Infant Hip. Stuttgart, Germany: George Thieme Verlag; 1987.
Graf R, Tschauner C, Klapsch W. Progress in prevention of late developmental dislocation of the hip by sonographic newborn hip ‘screening’: results of a comparative follow-up study. J Pediatr Orthop. 1988;8:12–16.
Grill F, Muller D. Results of hip ultrasonographic screening in Austria [in German]. Orthopade. 1997;26:25–32.
Harcke HT, Clarke NM, Lee MS, Borns PF, MacEwen GD. Examination of the infant hip with real-time ultrasonography. J Ultrasound Med. 1984;3:131–137.
Hauck W, Seyfert UT. Ultrasound study of the newborn hip: results and consequences [in German]. Z Orthop Ihre Grenzgeb. 1990;128:570–574.
Klisic PJ. Congenital dislocation of the hip—a misleading term: brief report. J Bone Joint Surg Br. 1989;71:136.
Kokavec M, Makai F, Maresch P. Present status of screening and prevention of developmental dysplasia of the hip in the Slovak Republic. J Pediatr Orthop B. 2003;12:106–108.
Kowalczyk B, Felus J, Kwinta P. Developmental dysplasia of the hip: the problem in the diagnosis process in our own experience [in Polish]. Med Wieku Rozwoj. 2005;9:395–406.
Lotito FM, Riccio R, Peluso M, Giustardi A. Ultrasound screening for neonatal dysplasia of the hip. Riv Ital Pediatr. 1990;16:657–661.
Ortolani M. Congenital hip dysplasia in the light of early and very early diagnosis. Clin Orthop Relat Res. 1976;119:6–10.
Patel H. the Canadian Task Force on Preventive Health Care. Preventive health care, 2001 update: screening, management of the hip in newborns. CMAJ. 2001;164:1669–1677.
Pauer M, Rossak K, Meilchen J. Hip screening of newborn infants. Type classification, therapy and follow-up [in German]. Z Orthop Ihre Grenzgeb. 1988;126:260–265.
Reibel T, Herzig N, Nasir R. Neonatales Huft-Screening. Monatsschr Kinderheilkd. 1995;143:268–273.
Reibel T, Nasir R, Kaeding M, Eckart L. Worsening found by continuous observation of the hip joints in neonatal screening. Monatsschr Kinderheilkd. 1990;138:664–669.
Rosendahl K, Markestad T, Lie RT. Ultrasound in the early diagnosis of congenital dislocation of the hip: the significance of hip stability versus acetabular morphology. Pediatr Radiol. 1992;22:430–433.
Rosendahl K, Markestad T, Lie RT. Ultrasound screening for developmental dysplasia of the hip in neonate: the effect on treatment rate and prevalence of late cases. Pediatrics. 1994;94:47–52.
Svec A, Kokavec M. Sonograficky skrining—moderny trend v prevencii vyvojovej dysplazie koxy. Detsky Lekar Marec. 2001;46:34–38.
Szoke N, Kuhl L, Heinrichs J. Ultrasound examination in the diagnosis of congenital hip dysplasia of newborns. J Pediatr Orthop. 1988;8:12–16.
Tachdjian MO. Congenital dysplasia of the hip. In: Tachdjian MO, ed. Pediatric Orthopedics. Vol 1, 2nd ed. Philadelphia, PA: WB Saunders; 1990:297–526.
Toma P, Valle M, Rossi U, Bruneughi GM. Paediatric hip—ultrasound screening for developmental dysplasia of the hip: a review. Eur J Ultrasound. 2001;14:45–55.
Tonnis D, Storch K, Ulbrich H. Results of newborn screening for CDH with and without sonography and correlation of risk factors. J Pediatr Orthop. 1990;10:145–152.
Weinstein SL. Developmental hip dysplasia, dislocation. In: Morrissy RT, Weinstein SL, eds. Lovell and Winter’s Pediatric Orthopaedics. 4th ed. Philadelphia, PA: Lippincott-Raven; 1996:903–943.
Acknowledgments
We thank Mrs Myrna Perlmutter for her help in the preparation of the manuscript and Mrs Ronit Leiba for help with the statistical analysis. We are very grateful to the medical staff of the Neonatal Unit who performed all the routine clinical examinations.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution has waived or does not require approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
About this article
Cite this article
Peled, E., Eidelman, M., Katzman, A. et al. Neonatal Incidence of Hip Dysplasia. Clin Orthop Relat Res 466, 771–775 (2008). https://doi.org/10.1007/s11999-008-0132-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-008-0132-8