
Abstract
Purpose of Review
The incidence of lymphatic leakage (iatrogenic and non-iatrogenic) is growing in cancer population due to the increased complexity of the surgical procedures and improved overall survival in cancer patients. The purpose of this article is to review the contemporary approach in the field of percutaneous lymphatic embolization in cancer patients with lymphatic leaks.
Recent Findings
Since the advent of intranodal lymphangiography in 2011 alongside with the MR and CT lymphangiography, the accuracy of diagnosis of the lymphatic diseases has significantly improved significantly. These advancements have triggered a revival of minimally invasive lymphatic interventions.
Summary
Lymphatic embolization is expanding from the classic indication, thoracic duct embolization, to other lymphatic disorders (chylous ascites, lymphoceles, liver lymphorrhea, protein-losing enteropathy). The growth of lymphatic research and the standardization of the lymphatic interventions require a multidisciplinary and collaborative approach between physicians and researchers.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Lymphatic-related complications (e.g., chylothorax, chylous ascites, and lymphoceles) are increasing in cancer patients due to the longer survival, furthering surgical complexity, and non-iatrogenic cancer complications. Understanding the anatomy and pathophysiology of the lymphatic system is crucial in diagnosing and treating these patients. In the last two decades, the refinement of the lymphatic imaging (e.g., CT and MR lymphangiography) and the development of intranodal lymphangiography (IL) and lymphatic embolization have revolutionized the diagnosis and treatment of oncologic patients with lymphatic leakage. The aim of this review is to illustrate the anatomy, pathophysiology, and imaging of the lymphatic system with a focus on pathological states in cancer patients and percutaneous management.
General
Anatomy of the Lymphatic System
The lymphatic system has a key role in body homeostasis, fat transportation from the intestine to the blood, and in immunity. Lymph is constituted by white blood cells, proteins, and fat (e.g., chylomicrons and triglycerides) which come from the plasma and flow to the interstitial tissue entering the lymphatic capillaries, vessels, lymph nodes, and lymphatic trunks. The anatomy of the lymphatic system closely follows the vascular system [1••]. The lymphatic system is absent in the central nervous system and bone marrow. Lymph flows from the lymphatic vessels in the lower extremities to via a complex and variable network of channels and nodes from the inguinal region along the iliac vessels to the retroperitoneum where it drains into the right and left lumbar trunks. These trunks connect with the cisterna chyli (CC), located at L1–L2 vertebral level in the right retrocrural space, which can measure up to 2 cm in diameter. The thoracic duct (TD) is the continuation of the CC and courses cranially between the azygos vein and aorta to the level of the T5–T7 vertebrae, where it crosses to the left chest and drains at the junction of the left jugular-subclavian junction (Fig. 1) [1••]. The liver and intestine are the main contributors of lymph via hepatic and intestinal trunks, which also drain into the CC [2]. The right lymphatic duct and TD are the two main lymphatic pathways in the body. The right lymphatic duct drains the right upper extremity, right thorax, and the right head and neck, whereas the TD drains the rest of the body [3]. Anatomic variations are very common (40–60%) [4]. The antegrade flow of the lymphatic fluid is due to muscle contractions and respiratory phasicity along with the presence of one-way valves to prevent reflux of the lymphatic fluid [1••].

Anatomy of the thoracic duct and cisterna chyli
Etiology and Pathophysiology of Chyle Leak
There are two general causes of chyle leak in cancer patients (Table 1): (1) non-iatrogenic causes arise from increases in lymphatic pressure, which can be due to malignant infiltration and obstruction of the lymphatic system, portal hypertension, or elevated central venous pressure which leads to increased lymph production [1••] and (2) iatrogenic causes are due to thoracic or abdomino-pelvic surgery. This is the most common cause of lymphatic leakage [5, 6]. Determining the etiology of the chyle leak is crucial to its subsequent management.
Clinical Manifestation and Laboratory Findings of Chyle Leak
Lymphatic leakage can cause serious metabolic derangements due to the depletion of proteins, fats, immunoglobulins, water, vitamins, and electrolytes which can lead to dehydration, electrolyte imbalance, malnourishment, and infection [1••]. However, these usually arise after a significant amount of chyle has been lost.
There are several major manifestations of chylous leak. Chylothorax (CX) is the accumulation of lymphatic fluid in the thoracic cavity and can present with shortness of breath, chest pain, and fever[4]. Chylous ascites (CA) is the accumulation of lymphatic fluid in the peritoneal cavity and can be associated with abdominal distension, anorexia, diarrhea, nausea, weight gain, fever, and enlarged lymph nodes [1••]. A lymphocele is a contained lymphatic leak, typically located in the pelvis or retroperitoneum, and can cause pain, infection, lower limb edema, venous thrombosis, and even compress pelvic organs [7]. Drainage of the fluid accumulating in the pleura, peritoneum, or lymphocele is the first step in managing these patients. Although chyle is milky in appearance, due to the presence of chylomicrons, not all milky turbid fluids are chyle and it should be differentiated from pseudochylothorax and pseudo-chylous ascites. Chylous fluid is characterized by elevated triglyceride levels usually greater than 100–150 mg/dL [4, 8]. Cholesterol in CX is usually less than 200 mg/dL, while in pseudochylothorax, this level is typically above 200 mg/dL [4]. Similarly, CA should be differentiated from pseudoCA, which is secondary to infection or malignancy without high triglycerides levels [1••]. Pleural and peritoneal fluid should be sent for cell count, microbiological evaluation, glucose, total protein, lactate dehydrogenase, triglyceride, and cholesterol level [6]. In CA, the serum to ascites albumin gradient is a good test to rule out ascites secondary to portal hypertension. Chylous fluid should also be differentiated from purulent fluid (e.g., empyema) which may also have a milky white appearance. Chylous fluid can lack a classic milky white appearance if the patient is fasting, in a post-operative state, or in patients with pelvic or low retroperitoneal leakage in which the fat content of the lymphatic fluid is low, below the return of triglyceride-rich chyle from the bowel.[4]. Other laboratory findings to support chylous leak include cell count above 500 with lymphocytic predominance, total protein between 2.5 and 7.0 g/dL, SAAG below 1.1 g/dL, and lactate dehydrogenase between 110 and 200 IU/L. Microbiological cultures can be positive in cases of secondary infection. Additionally, cytology may be positive due to superimposed malignancy. Amylase elevation can be seen in cases associated with pancreatic surgery and in these cases, glucose may be below 100 mg/dL [6]. If the diagnosis of lymphatic leakage has not been established or is confounded, chylomicron determination is gold standard for diagnosis (83% sensitivity and 100% specificity) [4].
Imaging in Chyle Leak: CT, Lymphoscintigraphy, and MRI
Determining the location and etiology of the chyle leak is the first step in the treatment. Imaging studies including computed tomography (CT), magnetic resonance imaging (MRI), radionuclide lymphoscintigraphy (LS), and pedal or intranodal lymphangiography are the most commonly used studies [4]. MRI and CT can diagnose masses and/or enlarged lymph nodes that might be obstructing the lymphatic pathway, as well as detecting the site of the lymphatic injury in post-operative cases [1••].
CT
Both chyle and water can have similar density on CT, but chyle can be differentiated from acute hemorrhage in post-operative cases [6]. The presence of a fat-fluid level is diagnostic of chyle leak [9]. CT can also show the site and extent of the chyle leak in post-operative cases, especially when there is a suspicion of TD injury [1••]. CT can be performed after direct opacification of the TD with oral fat emulsion [6] or with a water-soluble iodinated contrast medium[10]. Patel et al. highlighted the feasibility of intranodal CT lymphangiography (ICTL) in the diagnosis and planning of subsequent intervention in patients with thoracic lymphatic disorders and represent a good alternative to dynamic contrast-enhanced MR lymphangiography (DCMRL).
Lymphoscintigraphy
LS has a functional and anatomical value in chyle leak workup as it can diagnose abnormal lymphatic drainage in patients with suspected chyle leak with an overall sensitivity of 88% [1••]. One of its key advantages is that it can be repeated without side effects, although poor spatial and temporal resolution, lack of standardization, and exposure to ionizing radiation remain a drawback in using this modality [6]. SPECT/CT is a very helpful addition to LS as it provides better anatomic localization of the chyle leak and aids in treatment planning, whether surgical or percutaneous interventions are performed [1••].
MRI
MR lymphangiography and DCMRL with intranodal injection of gadolinium-based contrast have advantages over traditional lymphangiography. The lower viscosity of gadolinium makes it move faster through the lymphatic vessels and opacifies the lymphatic system faster than the higher viscosity ethiodized oil [11••]. MRI also provides better image quality than fluoroscopy, giving more precise localization of the lymphatic system and better delineation of the leak/obstruction site that is key to planning therapeutic intervention (Fig. 2). [1••] Gurevich et al. found that DCMRL can reveal the abnormal retroperitoneal lymphatic pathways that extend to the mediastinum and cause CX as opposed to those patients with CX coming from TD only. Identification of this defective retroperitoneal pathway avoids unneeded interruption of the TD flow via ligation and/or embolization [11••].

MR lymphangiography and intranodal lymphangiography. Patient with history of left chest lymphatic leakage status post several attempts of thoracic duct embolization and surgical ligation of the TD after neck surgery. Left upper chest throbbing pain. Left: MR lymphangiography showed an abnormal network of dilated lymphatic vessels extending from the axilla to the left neck (arrowheads). A short segment of the thoracic duct is identified in the upper chest (arrow). Right: intranodal lymphangiography via a left axillary node (arrow) with redemonstration of the lymphatic anomaly arising from the axillary nodes and the left chest wall lymphatic vessels
Percutaneous Lymphangiography
Percutaneous lymphangiography remains the gold standard in the detection and treatment of chyle leaks. It can detect lymphatic obstruction, leakage, lymphatic-venous fistula, abnormal retroperitoneal lymph nodes, and patency of the TD. However, there is a risk of complications including fat embolism, transient lymphedema, CA and/or CX, and contrast reaction [6]. Intranodal lymphangiography (IL) is performed by ultrasound-guided access to groin lymph nodes using a 25-gauge needle where the tip is placed at the corticomedullary junction and ethiodized oil is injected and monitored moving through the lymphatic system on fluoroscopy. The rate of lymphatic leak detection varies depending on the clinical setting, typically lower in CA than CX cases [12]. If hepatic lymphorrhea is suspected after hepatic or gastric surgery, percutaneous transhepatic lymphangiography can be performed by accessing the periportal hepatic lymphatics using a Chiba needle [13]. Lymphangiography can be therapeutic due to embolic properties of ethiodized oil. However, its therapeutic effect is limited by the volume of the chyle leak where it is more likely to be successful in low output leaks (less than 500 mL/day) [1••].
Chylothorax
CX is usually iatrogenic in cancer patients. Post-esophagectomy chylothorax occurs in 1.9–3.8% of patients, and similar rates have also been seen in pulmonary resections. CX is associated with an increased rate of major complications and length of stay in post-surgical patients. [14,15,16,17]. Non-iatrogenic CX can occur in the setting of lymphoma or metastatic disease and portends a poor outcome [18,19,20]. Dr. Constantine Cope pioneered thoracic duct embolization (TDE) to treat CX in the 1990s and it is now a well-established technique with a high success rate and fewer complications than thoracic duct ligation [21,22,23,24,25,26]. Patients should be considered for TDE if the conservative treatment fails (dietary modification and octreotide), particularly in cases with high output (> 500–1000 mL/day) and/or signs of clinical deterioration due to metabolic, electrolyte, or immunologic deficiency [25].
TDE Technique
IL allows for more reliable and faster identification of the TD and the lymphatic leak [12, 14, 27,28,29]. Once the area of leakage has been identified, trans-abdominal access of the TD is performed via CC, TD, or a lumbar trunk with a 21- or 22-gauge needle. A 0.018 wire is used to catheterize the TD and a microcatheter is advanced into the cranial aspect of the TD. Then, TDE is usually done with a combination of coils and glue (Fig. 3). When the TD cannot be selectively catheterized, needle disruption of the TD may also help to seal the leak off. The TD can also be accessed via retrograde transvenous approach from the left subclavian vein, cervical access under ultrasound or fluoroscopic guidance, and directly through the leak/chest tube [24, 30••, 31,32,33]. Stent graft TD reconstruction is a promising technique that allows to maintain normal physiologic lymphatic drainage but there is very limited experience [34, 35••].

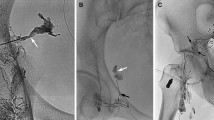
Thoracic duct (TD) embolization. Patient with history of lung carcinoma status post lobectomy complicated by chylothorax. Left: intranodal lymphagiography. Fluoroscopic image of the chest demonstrating the TD (arrow) filled with lipiodol and an area of lipiodol extravasation in relation with a lymphatic leak (arrowhead). Center: fluoroscopic image of the cannulation of the TD with a 22G needle and advancement of a 0.018 wire. Right: Final fluoroscopic image post TD embolization. A microcatheter is advanced over the wire and the TD is embolized with microcoils (arrowhead) and glue (arrow)
Outcomes of Percutaneous Treatment for Chylothorax
Outcomes of lymphangiography and TDE depend on the patient’s anatomy and technical success. If the TD can be visualized and accessed, embolization can be performed. In these cases, there is a high rate of clinical success (90%), particularly in iatrogenic and low output leaks (< 1L/day). In cases without standard anatomy (plexus type TD) or there is technical failure, lymphangiography may help heal the leak as ethiodized oil slows down the lymphatic flow, but overall success rates are lower. Higher output and leaks due to infiltrative or non-iatrogenic causes also have lower success rates.
Overall, success rates for TDE vary between 55 and 90%. Cope and Kaiser initially reported a success rate of 73.8% for TDE. Itkin et al. evaluated 109 patients with iatrogenic CX, with an overall clinical success rate of 90%. [24, 31] Pamarthi et al. retrospectively reviewed 120 TDE and disruption procedures in 105 patients (43 leaks secondary to esophagectomy and 39 after pulmonary resection). TDE clinical success was achieved in 72%. When cannulation cannot be performed, TD disruption clinical success was 55% [36]. This review also noted that successful cases of TDE had lower volumes of effusion, average 770 mL/day compared with 1775 mL/day for unsuccessful attempts [36].
In a study from the Mayo clinic, 40 patients underwent lymphangiography, and a leak was identified in 34 patients. TDE was only performed on 19 patients due to inability to cannulate the CC and it was clinically successful in 78.9% [37]. Several smaller studies evaluating leak have demonstrated clinical success in the range of 55.6–80% for leak after esophageal surgery and 83.3% after pulmonary resection [20, 38]. It is important to note that TDE can only be performed if an accessible portion of the lymphatic system is identified. If favorable anatomy is not identified, needle disruption can be used and has shown to be effective in some cases [36, 39].
Lymphangiography and TDE are less successful in patients with infiltrative etiologies such as lymphoma or metastasis. In a series of 33 patients who underwent attempted TDE for non-traumatic chylous leak, nine patients with lymphoma were included. Out of these patients, six had occlusion of the TD, two were normal, and only one patient had an identifiable leak. Only three patients were successfully catheterized and treated [12, 13, 28]. Pamarthi et al. also reported lower success with non-traumatic CX, albeit with a small number of patients [36].
Due to the viscosity of ethiodized oil, IL can be therapeutic by slowing the lymphatic flow down. In a retrospective review by Jardinet et al., 18 patients underwent IL and 15 of those patients had resolution of their post-surgical refractory chylothorax [40••]. A study by Yannes et al. had similar results with a clinical success rate of 71% in 57 patients with CX. Clinical success rates with therapeutic INL were similar to TDE for patients with less than 500 mL/day of chylous output [41].
Complications of TDE
Acute direct procedure-related complications include pulmonary embolism from the embolic agent, shearing of the wire during TD cannulation (without long-term sequelae), IVC and renal vein thrombus, and intra-abdominal hematoma, which have been reported, but are rare [23, 28, 32, 34, 39].
Chronic complications can occur after TDE due to pressure-related changes after altering physiologic lymphatic flow and despite the development of lympho-venous communications. These complications are most often transient and mild; however, some may require further treatment [24, 42]. In a retrospective review (78 patients, mean follow-up 34 months), Laslett et al.* found the rate of probably related long-term complications after TDE to be 14.3%: lower extremity swelling (8%, typically mild and limited), abdominal swelling (6%, mild), and chronic diarrhea (12%) [43].
Alternative Therapies
Lymphangiography and TDE are the mainstays of treatment after failure of conservative therapy. However, there are several other treatment options for chylothorax, including TD ligation, pleurodesis, and pleurectomy. While these procedures have relatively high success rates, they also have significant morbidity and mortality, up to 38.3 and 25%, respectively [25, 44]. Additional options for management include the placement of a drainage catheter or a pleurovenous shunt in refractory cases [25]. These treatments offer symptomatic relief, but as the underlying leak is not corrected, these patients remain at risk for nutritional/metabolic derangements [45].
Chylous Ascites
CA may occur after oncological abdominal surgery, particularly in patients with upper abdominal and retroperitoneal resections in approximately 7% of the cases. First-line treatment is conservative management (low fat diet/TPN alone or in combination with somatostatin/octreotide) [46, 47]. There are limited therapeutic options for CA; therefore, controlling the underlying disease and the conservative measures has been the main stay of management. Percutaneous treatment options include paracentesis, peritoneovenous shunt, and lymphatic embolization (LE). Trans-jugular intrahepatic porto-systemic shunt could be a potential option in patients with CA due to cirrhosis and portal hypertension, as it is known to decrease the lymphatic hypertension.
Paracentesis and Denver Shunt
Large-volume paracentesis can be used for diagnostic purposes and symptomatic relief, but repeated paracentesis can lead to severe malnutrition, electrolytic imbalance, and immunosuppression. A peritoneovenous shunt is a catheter with two limbs (peritoneal cavity and central veins) connected by a unidirectional pump. This shunt allows the chyle to return the systemic circulation, preventing metabolic derangements. [48] Yarmohammadi et al. studied the efficacy of Denver shunt placement in patients with refractory CA in cancer patients with focus on patients with a history of retroperitoneal lymph node dissection, reporting 90% clinical success [49, 50••]. Reported complications of this shunt include occlusion, venous thrombosis, fat embolism, DIC, and infection [49, 50••, 51].
IL and Lymphatic Embolization
IL and LE are nowadays gaining popularity in the management of CA.
Technique
IL is performed by tracking the ethiodized oil under fluoroscopy throughout the abdomen and pelvis seeking contrast extravasation as a sign of an underlying leak. The main drawback of this technique is the inability to evaluate the leaks coming from hepatic and intestinal lymphatic ducts [1••]. For this reason, it has been suggested to carry out retrograde access of the TD (transvenous approach or direct percutaneous puncture in the neck with ultrasound or fluoroscopic guidance) [32, 52,53,54]. Once the TD is catheterized, an occlusion balloon can be advanced in a retrograde fashion towards the lower end of the TD. Contrast injection after balloon inflation could opacify the abdominal/retroperitoneal ducts and hepatic and intestinal ducts and help identify the site of the leak.
If IL demonstrates a site of leakage, percutaneous glue (i.e., n-butyl cyanoacrylate [NBCA]/ethiodized oil mixture) embolization is performed under fluoroscopic guidance targeting the lymphatic channel or the closest lymph node feeding the leak (Fig. 4) [55, 56]. In cases of retrograde access and identification of multiple chyle leaks, retrograde embolization through the balloon occlusion catheter can be performed [57, 58]. Mesenteric IL has also been suggested to evaluate abdominal lymphatic channels not visualized on the standard inguinal IL [59]. Even when no leak is identified, therapeutic lymphangiography can lead to the cessation of leak [60, 61].

Chylous ascites embolization. Patient with history of renal cell carcinoma status post left nephrectomy and lymphadenectomy and complicated by chylous ascites. Left: fluoroscopic image after intranodal lymphangiography. Filling of the lymphatic nodes and vessels in the left pelvis with lipiodol extravasation in relation with a lymphatic leak at L4 level (surgical clips). Right: fluoroscopic image immediately after the glue injection. The lymphatic leak is identified at L4 level (arrow) and a 22G needle was used to access a left common iliac node under fluoroscopy (arrowhead). Glue injection was performed with a glue/lipiodol ratio of 1:5
Outcomes and Safety
The available data about lymphatic interventions for evaluation and management of CA is heterogeneous and limited to small case series and retrospective studies. Hur et al. reviewed 27 patients with chylous leaks, 17 of which had CA. Clinical success after lymphangiography with or without embolization was achieved in 14/17 patients (82%) [55]. Nadolski et al. reviewed a cohort of 31 patients with refractory CA with traumatic and non-traumatic etiology, and leak was identified in 55% of the patients. LE was performed in 65% of the cases with clinical success in 82% with an overall success rate of 52% [12]. Majdalany et al. reviewed 21 patients with iatrogenic CA who underwent INL with or without LE using different techniques and clinical success was achieved in 86% [62]. Kim et al. carried out a systematic review of the literature for studies evaluating lymphangiography with or without LE in the setting of CA. Eighty-seven patients with clinical success data available for 47 patients. Clinical success was achieved in 32/47 patients (68.1%) [63]. Other smaller retrospective series revealed similar results [64,65,66]. In pediatric patients, the available data is more limited. In a recent review of our experience with 6 patients, clinical success was achieved in 4 patients (66%) [67].
IL and LE are safe procedures with limited major complications in the published series. Few minor complications (< 3%) were reported including NBCA/ethiodized oil pulmonary embolism but these were not associated with any clinical repercussions [55, 62, 63].
Lymphoceles
Lymphoceles are one of the most common complications after pelvic and retroperitoneal lymphadenectomy. Treatment is reserved for symptomatic lymphoceles: infection, pain, pressure symptoms (leg swelling, venous obstruction, ureteric obstruction) [68].
Percutaneous Drainage and Sclerotherapy
Percutaneous aspiration is feasible and allows for complete drainage. However, this method was abandoned as a solitary treatment due to its high recurrence rate and is currently reserved for diagnostic purposes only [69]. Percutaneous drain placement has therefore become the mainstay of minimally invasive treatment for lymphoceles as it allows for continuous drainage and can be removed once the output drops below 10 cc/day. Unfortunately, it is associated with long dwell time which can be up to 4 months [70,71,72]. Even with drain placement, it still may be associated with high recurrence rates, with many cases requiring additional treatment (e.g., percutaneous sclerotherapy) [70].
Percutaneous sclerotherapy induces local inflammation and fibrosis of the lymphatic channels with subsequent obliteration of the chyle leak [72]. Contrast injection through the drain can be performed first to estimate the needed volume of sclerosant and to exclude extravasation or communication with important structures [31]. There is no consensus on the type, volume, or dwell time of the sclerosing agent and sclerotherapy may need to be repeated several times [1••, 31]. Commonly used sclerosants include ethanol, povidone iodine, doxycycline, and bleomycin [31, 70, 73,74,75,76]. The reported success rate of sclerotherapy ranges from 77 to 100%, with an average catheter dwell time from 4 to 19 days [31, 70, 73,74,75,76,77,78,79]. Despite the possibility of success after single session of sclerotherapy, the average number of procedures reported in the literature is between 1 and 4 procedures. Uyulmaz et al. reported their experience using OK-432 with a success rate of 95% and a mean number of 2.5 sessions [79]. Sclerotherapy can be associated with minor complications (0–13%) such as infection, catheter occlusion/dislodgement, peri catheter leakage, and pain [31, 70, 73,74,75,76,77].
A novel approach has been described by Franke et al. using vacuum-assisted drainage of lymphocele with clinical success of 95%, minor complication rate of 4.6%, and median indwelling time of the drainage catheter 8–9 days [80].
Lymphangiography and Lymphatic Embolization
IL can identify the source of leak in the pelvis or retroperitoneum and bilateral access might not be required in cases with pelvic lymphoceles restricted to one side [80]. Once the leak is identified, percutaneous LE using NBCA/ethiodized oil mixture under fluoroscopic guidance can be performed. Although the leaking lymphatic duct can directly be targeted, it is easier and more reproducible to target the closest lymph node draining into the culprit channel [7, 81••]. If the leak is not identified (< 20%), no percutaneous embolization would be performed. Even in those situations, the inflammatory reaction induced by lipiodol can help seal the leak [56, 60, 61, 72].
The reported success rate of IL and LE is very high, approaching 100%. The available studies report a median number of procedures to be 1, and the median time to drain removal is 5 to 7 days, which is much shorter, compared to sclerotherapy [7, 55, 81••, 82, 83]. A systematic review performed by Ten Hove et al. reported a success rate of 92% with time to drain removal of 4 to 9 days [84••]. Kim et al. compared IL/LE with sclerotherapy and reported higher 3-month clinical success rate with IL/LE (83.3% vs. 43.8%, P = 0.026) [85]. Hur et al. described back door glue embolization LE by accessing the leaking vessel through the lymphocele [86••]. LE and INL are safe procedures, and most of the reported complications are transient pain or leg swelling.
Conclusion
Lymphatic metastases are an important mechanism in the spread of cancer. Both iatrogenic and non-iatrogenic chylous leakage can occur and when it does, it is typically associated with significant impairment of patient’s quality of life. In recent years, the combination of advanced lymphatic imaging and advanced interventional techniques has enabled treatment of these patients through low-risk minimally invasive approaches. Fortunately, our improved understanding of lymphatic anatomy and continued technological advancements will help to expand the horizon for future lymphatic interventions.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
••Santos, E. and A.M. Moussa, 2020 CA and lymphoceles: evaluation and interventions. Semin Intervent Radiol. 37(3):274–284. State-of-the-art review about chylous ascites and lymphoceles with emphasis in lymphatic embolization
Null M, Agarwal M. Anatomy, lymphatic system. Treasure Island (FL): StatPearls Publishing; 2021.
Ohkura Y, et al. Risk factors for postoperative chylothorax after radical subtotal esophagectomy. Ann Surg Oncol. 2018;25(9):2739–46.
Braun CM, Ryu JH. Chylothorax and pseudochylothorax. Clin Chest Med. 2021;42(4):667–75.
Jeon YJ, et al. Management of chyle leak after general thoracic surgery: impact of thoracic duct embolization. Thorac Cancer. 2021;12(9):1382–6.
Al-Busafi SA, et al. CA: evaluation and management. ISRN Hepatol. 2014;2014: 240473.
Chu HH, et al. Lymphangiography and lymphatic embolization for the management of pelvic lymphocele after radical prostatectomy in prostatic cancer. Cardiovasc Intervent Radiol. 2019;42(6):873–9.
Ng ZQ, et al. CA in colorectal surgery: a systematic review. World J Gastrointest Surg. 2021;13(6):585–96.
Kim HY, et al. An analysis of the risk factors and management of lymphocele after pelvic lymphadenectomy in patients with gynecologic malignancies. Cancer Res Treat. 2004;36(6):377–83.
Patel S, et al. Intranodal CT Lymphangiography with water-soluble iodinated contrast medium for imaging of the central lymphatic system. Radiology. 2022;302(1):228–33.
••Gurevich, A., et al. 2021, Non-traumatic chylothorax and chylopericardium: diagnosis and treatment using an algorithmic approach based on novel lymphatic imaging. Ann Am Thorac Soc. The application of MRI-guided intervention algorithm helped to increase the management of non-iatrogenic chylothorax in 93% of the patients with abnormal pulmonary lymphatic flow.
Nadolski GJ, Chauhan NR, Itkin M. Lymphangiography and lymphatic embolization for the treatment of refractory CA. Cardiovasc Intervent Radiol. 2018;41(3):415–23.
Guez D, et al. Transhepatic lymphatic embolization of intractable hepatic lymphorrhea. J Vasc Interv Radiol. 2014;25(1):149–50.
Chen E, Itkin M. Thoracic duct embolization for chylous leaks. Semin Intervent Radiol. 2011;28(1):63–74.
Shah RD, et al. Postesophagectomy chylothorax: incidence, risk factors, and outcomes. Ann Thorac Surg. 2012;93(3):897–904.
Brinkmann S, et al. Incidence and management of chylothorax after Ivor Lewis esophagectomy for cancer of the esophagus. J Thorac Cardiovasc Surg. 2016;151(5):1398–404.
Cerfolio RJ, et al. Postoperative chylothorax. J Thorac Cardiovasc Surg. 1996;112(5):1361–5 (discussion 1365-6).
Doerr CH, et al. Etiology of chylothorax in 203 patients. Mayo Clin Proc. 2005;80(7):867–70.
Teng CL, et al. Malignancy-associated chylothorax: a 20-year study of 18 patients from a single institution. Eur J Cancer Care (Engl). 2012;21(5):599–605.
Marthaller KJ, et al. Percutaneous embolization of thoracic duct injury post-esophagectomy should be considered initial treatment for chylothorax before proceeding with open re-exploration. Am J Surg. 2015;209(2):235–9.
Cope C. Diagnosis and treatment of post-operative chyle leak via percutaneous transabdominal catheterization of the cisterna chyli: a preliminary study. J Vasc Interv Radiol. 1998;9(5):727–34.
Cope C. Percutaneous thoracic duct cannulation: feasibility study in swine. J Vasc Interv Radiol. 1995;6(4):559–64.
Cope C, Kaiser LR. Management of unremitting chylothorax by percutaneous embolization and blockage of retroperitoneal lymphatic vessels in 42 patients. J Vasc Interv Radiol. 2002;13(11):1139–48.
Itkin M, et al. Nonoperative thoracic duct embolization for traumatic thoracic duct leak: experience in 109 patients. J Thorac Cardiovasc Surg. 2010;139(3):584–9 (discussion 589-90).
Schild HH, et al. Treatment options in patients with chylothorax. Deutsches Arzteblatt International. 2013;110(48):819–26.
Bender B, Murthy V, Chamberlain RS. The changing management of chylothorax in the modern era. Eur J Cardiothorac Surg. 2016;49(1):18–24.
Nadolski GJ, Itkin M. Feasibility of ultrasound-guided intranodal lymphangiogram for thoracic duct embolization. J Vasc Interv Radiol. 2012;23(5):613–6.
Nadolski GJ, Itkin M. Thoracic duct embolization for nontraumatic chylothorax: experience in 34 patients. Chest. 2013;143(1):158–63.
Kariya S, et al. Intranodal lymphangiogram: technical aspects and findings. Cardiovasc Intervent Radiol. 2014;37(6):1606–10.
••Kariya, S., et al. 2018, Transvenous retrograde thoracic ductography: initial experience with 13 consecutive cases. Cardiovasc Intervent Radiol 41(3):406–414. Good review about transvenous access to the thoracic duct. Largest experience published with this challenging approach.
Mahrer A, et al. Sclerotherapy in the management of post-operative lymphocele. J Vasc Interv Radiol. 2010;21(7):1050–3.
Bundy JJ, et al. Percutaneous fluoroscopically-guided transcervical retrograde access facilitates successful thoracic duct embolization after failed antegrade transabdominal access. Lymphology. 2019;52(2):52–60.
Williams E, et al. Thoracic duct embolization via chest tube for a patient with post-operative traumatic chylothorax. Can J Surg. 2021;64(6):E650-e653.
Bundy JJ, et al. Vascular and lymphatic complications after thoracic duct cannulation. J Vasc Surg Venous Lymphat Disord. 2018;6(6):730–6.
••Srinivasa, R.N., et al. 2018, EndolymphatictThoracic duct stent-graft reconstruction for chylothorax: approach, technical success, safety, and short-term outcomes. Ann Vasc Surg. 48:97–103. New approach for patients with chylothorax. Interesting approach to explore: thoracic duct reconstruction instead embolization
Pamarthi V, et al. Thoracic duct embolization and disruption for treatment of chylothoraxs: experience with 105 patients. J Vasc Interv Radiol. 2014;25(9):1398–404.
Reisenauer JS, et al. Treatment of postsurgical chylothorax. Ann Thorac Surg. 2018;105(1):254–62.
Kortes N, et al. Therapeutic lymphangiography and CT-guided sclerotherapy for the treatment of refractory chyle leak. J Vasc Interv Radiol. 2014;25(1):127–32.
Binkert CA, et al. Percutaneous treatment of high-output chylothorax with embolization or needle disruption technique. J Vasc Interv Radiol. 2005;16(9):1257–62.
••Jardinet, T., et al. 2021, Intranodal lymphangiography with high-dose ethiodized oil shows efficient results in patients with refractory, high-output postsurgical chylothorax: a retrospective study. AJR Am J Roentgenol. 217(2):433–438. Therapeutic lymphangiography with high dose of ethiodized oil and no thoracic duct embolization. High success rate in chylothorax.
Yannes M, et al. Comparative analysis of intranodal lymphangiography with percutaneous intervention for postsurgical chylothoraxs. J Vasc Interv Radiol. 2017;28(5):704–11.
Bruna J. Collateral lymphatic circulation. Eur J Plast Surg. 2000;23(6):321–5.
Laslett D, Trerotola SO, Itkin M. Delayed complications following technically successful thoracic duct embolization. J Vasc Interv Radiol. 2012;23(1):76–9.
Ahn, H.Y. and H. I 2021, Non-conservative management of chylothorax. J Chest Surg. 54(4):325-329
Jimenez CA, et al. Use of an indwelling pleural catheter for the management of recurrent chylothorax in patients with cancer. Chest. 2007;132(5):1584–90.
Scaletta G, et al. Management of post-operative CA after surgery for ovarian cancer: a single-institution experience. Updates Surg. 2019;71(4):729–34.
Majdalany BS, El-Haddad G. Contemporary lymphatic interventions for post-operative chyle leaks. Transl Androl Urol. 2020;9(Suppl 1):S104–13.
Sugawara S, et al. Radiological insertion of Denver peritoneovenous shunts for malignant refractory ascites: a retrospective multicenter study (JIVROSG-0809). Cardiovasc Intervent Radiol. 2011;34(5):980–8.
Yarmohammadi H, et al. Therapeutic application of percutaneous peritoneovenous (Denver) shunt in treating CA in cancer patients. J Vasc Interv Radiol. 2016;27(5):665–73.
••Yarmohammadi, H., et al., 2020 Treatment of CA with peritoneovenous shunt (Denver shunt) following retroperitoneal lymph node dissection in patients with urological malignancies: update of efficacy and predictors of complications. J Urol. 204(4): 818–823. State-of-the-art article about the success and management of post-surgical chylous ascites with Denver shunt.
Defert C, et al. Peritoneovenous shunt for intractable ascites in children: a series of 4 cases. J Pediatr Gastroenterol Nutr. 2021;73(1):e7–10.
Kalia, S., et al., Retrograde transvenous selective lymphatic duct embolization in post donor nephrectomy CA. CEN Case Rep, 2021.
Guevara CJ, et al. US-guided, direct puncture retrograde thoracic duct access, lymphangiography, and embolization: feasibility and efficacy. J Vasc Interv Radiol. 2016;27(12):1890–6.
Chick JF, et al. Balloon-occluded retrograde abdominal lymphangiography and embolization for opacification and treatment of abdominal chyle leak. J Vasc Interv Radiol. 2017;28(4):616–8.
Hur S, et al. Early experience in the management of post-operative chyle leak using lipiodol lymphangiography and adjunctive glue embolization. J Vasc Interv Radiol. 2016;27(8):1177-1186.e1.
Hur S, Jun H, Jeong YS. Novel interventional radiological management for chyle leaks after gynecologic surgery: lymphangiography and embolization. Gland Surg. 2021;10(3):1260–7.
Mittleider D, et al. Retrograde cannulation of the thoracic duct and embolization of the cisterna chyli in the treatment of CA. J Vasc Interv Radiol. 2008;19(2 Pt 1):285–90.
Soga S, Suyama Y, Shinmoto H. Balloon-occluded retrograde glue embolization for intractable lymphorrhea from bilateral iliac lymphatics following surgery for rectal cancer. Radiol Case Rep. 2020;15(4):371–4.
Lee H, et al. The feasibility of mesenteric intranodal lymphangiography: its clinical application for refractory postoperative CA. J Vasc Interv Radiol. 2018;29(9):1290–2.
Alejandre-Lafont E, et al. Effectiveness of therapeutic lymphography on chyle leak. Acta Radiol. 2011;52(3):305–11.
Gruber-Rouh T, et al. Direct lymphangiography as treatment option of chyle leak: indications, outcomes and role in patient’s management. Eur J Radiol. 2014;83(12):2167–71.
Majdalany BS, et al. Lymphatic interventions for isolated, iatrogenic CA: a multi-institution experience. Eur J Radiol. 2018;109:41–7.
Kim PH, Tsauo J, Shin JH. Lymphangiography with or without embolization for the treatment of postoperative CA. Ann Vasc Surg. 2020;68:351–60.
Tai E, Min A, Rajan DK. A single-center experience with percutaneous interventional management of refractory CA. Can Assoc Radiol J. 2021;72(4):871–5.
Kwon LM, et al. Glue embolization of lymphopseudoaneurysm for CA after retroperitoneal surgery. Korean J Radiol. 2021;22(3):376–83.
Sun X, et al. Application of ultrasound-guided intranodal lymphangiography and embolisation in cancer patients with post-operative chyle leak. World J Surg Oncol. 2021;19(1):32.
Moussa, A.M., et al., Intranodal lymphangiography and lymphatic embolization for management of iatrogenic CA in children. Lymphat Res Biol, 2021.
Karcaaltincaba M, Akhan O. Radiologic imaging and percutaneous treatment of pelvic lymphocele. Eur J Radiol. 2005;55(3):340–54.
Andrews JR, et al. Treatment outcomes in patients with symptomatic lymphoceles following radical prostatectomy depend upon size and presence of infection. Urology. 2020;143:181–5.
Alago W, et al. Management of post-operative lymphoceles after lymphadenectomy: percutaneous catheter drainage with and without povidone-iodine sclerotherapy. Cardiovasc Intervent Radiol. 2013;36(2):466–71.
Kim JK, et al. Post-operative pelvic lymphocele: treatment with simple percutaneous catheter drainage. Radiology. 1999;212(2):390–4.
Khorshidi F, et al. Minimally invasive treatment of abdominal lymphocele: a review of contemporary options and how to approach them. Lymphology. 2021;54(2):56–67.
Baboudjian M, et al. Povidone-iodine sclerotherapy of primary symptomatic lymphocele after kidney transplantation. Int Urol Nephrol. 2021;53(4):685–90.
Kerlan RK, et al. Bleomycin sclerosis of pelvic lymphoceles. J Vasc Interv Radiol. 1997;8(5):885–7.
Kim Y, et al. Evaluation of sclerotherapy for the treatment of infected post-operative lymphocele. Taiwan J Obstet Gynecol. 2017;56(4):477–81.
Zuckerman DA, Yeager TD. Percutaneous ethanol sclerotherapy of post-operative lymphoceles. AJR Am J Roentgenol. 1997;169(2):433–7.
Klode J, et al. Polidocanol foam sclerotherapy is a new and effective treatment for post-operative lymphorrhea and lymphocele. J Eur Acad Dermatol Venereol. 2010;24(8):904–9.
Sawhney R, et al. Treatment of post-operative lymphoceles with percutaneous drainage and alcohol sclerotherapy. J Vasc Interv Radiol. 1996;7(2):241–5.
Uyulmaz S, et al. Sclerotherapy with OK-432 for the treatment of symptomatic lymphocele after lymph node dissection: a retrospective comparative cohort study. Ann Plast Surg. 2020;85(4):407–12.
Franke, M., et al., Vacuum-assisted suction drainage as a successful treatment option for postoperative symptomatic lymphoceles. Rofo, 2021
••Moussa, A.M., et al. 2021, Percutaneous lymphatic embolization as primary management of pelvic and retroperitoneal iatrogenic lymphoceles. J Vasc Interv Radiol. 32(11):1529–1535. This paper shows one of the largest series published about lymphatic embolization in patients with post-operative lymphoceles. Good review of the technique and results
Baek Y, et al. Lymphatic embolization for the treatment of pelvic lymphoceles: preliminary experience in five patients. J Vasc Interv Radiol. 2016;27(8):1170–6.
Smolock AR, Nadolski G, Itkin M. Intranodal glue embolization for the management of postsurgical groin lymphocele and lymphorrhea. J Vasc Interv Radiol. 2018;29(10):1462–5.
••Ten Hove, A.S., M.Y. Tjiong, and I.A.J. Zijlstra, 2021 Treatment of symptomatic post-operative pelvic lymphoceles: a systematic review. Eur J Radiol. 134:109459. Up-to-date review of the different percutaneosu treatment options in patients with lymphoceles
Kim SW, et al. The efficacy of lymph node embolization using N-butyl cyanoacrylate compared to ethanol sclerotherapy in the management of symptomatic lymphorrhea after pelvic surgery. J Vasc Interv Radiol. 2019;30(2):195-202.e1.
•• Hur J, et al. Reversed approach through lymphocele/lymphatic fluid collection for glue embolization of injured lymphatic vessels. J Vasc Interv Radiol. 2021;32(2):299–304. ( Retrograde embolization of the lymphatic vessels feeding the leak can be a good alternative in patients with lymphatic leakage and no leak intranodal lymphangiography)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Interventional Oncology.
Rights and permissions
About this article

Cite this article
Youssef, E.W., Aly, A., Brahmbhatt, A. et al. Lymphatic Interventions in the Cancer Patient. Curr Oncol Rep 24, 1351–1361 (2022). https://doi.org/10.1007/s11912-022-01293-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11912-022-01293-1