
Abstract
Degeneration of neuron and axons following injury to cells with which they synapse is termed trans-synaptic degeneration. This phenomenon may be seen in postsynaptic neurons (anterograde) or in presynaptic neurons (retrograde). Retrograde trans-synaptic degeneration (RTSD) of the retinal ganglion cells and retinal nerve fiber layer following injury to the occipital lobe has been well documented histologically in animal studies, but its occurrence in the human retina was, for many years, felt to be limited to cases of neonatal injury during a critical period of neuronal development. Over the last decade, imaging techniques such as MRI and optical coherence tomography have allowed us to visualize and quantify RTSD and analyze its time course and relationship to degree of vision loss and age of cortical injury. A deeper understanding of RTSD in the human visual system may allow us to interfere with its occurrence, potentially allowing for greater recovery following visual cortex injury.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Secondary degeneration of neuronal elements following remote injury to the neuron is a well-established phenomenon. Both axonal loss following cell body injury (anterograde or Wallerian degeneration) and cell body apoptosis following axonal injury (retrograde degeneration) have been demonstrated in the primate motor, sensory, and visual systems. Furthermore, the loss of one population of neurons can at times lead to secondary degeneration of neurons to whom they supply significant efferent or afferent connections. Such a trans-synaptic degeneration has been long recognized in the motor system and cerebellar pathways, but its existence in the human visual system was doubted for years, except in the case of injury to the visual cortex during early development, either in the fetal or neonatal period. Over the last two decades, increasing evidence for retrograde trans-synaptic degeneration (RTSD) in even the adult human visual system has been presented, with the aid of new technologies such as optical coherence tomography (OCT). In this paper, I will review the available evidence for the existence of RTSD in animals and in the adult human visual system, discuss possible mechanisms for its occurrence, and address any clinical relevance of RTSD, especially as it may relate to future attempts to utilize intense rehabilitation as a means of visual restoration therapy.
Histology of Retrograde Degeneration
Retrograde degeneration was recognized as far back as 1892 when Nissl demonstrated dissolution of nuclear chromatin (chromalysis) in anterior horn cells as soon as 24 h following peripheral nerve transection [1]. The same chromalytic process was described by James in retinal ganglion cells (RGCs) following transection of the optic nerve within the orbit of the rabbit, followed by near-complete dissolution of the ganglion cells [2]. However, multiple studies showed little to no dissolution of the associated optic nerve fibers, except in the portion adjacent to the injury [3, 4]. In 1938, Leinfelder performed electrolysis at various points along the pregeniculate visual pathway in cats [5]. Of note is that they found degeneration of the RGCs and the optic nerve fibers anterior to the lesion following prechiasmatic optic nerve injury, but following injury to the chiasm or optic tract, RGC degeneration was observed, but was accompanied by little to no loss of optic nerve fibers.
Early Evidence for Anterograde Trans-synaptic Degeneration in the Visual System
It has long been observed that RTSD occurs outside the visual system in humans, with pathological degeneration demonstrated in Brodmann area 4 following limb amputations [6] and in the corticopontine and central tegmental tract 14 years after a hemicerebellectomy [7]. Within the visual system, evidence for anterograde trans-synaptic degeneration (ATSD) has also been well established. As early as 1911, Ramon y Cajal described anterograde trans-synaptic degeneration in his landmark review of the visual cortex when he declared that “Many investigators and we ourselves have observed that in those peripherally blind or one eyed by a peripheral lesion, the plexus of the Band of Gennari is infinitely less rich and at the same time these wide fibers almost completely disappear” [8]. In 1913, Minkowski observed chromalytic changes in the lateral geniculate nucleus (LGN) in animals following enucleation [9], and Clarke later showed loss of those lamina in the LGN corresponding to the enucleated eye of a patient with glaucoma [10]. Gartner also demonstrated atrophy of the LGN following chiasmal compression by a pituitary tumor [11]. Corresponding occipital lobe degeneration was even described in one case [12]. But while these studies offered evidence for anterograde trans-synaptic degeneration, the existence of retrograde trans-synaptic degeneration in the visual system remained controversial for most of the twentieth century.
Animal Studies Demonstrating RTSD
Over the years, some studies have failed to demonstrate RTSD in the mammalian visual system. In the rat, for example, no evidence of RTSD was seen of the RGCs up to 15 months following removal of the striate cortex, whether performed during infancy or adulthood [13]. The bulk of animal studies, however, which will be reviewed, has shown RTSD following visual cortex lesions, begging the crucial questions: what determines the extent of RTSD, which RGCs does it affect, and in which species does it occur dependably?
Retinal Ganglion Cell Subtypes
Before proceeding to a discussion of RGC loss following cortical lesions, let us briefly review the cell types of the ganglion cell layer (GCL) and their connections. In adult humans, there are approximately 1.7 million RGCs, 70% of which subserve the central 30° of vision. RGCs, as a rule, project to the LGN that is ipsilateral to their position relative to the fovea in each eye. Physiologically, RGCs can be divided into three types with varied response profiles: the most common, the medium-sized X cells, demonstrate a sustained response to stimulation of their receptive field and also tend to respond with a magnitude that reflects the luminosity and contrast within the center of their receptive field, while the larger Y cells demonstrate a more transient response to light. The small W cells have large receptive fields, slow axonal conduction, and respond to movement. RGCs can further be subdivided by their presumed function into four groups. The most numerous are the small P cells (also known as midget cells), which project to the parvocellular layers (3–6) of the LGN and are sensitive to color and fine details of the visual image. The larger M cells (also known as parasol cells) synapse in the magnocellular layers (1 and 2) of the LGN and are sensitive to motion and contrast. Small bistratified cells project to the intercalated layers of the LGN connecting with ĸ cells (for koniocellular pathway, meaning “as small as dust”), which in turn project to blobs in V1 [14]. The ĸ cells of the LGN also appear to receive input from the superior colliculus [15] and make connections with extrastriate regions in the dorsal visual pathways in the parietal lobe [16]. As such, these cells are felt to carry information about eye movements to help inform visual processing. Finally, the most recently discovered cells are the melanopsin-containing RGCs, which project to various subcortical nuclei including the suprachiasmatic nucleus of the hypothalamus which synchronizes circadian rhythms and to the pretectal olivary nuclei for regulating the pupillary light response. Most P cells demonstrate X cell physiology, while M cells demonstrate Y cell physiology and ĸ- and melanopsin-containing cells incorporate X, Y, and W cell types. See Table 1 for a review of the RGC subtypes. A review of the RGC anatomy and physiology can be found in Walsh and Hoyt’s Clinical Neuro-ophthalmology [17].
Pathological Changes in the Cat Retina Associated with RTSD
Several studies aimed to describe the specific cell types which degenerated in RTSD of the feline retina following cortical damage. Pearson and colleagues performed bilateral visual cortex ablations in three infant cats at 3 days of age and compared their retinal histology after 14 months with those of non-lesioned cats [18]. They found a mean reduction in RGC density of 16% in the central retina and 32% in the peripheral retina. Of note is that a loss of almost 70% of the medium-sized ganglion cells (felt to likely be X cells) was observed. This demonstrated an interspecies difference with the monkey where 100% of the medium cells were gone after lobectomy, a difference that might have reflected the fact that in cats, X, Y, and Z cells all projected to the LGN, but in monkeys, only the X and Y cells do. Tong and colleagues used soma recordings rather than histology to demonstrate that Y and W cells in the nasal macula were unaffected at approximately a year after lobectomy of the contralateral visual cortex. However, 78% of the X cells were lost, provided the lobectomy was performed on the day of birth, while only 22% of the X cells were lost following lesions made during adulthood [19]. The specific effect on X cells was attributed to the finding that while W and Y cells projected to the mesencephalon as well as the LGN, approximately 90% of the X cells project only to the LGN [20]. Thus, with loss of their one target cell, these neurons received no feedback to keep them alive, while W and Y cells had other sources of postsynaptic feedback. Further work by the same group, in which nine kittens underwent removal of Brodmann areas 17, 18, and 19, varying the time of resection to either day 1, at 2 weeks, or at 4 weeks, showed that the loss of corresponding RGCs (again mostly X cells) was maximal after the day 1 lesion, but in the 2- and 4-week animals, it was not much more than that seen following resections performed in adulthood. Thus, in cats at least, there appears to be a critical time during which significant RTSD may occur, after which it hardly occurs, as opposed to a spectrum of RTSD that slowly diminishes with age. The work of Théoret and colleagues added to the recognition that the extent of RTSD in cats was linked to age of the lesion: in an animal that underwent removal of a whole cerebral hemisphere at postnatal day 16, there was RTSD 53 days later in the corresponding hemiretinas, but this was not seen in a cat whose hemispherectomy was performed at postnatal day 25 [21]. As in previous studies, the majority of degeneration was of medium-sized X cells. Of note is that the authors found more RGC loss in the nasal retina contralateral to the hemispherectomy (41%) than in the temporal retina ipsilateral to the lesion (33%), suggesting that RTSD does not necessarily occur to an equal extent, or at an equal speed, in both eyes. This finding had also been shown by Rowe, who reported twice as much RGC loss in the contralateral nasal retina as in the ipsilateral temporal retina following unilateral visual cortex lobectomy in cats [22]. Moreover, this author found that there was loss of large-medium cells in the ipsilateral temporal retina, suggesting a degeneration of the larger W cells as well as X cells.
Why Would There Be a Critical Period During Which Significant RTSD Occurs?
In humans, there is a significant attrition of RGCs in early development, achieved through apoptosis, with a loss of anywhere between 50 and 90% of the original population [23], similar to what occurs in other parts of the developing brain. This process occurs in cats as well, with the bulk of attrition occurring during the first 2 weeks of life [24]. Selective ablations of superior colliculus neurons in the rat, to which 90% of RGCs project, demonstrated a 41% reduction in the number of neurons that survived the period of “naturally occurring cell death,” presumably because the survival of any given RGC was predicated on finding a target neuron [25]. Cortical ablation in early development leads to loss of LGN cells, which could in turn result in fewer potential targets for RGCs, resulting in greater competition for target acquisition and, ultimately, a smaller number of survivors. After this period of natural attrition, the continued existence of an RGC would no longer be as dependent on the presence of its target cell, and RTSD would occur to a lesser extent.
Pathological Changes in the Monkey Retina Associated with RTSD
Histological evidence for RTSD was offered by Klüver in 1937, who noted a loss of hemiretinal GCL staining on the left side of both retinas following a left occipital hemi-lobectomy in a rhesus monkey [26]. Quantitative histological analysis of RTSD in the monkey retina was performed as early as 1963, when Van Buren and colleagues demonstrated two examples of the phenomenon in the macaque [27]. In one monkey, a right occipital lobectomy was performed, and 48 months later, degeneration was observed in the ipsilateral LGN and optic tract, the latter showing a cross-sectional area 44% of the contralateral side. While no degeneration was seen in the optic nerves, RTSD of the RGCs was observed within the right side of the fovea so that the layer was at most two cells thick, as opposed to six cells on the left. RTSD in the monkey was later confirmed by Cowey [28] and by Weller and colleagues, who demonstrated a preponderance of degeneration of X cells, most severely in the central retina, in two macaque monkeys who had long-standing bilateral lesions of the primary visual cortex [29]. Weller and colleagues found that macaque monkeys lesioned as infants lost between 38.5 and 78%, and notably never more than 80% of RGCs, even when killed up to 8 years after the lesion [30], concluding that those monkeys with 80% loss of RGCs were likely missing all of their X cells. The speed of RTSD was correlated again with the time of lesion: those lesioned just after birth lost approximately 50% of their RGCs within the first few weeks and almost the entire loss occurred by 1 year. Conversely, those lesioned as adolescents or adults took years to develop severe GCL loss. Cowey and colleagues confirmed a selective loss of Pβ cells, which are roughly equivalent to the X cells, and suggest that their susceptibility in macaques may be linked in part to their small size and not just their lack of extra-geniculate targets [31]. Such a selective damage to the parvocellular pathway, which subserves color perception and fine spatial contrast, is one possible explanation for “blindsight” following cortical injury, where a residual sensitivity to motion is demonstrated in regions of the visual field where detailed form and color sensitivity is absent [32].
Herbin and colleagues pinpointed a critical time, between 8 and 9 months, after which very little RTSD occurred in their series of six green monkeys [33]. Prior to that critical period, the degree of RGC loss at 15° from the fovea appears to show a linear relationship with age at lesion, while that at 7° appears parabolic. Cowey showed that the degree of RTSD, which appeared complete by 4–5 years, was also associated with lesion size, but that enlarging the lesion beyond the striate cortex did not have a significant effect [34]. Of note is that they pointed out that in two of their monkeys, impingement of the lesion on the vascular supply to the caudal LGN and optic tract likely produced a non-trans-synaptic retrograde degeneration eclipsing any RTSD. As they point out, Kupersmith and colleagues attributed their finding of optic atrophy in patients with cortical arteriovenous malformations to this same phenomenon [35]. However, involvement of the LGN and optic tract as a primary mediator of GCL atrophy in macaques was put to rest by the demonstration of extensive RGC loss in the central retina in monkeys in which selective destruction of the macular-projecting striate cortex had been performed, clearly avoiding any effect on the primary retinal targets [36].
Clinical and Histological Evidence of RTSD in Humans
Multiple early case series on patients with occipital injury did not describe fiber atrophy in the optic nerves [37, 38] (although in the latter study, there is no evidence that funduscopy was performed). On the other hand, in 1913, Wilbrand and Saenger referred to cases by Carl Moeli where atrophy of the optic nerve and tract (observed histologically) occurred years after occipital lobe injury to the “developing brain” of the fetal period [39]. Several case reports purported to demonstrate RTSD many years after occipital lobe injury in adult humans, including two in the French literature [40, 41] (18 and 30 years after injury, respectively), and one report by Haddock and Berlin in which a soldier sustained bilateral occipital lobe injury during World War II and developed mild bilateral optic atrophy 3.5 years later, progressing to severe optic atrophy, 5.5 years after the injury [42]. While alternative explanations could be proposed for the development of optic atrophy in these patients, such as papilledema, which was present following the injury in Haddock’s case, or traumatic optic nerve injuries, none of these would explain the considerable latency between the injury and atrophy.
Despite these early reports of RTSD in adults, the bulk of clinical evidence of RTSD in the twentieth century supported its occurrence primarily following injury to the fetus or neonate, suggesting that a critical period for RTSD was present in humans, similar to cats. Indeed, the understanding of RTSD as a phenomenon that followed only congenital lesions in humans is demonstrated by a case report in 1988 in which the authors conclude that, since RTSD of the retinal nerve fiber layer (RNFL) was present in a man with an occipital lobe ganglioglioma, “these lesions may arise during neural development” [43]. In a seminal paper of three patients with congenital cerebral hemiatrophy, Hoyt and colleagues described band atrophy in the contralateral optic disc, similar to what is observed with a contralateral optic tract lesion, optic disc hypoplasia, and using Vogt’s red-free funduscopy, observed loss of RNFL in the temporal hemiretina in the eye ipsilateral to the cortical atrophy and along non-arcuate bundles (i.e., maculopapular bundle) in the eye contralateral to the atrophy [44]. While this phenomenon, termed “homonymous hemioptic hypoplasia,” by the authors, might have resulted in part due to RTSD, the authors acknowledge that the vascular insults felt to be responsible for congenital hemiatrophy might cause direct damage to the optic tract and LGN.
In another case of early cerebral injury associated with optic disc changes, Jacobson and colleagues later described a unique form of optic nerve hypoplasia, with large cups but normal disc diameter, in children with periventricular leukomalacia (PVL), a condition of perinatal hypoxic-ischemic events affecting the corticospinal tracts and optic radiations in preterm infants [45]. These patients typically have a form of cerebral palsy and visual loss reflective of cortical disease, including homonymous field defects, perceptual deficits, and the crowding phenomenon, where letters of a given optotype can be read when displayed alone, but not when placed in a linear sequence. The authors theorize that when intrauterine ischemia occurs early during gestation, plasticity of the scleral ring allows shrinkage of the disc in response to loss of axons from RTSD, thus producing the small hypoplastic disc. Conversely, when the damage occurs late in the third trimester, loss of this plasticity forces the reduced number of axons to rearrange within the same aperture, producing a normal-sized disc with cupping.
Again, it is difficult to deduce a true trans-synaptic degeneration from these observations since ischemia to the optic tracts or their terminal axons within the LGN is not excluded. Indeed, the authors cite the presence of homonymous vision loss in their cases as evidence against direct optic nerve ischemia in their cases, but of course, such patterns of field loss could be associated with tract or LGN pathology.
Histopathologic evidence of RTSD in the human visual system may be seen in a case report by Beatty and colleagues who used paraphenylenediamine staining to demonstrate degenerated axons within the ipsilateral optic radiations, lateral geniculate nucleus and optic tract, and within the optic chiasm in a man who, 40 years previously, had undergone resection of his right occipital lobe at age 46 [46]. Since the etiology precipitating resection was an underlying angiomatous malformation which was presumably congenital, one must remain cautious in concluding from this case that adult-onset occipital injury leads to RTSD. Although a left homonymous hemianopia only developed after the resection, this does not preclude the possibility that the congenital lesion was sufficient to cause the observed histological changes. Furthermore, although optic atrophy was only noted 35 years after the resection, suggesting that funduscopic evidence of RTSD could be found after adult-onset cortical damage, it is also noted that the visual acuities were decreased at the time of recognition of such atrophy, so that an alternative cause for the optic disc appearance other than RTSD (which should not affect acuity) cannot be ruled out. Nevertheless, the case offered, for the first time, compelling evidence that RTSD occurred in the human retina, following injury to the visual cortex, even in adults.
MRI Evidence of RTSD in Humans
With the advent of improved brain imaging techniques, MRI was put forth as indirect evidence for RTSD and ATSD in the human visual system in 1997. The authors observed bilateral LGN T2 hypointensity in a group of patients with an array of congenital lesions causing blindness, including neuroaxonal dystrophy, PVL, and bilateral posterior cerebral artery infarction due to compression by the parahippocampal gyri [47]. Using MRI, Guedes and colleagues showed shrinkage and T2 hyperintensity of the optic tract 4 years after a resection of an occipital lobe ependymoma, along with corresponding thinning of the RNFL and even expected funduscopic changes (bowtie atrophy in the contralateral eye and temporal pallor ipsilaterally) [48]. Bridge and colleagues used structural MRI to quantitatively demonstrate optic tract degeneration in patients with homonymous hemianopia from occipital (two out of three patients) or LGN (one out of two patients) lesions by measuring a laterality index (LI) for the cross-sectional area and volume of the tracts: (contralesional − ipsilesional)/(contralesional + ipsilesional) and comparing it to controls [49]. It can be argued that the optic tract atrophy in the cases of LGN damage does not necessarily reflect trans-synaptic degeneration since the distal fibers of the optic tract reach the LGN and would likely be injured along with it. In a more qualitative fashion, this same study demonstrated LGN atrophy ipsilateral to the cortical injury in the two patients who were farthest out from the injury. In a 2012 study, the same group found similar results in 17 cases of acquired and nine cases of congenital homonymous field defects [50•]. Interestingly, they found that lesion size corresponded with the LI in the acquired patients, but not the congenital ones. However, in both groups, the degree of visual field loss predicted the degree of RTSD. Finally, T1 structural MRI was superior to diffusion-weighted imaging in visualizing the optic tract atrophy. More recently, Patel and colleagues demonstrated asymmetry of optic tract fractional anisotropy using diffusion tensor imaging (DTI) as early as 3 months, claiming the earliest noninvasive evidence of RTSD in any species [51•].
ERG Evidence of RTSD
Stoerig and Zrenner were the first to demonstrate a reduction in signal on the pattern electroretinograms (pERG) in a patient with a cortical lesion and a homonymous hemianopsia [52].
In 1999, Porello and Falsini analyzed eight patients with post-geniculate infarcts or surgical resection and found that responses were reduced in the blind hemiretina of both eyes as compared to the seeing hemiretina [53]. Of note is that the phenomenon was observed when using low-temporal and high-spatial frequency stimuli (the 6 Hz–5 c deg−1 and not the 15 Hz–0.58 c deg−1 stimulus), reflective of parvocellular pathway activity and consistent with previously described animal studies showing predominant loss of X cells in RTSD. Furthermore, the amplitude of signal loss correlated inversely with the age at onset of the lesion, in agreement with similar observations in primate studies. As the authors point out, the pERG abnormalities do not necessarily reflect structural loss of RGCs, and in fact, some patients demonstrated significant loss of corresponding signal within weeks of injury, obviously too early to reflect RTSD. They conclude that RGC dysfunction may, in some cases, precede actual death of neurons. They further demonstrated that pERG abnormalities did not necessarily only occur in patients with optic atrophy observed on funduscopy. In reviewing the drawings of the lesions provided in the paper, one of the lesions appears close to the LGN, offering another possible explanation for the relatively fast changes observed.
Perhaps the most interesting finding of this study was that while the amplitude of signal loss in the temporal hemiretina of the eye ipsilateral to the lesion correlated with time since injury and inversely with age at time of injury, this was not true of the nasal hemiretina in the contralateral eye. They attribute this difference to the higher RGC density in the nasal hemiretina, conferring upon them a greater resistance to RTSD early in life, making the phenomenon less time-dependent.
Azzopardi and colleagues utilized pERG to study blindsight, the ability to unconsciously detect objects in the blind field in the absence of conscious visual perception in certain patients following striate cortex injury [54]. These authors studied three patients with complete cerebral hemispherectomies (that include not just striate cortex but extrastriate cortex as well, ostensibly sparing the LGN and optic tract) who did not demonstrate blindsight. Interestingly, they found that evidence of RGC degeneration/dysfunction was no worse in these patients compared with those with only striate cortical lesions from other studies. Thus, absence of blindsight is not likely related to RTSD, but rather to loss of extrastriate association areas. Their results correlated well with the pathological findings of Herbin et al. in monkeys [28].
Visualizing RTSD Using Optical Coherence Tomography
Retinal Nerve Fiber Layer Analysis
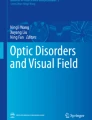
The advent of OCT in clinical practice, which visualizes individual retinal layers though analysis of the interference pattern of low coherent light rays aimed at the retina, has provided a new means to study RTSD in the human visual system. Figure 1 provides a review of the anatomy of the RNFL. Since axons of the RNFL destined for the ipsilateral LGN (non-decussating fibers) enter the optic nerve through the superior and inferior sectors of the optic nerve head (ONH) and those fibers that will synapse with the contralateral LGN (decussating fibers) enter through the nasal and temporal sectors of the ONH, atrophy of these regions on OCT would be expected in the ipsilateral and contralateral eye, respectively, when RTSD resulted from a unilateral occipital lesion. Indeed, as early as 2005, in two patients with incidentally discovered occipital infarcts, Mehta and Plant demonstrated RNFL thinning within the regions nasal and temporal to the disc (band atrophy) in the eye contralateral to an infarct and thinning of the superior and inferior arcuate bundles in the ipsilateral eye [55]. Since the patients were asymptomatic and unaware of their homonymous hemianopsia, and since there was band atrophy observed on funduscopy, it was concluded that these were likely congenital infarcts. The authors argued that the presence of RTSD on OCT in patients with incidentally found occipital infarct could indicate its congenital onset and therefore avoid the workup that might be necessitated by an adult-onset stroke. But was this the case? Would OCT only show thinning after congenital lesions? Jindahra and colleagues used OCT to analyze the RNFL of seven patients with congenital lesions causing homonymous hemianopsia (HH), 19 patients with acquired HH, and 22 controls [56•]. In both the congenital and acquired groups, they found thinning of the superior and inferior fibers in the eye ipsilateral to the lesion (the eye with the nasal hemianopsia or “non-crossing fiber defect eye”) and thinning predominantly of the nasal side and temporal side of the disc in the eye contralateral to the lesion (the eye with the temporal hemianopsia or “crossing fiber defect eye”), consistent with RTSD. Surprisingly, the authors found that while the degree of RTSD was slightly greater in the congenital group than in the acquired group, this difference was not statistically different. This finding challenged the long-standing dogma that RTSD did not occur following adult-onset lesions, even after extended periods of time. This concept was based on the lack of funduscopic evidence of optic atrophy or obvious changes in the RNFL in such patients, such as the 86-year-old woman who presented to Newman and Miller 57 years after a cortical infarction left her with a HH [57], prompting the authors to cite this as “strong evidence against the occurrence of acquired transsynaptic degeneration in the visual system of adults.” But Jindahra’s work indicated that the RTSD might be clinically occult, observable only with the help of OCT. The same group subsequently reported RTSD of the RNFL in seven patients with congenital and 14 with acquired quadrantanopia, showing the most pronounced thinning in the superior hemiretina in patients with inferior quadrantanopia and vice versa [58]. Looking at these results together with patients with complete hemianopsias, they were able to demonstrate a linear relationship between the degree of RTSD and the average of the two eyes’ mean deviation score (which is the mean of the degree that a patient’s light sensitivity score deviates from an age-matched control at each point on a Humphrey visual field). A cross-sectional study of 38 patients with HH and a longitudinal study of 11 patients with homonymous defects were then performed to investigate the time course of RTSD [59••]. The cross-sectional study demonstrated a logarithmic relationship between the degree of thinning and the time elapsed since the stroke. The speed of RTSD was highest in the first few years, after which it slowed down and reduced to just slightly higher than the background age-related thinning after 10 years. The authors were able to derive an equation which could predict the mean RNFL thickness in the event of RTSD from cortical injury: Mean RNFL (μm) = 110.3 − (9.08) * (elapsed time in log years) − (0.4) * (age at time of measurement). The longitudinal study allowed for serial measurements in each individual patient and confirmed maximal degeneration in the first 2 years, with a linear course during that time period and a mean slope of 4.4 μm/year, which is approximately 10 times that of simple age-related thinning. Thus, Cowey’s observations that RTSD occurred primarily in the first few years after a lesion in monkeys was now confirmed in humans.

Simplified representation of the anatomy of the retinal nerve fiber layer. Fibers carrying information from the temporal peripheral visual field which will contribute to the contralateral optic tract (crossed fibers) enter the optic nerve from the nasal side of the retina (N). Fibers carrying information from the nasal peripheral visual field which will contribute to the ipsilateral optic tract (uncrossed fibers) arc above and below the maculopapular bundle to enter the optic nerve from the superior (S) and inferior (I) sides of the retina. The maculopapular bundle which enters from the temporal side of the retina (T) contains fibers serving the central temporal visual field which will contribute to the contralateral optic tract (crossed) and the central nasal visual field, which will contribute to the ipsilateral optic tract (uncrossed). ONH optic nerve head, F fovea
Most notably, the time course study of Jindahra et al. found that those patients with less RTSD on OCT in the first few years after stroke were observed to demonstrate a greater degree of visual field recovery, providing a real-life clinical use for serial OCT in stroke patients with HH as a potential prognosticator of clinical improvement. Finally, their study found that patients with smaller hemianopic defects did not tend to show RTSD, either due to a limitation of the sensitivity of OCT RNFL measurements or due to some protective effect of the surrounding surviving neurons that represented uninjured cortex.
Goto and colleagues confirmed Jindahra’s findings in seven patients with acquired occipital disease (six were stroke) of varying durations using spectral domain OCT (SD-OCT), which has greater resolution and accuracy than the previous technique of time domain OCT [60]. Interestingly, they found RNFL thinning superonasally, but not inferonasally, in the contralateral eye, in accordance with prior study showing greater band atrophy at 1 o’clock on the nasal side [61]. It should be noted that Goto and colleagues’ observation of RNFL thinning even at the first visit (some of which were just a few months post-infarct) prompted them to consider a direct retrograde degeneration due to optic tract injury as a contributing mechanism.
Park and colleagues studied RNFL thickness in 46 patients who had suffered infarction of different territories, including 8 ACA (anterior cerebral), 21 middle cerebral (MCA), and 17 posterior cerebral artery (PCA) infarctions, and found evidence of RTSD in all three groups, with the most significant effect, not surprisingly, in the PCA group [62•]. Similar to other studies, they found a logarithmic correlation between time after infarction and degree of RNFL thinning. While the presence of apparent RTSD within the retina following ACA and MCA strokes is intriguing, it is not clear to the author that such atrophy is truly trans-synaptic since the optic tract itself is perfused by the anterior choroidal artery, a branch off the proximal MCA, and therefore, RNFL thinning in such cases could simply be simple retrograde. Similarly, the anterior optic chiasm and even sections of the distal optic nerves may be perfused by branches off the proximal ACA and anterior communicating arteries.
Ganglion Cell Layer Atrophy in RTSD
With the advent of SD-OCT, improvements in axial resolution have allowed for further segmentation of retinal layers and measurement of the combined thickness of the ganglion cell layer (GCL) and the adjacent inner plexiform layer (IPL). Such analysis can complement RNFL assessment in clinical practice in several ways. For example, by measuring the GCL-IPL complex thickness within the macula, rather than in a circumpapillary fashion, one can visualize neuronal atrophy due to papilledema or anterior ischemic optic neuropathy when there is still fiber swelling at the disc obscuring RNFL atrophy (although if the papilledema is severe, accurate GCL measurement is affected and artifactual GCL thinning may appear). Furthermore, since the measurements are performed in a rectangle around the macula, observed thinning can easily be related to the associated visual field loss with a simple mirror image relationship (left superior GCL thinning leads to right inferior visual field loss, for example), avoiding the complex relationship between RNFL bundles and visual field sectors that have been mapped most notably by Garway-Heath [63]. In 2012, Yamashita demonstrated homonymous GCL thinning in both eyes corresponding to the side of PCA infarction in three patients, 20, 36, and 12 months following the stroke [64]. Since the GCL thinning in the last patient was obvious by 12 months in the last patient, the implication was that RTSD of the GCL likely begins much earlier, although serial OCTs were not performed throughout that year to further elucidate this. The case series has the advantage that all subjects had suffered strokes, which offers a clear-cut date of onset of injury to the occipital cortex. The disadvantage, however, as pointed out by the authors, is that LGN ischemia might also occur in the setting of a PCA infarction, thus shedding some doubt on whether pure occipital damage would cause RTSD of the GCL. This point was addressed by a series of eight patients studied by Keller and colleagues in which four had suffered an intraparenchymal hemorrhage, two were status post-occipital lobectomy, and one had suffered a toxoplasmosis encephalopathy [65]. Latency between injury and OCT ranged from 1.4 to 9.8 years in this series. Since the majority of patients had quadrantanopia, the authors were able to show a correlation between the sector affected and the corresponding region of the occipital lobe affected. Furthermore, the degree of GCL atrophy in each quadrant showed a strong correlation to the pattern deviation scores in the corresponding quadrant on the Humphrey visual field.
Mitchell and colleagues studied the GCL of 22 patients with homonymous visual field loss due to occipital cortical disease of varying etiologies, including stroke, hemorrhage, tumor, encephalitis epilepsy mapping surgery, and multiple sclerosis, and found RTSD of the GCL in 15 patients, some of whom showed no RNFL thinning at all [66•]. The study required as an inclusion criteria exoneration of optic tract or LGN involvement, following careful review of MRI by two authors independently, one of whom was a neuroradiologist. This study utilized a normalized asymmetry score (NAS), defined as the summed contralateral sectors − the summed ipsilateral sectors, all divided by the contralateral sectors, as a reflection of the degree of GCL-IPL asymmetry, and compared this NAS to a group of 15 controls. The study indicated obvious RTSD of the GCL-IPL as early as 1 year, again indicating that RTSD must begin even earlier. A strong correlation between the degree of asymmetry and latency since occipital injury was demonstrated, and interestingly, the results suggested that some degree of RTSD continued on as far out as 10 years, with a plateau effect observed afterwards. Perhaps the most noteworthy finding in this study was the lack of observed RTSD of the GCL in two patients with quadrantanopia whose injury had occurred 10 years or more prior to assessment (one with infarct and one with epilepsy mapping surgery). Thus, RTSD clearly does not occur in all patients, at least as observable by OCT of the GCL, but the factors responsible for its presence or absence remain unclear. A more detailed look at one patient from this study can be found in Fig. 2.

Case study demonstrating retrograde trans-synaptic degeneration (RTSD) in the retinal GCL, but not RNFL. A 42-year-old woman presented after a year of intermittent headaches and brief episodes of blurry vision. a MRI with contrast revealed an enhancing mass in the right occipital lobe. The mass was resected and the pathology was consistent with a meningioma. Following the resection, the patient reported a new, constant loss of vision in her left visual field. b Humphrey visual fields revealed a left homonymous central field defect. c OCT of the GCL revealed homonymous thinning of the right side of both retinas consistent with RTSD. d OCT of the RNFL on the same day did not reveal evidence of RTSD. GCL ganglion cell layer, RNFL retinal nerve fiber layer, OCT optical coherence tomography, OD right eye, OS left eye
The greater sensitivity of GCL assessment over RNFL assessment for the detection of RTSD was further demonstrated by Herro and Lam, who showed GCL but not RNFL thinning in nine patients who had suffered an ischemic stroke, although the time between stroke and OCT was not known [67]. The results of Shin and colleagues, who looked at 11 patients with quadrantanopia from a variety of causes, were similar: a significant thinning of the GCL was observed in 20 of 22 eyes, and RNFL thinning was only observed in 15 [68]. It may be added that not only is GCL thinning more apt to occur following occipital lobe damage, but when it is present, its association with the cortical damage (as opposed to some occult retinal phenomenon) is more easily discerned as the atrophy respects the vertical meridian in both eyes. Conversely, the more complex pattern of RNFL thinning demonstrated by Jindahra and others must be carefully analyzed to differentiate RTSD from concomitant optic atrophy of other causes. See Table 2 for a summary of reports of RTSD in the human visual system.
RTSD in Multiple Sclerosis
In 2014, Gabilondo and colleagues published their observations of RTSD using OCT in a large cohort (n = 100) of patients with multiple sclerosis or clinically isolated syndrome [69••]. They found a strong correlation between a decrease in visual cortex volume and the degree of RNFL thinning, even when accounting for confounding events such as optic neuritis (ON), so that a decrease of 1 cm3 in the volume of visual cortex correlated to a 0.6 reduction in the mean RNFL. They also showed an association between the degree of NAA drop-off on MR spectroscopy and mean RNFL thickness, and an association between optic radiation lesion burden and RNFL thinning. Even though acute ON was accounted for, it has become apparent that OCT shows background RNFL thinning in MS patients apart from acute demyelinating events. Therefore, since there was no analysis of laterality or attempt to correlate exact cortical lesion location to corresponding retina degeneration, it is possible that these results do not indicate true RTSD, but rather reflect the fact that the background attrition of cortical fibers is roughly equivalent across the central nervous system in patients with MS, depending on the severity of their condition. ATSD was also observed: patients with a history of ON were found to have lower visual cortex volumes, and the decrement in volume was greater in patients with severe ON. On the whole, a history of ON predicted a 3-cm3 reduction in visual cortex volume. Such a relationship was not seen between ON and precentral gyrus volume, supporting the notion that the link reflected true ATSD of the visual pathway.
Petracca and colleagues analyzed GCL-IPL and total macular volume as well as RNFL and compared them to various measurements of cortical involvement using MRI in a cohort of 25 patients with primary progressive multiple sclerosis who had not had optic neuritis [70]. Their finding that RNFL thickness correlated with thalamic and cortical volume suggested RTSD, but since macular volume did not correlate with either thalamic or visual cortex volume, and since GCL-IPL thinning did not correlate with visual cortex volume, alternative mechanisms for retinal atrophy outside of RTSD were posited. Interestingly, they found that while GCL-IPL thickness was associated with cortical lesion number and volume, RNFL was not, suggesting that a common processing was affecting neuronal bodies in the cortical gray matter and retina, with relative sparing of axons. As in any MS study, differentiating RTSD in the retina from a direct effect of global degeneration proved challenging, but larger longitudinal studies with a greater capacity to match the specific location of retinal atrophy with corresponding regions in the cortex may help answer this question.
RTSD in Patients with Parkinson’s Disease?
The advent of OCT has allowed measurements of retinal parameters of patients with a wide array of degenerative diseases, including Parkinson’s disease (PD). One case–control study revealed RNFL thinning in patients with PD and visual hallucinations as compared to PD patients without hallucinations and controls [71]. With the assumption that patients with PD and hallucinations have dysfunction of the primary visual cortex or visual association cortex, the authors concluded that the RNFL thinning might be the product of RTSD. The same group performed MRI with DTI in patients with PD with and without visual hallucination and found reduced fractional anisotropy in the left optic nerve, atrophy of the left LGN, and an increase in diffusivity in the left optic radiation in the group with hallucinations, but no differences in visual cortex volume [72]. The authors surmised that loss of retinal cells due to direct effects of PD (alpha-synuclein inclusion bodies had previously been demonstrated in the inner nuclear layer, inner plexiform layer, and even GCL) [73] might lead to anterograde trans-synaptic degeneration of the LGN and optic radiations, thus placing the patients at greater risk of visual hallucinations.
Time Course of RTSD
As mentioned previously, Jindahra showed a rate of atrophy of the RNFL of 4.4 μm/year within the first 2 years following occipital lobe injury and found a logarithmic relationship between years past the injury and the degree of thinning. GCL thinning also follows a logarithmic curve based on Mitchell and colleagues’ study, but Yamashita’s analysis of seven patients with PCA stroke indicated a linear relationship [74]. These observations of GCL are based on cross-sectional analysis, and to my knowledge, there is no prospective longitudinal study of RTSD of the GCL at this point, although our group has begun such a study.
Interocular Differences
One would think that RTSD following unilateral occipital injury would affect the RNFL and GCL of both eyes to an equal extent, but this may not always be the case. Interestingly, in Yamashita’s 2016 study of seven patients with PCA stroke, there was increased thinning in the superotemporal and inferotemporal RNFL in the eye ipsilateral to the stroke, but thinning with the nasal sectors of the contralateral eye did not reach statistical significance. This is contrary to Théoret and colleagues’ findings in cats that the contralateral retina was affected to a greater extent. The latter finding might reflect the fact that there is a greater number of crossing fibers in a given eye, to account for the fact that the temporal field is slightly larger in each eye. The author has found that RTSD of the GCL may develop in one eye before the second as well, but the factors responsible for such interocular differences in timing and extent of RTSD remain unclear.
Pupillary Findings in RTSD
As pointed out in one case report showing RTSD of the GCL [75], one does not find a relative afferent pupillary defect (RAPD) in association with the RTSD, even though a contralateral RAPD is the norm following direct optic tract injury, due to the fact that there is a greater degree of crossing fibers than non-crossing fibers in each optic tract. This is not too surprising since the fibers responsible for the consensual pupillary response project to the midbrain and not the LGN and are therefore unlikely to be affected by RTSD. Quantitative analysis of pupillary function in patients with RTSD would help confirm this observation.
Pitfalls
As mentioned previously, direct retrograde retinal degeneration may be mislabeled as RTSD if optic tract damage is not carefully ruled out. In one recent case report, for example, obvious corresponding thinning of the RNFL and GCL was demonstrated as early as 2 months following severe head trauma [76]. While this was attributed to RTSD, there was no occipital lobe damage reported on the MRI (only intraventricular hemorrhage layering within the bilateral occipital horns), but diffuse axonal injury was shown. It is quite possible, therefore, that the observed retinal changes were the consequence of posttraumatic optic tract injury, which is known to occur [77] and may occur unilaterally depending on the vectors of blunt head trauma. Such an interpretation would be more consistent with the presence of such early retinal atrophy. Nevertheless, the study is notable for the fact that a significant (although not complete) improvement in visual fields was noted over time despite the progression of retinal atrophy, indicating that some degree of visual field loss is due to dysfunctional neurons that may come back online with time.
Clinical Utility of RTSD of the Human Visual System
It is still too early to know the extent to which our relatively newfound knowledge that RTSD occurs in the majority of human patients who acquire cortically based vision loss will result in any changes in clinical practice. One potential use, as put forth by Schwartz and colleagues, would be to diagnose likely visual field defects in patients with cortical disease who cannot tolerate formal visual field testing [78]. While structural assessment with OCT could never replace the functional testing of formal visual field testing (or confrontational visual field testing, for that matter), one can envision its utility in predicting and addressing suspected homonymous visual field (VF) loss in a patient who could not sit for VF testing.
A second use would be as a prognosticator of visual field recovery. It is logical to presume that patients with secondary retinal degeneration from a cortical insult would be less likely to recover their vision loss since, firstly, the lack of RTSD suggests true structural loss within the cortex and, secondly, since any cortical plasticity that might occur with time (or, as some believe, with “visual restoration therapy”) would likely not restore vision if the neurons responsible for upstream acquisition of the visual image had degenerated. Indeed, Jindahra’s finding that greater RNFL thinning was associated with a smaller chance of improvement supports this assumption. The problem of course is that, by the time OCT shows clear-cut RTSD, the time window for recovery of cortically mediated visual field loss is essentially over. In this regard, the degree of VF improvement is more likely to serve as a predictor of whether RTSD will show up on a future OCT. Perhaps future means of assessment will increase our sensitivity for the early changes of RTSD in the retina, allowing its practical use for prognosis.
A third use of RTSD is to aid in pinpointing the onset of an occipital stroke that was incidentally found on MRI.
Preventing RTSD?
It remains to be seen as to whether any intervention will dependably reduce RTSD in the human retina or, even if it does, whether that would reduce permanent visual field loss. It is possible that VRT, to the extent that it effects recovery after occipital lobe injury, might do so by reducing RTSD in the retina, by stimulating the ganglion cells, although it is hard to imagine why VRT would be stimulating those cells more than the regular light stimulation of typical daily activity. There is some evidence that neuroprotective agents might reduce ATSD: memantine, for example, when given to 16 monkeys with experimental glaucoma, resulted in less neuronal shrinkage in the occipital cortex than placebo [79], and intravitreal injection of the calcium channel blocker lomerizine decreased secondary atrophy of the LGN in rats with previous retinal lesions [80]. It is possible that RTSD could be similarly blocked following cortical lesions.
Key Points:
-
Retrograde trans-synaptic degeneration (RTSD) is defined as the secondary death of neurons following damage to their target neurons.
-
RTSD within the retina has been demonstrated pathologically in numerous feline and primate studies.
-
Retrograde trans-synaptic degeneration occurs in the human visual system following occipital cortex injury and can be demonstrated using optical coherence tomography (OCT) of the retina and with specialized MRI of the optic tract.
-
OCT analysis of the retinal nerve fiber layer (RNFL) and ganglion cell layer (GCL) both demonstrate RTSD, but GCL analysis appears to be more sensitive and offer a clearer demonstration of the phenomenon.
-
The speed of RTSD is greatest within the first 2 years, occurring in the RNFL at a rate of 4.4 μm/year. Clear evidence of RTSD typically becomes apparent by 1 year, and progression may continue over the course of a decade.
-
Animal studies indicate that RTSD of the ganglion cell layer affects mostly the B cells of the parvocellular pathway.
Conclusions
Although the idea of RTSD of the human visual system following cortical damage was controversial for much of the twentieth century, recent work using MRI and OCT has shown definitively that it does occur, both following congenital/neonatal lesions and those acquired as an adult. This is in accordance with a wealth of previous animal data showing the phenomenon pathologically. RTSD of the human visual system becomes easily apparent with OCT by 1 year and likely begins within a few months, if not immediately, following injury to the visual cortex. The speed of atrophy slows down after the first 2 years, but continues on steadily for up to 10 years. If we take into account this degeneration, we can conclude that the damage to the central nervous system following cortical injury, even after an acute stroke, is one that occurs for over a decade. Whether or not the recognition of this form of RTSD will prove clinically useful, and whether strategies to arrest it will help us in our attempt to restore vision loss following cortical injury, remain to be elucidated.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Nissl: Allg. Ztschr. f. Psychiat., 1891–1892, xlviii, p. 197.
James: Arch. Ophth., 1933, ix, p. 338.
Ranvier: Quoted by Ramon y Cajal, Degeneration and regeneration of the nervous system (translated by R. M. May). London: Oxford University Press; 1928, i, p. 6.
Bielschowsky: Bumke and Foerster, Handbuch der Neurologie. Berlin: Julius Springer; 1935, i, p. 155.
Leinfelder PJ. Retrograde degeneration in the optic nerves and retinal ganglion cells. Trans Am Ophthalmol Soc. 1938;36:307–15.
Campbell A. Histological studies on the localisation of cerebral function. Cambridge: Cambridge University Press; 1905.
Smith MC. Histological findings after hemicerebellectomy in man: anterograde, retrograde and transneuronal degeneration. Brain Res. 1975;95:423–42.
Cajal S, Ramon Y. Histologie du systeme nerveux de l’homme et des verte’bres. vol. 2, Paris: Maloine; 1911.
Minkowski M. Experimentelle Untersuchungen über die Beziehungen der Grosshirnrinde und der Netzhaut zu den primären optischen Zentren, besonders zum Corpus geniculatum externum. Arb. a. d. hirnanat. Inst., Zürich. 1913;7:255.
Clark WEL. A morphological study of the lateral geniculate body. Br J Ophthalmol. 1932;16:264.
Gartner S. Ocular pathology in the chiasmal syndrome. Am J Ophthalmol. 1951;34(4):593–6.
Juba A, Szatmari A. Ueber seltene hirnanatomische Befunde in Fällen von einseitiger peripherer Blindheit, Klin. Monatsbl. f. Augenh. 1937;99:173.
Perry VH, Cowey A. The effects of unilateral cortical and tectal lesions on retinal ganglion cells in rats. Exp Brain Res. 1979;35(1):85–95.
Hendrickson AE, Wilson JR, Ogren MP. The neuroanatomical organization of pathways between dorsal lateral geniculate nucleus and visual cortex in Old and New World primates. J Comp Neurol. 1978;182:123–36.
Harting JK, Huerta MF, Hashikawa T, van Lieshout DP. Projection of the mammalian superior colliculus upon the dorsal lateral geniculate nucleus: organization of tectogeniculate pathways in nineteen species. J Comp Neurol. 1991;304:275–306.
Hendry SHC. Striate and extrastriateoutput of a third geniculate channel in macaques. Invest Opthalmol Vis Sci. 1995;36:S292.
Rizzo III JF. Embryology, anatomy, and physiology of the afferent visual pathway. In: Miller NR, Newman NJ, editors. Walsh and Hoyt’s clinical neuro-ophthalmology. 6th ed. Philadelphia: Lippincott, Williams and Wilkins; 2005. p. 3–82.
Pearson HE, Labar DR, Payne BR, Cornwell P, Aggarwal N. Transneuronal retrograde degeneration in the cat retina following neonatal ablation of visual cortex. Brain Res. 1981;212(2):470–5.
Tong L, Spear PD, Kalil RE, Callahan EC. Loss of retinal X-cells in cats with neonatal or adult visual cortex damage. Science. 1982;217(4554):72–5.
Bowling DB, Michael CR. Projection patterns of single physiologically characterized optic tract fibres in cat. Nature. 1980;286(5776):899-902.
Théoret H, Herbin M, Boire D, Ptito M. Transneuronal retrograde degeneration of retinal ganglion cells following cerebral hemispherectomy in cats. Brain Res. 1997;775(1–2):203–8.
Rowe MH. Evidence for degeneration of retinal W cells following early visual cortical removal in cats. Brain Behav Evol. 1990;35(5):253–67.
Sturrock RR. Changes in the number of axons in the human embryonic optic nerve from 8 to 18 weeks gestation. J Hirnforsch. 1987;28:649–52.
Ng AYK, Stone J. The optic nerve of the cat: appearance and loss of axons during normal development. Dev Brain Res. 1982;5:263–71.
Carpenter P, Sefton AJ, Dreher B, Lim WL. Role of target tissue in regulating the development of retinal ganglion cells in the albino rat: effects of kainate lesions in the superior colliculus. J Comp Neurol. 1986;251(2):240–59.
Klüver H. Certain effects of lesions of the occipital lobes in macaques. J Psychol. 1937;4:383.
Van Buren JM. Trans-synaptic retrograde degeneration in the visual system of primates. J Neurol Neurosurg Psychiatry. 1963;26:402-9.
Cowey A. Atrophy of retinal ganglion cells after removal of striate cortex in a rhesus monkey. Perception. 1974;3:257–60.
Weller RE, Kaas JH, Wetzel AB. Evidence for the loss of X-cells of the retina after long-term ablation of visual cortex in monkeys. Brain Res. 1979;160:134–8.
Weller RE, Kaas JH, Ward J. Preservation of retinal ganglion cells and normal patterns of retinogeniculate projections in prosimian primates with long-term ablations of striate cortex. Invest Ophthalmol Vis Sci. 1981;20(2):139–48.
Cowey A, Stoerig P, Perry VH. Transneuronal retrograde degeneration of retinal ganglion cells after damage to striate cortex in macaque monkeys: selective loss of P beta cells. Neuroscience. 1989;29(1):65–80.
Ajina S, Pestilli F, Rokem A, Kennard C, Bridge H. Human blindsight is mediated by an intact geniculo-extrastriate pathway. Elife. 2015;20:4.
Herbin M, Boire D, Théoret H, Ptito M. Transneuronal degeneration of retinal ganglion cells in early hemispherectomized monkeys. Neuroreport. 1999;10(7):1447–52.
Cowey A, Stoerig P, Williams C. Variance in transneuronal retrograde ganglion cell degeneration in monkeys after removal of striate cortex: effects of size of the cortical lesion. Vis Res. 1999;39(21):3642–52.
Kupersmith MJ, Vargas M, Hoyt WF, Berenstein AB. Optic atrophy with cerebral arteriovenous malformations: direct and transsynaptic degeneration. Neurology. 1994;44:80–3.
Johnson H, Cowey A. Transneuronal retrograde degeneration of retinal ganglion cells following restricted lesions of striate cortex in the monkey. Exp Brain Res. 2000;132(2):269–75.
Scarlett HU, Ingham SD. Visual defects caused by occipital lobe lesions: report of 13 cases. Arch Neurol Psychiatr. 1922;8:225.
Austin GM, Lewey FH, Grant FC. Studies on the occipital lobe. 1. Significance of small areas of preserved central vision. Arch Neurol Psychiatr. 1949;62(2):204–21.
Wilbrand H, Saenger A. Die Erkrankungen des Opticusstammes, in Die Neurologie des Auges, Wiesbaden, J. F. Bergman. 1913;5.
Euzière J, Viallefont H, Vidal J. Double atrophie optique et hèmianopsie gauche consecutives à une blessure occipitale droite. Arch. Soc. d. sc. méd. et biol. de Montpellier. 1933;4:212.
Fledelius M. A propos de l’hémianopsie d’origine traumatique. Arch. d’opht. 1934;51:561.
Haddock JN, Berlin L. Transsynaptic degeneration in the visual system; report of a case. Arch Neurol Psychiatr. 1950;64(1):66–73.
Fletcher WA, Hoyt WF, Narahara MH. Congenital quadrantanopia with occipital lobe ganglioglioma. Neurology. 1988;38(12):1892–4.
Hoyt WF, Rios-Montenegro EN, Behrens MM, Eckelhoff RJ. Homonymous hemioptic hypoplasia. Fundoscopic features in standard and red-free illumination in three patients with congenital hemiplegia. Br J Ophthalmol. 1972;56(7):537–45.
Jacobson L, Hellström A, Flodmark O. Large cups in normal-sized optic discs: a variant of optic nerve hypoplasia in children with periventricular leukomalacia. Arch Ophthalmol. 1997;115(10):1263–9.
Beatty RM, Sadun AA, Smith L, Vonsattel JP, Richardson Jr EP. Direct demonstration of transsynaptic degeneration in the human visual system: a comparison of retrograde and anterograde changes. J Neurol Neurosurg Psychiatry. 1982;45(2):143–6.
Uggetti C, Egitto MG, Fazzi E, et al. Transsynaptic degeneration of lateral geniculate bodies in blind children: in vivo MR demonstration. AJNR Am J Neuroradiol. 1997;18(2):233–8.
Guedes ME, Almeida AC, Patricio MS, Costa JM. Acquired retrograde transsynaptic degeneration. BMJ Case Rep. 2011.
Bridge H, Jindahra P, Barbur J, Plant GT. Imaging reveals optic tract degeneration in hemianopia. Invest Ophthalmol Vis Sci. 2011;52(1):382–8.
• Millington RS, Yasuda CL, Jindahra P, et al. Quantifying the pattern of optic tract degeneration in human hemianopia. J Neurol Neurosurg Psychiatry. 2014;85(4):379–86. Millington et al. demonstrated trans-synaptic retrograde degeneration of the optic tract using diffusion-weighted imaging and T1 MRI in 22 patients following cortical injury, 13 with adult-onset hemianopsia and nine with congenital hemianopsia.
• Patel KR, Ramsey LE, Metcalf NV, Shulman GL, Corbetta M. Early diffusion evidence of retrograde transsynaptic degeneration in the human visual system. Neurology. 2016;87(2):198–205. Patel et al. used diffuse tensor imaging (DTI) MRI to demonstrate a greater asymmetry of fractional isometry in the optic tracts of 12 patients who were status post-injury to cortical visual pathways as compared to 12 patients with non-visual strokes and 28 healthy controls.
Stoerig P, Zrenner E. A pattern-ERG study of transneuronal retrograde degeneration in the human retina after a postgeniculate lesion. In: Kulikowski JJ, Dickinson CM, Murray JJ, editors. Seeing contour and colour. Oxford: Pergamon; 1989. p. 553–6.
Porrello G, Falsini B. Retinal ganglion cell dysfunction in humans following post-geniculate lesions: specific spatio-temporal losses revealed by pattern ERG. Vis Res. 1999;39(9):1739–45.
Azzopardi, King SM, Cowey A. Pattern electroretinograms after cerebral hemispherectomy. Brain. 2001;124(Pt 6):1228–40.
Mehta JS, Plant GT. Optical coherence tomography (OCT) findings in congenital/longstanding homonymous hemianopia. Am J Ophthalmol. 2005;140:727–9.
• Jindahra P, Petrie A, Plant G. Retrograde trans-synaptic retinal ganglion cell loss identified by optical coherence tomography. Brain. 2009;132:628–34. Here, Jindahra et al. demonstrated, for the first time, retrograde trans-synaptic degeneration in the human retina using optical coherence tomography following acquired lesions. Corresponding thinning of the retinal nerve fiber layer was observed in both patients with congenital lesions and in those with acquired lesions as compared to controls.
Miller NR, Newman SA. Transsynaptic degeneration. Arch Ophthalmol. 1981;99:1654.
Jindahra P, Petrie A, Plant GT. Thinning of the retinal nerve fibre layer in homonymous quadrantanopia: further evidence for retrograde trans-synaptic degeneration in the human visual system. Neuro-Ophthalmology. 2012;36:79–84.
•• Jindahra P, Petrie A, Plant GT. The time course of retrograde trans-synaptic degeneration following occipital lobe damage in humans. Brain. 2012;135:534–41. Jindahra et al. used cross-sectional data and longitudinal studies of individual patients to study the speed of RTSD in the retina. They also found that those patients with less RTSD in the first few years experienced greater recovery of visual field.
Goto K, Miki A, Yamashita T, et al. Sectoral analysis of the retinal nerve fiber layer thinning and its association with visual field loss in homonymous hemianopia caused by post-geniculate lesions using spectral-domain optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2016;254(4):745–56.
Ueda K, Kanamori A, Akashi A, Matsumoto Y, Yamada Y, Nakamura M. Evaluation of the distribution pattern of the circumpapillary retinal nerve fibre layer from the nasal hemiretina. Br J Ophthalmol. 2015;99:1419–23.
• Park HY, Park YG, Cho AH, Park CK. Transneuronal retrograde degeneration of the retinal ganglion cells in patients with cerebral infarction. Ophthalmology. 2013;120(6):1292–9. Park et al. showed RTSD in the retina of patients following infarcts of the ACA (n = 8), MCA (n = 21), and, most notably, of the PCA (n = 17). A logarithmic relationship between the degree of RNFL thinning and time since injury was demonstrated.
Garway-Heath DF, Poinoosawmy D, Fitzke FW, Hitchings RA. Mapping the visual field to the optic disc in normal tension glaucoma eyes. Ophthalmology. 2000;107(10):1809–15.
Yamashita T, Miki A, Iguchi Y, Kimura K, Maeda F, Kiryu J. Reduced retinal ganglion cell complex thickness in patients with posterior cerebral artery infarction detected using spectral-domain optical coherence tomography. Jpn J Ophthalmol. 2012;56(5):502–10.
Keller J, Sánchez-Dalmau BF, Villoslada P. Lesions in the posterior visual pathway promote trans-synaptic degeneration of retinal ganglion cells. PLoS One. 2014;9(5):e97444.
• Mitchell JR, Oliveira C, Tsiouris AJ, Dinkin MJ. Corresponding ganglion cell atrophy in patients with postgeniculate homonymous visual field loss. J Neuroophthalmol. 2015;35(4):353–9. Mitchell et al. devised a normalized asymmetry score to quantify RTSD in the GCL using OCT in 15 patients with adult-onset cortical injury, noting its onset by 1 year post-injury. They found that the time course of GCL atrophy extended as far out as 10 years. Of note is that RTSD was not observed in two patients with quadrantanopia from lesions that were over a decade old, demonstrating that RTSD of the GCL does not occur in every case.
Herro AM, Lam BL. Retrograde degeneration of retinal ganglion cells in homonymous hemianopsia. Clin Ophthalmol. 2015;9:1057–64.
Shin HY, Park HY, Choi JA, Park CK. Macular ganglion cell-inner plexiform layer thinning in patients with visual field defect that respects the vertical meridian. Graefes Arch Clin Exp Ophthalmol. 2014;252(9):1501–7.
•• Gabilondo I, Martínez-Lapiscina EH, Martínez-Heras E, et al. Trans-synaptic axonal degeneration in the visual pathway in multiple sclerosis. Ann Neurol. 2014;75(1):98–107. Gabilondo et al. showed that loss of visual cortex volume on MRI and a decrease in NAA signal on MR spectroscopy correlated with RNFL thinning, even when accounting for the occurrence of optic neuritis (ON), suggesting that this relationship was due to RTSD. Anterior trans-synaptic degeneration was also demonstrated as patients with optic neuritis had lower volume of their visual cortex, but not of the precentral gyrus.
Petracca M, Cordano C, Cellerino M, Button J, Krieger S, Vancea R, Ghassemi R, Farrell C, Miller A, Calabresi PA, Lublin F, Inglese M. Retinal degeneration in primary-progressive multiple sclerosis: a role for cortical lesions? Mult Scler. 2016. 2017;23(1):43-50
Lee JY, Kim JM, Ahn J, Kim HJ, Jeon BS, Kim TW. Retinal nerve fiber layer thickness and visual hallucinations in Parkinson’s disease. Mov Disord. 2014;29(1):61–7.
Lee JY, Yoon EJ, Lee WW, Kim YK, Lee JY, Jeon B. Lateral geniculate atrophy in Parkinson’s with visual hallucination: a trans-synaptic degeneration? Mov Disord. 2016;31(4):547–54.
Bodis-Wollner I, Kozlowski PB, Glazman S, Miri S. α-synuclein in the inner retina in Parkinson disease. Ann Neurol. 2014;75:964–6.
Yamashita T, Miki A, Goto K, Araki S, Takizawa G, Leki Y, Kiryu J, Tabuchi A, Iguchi Y, Kimura K, Yagita Y. Retinal ganglion cell atrophy in homonymous hemianopia due to acquired occipital lesions observed using cirrus high-definition-OCT. J Ophthalmol. 2016.
Meier PG, Maeder P, Kardon RH, Borruat FX. Homonymous ganglion cell layer thinning after isolated occipital lesion: macular OCT demonstrates transsynaptic retrograde retinal degeneration. J Neuroophthalmol. 2015;35(2):112–6.
Vien L, DalPorto C, Yang D. Retrograde degeneration of retinal ganglion cells secondary to head trauma. Optom Vis Sci. 2017;94(1):125–34.
Al-Zubidi N, Ansari W, Fung SH, Lee AG. Diffusion tensor imaging in traumatic optic tract syndrome. J Neuroophthalmol. 2014;34(1):95–8.
Schwartz SG, Pasol J, Lam BL, Flynn Jr HW. Spectral-domain optical coherence tomography documentation of transsynaptic retinal degeneration. Ophthalmic Surg Lasers Imaging Retina. 2016;47(8):768–72.
Yücel YH, Gupta N, Zhang Q, Mizisin AP, Kalichman MW, Weinreb RN. Memantine protects neurons from shrinkage in the lateral geniculate nucleus in experimental glaucoma. Arch Ophthalmol. 2006;124(2):217–25.
Ito Y, Nakamura S, Tanaka H, et al. Lomerizine, a Ca2+ channel blocker, protects against neuronal degeneration within the visual center of the brain after retinal damage in mice. CNS Neurosci Ther. 2010;16(2):103–14.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Marc Dinkin declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Neuro-Ophthalmology
Rights and permissions
About this article

Cite this article
Dinkin, M. Trans-synaptic Retrograde Degeneration in the Human Visual System: Slow, Silent, and Real. Curr Neurol Neurosci Rep 17, 16 (2017). https://doi.org/10.1007/s11910-017-0725-2
Published:
DOI: https://doi.org/10.1007/s11910-017-0725-2