
Abstract
The incidence of resistant hypertension, obesity, and obstructive sleep apnea (OSA), three highly prevalent conditions in the United States, is rising. Approximately one in three adults in the US has hypertension, and a significant proportion of these individuals have hypertension that is difficult to treat, or resistant. Obesity and OSA are well-established risk factors for resistant hypertension, a condition that portends significant cardiovascular risk. Awareness of the various mechanisms by which obesity and OSA impact systemic blood pressure is essential to better understand how best to effectively care for patients with resistant hypertension. In this review, we discuss the clinical and pathophysiologic associations between obesity, OSA, and resistant hypertension. Furthermore, we will explore the effect of continuous positive airway pressure therapy (CPAP) and other therapeutic interventions on blood pressure control in patients with resistant hypertension.
Key Points
• Obesity, obstructive sleep apnea, and resistant hypertension are highly prevalent conditions, with increasing overall incidence [1–3].
• Both obesity and obstructive sleep apnea are independent risk factors for the development of resistant hypertension.
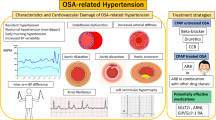
• OSA is characterized by a physiologic cascade of collapse of the upper airway, which can lead to intermittent hypoxia, hypercapnia, significant negative intra-thoracic pressure, and increased SNS output.
• Intermittent hypoxia leads to activation of the endothelin system [17, 18, 19•], which can lead to the development of resistant hypertension.
• Intermittent hypoxia can lead to the over activation of the SNS, which can also contribute to the development of resistant hypertension [20, 21].
• OSA leads to state of elevated adrenergic tone, which in turn may contribute to resistant hypertension [25–27].
• OSA patients have a higher incidence of “non-dipping” of nocturnal systolic blood pressure, a marker of increased adrenergic tone. This potentially represents a risk factor for hypertensive end organ disease [31, 32].
• The prevalence of OSA is significantly higher in patients predisposed to fluid accumulation: including kidney disease, heart failure and resistant hypertension [33].
• Interventions (such as the daytime use of compression stocking) which reduce daytime lower extremity fluid accumulation can significantly reduce the severity of OSA, particularly in patients with comorbid resistant hypertension [35, 36].
• CPAP therapy can significantly reduce blood pressure in patients with comorbid hypertension and OSA. The treatment effect is most pronounced in those with resistant hypertension and OSA [16••, 38–42].
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity, OSA, and hypertension are highly prevalent conditions, with increasing overall incidence [1–3]. In recent years, our growing understanding of the pathophysiology of these problems has led to increased realization of how they are interrelated. This review will provide an overview of our current understanding of the mechanisms linking obesity, OSA, and resistant hypertension.
Resistant hypertension is defined by the American Heart Association as blood pressure that remains above 140/90 mmHg in spite of concurrent use of three antihypertensive agents of three different classes at optimal dosing, of which one is a diuretic [4]. The prevalence of systemic hypertension as reported from the National Health and Nutrition Examination Survey (NHANES) is estimated at approximately 29 % to 31 % of adults [5]. The true prevalence of resistant hypertension is unknown, though it likely represents a significant portion of hypertensive patients [4].
OSA is a common disorder characterized by recurrent collapse of the upper airway during sleep. This leads to physiologic changes including transient hypoxia, intra-thoracic pressure changes, increased sympathetic nervous system (SNS) output, and recurrent cortical arousals. It is estimated to occur in approximately 5 % of the US population [6]. Large population based studies have consistently shown that OSA is somewhat more common in men than women [7]. As the prevalence of these problems grows, it is important as clinicians and scientists that we understand their interconnectedness so that we may offer improved treatments, and reduce the risk of cardiovascular disease.
Obstructive Sleep Apnea and Obesity are Risk Factors for Resistant Hypertension
The Framingham Heart Study, along with the HYDRA study, established a strong correlation between obesity and poor blood pressure control [8]. Obesity is defined as a body mass index (BMI) of ≥ 30, and is a major risk factor for both uncontrolled hypertension and OSA. In a retrospective review of participants of the Framingham Heart Study from 1990 to 1995, three main factors were identified in association with poor blood pressure control: older age, left ventricular hypertrophy, and obesity [9].
Although the development of hypertension may be partially genetic in etiology, several factors including increased sodium intake, older age, and obesity can clearly be associated with increased levels of blood pressure. Obesity can cause the earlier onset of hypertension. Weight loss, particularly the first ten pounds, can cause a substantial improvement in blood pressure. Obesity can also lead to decreased physical activity that can worsen blood pressure as well as allow progression of the obesity itself. The plight of patients who have entered this disastrous spiral is often minimized by health care providers who often view weight gain as a sign of poor self-control and a patients’ lack of ambition to take control of their own health. Rather, it is important for providers to be sympathetic to the conditions that allowed a patient to become overweight in the first place, remain understanding to the barriers that an individual patient may have to a better diet and access to regular exercise, as well as cultural and environmental barriers to weight loss.
Obstructive sleep apnea is also a risk factor for the development of resistant hypertension. In fact, in a recent study by Pedrosa et al., OSA was identified as the most common secondary condition associated with the development of resistant hypertension [10]. In their cohort of middle-aged patients with resistant hypertension, greater than 60 % of subjects were found to have at least moderate to severe OSA, based on standard diagnostic criteria. In comparison, the second most common etiology identified, primary aldosteronism, was seen in 5.6 % of subjects.
Similar findings were reported in two earlier trials, finding that the majority of patients with resistant hypertension who were referred for polysomnography had a significant degree of OSA [11, 12]. Concomitant OSA and resistant hypertension were much more common than concomitant OSA in subjects with controlled hypertension. Specifically, Gonçalves et al., reported that OSA was diagnosed in 71 % of patients with resistant hypertension, compared to 38 % of those with controlled systemic hypertension. Furthermore, there was a linear relationship between the severity of hypertension and the severity of OSA.
In a secondary analysis of data from the Metabolic Syndrome Outcome Study (MetSO), which is investigating metabolic syndrome among 200 African American patients in the primary-care setting, Demede et al., looked at associations between hypertension and OSA [13]. The prevalence of resistant hypertension in this cohort of patients was 26 %, which is in line with other published sources, which have estimated prevalence at 15–30 % of treated hypertensive patients [14•]. In their regression analysis, they concluded that patients with resistant hypertension were 2.5 times more likely to be at high risk for OSA compared to those with non-resistant hypertension.
Likewise, this has recently been reported in patients with resistant hypertension and end stage renal disease. Abdel – Kader reported that the severity of OSA was associated with a higher risk of resistant hypertension in a community based sample of subjects with end stage renal disease (N = 95), odds ratio: 7.1, 95 % confidence interval: 2.2-23.2 [15].
In 2012, Marin et al., published results from the Zaragoza Sleep Cohort Study, a prospective, observational study of 1889 subjects in Zaragoza, Spain who were referred by primary care physicians for evaluation of sleep-disordered breathing [16••]. Mean follow up time of these subjects was greater than 10 years. They reported that subjects with untreated OSA had a significantly increased risk of developing new-onset hypertension over time. This association persisted after adjusting for potential confounding variables, including baseline BMI, and change in BMI over time.
Pathophysiology of OSA, Obesity, and Resistant Hypertension
As described earlier, OSA is characterized by the repeated collapse of the upper airway during periods of sleep. This leads to a cascade of various physiologic changes that have been implicated in the development of multiple medical comorbidities, including resistant hypertension. Following collapse of the upper airway there can be intermittent hypoxia, hypercapnia, development of significant negative intra-thoracic pressure, and increased SNS output. Frequently these episodes lead to arousals from sleep, and thereby contribute to increased sleep fragmentation. These processes directly and indirectly may lead to the development of resistant hypertension. It is important to consider that this may be a bidirectional relationship, as processes involved in the development of hypertension may lead to or worsen OSA. In this section we will review the main pathophysiologic mechanisms that have been implicated. They include the downstream physiologic effects of recurrent hypoxia, endothelial dysfunction, autonomic dysfunction/increased SNS activity, nocturnal fluid shifts, and overactivation of the renin-angiotensin system.
Pathophysiology: Intermittent Hypoxia/Endothelial Dysfunction
We will first consider the impact that recurrent, intermittent hypoxia may have on the development of resistant hypertension. In patients with OSA following episodes of upper airway restriction or upper airway collapse, they will often have a brief oxyhemoglobin desaturation. As they arouse from sleep, there is resumption of airway patency and in turn a return to baseline oxyhemoglobin saturation. It is well established that oxidative stress and endothelial damage result from reactive oxygen species generated during periods of hypoxia and hypercapnia.
As the patient becomes hypoxemic there is a release of endothelin, a potent vasoconstrictor by the vascular endothelium [17]. As the oxygenation improves, there is a subsequent decrease in endothelin production and thereby vasodilation occurs. Earlier work by Phillips et al., suggested that in fact the cyclic alterations in endothelin levels throughout the night in OSA patients may contribute to the development of resistant hypertension [18]. Belaidi et al., looked at the expression of various factors in the endothelin system in a murine model of OSA [19•]. They used rats with a genetic predisposition towards the development of hypertension, and placed them in an experimental condition designed to mimic the intermittent hypoxia that characterizes this condition.They concluded that activation of the endothelin system, mediated by hypoxia inducible factor-1, is responsible for the cardiovascular changes leading to hypertension and ischemia.
Evidence has also suggested that hypoxia is likely the most potent stimulus for the increased SNS activity seen in OSA [20]. In a 2008 study, Gilmartin et al., set up an experimental condition in which ten healthy volunteers were placed in a condition with sustained nocturnal hypoxia (mean oxygen saturation 84.2 %, 9 h/night) for 14 consecutive nights [21]. At the end of this period they were shown to have a significant rise in mean arterial pressure, muscle sympathetic nerve activity, and forearm vascular resistance and blood flow. Though the mechanisms underlying this are uncertain, the authors concluded that recurrent nocturnal hypoxia increased sympathetic activity and thereby altered peripheral vascular tone. This type of model may not be directly applicable to the intermittent hypoxia that typically characterizes OSA, though there likely is some overlap in pathophysiologic mechanisms.
In 2000, Kato et al., published their findings regarding impairment of endothelium dependent vasodilation in subjects with OSA [22]. This was done by measuring forearm blood flow (by ultrasonography) after intra-arterial infusion of acetylcholine (a vasodilator that stimulates endothelial release of nitric oxide). They found that vasodilation was reduced in obese patients with severe OSA compared with age and body mass index matched controls. More recently several groups have published work demonstrating that these vascular changes can be reversed with the use of continuous positive airway pressure (CPAP) therapy [23•, 24]. Bayram et al.,, in a prospective, controlled, observational study, reported that endothelium-dependent flow-mediated dilation was improved after six months of continuous positive airway pressure (CPAP) in compliant subjects [23•].
In sum, the intermittent hypoxia that characterizes OSA leads to a cascade of physiologic changes including activation of the endothelin system, change in vascular tone, and increase in SNS tone.
Pathophysiology: Sympathetic Nervous System
We will now directly consider the role of excess SNS activity in OSA. Cyclic variation in heart rate (tachycardia-bradycardia phenomenon), atrio-ventricular conduction disturbances, and rises in blood pressure frequently occur during a post-apneic arousal. These processes are likely reflective of dynamic changes in both sympathetic and parasympathetic activity in response to an apnea or hypopnea. It is accepted that OSA leads to persistent increase in adrenergic tone both during periods of wakefulness and sleep [25]. Similarly, it is well established that adrenergic activity plays a key pathologic role in the development and maintenance of hypertension [26, 27].
In part, increased SNS activity occurs secondary to an increase in the chemoreflex drive [28]. These pathways have been delineated in several classic studies over the past 25 years. The chemoreflex drive is the system of negative feedback that regulates ventilation. Central chemoreceptors in the brain, and peripheral chemoreceptors in the body, detect and respond to changes in hydrogen ion concentration. Peripheral chemoreceptors, located in the carotid bodies, respond primarily to hypoxia. Central chemoreceptors, located on the ventral surface of the medulla, respond primarily to hypercapnia. Upon detection of an increased hydrogen ion concentration, chemoreceptors stimulate breathing via the chemoreflex arc. This term implies the signaling pathway from the central nervous system to the respiratory smooth muscle, which drives increased ventilation in response to increased brain tissue hydrogen ion concentration [29]. In addition to revving up minute ventilation, activation of the chemoreflex arc also causes increases in sympathetic activity, heart rate, and blood pressure [30].
A clinical correlate of these observations is reflected in the finding that OSA patients have a higher incidence of non-dipping of nocturnal systolic blood pressure [31]. Blood pressure normally decreases 10 % to 20 % during periods of sleep, compared to wake. A nocturnal decrease less than 10 % of daytime values defines nondipping [32]. It has been proposed that nondipping reflects increased underlying adrenergic tone. Perhaps most importantly, the loss of nocturnal dipping has been associated with increased end organ damage from hypertensive disease (renal, cardiovascular, and cerebrovascular)[32].
Pathophysiology: Rostral Fluid Shifts
The pathophysiologic relationship between obesity, OSA, and resistant hypertension also involves rostral fluid shifts. The prevalence of OSA increases with greater BMI and neck circumference/girth. This is likely secondary to fat deposition in the soft tissues surrounding the pharynx, which in turn narrows the upper airway lumen and increases collapsibility. However, there are other anatomic and physiologic factors that can influence the severity of OSA. One such dynamic that can impact severity of sleep apnea relates to the role of fluid retention states. Several studies have shown that the prevalence of OSA is significantly higher in patients predisposed to fluid accumulation, including kidney disease, heart failure and resistant hypertension [33].
Interestingly, the normally robust correlation between BMI/neck circumference and severity of OSA is poor in patients with fluid retention states [33]. This is explained by the fact that, during waking hours, fluid can accumulate in the intravascular and interstitial spaces of the legs. At night when people lay in a recumbent position, there can be redistribution of this fluid, leading to accumulation in the soft tissues surrounding the pharynx, thereby leading to a decrease in the cross sectional surface area of the upper airway [34•]. Other potential physiologic mechanisms are outlined clearly in the review by White & Bradley [34•]. Given these observations, it does not come as a surprise that daytime neck circumference may not accurately reflect the nocturnal dimensions of the upper airway.
Several studies have shown that interventions that reduce, daytime lower extremity fluid accumulation can significantly reduce the severity of OSA [35, 36]. Redolfi et al., studied 12 subjects with chronic venous insufficiency and OSA and had them wear compression stockings for 7 days [35]. They reported a significant decrease in overnight leg volume, neck circumference, and severity of OSA. Friedman and colleagues looked at a similar question in patients with resistant hypertension [36]. Their study looked at patients with drug-resistant hypertension (N = 25) and controlled hypertension (N = 15), and assessed their response to graded lower body positive pressure with compression stockings. The displacement of leg fluid volume was significantly greater in those with resistant hypertension compared to controlled hypertension. Accordingly, the resistant hypertension group had larger reductions in mean upper airway cross-sectional area and oropharyngeal junction area. Following from this, the authors concluded that rostral fluid shifts can represent a significant important pathophysiologic mechanism in patients with resistant hypertension and OSA.
Treatment of OSA and Resistant Hypertension
Positive Airway Pressure Therapy for Treatment of Resistant Hypertension
The most widely used therapy for the treatment of OSA is continuous positive airway pressure (CPAP). Mandibular advancement devices fashioned by dentists and otolaryngologic procedures are also utilized at times. An important question that follows our review of the pathophysiology linking these conditions is whether treatment of OSA leads to an improvement in resistant hypertension. Less is known about the converse, whether treatment of resistant hypertension can lead to improvement in OSA.
In several randomized trials and meta-analyses, CPAP for the treatment of OSA has effectively reduced blood pressure in patients, whether they were hypertensive at baseline or not [37]. Moreover, in the Zaragoza Sleep Cohort Study, treatment of OSA with CPAP was associated with a lower incidence of hypertension in patients followed for an approximate 12-year time period [16••].
When compared to antihypertensive medications, however, the degree of reduction in systemic blood pressure by CPAP therapy is lower. In a randomized crossover trial of 23 patients with both untreated hypertension and untreated OSA, treatment with valsartan (160 mg daily) lowered mean 24-hour blood pressure significantly more than treatment with CPAP. However, for those patients whose hypertension was not adequately controlled with either treatment modality, a combination of both valsartan and CPAP led to significant reduction in blood pressure [38]. While several studies have been conducted to determine the effect of CPAP on hypertension, only a few have specifically honed in on its effect in patients with resistant hypertension. Martinez-Garcia et al., described a reduction in systolic blood pressure and normalization of nighttime blood pressure patterns following treatment with CPAP, in 33 patients with OSA and resistant hypertension [39].
A few years earlier in the same journal, Logan et al., published their findings from a small study population of 11 patients with OSA and resistant hypertension who were treated with CPAP (in addition to three or more antihypertensive medications, including a diuretic, titrated to maximally effective doses). Results in this cohort of patients revealed a significant decrease in blood pressure, both systolic and diastolic [40].
In a retrospective chart review of 98 patients with OSA and hypertension, Dernaika et al., compared patients with resistant hypertension (n = 42) to those with controlled hypertension (n = 56). Mean difference in mean arterial pressure was −5.6 (95 % confidence interval [CI] -2.0 to −8.7 mm Hg; p = 0.03) in the group with resistant hypertension and −0.8 mm Hg (95 % CI −2.9 to 3.3 mm Hg; p = 0.53) in patients with controlled BP at the end of a 12-month follow up period. Seventy one percent of the patients with resistant hypertension were able to decrease their antihypertensive treatment while on CPAP therapy. Conversely, CPAP did not seem to have the same effect on patients with controlled hypertension. The authors concluded that a favorable response to CPAP therapy was found mainly in subjects with resistant hypertension [41].
Lozano et al., conducted one of the first prospective, randomized controlled parallel trials, looking at CPAP therapy in 75 patients with resistant HTN and apnea hypopnea index of ≥15 (at least moderate OSA) [42]. Study patients were randomized to receive CPAP therapy in addition to conventional antihypertensive therapy, versus conventional antihypertensive therapy alone. The medication regimen was not altered at all in the CPAP group. Ambulatory blood pressures were measured at initiation of the study, and at 3 months. Patients who used CPAP ≥5.8 hours nightly had clinically significant improvements in their systolic and diastolic blood pressure and a significant improvement in the nocturnal dipping pattern, the number of patients with a dipping pattern significantly increased in the CPAP group from 24.1 % to 57.1 %, P = 0.008. The end-point of the study was the change in ambulatory diastolic and systolic blood pressure at 3 months. They conclude that for patients with resistant hypertension and OSA, CPAP treatment for 3 months achieves significant reductions in 24-hour blood pressure.
As we consider the potential benefit of CPAP therapy on resistant hypertension, it is important to keep in mind the findings from the Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, that a decrease of only a few mmHg in blood pressure is sufficient to decrease significantly cardiovascular risk [1].
Novel Therapeutic Approaches for OSA and Resistant Hypertension
Gaddam et al., assessed the role of aldosterone-mediated fluid retention in patients with OSA and resistant hypertension. They completed a small, prospective, open-label study of 12 patients with resistant hypertension and OSA [43]. Following initial full diagnostic polysomnography, spironolactone (25–50 mg daily) was added to the patients’ antihypertensive regimen. Polysomnography performed 8 weeks after addition of spironolactone revealed a significant decrease in the apnea hypopnea index (AHI), the principal marker of the severity of OSA, from 39.8 +/− 19.5 respiratory events per hour of sleep to 22.0 +/− 6.8(p < 0.05) .
Moreover, weight and blood pressure measurements were significantly reduced as well. This study, though not a large randomized controlled trial, is the first study linking treatment with an aldosterone receptor antagonist with reduction of OSA severity. These results support the role of aldosterone-mediated fluid retention in OSA severity in individuals with resistant hypertension. Larger, randomized controlled studies are necessary to confirm the findings, and to better define the role of spironolactone as an adjunct treatment for patients with OSA and resistant hypertension.
Another area of interest with regard to therapy for OSA and resistant hypertension is that of renal sympathetic denervation. Briefly, renal sympathetic denervation therapy employs radio frequency ablation to the renal artery endothelial surface via a percutaneous catheter-based procedure. Studies have found that this intervention leads to a reduction of blood pressure; as efferent and afferent signaling is selectively inhibited in the kidney, decreased sodium is reabsorbed [44]. Decreased retention of sodium leads to a reduction in total body fluid by osmotic diuresis. In theory, one can postulate that lower total body fluid retention translates to less peri-pharyngeal fluid accumulation, ameliorating upper airway obstruction in patients with OSA.
Witkowski et al., investigated the effects of renal sympathetic denervation in a small cohort of patients with resistant hypertension and OSA [45•]. In this non-randomized, open-label study, ten patients with refractory hypertension and OSA received renal denervation therapy and subsequently underwent polysomnography and blood pressure measurements at 3-months and 6-months. At both the 3-month and 6-month follow-up points, significant decreases in systolic and diastolic blood pressures were observed (median: -34/-13 mm Hg for systolic and diastolic BPs at 6 months; P < 0.01). Moreover, a near-significant decrease was noted in the AHI at 6 months post renal denervation (median: 16.3 events per hour of sleep compared to 4.5 events per hour of sleep; P = 0.059). This is certainly an intriguing treatment option, though this study was not sufficiently powered to show a treatment benefit for OSA.
Treatment of Obesity and Resistant Hypertension
The treatment of obesity has long been approached with therapeutic lifestyle modifications including patient counseling, an exercise prescription, and an ongoing relationship with a nutritionist. Although such interventions are successful in a handful of people, successful weight loss and weight maintenance is a challenge to the majority of patients. Although once felt to be a treatment of last resort, improvements in bariatric surgery have been great over the past decade and can provide great therapeutic benefit to patients unable to achieve sustained weight loss by other means. The present guidelines suggest that patients with a BMI of >40 or a BMI >35 with significant comorbidities from their weight may benefit from weight loss surgery. Naturally, patients need to be of acceptable operative risk and be appropriate long-term candidates for such a procedure [46]. The increased recognition of the risks of severe obesity as well as improvements in the operations available make it incumbent upon health care providers to offer this option to the many patients who have failed standard weight loss attempts, particularly those who have tried for longer periods of times or repeatedly without true progress in achieving weight loss and maintenance.
Conclusions
Obesity, OSA, and resistant hypertension are highly prevalent problems that reflect a serious public-health burden. As clinicians and scientists caring for these patients, it is critical that we understand how these problems are interconnected. The reason being, with a better understanding of the pathophysiology underlying these problems, we will hopefully be able to offer easily accessible, efficacious therapies. Further, awareness of their interconnectedness, will hopefully remind clinicians that these are multidisciplinary problems, and may require clinicians to think outside the scope of their specialty.
All clinicians who are treating patients with resistant hypertension need to be aware of the high prevalence of underlying OSA in this population. We reviewed the pathophysiological mechanism, which may explain its association including: intermittent hypoxia, increased SNS output, and activation of the endothelin system [17, 18, 19•, 20, 21, 25–27]. Further, it should be recognized that in certain subpopulations of resistant hypertension, such as those predisposed to fluid accumulation including kidney disease and heart failure, risk of OSA is significantly higher [33].
It is well established that standard treatment for OSA with CPAP therapy, can significantly reduce comorbid hypertension [16••, 38–42]. The effect on lowering blood pressure appears to be most prominent in patients with resistant hypertension. Additionally, there is evidence of alternative therapies that may ameliorate the severity of sleep-disordered breathing in patients with resistant hypertension. Compression stockings, which reduce daytime lower extremity fluid accumulation, can significantly reduce the severity of OSA, particularly in patients with comorbid resistant hypertension [35, 36]. Additionally, renal sympathetic denervation may provide treatment benefit for both resistant hypertension and OSA [45•].
Finally, it is important to recognize that one of the biggest challenges in treating OSA is patient acceptance of CPAP therapy. CPAP is a highly effective therapy, with a diversity of clinical benefits, but patients often have a hard time getting beyond the idea of “I have to sleep with that on my face?” In our experience we have found that the more time spent explaining the clinical reason for using CPAP treatment, and the potential clinical benefits, the better the outcomes. Specifically, we have found that discussing potential associations, such as hypertension control and cardiovascular risk, resonates with a majority of patients. In sum, it helps patients answer the question of “Why am I going to wear that mask?”
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Chobanian AV, Bakris GL, Black HR. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee: Seventh Report of the Joint National. Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206–52.
Pubjabi NM. The Epidemiology of Adult Obstructive Sleep Apnea. Proc Am Thorac Soc. 2008;5(2):136–43.
Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999–2008. JAMA. 2010;303(3):235–41.
Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403.
Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension. JAMA. 2010;303(20):2043.
Jennum P, Riha RL. Epidemiology of sleep apnoea/hypopnoea syndrome and sleep-disordered breathing. Eur Respir J. 2009;33:907–14.
Young T, Palta M, Dempsey J, et al. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ. 2009;108(5):246.
Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403.
Persell SD. Prevalence of resistant hypertension in the United States, 2003–2008. Hypertension. 2011;57(6):1076–80.
Pedrosa RP, Drager LF, Gonzaga CC, Sousa MG, de Paula LK, Amaro AC, et al. Obstructive sleep apnea: the most common secondary cause of hypertension associated with resistant hypertension. Hypertension. 2011;58(5):811–7.
Gonçalves SC, Martinez D, Gus M, et al. Obstructive sleep apnea and resistant hypertension: a case–control study. Chest. 2007;132:1858.
Pratt-Ubunama MN, Nishizaka MK, Boedefeld RL, et al. Plasma aldosterone is related to severity of obstructive sleep apnea in subjects with resistant hypertension. Chest. 2007;131:453.
Demede M, Pandey A, Zizi F, et al. Resistant hypertension and obstructive sleep apnea in the primary-care setting. Int J Hypertens. 2011;2011:340929.
Pimenta E, Calhoun DA. Resistant hypertension: incidence, prevalence, and prognosis. Circulation. 2012;125(13):1594–6.
Abdel-Kader K, Dohar S, Shah N, Jhamb M, Reis SE, Strollo P, et al. Resistant hypertension and obstructive sleep apnea in the setting of kidney disease. Hypertens. 2012;30(5):960–6.
Marin JM, Agusti A, Villar I, et al. Association between treated and untreated obstructive sleep apnea and risk of hypertension. J Am Med Assoc. 2012;307(20):2169–76.
Khan A, Patel NK, O'Hearn DJ, Khan S. Resistant hypertension and obstructive sleep apnea. Int J Hypertens. 2013;2013:193010.
Phillips BG, Narkiewicz K, Pesek CA, et al. Effects of obstructive sleep apnea on endothelin-1 and blood pressure. J Hyper. 1999;17(1):61–6.
Belaidi E, Joyeux-Faure C, Ribuot SH, et al. Major role for hypoxia inducible factor-1 and the endothelin system in promoting myocardial infarction and hypertension in an animal model of obstructive sleep apnea. J Am Col Cardiol. 2009;53(15):1309–17.
Fava C, Montagnana M, Favaloro EJ, Guidi GC, Lippi G. Obstructive sleep apnea syndrome and cardiovascular diseases. Semin Thromb Hemost. 2011;37(3):280–97.
Gilmartin GS, Tamisier R, Curley M, et al. Ventilatory, hemodynamic, sympathetic nervous system, and vascular reactivity changes after recurrent nocturnal sustained hypoxia in humans. Am J Physiol Heart Circ Physiol. 2008;295(2):H778–85.
Kato M, Roberts-Thomson P, Phillips BG, et al. Impairment of endothelium-dependent vasodilation of resistance vessels in patients with obstructive sleep apnea. Circulation. 2000;102(21):2607–10.
Bayram NA, Ciftci B, Keles T, Durmaz T, Turhan S, Bozkurt E, et al. Endothelial function in normotensive men with obstructive sleep apnea before and 6 months after CPAP treatment. SLEEP. 2009;32(10):1257–63.
Panoutsopoulos A, Kallianos A, Kostopoulos K, Seretis C, Koufogiorga E, Protogerou A, et al. Effect of CPAP treatment on endothelial function and plasma CRP levels in patients with sleep apnea. Med Sci Monit. 2012;18(12):CR747–51.
Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest. 1995;96:1897–904.
Anderson EA, Sinkey CA, Lawton WJ, Mark AL. Elevated sympathetic nerve activity in borderline hypertensive humans. Evidence from direct intraneural recordings. Hypertension. 1989 Aug;14(2):177–83.
Grassi G, Cattaneo BM, Seravalle G, Lanfranchi A, Mancia G. Baroreflex control of sympathetic nerve activity in essential and secondary hypertension. Hypertension. 1998;31:68–72.
Cortelli P, Lombardi C, Montagna P. Parati Baroreflex modulation during sleep and in obstructive sleep apnea syndrome. G Auton Neurosci. 2012 Jul 2;169(1):7–11.
Narkiewicz K, Pesek CA, Kato M, et al. Baroreflex control of sympathetic nerve activity and heart rate in obstructive sleep apnea. Hypertension. 1998;32(6):1039–43.
Florczak E, Prejbisz A, Szwench-Pietrasz E, Sliwiński P, Bieleń P, Klisiewicz A, Michałowska I, Warchoł E, Januszewicz M, Kała M, Witkowski A, Więcek A, Narkiewicz K, Somers VK, Januszewicz A Clinical characteristics of patients with resistant hypertension: the RESIST-POL study. J Hum Hypertens. 2013 May 23.
Hla KM, Young T, Finn L, et al. Longitudinal association of sleep disordered breathing and nondipping of nocturnal blood pressure in the Wisconsin sleep cohort study. Sleep. 2008;31:795–800.
Ingelsson E, Bjorklund-Bodegard K, Lind L, Arnlov J, Sundstrom J. Diurnal blood pressure pattern and risk of congestive heart failure. JAMA. 2006;295:2859–66.
Yumino D, Redolfi S, Ruttanaumpawan P, Su MC, Smith S, Newton GE, et al. Nocturnal rostral fluid shift: a unifying concept for the pathogenesis of obstructive and central sleep apnea in men with heart failure. Circulation. 2010;121:1598–605.
White LH, Bradley TD. Role of nocturnal rostral fluid shift in the pathogenesis of obstructive and central sleep apnoea. J Physiol. 2013;591(Pt 5):1179–93.
Redolfi S, Arnulf I, Pottier M, Lajou J, Koskas I, Bradley TD, et al. Attenuation of obstructive sleep apnea by compression stockings in subjects with venous insufficiency. Am J Respir Crit Care Med. 2011 Nov 1;184(9):1062–6.
Friedman O, Bradley TD, Logan AG. Influence of lower body positive pressure on upper airway cross-sectional area in drug-resistant hypertension. Hypertension. 2013 Jan;61(1):240–5.
Alajmi M, Mulgrew AT, Fox J, et al. Impact of contiuous positive airway pressure therapy on blood pressure in patients with obstructive sleep apnea hypopnea: a meta-analysis of randomized controlled trials. Lung. 2007;185:67.
Pepin JL, Tamisier R, Barone-Rochette G, et al. Comparison of continuous positive airway pressure and valsartan in hypertensive patients with sleep apnea. Am J Respir Crit Care Med. 2010;182:954.
Martinez-Garcia MA, Gomez-Aldaravi JJ, Soler-Cataluna TG, et al. Positive effect of CPAP treatment on the control of difficult-to-treat hypertension. Eur Respir J. 2007;29(5):951–7.
Logan AG, Tkacova R, Perlikowski SM, et al. Refractory hypertension and sleep apnea: effect of CPAP on blood pressure and baroreflex. Eur Respir J. 2003;21(2):241–7.
Dernaika TA, Kinasewitz GT, Tawk MM. Effects of nocturnal continuous positive airway pressure therapy in patients with resistant hypertension and obstructive sleep apnea. J Clin Sleep Med. 2009;5(2):103–7.
Lozano L, Tovar JL, Sampol G, et al. Continuous positive airway pressure treatment in sleep apnea patients with resistant hypertension: a randomized, controlled trial. J Hypertens. 2010;28(10):2161–8.
Gaddam K, Pimenta E, Thomas SJ, Cofield SS, Oparil S, Harding SM, et al. Spironolactone reduces severity of obstructive sleep apnoea in patients with resistant hypertension: a preliminary report. J Hum Hypertens. 2010 Aug;24(8):532–7.
Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, Bohm M. Renal sympathetic denervation in patients with treatment-resistant hypertension (the Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376:1903–9.
Witkowski A, Prejbisz A, Florczak E, Kądziela J, Sliwiński P, Bieleń P, et al. Effects of renal sympathetic denervation on blood pressure, sleep apnea course, and glycemic control in patients with resistant hypertension and sleep apnea. Hypertension. 2011;58(4):559–65.
Bariatric surgery for severe obesity. National Institute of Diabetes and Digestive and Kidney Diseases. http://win.niddk.nih.gov/publications/PDFs/gasurg12.04bw.pdf, accessed October 12, 2013
Compliance with Ethics Guidelines
Conflict of Interest
Jonathan A. Marcus, Aravind Pothineni, Carolina Z. Marcus, and John D. Bisognano declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Hypertension and Metabolic Syndrome
Rights and permissions
About this article
Cite this article
Marcus, J.A., Pothineni, A., Marcus, C.Z. et al. The Role of Obesity and Obstructive Sleep Apnea in the Pathogenesis and Treatment of Resistant Hypertension. Curr Hypertens Rep 16, 411 (2014). https://doi.org/10.1007/s11906-013-0411-y
Published:
DOI: https://doi.org/10.1007/s11906-013-0411-y