
Abstract
Medical and device therapies that reduce heart failure morbidity and mortality also lead to decreased left ventricular volume and mass, and a more normal elliptical shape of the ventricle. These are due to changes in myocyte size, structure, and organization that have been referred to collectively as “reverse remodeling.” Moreover, there are subsets of patients whose hearts have undergone reverse remodeling following mechanical circulatory support with a ventricular assist device (VAD), who are able to be weaned from their VADs, which has been referred to as “myocardial recovery.” Although the term myocardial recovery has been used to describe the reversal of various aspects of the heart failure phenotype following medical and device therapy, there is no consensus with regard to what constitutes myocardial recovery; moreover, the methodology for identifying myocardial recovery in patients is unclear. These topics will be discussed in the current review.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Clinical studies have shown that medical and device therapies that reduce heart failure morbidity and mortality also lead to decreased left ventricular (LV) volume and mass and restore a more normal elliptical shape to the ventricle. These are due to changes in myocyte size, structure, and organization that, on a global level, are reflected in shifts of the LV end-diastolic pressure-volume relationship (EDPVR) toward normal. For want of better terminology these changes, which encompasses a myriad of changes at the molecular, cellular, tissue, and organ level, has been referred to as “reverse remodeling” [1, 2]. More recently, it has also become clear that a small subset of patients whose hearts have undergone reverse remodeling following support with a mechanical circulatory ventricular assist device (VAD) are able to be weaned from their VADs, which has been referred to as “myocardial recovery” [3]. These observations have engendered a great deal of interest, insofar as they may provide insight into understanding of fundamental mechanisms of heart failure that can lead to development of novel therapies to cure heart failure, as opposed to current approaches that are primarily designed to prevent disease progression by blocking the body’s homeostatic responses to heart failure (eg, neurohormonal activation) [1]. Despite the frequent synonymous use of the terms “myocardial recovery” and “reverse remodeling” to describe the reversal of various aspects of the heart failure phenotype following medical and device therapy, these terms describe different phenomena. Although there is abundant phenomenological understanding of “reverse remodeling,” there is no consensus with regard to the definition of what constitutes “myocardial recovery;” moreover, the methodology for identifying myocardial recovery in patients is unclear. Accordingly, these topics will be the focus of this review.
Myocardial Recovery
The concept that the failing heart could “recover” emerged in the heart failure literature in the mid-1990s following the observation that mechanical circulatory support with VADs was associated with decreased LV size and marked leftward shifts toward normal of the LV EDPVR, indicating that the heart was not simply unloaded, but rather that there were fundamental changes in the biological properties of the heart that allowed the ventricle to return toward normal size, shape, and function [2]. Moreover, there were anecdotal reports that some patients could be weaned from their VADs [4, 5]. These early observations were complemented by studies in heart failure patients treated with angiotensin-converting enzyme inhibitors and β blockers, in whom significant decreases in LV end-diastolic volume were noted compared to placebo controls [6, 7], although not to the same degree as observed with VADs. Viewed together these studies challenged the prevailing dogma that heart failure was irreversible and, in turn, fostered a greater interest in understanding the biological processes responsible for restoration of normal cardiac structure and function. However, our understanding of myocardial recovery has been called into question by studies in patients that have shown that while the mechanical unloading and normalization of the neurohormonal milieu provided by VADs routinely results in “reverse remodeling” (ie, restoration of LV size, shape, and EDPVR), as well as partial reversal of many aspects of the molecular and cellular heart failure phenotype, the vast majority of patients cannot be weaned from mechanical circulatory support: that is, they do not exhibit “myocardial recovery.” As shown in Table 1, the incidence of myocardial recovery is at best about 15 % (n = 120) in the selected cohorts of patients that have been reported (Table 1). Of note, the latest annual report from INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support), which summarized results of 2680 LVAD recipients from June 2006 to June 2010, reported a 1 % rate of VAD explantation for myocardial recovery [8••]. Thus, although reverse remodeling occurs in almost every patient receiving prolonged mechanical LV assist and is a requirement for myocardial recovery, reverse remodeling only rarely results in myocardial recovery. This then raises the broader question of what constitutes myocardial recovery.
Despite the frequent use of the term “myocardial recovery” to describe the reversal of various aspects of the heart failure phenotype following medical and device therapy, myocardial recovery has never been defined in the medical literature. In the absence of a previously established working definition, we have recently proposed that myocardial recovery of a failed heart be defined as the normalization of the molecular, cellular, myocardial, and LV geometric changes that provoked cardiac remodeling, which allows the heart to maintain preserved LV structure and function in the face of normal and/or perturbed hemodynamic loading conditions [9••]. Thus, although reversal of the heart failure phenotype at the cellular (myocyte) and molecular levels is likely necessary for the initiation of myocardial recovery and is responsible for the restoration of normal LV size and shape (ie, reverse remodeling), the sustainability of myocardial recovery will likely depend upon the ability of the heart to maintain preserved structure and function when the heart is once again exposed to normal and/or even perturbed hemodynamic loading conditions following withdrawal of mechanical support.
The observation that reverse remodeling and myocardial recovery are both associated with a normalization of many of the molecular, cellular, and anatomic changes that contribute to cardiac remodeling, suggests that recovery and reverse remodeling represent a simple reversal of the changes that occur during the progression of heart failure. However, this interpretation does not explain why reverse remodeling and myocardial recovery are not synonymous. One potential explanation for the disparity is that while the biology of reverse remodeling represents a return toward the normal non-pathological condition, reverse remodeling does not really represent normalization of the pathological heart failure condition. Several lines of evidence support this point of view. First, gene expression profiling studies have shown that only about 5 % of genes that are dysregulated in failing hearts revert back to normal following VAD support, despite typical morphologic and functional responses to VAD support [10, 11, 12•, 13]. Second, the majority of studies that have examined changes in the extracellular matrix (ECM) following VAD have suggested that the ECM does not revert to normal on its own, and can actually be characterized by increased myocardial fibrosis. It is only with simultaneous administration of pharmacologic neurohormonal blockade that ECM content reverts towards normal. Moreover, our current understanding of changes in the ECM during LVAD support have focused on ECM content and not with the more fundamental issues of its three-dimensional (3D) organization or with the interactions between the collagen matrix and the resident cardiac myocytes, which are likely to be critically important. Third, detailed studies of LV structure and function in human hearts following VAD support suggest that although the LV EDPVRs of VAD-supported hearts are shifted leftward, and more closely approximate those found in non-failing ventricles, the ratio of LV wall thickness to LV wall radius does not return to normal despite normalization of LV chamber geometry [14]. Thus, reverse LV remodeling does not result in normalization of LV wall stress. Whether this represents loss of functioning cardiac myocytes, myocyte atrophy from unloading, or failure of the 3D organization of the ECM to revert to normal is unknown. Taken together these observations suggest that the reverse remodeled heart is by no means a normal heart.
If reverse remodeling represents a partial normalization of the heart failure phenotype, does myocardial recovery represent a more complete normalization of the heart failure phenotype, or does it represent a unique biologic process that is distinct from reverse remodeling? Unfortunately, the extant literature is insufficient to address this question. Although the anatomic changes that occur during reverse remodeling and myocardial recovery appear to be identical, the opportunity to understand the biology of myocardial recovery at the molecular and cellular level has been limited to a small number of patients (n = 6), in whom myocardial tissue was obtained at the time of VAD explanation [15, 16]. The results of these studies suggest that recovery is associated with changes in the integrin signaling and β-adrenergic signaling pathways [16]. Unfortunately, parallel pathway analysis studies were not performed in patients who had undergone reverse remodeling but who did not recover. Accordingly, it is not possible to determine whether the aforementioned pathways are unique to recovery, or whether instead they also overlap with the pathways involved in reverse remodeling. In addition, given that there are thousands of genes that are dysregulated in heart failure, and that about 5 % are normalized during VAD support, it is unlikely that recovery is driven by a few unique genes. Thus, at the time of this writing we simply do not understand the biological differences between reverse remodeling and myocardial recovery.
How Can Myocardial Recovery Be Recognized Clinically?
In the absence of an established and well agreed upon definition of myocardial recovery, it is probably not surprising that we do not have well-defined ways to identify myocardial recovery in the clinical setting. As noted above, the normalization of LV geometry and end-diastolic properties of the left ventricle can, in certain clinical settings, be viewed as signature of reverse remodeling, but not necessarily a surrogate for myocardial recovery. The predictive accuracy of reverse remodeling as a surrogate for myocardial recovery is directly related to the “probability” that a patient will recover. That is, hearts are more likely to recover after treatment with drugs and/or devices in clinical situations wherein resolution of inflammation (ie, viral myocarditis or postpartum cardiomyopathy), removal of a toxic insult (eg, anthracyclines or alcohol), or restoration of more favorable energetics (ie, cessation of tachycardia) occurs. Several strategies have been employed clinically to evaluate the likelihood of recovery in patients who have been supported with a VAD. Mancini et al. [17] showed that performing rest and stress hemodynamics in patients with reduced VAD pumps speeds was useful for identifying potential “recovery” patients in whom the VAD could be explanted. Birks et al. [18•] used two-dimensional echocardiography to monitor LV structure and function following serial reductions in VAD pump speed, followed by 6-minute walk tests and cardiopulmonary exercise testing. VAD explantation was considered if, after reducing VAD pump speed to 6,000 rpm, the: 1) LV end-diastolic dimension was less than 60 mm, LV end-systolic diameter was less than 50 mm, and ejection fraction was greater than 45 %; 2) LV end-diastolic pressure or pulmonary capillary wedge were less than 12 mm Hg; 3) the resting cardiac index was greater than 2.8 L/min/m2; and 4) maximal oxygen consumption with exercise (mVO2) was greater than 16 mL/kg/min. However, it bears emphasis that, at the time of this writing, there is no universally agreed upon methodology for identifying patients who are most likely to recover following VAD explantation.
As noted above, the demographics of patients who “recover” suggest overwhelmingly that recovery is most likely to occur in younger patients with dilated, idiopathic cardiomyopathy of relatively short duration. In these settings medical and device therapy serve to support the heart and circulation, and/or to prevent further irreversible damage to the heart during the period of greatest hemodynamic compromise. Of interest, a recent study that examined microRNA profiling in patients with dilated cardiomyopathy who underwent successful VAD explantation showed that the expression levels of two microRNAs (miR 23a and 195) that predicted recovery were not different than those observed in non-failing hearts from age- and gender-matched controls, suggesting that recovery is possible in hearts with less advanced heart failure. Thus, for the present, although there are certain clinical characteristics that predict a more favorable probability of myocardial recovery, we do not have a reliable method for identifying which of these patients have truly recovered.
Conclusions
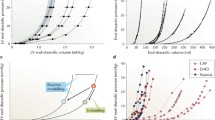
As discussed in the foregoing review, the failing heart is capable of undergoing favorable changes in LV volume and mass and to assume a more normal energetically favorable elliptical shape (reverse remodeling). Although the various components of reverse remodeling have been carefully studied and annotated, it is unclear at present exactly how these changes contribute to restoration of normal LV structure and function. That is, we simply do not understand what the essential biological “drivers” of myocardial recovery are, nor do we understand how they are coordinated. More importantly, we do not understand the key biological differences between reverse remodeling and myocardial recovery [9••, 19]. That is, the extant literature does not suggest which of the myriad of changes that occur during reversal of the heart failure phenotype are most important and/or necessary to preserve LV structure and function in the long term. Intuitively, one can speculate that changes within the myocardium, including both progressive loss of cardiac myocytes, as well as loss of the 3D organization of the ECM surrounding the cardiac myocytes are likely to be extremely important in terms of allowing the heart to respond to altered hemodynamic loading conditions (Fig. 1). The quest for seeking the answers to these questions extends well beyond simple intellectual curiosity about the biology of heart failure. The answers to these questions may help to better understand the differences between responders and nonresponders to medical and device therapy, as well as allow for the development of therapies that directly target myocardial recovery and effect a cure for heart failure, rather than continuing to target signaling pathways that attenuate remodeling.

Reverse remodeling and myocardial recovery. Cardiac remodeling arises secondary to abnormalities that arise in the biology of the cardiac myocyte (C), the myocardium (cardiocytes and extracellular matrix [M]), as well as LV geometry (LV), which have collectively been referred to as the heart failure (HF) phenotype. During reverse remodeling there is partial reversal of the abnormalities in the cardiac myocyte, as well as the extracellular matrix, leading to a reversal of the abnormalities in LV geometry. Although the biology of myocardial recovery is less well understood, it is likely that recovery occurs in hearts in which there is less underlying structural damage and a reversal of the HF phenotype. (Modified from Mann and Burkhoff [31])
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Kass DA, Baughman KL, Pak PH, Cho PW, Levin HR, Gardner TJ, Halperin HR, Tsitlik JE, Acker MA. Reverse remodeling from cardiomyoplasty in human heart failure. External constraint versus active assist. Circulation. 1995;91:2314–8.
Levin HR, Oz MC, Chen JM, Packer M, Rose EA, Burkhoff D. Reversal of chronic ventricular dilation in patients with end-stage cardiomyopathy by prolonged mechanical unloading. Circulation. 1995;91:2717–20.
Westaby S, Jin XY, Katsumata T, Taggart DP, Coats AJ, Frazier OH: Mechanical support in dilated cardiomyopathy: signs of early left ventricular recovery; 1997, pp 1303–1308.
Frazier OH. First use of an untethered, vented electric left ventricular assist device for long-term support. Circulation. 1994;89:2908–14.
Levin HR, Oz MC, Catanese KA, Rose EA, Burkhoff D. Transient normalization of systolic and diastolic function after support with a left ventricular assist device in a patient with dilated cardiomyopathy. J Heart Lung Transplant. 1996;15:840–2.
Konstam MA, Kronenberg MW, Rousseau MF, Udelson JE, Melin J, Stewart D, Dolan N, Edens TR, Ahn S, Kinan D. Effects of the angiotensin converting enzyme inhibitor enalapril on the long-term progression of left ventricular dilatation in patients with asymptomatic systolic dysfunction. SOLVD (Studies of Left Ventricular Dysfunction) Investigators. Circulation. 1993;88:2277–83.
Lindpaintner K, Lee MA, Larson MG, Rao S, Pfeffer MA, Ordovas JM, Schaefer EJ, Wilson AF, Wilson PWF, Vasan RS, Myers RH, Levy D. Absence of association or genetic linkage between the angiotensin-converting-enzyme gene and left ventricular mass. N Engl J Med. 1996;334:1023–8.
•• Kirklin JK, Naftel DC, Kormos RL, Stevenson LW, Pagani FD, Miller MA, Ulisney KL, Baldwin JT, Young JB: Third INTERMACS Annual Report: the evolution of destination therapy in the United States. J Heart Lung Transplant 2011, 30:115–23. This is the most recent report from the INTERMACS registry that shows that 1 % of VAD patients were explanted for myocardial recovery.
•• Mann DL, Burkhoff D: Myocardial expression levels of micro-ribonucleic acids in patients with left ventricular assist devices signature of myocardial recovery, signature of reverse remodeling, or signature with no name? J Am Coll Cardiol 2011, 58:2279–81. This is an editorial that provides the first working definition of myocardial recovery.
Margulies KB, Matiwala S, Cornejo C, Olsen H, Craven WA, Bednarik D. Mixed messages: transcription patterns in failing and recovering human myocardium. Circ Res. 2005;96:592–9.
Rodrigue-Way A, Burkhoff D, Geesaman BJ, Golden S, Xu J, Pollman MJ, Donoghue M, Jeyaseelan R, Houser S, Breitbart RE, Marks A, Acton S. Sarcomeric genes involved in reverse remodeling of the heart during left ventricular assist device support. J Heart Lung Transplant. 2005;24:73–80.
• Schwientek P, Ellinghaus P, Steppan S, D'Urso D, Seewald M, Kassner A, Cebulla R, Schulte-Eistrup S, Morshuis M, Rofe D, El BA, Korfer R, Milting H: Global gene expression analysis in nonfailing and failing myocardium pre- and postpulsatile and nonpulsatile ventricular assist device support. Physiol Genomics 2010, 42:397–405. This is a recent microarray analysis showing that the heart failure gene program is not reversed following pulsatile and nonpulsatile VADs.
Lowes BD, Zolty R, Shakar SF, Brieke A, Gray N, Reed M, Calalb M, Minobe W, Lindenfeld J, Wolfel EE, Geraci M, Bristow MR, Cleveland Jr J. Assist devices fail to reverse patterns of fetal gene expression despite beta-blockers. J Heart Lung Transplant. 2007;26:1170–6.
Barbone A, Oz MC, Burkhoff D, Holmes JW. Normalized diastolic properties after left ventricular assist result from reverse remodeling of chamber geometry. Circulation. 2001;104:I229–32.
Birks EJ, Tansley PD, Hardy J, George RS, Bowles CT, Burke M, Banner NR, Khaghani A, Yacoub MH. Left ventricular assist device and drug therapy for the reversal of heart failure. N Engl J Med. 2006;355:1873–84.
Hall JL, Birks EJ, Grindle S, Cullen ME, Barton PJ, Rider JE, Lee S, Harwalker S, Mariash A, Adhikari N, Charles NJ, Felkin LE, Polster S, George RS, Miller LW, Yacoub MH. Molecular signature of recovery following combination left ventricular assist device (LVAD) support and pharmacologic therapy. Eur Heart J. 2007;28:613–27.
Mancini DM, Beniaminovitz A, Levin H, Catanese K, Flannery M, DiTullio M, Savin S, Cordisco ME, Rose E, Oz M. Low incidence of myocardial recovery after left ventricular assist device implantation in patients with chronic heart failure. Circulation. 1998;98:2383–9.
• Birks EJ, George RS, Hedger M, Bahrami T, Wilton P, Bowles CT, Webb C, Bougard R, Amrani M, Yacoub MH, Dreyfus G, Khaghani A: Reversal of Severe Heart Failure With a Continuous-Flow Left Ventricular Assist Device and Pharmacological Therapy: A Prospective Study. Circulation 2011, 123:381–390. This is a recent prospective study that shows that the a combination of medical therapy and VAD support resulted in recovery in 60 % of the patients that were studied.
Mann DL. Mechanisms and models in heart failure: a combinatorial approach. Circulation. 1999;100:999–1088.
Maybaum S, Mancini D, Xydas S, Starling RC, Aaronson K, Pagani FD, Miller LW, Margulies K, McRee S, Frazier OH, Torre-Amione G. Cardiac improvement during mechanical circulatory support: a prospective multicenter study of the LVAD Working Group. Circulation. 2007;115:2497–505.
Dandel M, Weng Y, Siniawski H, Potapov E, Drews T, Lehmkuhl HB, Knosalla C, Hetzer R. Prediction of cardiac stability after weaning from left ventricular assist devices in patients with idiopathic dilated cardiomyopathy. Circulation. 2008;118:S94–S105.
Dandel M, Weng Y, Siniawski H, Stepanenko A, Krabatsch T, Potapov E, Lehmkuhl HB, Knosalla C, Hetzer R. Heart failure reversal by ventricular unloading in patients with chronic cardiomyopathy: criteria for weaning from ventricular assist devices. Eur Heart J. 2011;32:1148–60.
Drakos SG, Terrovitis JV, Nastasiou-Nana MI, Nanas JN. Reverse remodeling during long-term mechanical unloading of the left ventricle. J Mol Cell Cardiol. 2007;43:231–42.
Drakos SG, Charitos EI, Nanas SN, Nanas JN. Ventricular-assist devices for the treatment of chronic heart failure. Expert Rev Cardiovasc Ther. 2007;5:571–84.
Liden H, Karason K, Bergh CH, Nilsson F, Koul B, Wiklund L. The feasibility of left ventricular mechanical support as a bridge to cardiac recovery. Eur J Heart Fail. 2007;9:525–30.
Gorcsan III J, Severyn D, Murali S, Kormos RL. Non-invasive assessment of myocardial recovery on chronic left ventricular assist device: results associated with successful device removal. J Heart Lung Transplant. 2003;22:1304–13.
Matsumiya G, Monta O, Fukushima N, Sawa Y, Funatsu T, Toda K, Matsuda H. Who would be a candidate for bridge to recovery during prolonged mechanical left ventricular support in idiopathic dilated cardiomyopathy? J Thorac Cardiovasc Surg. 2005;130:699–704.
Simon MA, Primack BA, Teuteberg J, Kormos RL, Bermudez C, Toyoda Y, Shah H, Gorcsan III J, McNamara DM. Left ventricular remodeling and myocardial recovery on mechanical circulatory support. J Card Fail. 2010;16:99–105.
Farrar DJ, Holman WR, McBride LR, Kormos RL, Icenogle TB, Hendry PJ, Moore CH, Loisance DY, El Banayosy A, Frazier H. Long-term follow-up of Thoratec ventricular assist device bridge-to-recovery patients successfully removed from support after recovery of ventricular function. J Heart Lung Transplant. 2002;21:516–21.
Drakos SG, Kfoury AG, Selzman CH, Verma DR, Nanas JN, Li DY, Stehlik J. Left ventricular assist device unloading effects on myocardial structure and function: current status of the field and call for action. Curr Opin Cardiol. 2011;26:245–55.
Mann DL, Burkhoff D. Myocardial expression levels of micro-ribonucleic acids in patients with left ventricular assist devices signature of myocardial recovery, signature of reverse remodeling, or signature with no name? J Am Coll Cardiol. 2011;58:2279–81.
Acknowledgments
This research was supported by research funds from the National Institutes of Health (RO1 HL58081, RO1 HL61543, RO1 HL-42250).
Disclosure
Conflicts of interest: D.L. Mann: none; D. Burkhoff: is employed by and has stock/stock options with CircuLite.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mann, D.L., Burkhoff, D. Is Myocardial Recovery Possible and How Do You Measure It?. Curr Cardiol Rep 14, 293–298 (2012). https://doi.org/10.1007/s11886-012-0264-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11886-012-0264-z