
Abstract
Background
Pelvic fractures are usually the result of high-energy trauma and may have associated soft tissue and organ damage resulting in significant morbidity and mortality in these patients. Currently, there is little data from Ireland regarding these injuries.
Objective
To study the epidemiology of pelvic fractures presenting to a tertiary referral centre in Dublin.
Methods
Patients referred with a pelvic fracture were identified using the Hospital Inpatient Enquiry System (HIPE) from 1998 to 2008. The patient’s medical notes were reviewed for demographic data, type and mechanism of fracture and associated injuries.
Results
A total of 509 patients were identified over the 10-year period. 466 patients were included in the study. There was a significant male preponderance 76% (n = 354) as compared to females 24% (n = 112). Mean age was 36.5 years (range 16–83). Road traffic accidents (RTA) were the cause in 74% (n = 346) of the cases.
Conclusion
From our study, the typical patient profile is one of a male in his 30’s involved in an RTA requiring acetabular surgery. This is in accordance with previously published international data and highlights the need for specialised units, training in this subspecialty and allocation of resources.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pelvic fractures are relatively uncommon injuries and are challenging to manage. The high energy required to disrupt the pelvis often results in complex injury patterns with significant morbidity and mortality. Road traffic accidents (RTAs) are the commonest cause of major pelvic ring injuries, followed by falls from a height [1–3]. Such injuries can be life-threatening and with devastating physical, psychological and social long-term sequalae. The costs to the patient, their family and the health care system can be enormous [4].
Relatively little data exists regarding the aetiology and demographics of pelvic and acetabular trauma [5]. Current research focuses on a specific patient profile, the mode and the pattern (stable vs unstable) of injury and of course the effect on morbidity and functional outcome of a possible surgical intervention.
The aim of this study is to identify and analyse the demographic data of pelvic and acetabular trauma in a Dublin tertiary hospital over a 10-year period.
Materials and methods
An analysis of all the cases of pelvic and acetabular trauma that underwent surgery over a 10-year period (June 1998–June 2008) was carried out, retrospectively. Our unit undertakes the majority of orthopaedic trauma from a population base of approximately 400,000 in its catchment area. It is also the National Referral Centre for pelvic and acetabular trauma. Two surgeons carried out all pelvic and acetabular surgeries during this period.
Any procedure to the pelvis, acetabulum or both was included. Removals of metal and soft tissue debridement procedures were excluded. The hospital inpatient inquiry (HIPE) system, operating theatre registry, electronic operative note and radiographic archives were used to gather the data. Demographic data, geographical case distribution by county, mechanism and site of injury were noted. Two independent orthopaedic trainee registrars reviewed the charts and radiographs of each patient. Data for each patient were entered into a Microsoft Excel (Microsoft Corporation) database.
Results
During the 10-year period, a total of 509 pelvic and acetabular surgeries took place. The incidence of traumatic pelvic and acetabular injury requiring surgical intervention was 1.13 per 100,000 people per year based on the national population statistics [6]. Such pelvic trauma (including transfers) constituted 2% of the total admissions per year. Due to incomplete data and records, 466 of such operations were analysed.
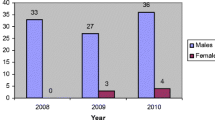
The number of operative procedures per annum over the 10-year period is depicted in Fig. 1. The average age was 36.5 years (16–83) with a significant male preponderance of 76%. Figure 2 depicts the number of patients per age group. The vast majority of the injuries were due to RTAs (72.4%), the remainder primarily due to falls from a height (27.6%). The acetabulum was the most common site (68%) of injury requiring surgery as depicted in Fig. 3. There was an average of 31.4 acetabular surgeries performed per annum, with 61% of these carried out on the left acetabulum. The geographical distribution of referrals to our unit is represented in Fig. 4. While the number of injuries due to RTAs remained similar over this time, the number due to falls from a height increased from 2001 onwards. Similarly, the number of non-nationals injured increased during this time as depicted in Fig. 5.

Number of operative procedures per annum

The number of cases per age group

Sites of injury

Geographical distribution of referrals

Non-national group numbers as a percentage of the workload
Discussion
This study describes the demographic and epidemiologic data of pelvic and acetabular injuries seen in an Irish tertiary trauma centre over a 10-year period. The typical patient profile is one of a male in his 30’s involved in an RTA requiring acetabular surgery. Two specific patterns emerge from our study: the 20–39 year age group and the non-national group. As there is no National Trauma Registry and our data only captured injuries requiring surgical intervention, it does not include conservatively managed cases or the small number of cases surgically managed elsewhere. It makes comparison of our data to that available in the literature difficult. Our calculated incidence of 1.13 per 100,000 people per annum is therefore a conservative estimate of only the injuries that need surgical intervention. This is lower than the reported 19–37 per 100,000 incidence of pelvic trauma requiring hospitalisation [7, 8].
The steady workload over the decade analysed in combination with such a young population profile requiring aggressive surgical management highlights the need for specialized units, pelvic and acetabular reconstruction surgery training and dedicated resources [1]. Outcome from such fractures has been demonstrated to be associated with accuracy of surgical reduction [12, 13]. Therefore, the likelihood of these patients returning to employment is predicated on optimal surgical management.
Patients had been transferred for surgical management from all corners of the country. The counties with the higher number of these injuries were also noted to have recorded higher number of RTA-related fatalities [9]. Despite improvements in motor vehicle safety and better motorway networks over the last decade, the number of these injuries has remained constant. This may in part be due to the rising number of injuries due to falls, this was the most notable in 2008.
The increasing trend in non-nationals injured during this period seems to correlate well with the increased migration into Ireland fuelled by the economic and construction boom. Analysis within this group showed an increase in the number of falls from a considerable height reflecting work-related injuries. Work safety regulations and their potential lack of stringent enforcement needs to be addressed at a national level. RTAs remained the predominant mechanism of injury within this group. Most non-nationals in our study emigrated from continental Europe where they drive on the right hand side of the road unlike Ireland. Influx of non-nationals into Ireland peaked in 2006, with Poland, Lithuania and Slovakia contributing to more than half of the 227,000 migrants that year. A further 180 countries contributed to the rest [10]. This may underscore a need to examine the driving licensing requirements in this country. The language barrier adds a layer of complexity necessitating organised interpreter services and an increasing expense [11]. Most of these injuries incur extensive time off from work and most of these patients prefer to return to their homes. Similar trend has been noted by Sattler et al. in their single center study describing hand injuries in the non-national population [12]. A centralised repatriation service would seem to benefit non-national patients who would wish to do so.
Kirkler [14] identifies current difficulties that exist in UK with regards to pelvic and acetabular fracture data and concluded that timely and high quality systems are needed for the optimal management of these patients. This will require a new coding system, coupled with robust and reliable collection of data. Geoghegan et al. [15] have demonstrated that inconsistent and inadequate data leads to incorrect proportioning of resources and between 2003 and 2004 trauma centres across the UK may have lost funding of more than £7 million as a result. Countries such as Germany where trauma registries have already been established have demonstrated that the outcomes are improving and overall mortality is decreasing [16–18].
One of the limitations of our study is that it includes only the patients requiring surgery. As such our figures with regards to the incidence of pelvic and acetabular trauma do not take into account non-displaced fractures that may have been managed in regional centres. This is a retrospective study with its inherent limitations, the main disadvantage being that the data were extracted from information already gathered and documented without our control or design. For example due to incomplete data from medical records and from HIPE, we were unable to accurately calculate the average length of stay.
Conclusion
From our study, the typical patient profile is one of a male in his 30’s involved in an RTA requiring acetabular surgery. Two specific patterns emerge from our study: the 20–39-year age group and the non-national group. We noted a constant workload of around 50 admissions per annum requiring surgical intervention. In the current economic climate, careful planning and allocation of resources is even more crucial. With this data, our hospital will be able to better estimate the costs involved and make future provisions. We highlight the need for a national trauma register and for dedicated systems to be developed for seamless transfer of patients to an institution where an appropriate standard of care is available.
References
Giannoudis PV, Grotz MR, Tzioupis C et al (2007) Prevalence of pelvic fractures, associated injuries, and mortality: the United Kingdom perspective. J Trauma 63(4):875–883
Gänsslen A, Pohlemann T, Paul C, Lobenhoffer P, Tscherne H (1996) Epidemiology of pelvic ring injuries. Injury 27(Suppl 1):S-A13-20
Laird A, Keating JF (2005) Acetabular fractures: a 16-year prospective epidemiological study. J Bone Joint Surg Br 87(7):969–973
Geoghegan JM, Longdon EJ, Hassan K, Calthorpe D (2007) Acetabular fractures in the UK. What are the numbers? Injury 38(3):329–333 (Epub 2006 Dec 18).
Demetriades D, Karaiskakis M, Toutouzas K, Alo K, Velmahos G, Chan L (2002) Pelvic fractures: epidemiology and predictors of associated abdominal injuries and outcomes. J Am Coll Surg 195(1):1–10
Population Estimates: Central Statistics Office http://www.cso.ie/px/pxeirestat/database/eirestat/Population%20Estimates/Population%20Estimates_statbank.asp. Accessed 15 December 2009
Ragnarsson B, Jacobsson B (1992) Epidemiology of pelvic fractures in a Swedish county. Acta Orthop Scand 63(3):297–300
Melton LJ, Sampson JM, Morrey BF, Ilstrup DM (1981) Epidemiologic features of pelvic fractures. Clin Orthop Relat Res 155:43–47
Collision Fact Book: Road Safety Authority (2009) http://www.rsa.ie/Documents/Road%20Safety/Crash%20Stats/Collision_Fact_Book_07.pdf. Accessed 15 December 2009
Foreign National Activity: Central Statistics Office (2009) http://www.cso.ie/px/pxeirestat/database/eirestat/Foreign%20National%20Activity/Foreign%20National%20Activity_statbank.asp?SP=ForeignNationalActivity&Planguage=0. Accessed 15 December 2009
Sattler T, Tobbia D, O’Shaughnessy M (2009) Hand injuries in foreign labour workers in an Irish university hospital. Can J Plast Surg Spring 17(1):22–24
Matta JM (1996) Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 78(11):1632–1645
Wright R, Barrett K, Christie MJ, Johnson KD (1994) Acetabular fractures: long-term followup of open reduction and internal fixation. J Orthop Trauma 8(5):397–403
Krikler SJ (2010) Problems with pelvic and acetabular fracture data. Injury 41(7):676
Geoghegan JM, Longdon EJ, Hassan K, Calthorpe D (2007) Acetabular fractures in the UK. What are the numbers? Injury 38(3):329–333
Hauschild O, Strohm PC, Culemann U et al. (2008) Mortality in patients with pelvic fractures: results from the German pelvic injury register. J Trauma 64(2):449–455
Pohlemann T, Tosounidis G, Bircher M, Giannoudis P, Culemann U (2007) The German Multicentre Pelvis Registry: a template for an European Expert Network? Injury 38(4):416–423 (Epub 2007 Mar 29)
Nwomeh BC, Lowell W, Kable R, Haley K, Ameh EA (2006) History and development of trauma registry: lessons from developed to developing countries. World J Emerg Surg 1:32
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Davarinos, N., Ellanti, P., Morris, S. et al. Epidemiology of pelvic and acetabular trauma in a Dublin tertiary hospital: a 10-year experience. Ir J Med Sci 181, 243–246 (2012). https://doi.org/10.1007/s11845-011-0791-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-011-0791-4