
Abstract
Objectives
This study aimed to review the epidemiological aspects of acetabular fractures treated at Hamad Medical Corporation in Qatar. The study is the first orthopaedic trauma epidemiological study in Qatar and will provide a platform to advance high-level clinical research.
Methods
We obtained data for 103 patients who presented to our level I trauma centre from 2008 to 2010 with a diagnosis of acetabular fracture. Age, sex, the cause of injury, fracture classification, mode of treatment, associated nerve injuries, and other complications were analyzed.
Results
The incidence of acetabular fracture was 2/100,000/year. Males (93.2%) predominated. The mean age at injury time was 36 years, and the most common cause of injury was motor vehicle collisions (49.5%). Injuries were mostly primary acetabular fractures (73.6%) in comparison to (26.4%) for associated fractures. Posterior wall fractures were the most common pattern (25.2%). Associated posterior hip dislocation occurred in 21.3% of cases. Data revealed a lower incidence of post-traumatic sciatic nerve palsy (7%) that was present at the time of injury. There were no cases of reported mortality.
Conclusion
Acetabular fractures are uncommon injuries with motor vehicle collision being the most common cause of injury. Posterior wall fracture was the most frequent pattern, and most of the patients were males. The incidence of post-traumatic sciatic nerve palsy and the proportion of injured women were lower than those reported in literature. Well-trained surgeons and specialized centres for treating these injuries are recommended.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acetabular fractures are usually severe injuries and mostly associated with high-energy trauma [1, 2]. They are challenging orthopedic injuries that require particular attention and expertise for treatment. The literature on the epidemiology of acetabular fractures is scant. Road traffic accidents reported as the most common cause of injury [1,2,3,4,5,6,7].
Due to massive construction and growing industry, increasing numbers of acetabular fractures are encountered, although more recent publications have shown that the incidence of acetabular fractures is decreasing with the introduction of the seat belt, improved worksite, and automobile safety [2, 5, 8, 9].
Over the last decade, treatment of displaced acetabular fractures has progressed from non-surgical to the surgical approach. Through the contribution made by Letournel [1], open anatomical reduction and rigid internal fixation are now the gold standards for treating displaced fractures of the acetabulum [10,11,12,13].
Qatar is one of the fastest developing economies in the world. It has a particular demographic as 80% of the population are expatriate young male workers. Major construction projects across the country, including stadiums, railways, and large-scale residential and commercial buildings have added an extra burden to the healthcare system [14].
Hamad Medical Corporation (HMC) has a level I trauma centre in Hamad General Hospital (HGH), which is the only trauma centre of its kind in Qatar that is promoting clinical excellence and high-quality research, and serves a population of around two million with an average of 3000 musculoskeletal injuries per year [15].
The purpose of this retrospective study was to make a comparison of our epidemiological analysis of acetabular fractures managed between March 2008 and November 2010 with epidemiological data reported in literature [1, 2, 6, 11, 16].
Methods and materials
A retrospective analysis was conducted on all the cases of acetabular fracture treated at HGH between March 2008 and November 2010. The institutional review board at HMC approved the study.
Patient data, retrieved from medical records and radiology archives, were reviewed to identify patients diagnosed with acetabular fractures. All patients with acetabular fracture and a follow-up until February 2011 were included regardless the age or other injuries. Radiographs were reviewed to exclude any miscoded diagnosis for all cases.
Data for essential details including age, gender, the cause of injury, associated hip dislocations, nerve injuries, other associated injuries, the nature of treatment, and complications were recorded.
All data concerning treatment and post-treatment complications were recorded in a computer database for subsequent analysis. Fractures are classified according to Letournel [1] classification by senior surgeons using AP and Judet radiographs in addition to CT scan.
For statistical analysis, categorical and continuous data were expressed in percentage, mean, and range and were correlated using percentages and graphical comparisons. Descriptive statistics were used to summarize the demographic, classification, treatment methods, and complications. All statistical analyses were performed using the statistical packages SPSS 22.0 (SPSS Inc. Chicago, IL) and Epi Info TM 2000 (Centers for Disease Control and Prevention, Atlanta, GA).
Results
Incidence over time
Over the years 2008 to 2010, our orthopaedic unit treated 6046 patients with different types of fractures. Of these, 103 cases had sustained an acetabular fracture comprising about 1.7% of all types of fractures. There was no change in the overall incidence of these fractures over the three year period. Based on the fact that our unit is the sole unit serving the local population of 1,699,435, the estimated annual incidence of acetabulum fractures in the local population was two patients/100,000/year (1.94 per 100,000 in 2008 (33 cases), 1.76 per 100,000 in 2009 (30 cases), and 2.35 per 100,000 in 2010 (40 cases) (Fig. 1)).

Acetabulum fracture cases presented at HMC per year
Trends in age and gender
The mean age of patients sustaining an acetabular fracture between 2008 and 2010 was 36 years (8–84 years). Patients were distributed according to the age into five groups as shown in Table 1. Thirty-five percent (36cases) were in the 20–29-year group, 24.3% (25 cases) in the 40–49-year group, and 22.3% (23 cases) in the 30–39-year group. 13.6% (14 cases) in 50 years and above, and only 4.9% (5 cases) were under 20 years of age. A decline in the incidence per age group was noticed as age increases. Most of the patients (35%) were in the third decade of life (20–29 years) at the time of injury.
During the study period, the male-to-female predominance was 93.2 to 6.8% with an increase over time in the incidence among men (Fig. 1).
Alteration in the mechanism of injury
The most common cause of injury was motor vehicle collisions (MVC) (49.5%) followed by falls from heights (FFH) (28.1%), pedestrians struck by vehicles (13.6%), fall of heavy objects (5.8%), and ATV injuries (3%). MVCs were more common in the younger age group (20–29 years) than those in other groups.
Furthermore, MVCs were the most common cause of injury in the isolated posterior wall (69.2%) and posterior column fractures (66.7%). Most patients with anterior wall fractures were pedestrians struck by vehicles (36.4%) followed by MVCs (27.3%). The majority of the anterior column and associated both column fractures were due to falling from heights followed by MVCs (Tables 2 and 3 and Fig. 2).

Mechanism of injury according to age group
Changes in the types of fracture
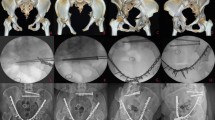
We used the Letournel system for classifying 87 displaced and undisplaced fractures. The remaining 16 fractures were not classified either because it cannot be classified using the Letournel system (isolated roof fracture) in five cases or because the original radiographs were not available. There were 64 (73.6%) primary acetabular fractures and 23 (26.4%) associated fractures (Figs. 3, 4, and 5).

Primary acetabular fractures. a Posterior wall. b Posterior column. c Anterior wall. d Anterior column. e Transverse

Associated acetabular fractures. a Posterior column and posterior wall. b Anterior column/wall and posterior hemi-transverse. c Transverse and post wall. d Both columns

Non-classified acetabular fracture involving the roof
The posterior wall fractures were the most common in 26 cases (25.2%) with a high incidence of the anterior column (18.4%) and anterior wall (10.7%) fractures while no change in the frequency of other subtypes of fracture was recorded over the study period (Table 4).
Other associated injuries
Over the 3-year period, associated hip dislocation occurred in 22 (21.3%) cases, 13 of which were with posterior wall fractures. Other injuries occurred in 64 (62.1%) cases, e.g., long bone fractures, chest, head, and abdominal injuries.
Treatment options
Patients with displaced fractures, instability, or incongruity of > 2 mm of the hip on plain radiographs and Judet views, unless contraindicated, were considered for treatment by internal fixation in 31 (30%) of cases. Non-operative treatment was considered for elderly patients, minimally displaced fractures, and both columns with secondary congruence in 72 (70%) of cases.
For surgically treated patients, the approach was Kocher-Langenbeck for posterior wall fractures and the ilio-inguinal or combined approach for both column fractures.
Out of the 31 operated patients, 14 cases are classified as primary fractures and 17 cases were associated fractures according to the Letournel system. Non-operative treatment was by using skin or skeletal traction depending upon the type of fracture. Full weight bearing started after an average of 12 weeks depending on the pattern of fracture and treatment. Twenty-four (23.3%) cases were lost to follow-up as they returned to their home countries or just did not come for the follow-up.
Mortality
There was no reported mortality directly related to acetabular fractures during the three year period in our unit which could be explained by the reduced number of severely traumatized patients over the study period. In addition, the patients with poly-trauma and haemodynamic instability are managed in our level I trauma centre.
Other outcomes
Sciatic nerve palsy was present at the time of injury in seven patients (7%). Lateral cutaneous nerve palsy was iatrogenic in one patient occurring in the early post-operative period. There was one late superficial wound infection that is treated with IV antibiotics.
Post-traumatic osteoarthritis occurred in five cases (4.8%). The low incidence of osteoarthritis in the early years may be due to the short period of follow-up and loss of follow-up in 24 (23.3%) cases.
Discussion
In this retrospective study, we analyzed data from a distinct population who attended the main trauma centre over a period of three years to study the epidemiology of acetabular fractures. The tremendous growth in the construction sector in the region during the past few years is causing an increment in complex orthopaedic injuries. Acetabular fractures are rare and complex injuries that require particular attention and surgical expertise for proper management [3, 6, 7, 16].
To our knowledge, there is no previous study on the epidemiology of the acetabular fracture in Qatar.
There was no significant difference in the incidence of acetabular fractures during the study period (2 per 100,000 per year compared to 3 per 100,000 per year in the UK) [2, 16].
Many previous studies reported that most acetabular fractures are caused by MVC [1, 2, 4, 5, 16]. Letournel [1] reported an increase in the number of acetabular fractures as the number of motor vehicles increased. Al-Qahtani and O’Connor [5] and Blum et al. [4] demonstrated the incidence and severity of acetabular fractures are reduced with the introduction of seat belts. Although, legislation of seat belt usage is strict, we found that MVC was still the most common cause of acetabular fractures in Qatar (49.5%) in comparison to rates of Laird and Keating [2] in 2005 (38.2%), Madhu et al. [6] in 2006 (76%), and 80% by Gianoudis [16]. It is followed by FFH (28.8%) which was also found to be the primary cause in the anterior column, both columns, and patients above 50 years of age. The fall from height might explain the higher incidence of anterior column fracture (18.4%) in our study compared to other literature [7], and therefore, requires special attention in the form of preventive measures to avoid such disastrous injuries. Moreover, as this study depicts that motor vehicle collisions are the most common mechanism for sustaining acetabular fractures, particularly posterior wall (69.2%) and posterior column (66.7%) fractures, it is necessary to make suitable arrangements and laws to enhance road traffic safety. It is also backed up by the finding that the majority of anterior wall fractures were due to a pedestrian struck by vehicles (36.4%) followed by MVCs (27.3%) and this might explain the higher incidence of the anterior wall fracture (10.7%) in this study compared to other literature [7].
In our study, the most common fracture pattern is posterior wall fracture (25.2%) which is comparable to 24% published in the literature [2, 3, 16, 17].
Our study showed that the majority of the patients belong to a younger age group with a mean age of 36 years, which correlates with the mean age of 38.6 ± 4.6 years in most of the literature [1, 6, 8, 9, 16,17,18].
There was a much lower proportion of women (6.8%) with these injuries in comparison to that found in literature [2, 14] which may be attributed to the fact that the majority of the workforce in Qatar is men, with a male:female ratio of 3:1 [16, 17].
The main aim of our study was not to evaluate outcome; however, our findings are not comparable to those published in the literature in term of complications and the development of osteoarthritis [6, 7, 16, 19]. The reported incidence of osteoarthritis is 26.6% [6, 7, 16]. In this study, we encountered only five cases (4.8%) of osteoarthritis. It is probably due to the short period of follow-up and the fact that 24 patients (23.3%) had lost to follow-up. However, all acetabular fractures at our centre were treated by the most senior experts in this field and this supports the view that providing surgeons trained in the management of acetabular fractures working in specialized centres is associated with better outcomes [2, 7, 16, 19].
Seven cases (7%) of post-traumatic sciatic nerve palsy was encountered in this study in comparison to 16.4% reported by Giannoudis and Madhu [6, 16]. No mortality cases were recorded over the study period.
Long-term complications, including post-traumatic arthritis and AVN, have not been observed in this study. It is due to several limitations, including a high rate of lost to follow-up which was attributed in many instances to patients relocating back to home countries after completion of their treatment. However, this retrospective review remains an epidemiological study, which can serve as a base for future prospective cohort studies.
Conclusion
Acetabular fractures are uncommon. The most common cause was motor vehicle collision. Posterior wall fracture was the most common fracture pattern. The incidence of post-traumatic sciatic nerve palsy and the proportion of women were lower than those reported in the literature. The reduction in the mortality rate may be attributed to improved road and vehicle safety measures. Well-trained surgeons and specialized centres for treating these injuries are recommended to achieve better outcomes.
References
Letournel E (1980) Acetabulum fractures: classification and management. Clin Orthop Relat Res 151:81–106
Laird A, Keating J (2005) Acetabular fractures: a 16-year prospective epidemiological study. J Bone Joint Surg, (Br) 87-B:969–973. https://doi.org/10.1302/0301-620X.87B7.16017
Moed BR, Carr SE, Watson JT (2000) Open reduction and internal fixation of posterior wall fractures of the acetabulum. Clin Orthop 377:57–67
Blum J, Beyermann K, Ritter G (1991) Incidence of acetabular fractures before and after the introduction of compulsory seat belt fastening. Unfallchirurgie 17:274–279 (in German)
Al-Qahtani S, O’Connor G (1996) Acetabular fractures before and after the introduction of seatbelt legislation. Can J Surg 39:317–320
Madhu R et al (2006) Outcome of surgery for reconstruction of fractures of the acetabulum—the time-dependent effect of delay. J Bone Joint Surg 86B:1197–1203. https://doi.org/10.1302/0301-620X.88B9.17588
Liebergall M, Mosheiff R, Low J et al (1999) Acetabular fractures: clinical outcome of surgical treatment. Clin Orthop 366:205–216
Mauffre C, Hao J et al (2014) The epidemiology and injury patterns of acetabular fractures are the USA and China comparable? Clin Orthop Relat Res 472:3332–3337. https://doi.org/10.1007/s11999-014-3462-8
Dias MV, Goldsztajn F et al (2015) The epidemiology of acetabulum fractures treated at Instituto Nacional De Traumatologia E Ortopedia. Rev Bras Ortop 45(5):474–477. https://doi.org/10.1016/S2255-4971(15)30438-9
McMaster J, Powell J (2005) Acetabular Fractures. Curr Orthop 19(2):140–154. https://doi.org/10.1016/j.cuor.2005.03.001
Matta JM, Merritt PO (1988) Displaced acetabular fractures. Clin Orthop Relat Res 230:83–97
Johnson EE, Matta JM, Mast JW, Letournel E (1994) Delayed reconstruction of acetabular fractures 21–120 days following injury. Clin Orthop Relat Res 305:20–30
Bozzio AE, Johnson CR, Mauffrey C (2016) Percutaneous management of acetabular fractures as an effective alternative to open reduction and internal fixation. Int Orthop 40:1703. https://doi.org/10.1007/s00264-015-2987-0
Qatar Statistics Authority. Qatar 2010 census of population, housing, and establishments. https://www.mdps.gov.qa/en/statistics/Statistical%20Releases/General/Census/Population_Households_Establishment_QSA_Census_AE_2010_1.pdf
Al-Thani H, El-Menyar A, Consunji R et al (2015) Epidemiology of occupational injuries by nationality in Qatar: evidence for focused occupational safety programmes. Injury 46:1806–1813. https://doi.org/10.1016/j.injury.2015.04.023
Giannoudis PV (2005) Operative treatment of displaced fractures of the acetabulum: a meta-analysis. J Bone Joint Surg Br 87(1):2–9. https://doi.org/10.1302/0301-620X.87B1.15605
Maia M, Santos D et al (2011) Epidemiological analysis of acetabulum. Rev Bras Ortop 46(1):23–26. https://doi.org/10.1590/S0102-36162011000100004
Kim JW, Herbert B, Hao J et al (2015) Acetabular fractures in elderly patients: a comparative study of low-energy versus high-energy injuries. Int Orthop 39:1175–1179. https://doi.org/10.1007/s00264-015-2711-0
Sen RK, Tripathy SK, Aggarwal S, Tamuk T (2011) Posterior wall reconstruction using iliac crest strut graft in severely comminuted posterior acetabular wall fracture. Int Orthop 35:1223–1228. https://doi.org/10.1007/s00264-010-1177-3
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Ahmed, M., Abuodeh, Y., Alhammoud, A. et al. Epidemiology of acetabular fractures in Qatar. International Orthopaedics (SICOT) 42, 2211–2217 (2018). https://doi.org/10.1007/s00264-018-3824-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-3824-z