
Abstract
ATP-binding cassette hetero-dimeric transporters G5 and G8 (ABCG5/G8) have been postulated to mediate intestinal cholesterol efflux, whereas Niemann-Pick C1 Like 1 (NPC1L1) protein is believed to be essential for intestinal cholesterol influx. The individual or combined genetic markers, such as single nuclear polymorphisms (SNPs), of these two transporter genes may explain inter-individual variations in plasma cholesterol response following plant sterol (PS) intervention. The present study was aimed at investigating the association between ABCG5/G8 and NPC1L1 genotype SNPs with sterol absorption and corresponding plasma concentrations. The study used a 4-week crossover design with 82 hypercholesterolemic men characterized by high vs. low basal plasma PS concentrations consuming spreads with or without 2 g/day of PS. For the ABCG8 1289 C > A (T400 K) polymorphism, the A allele carriers with high basal plasma PS concentrations demonstrated a 3.9-fold greater reduction (p < 0.05) in serum low density lipoprotein cholesterol (LDL-C) than their low basal plasma PS counterparts. For the NPC1L1 haplotype of 872 C > G (L272L) and 3929 G > A (Y1291Y), individuals carrying mutant alleles showed a 2.4-fold greater (p < 0.05) reduction in LDL-C levels, compared to wild type counterparts. Results suggest that genetic and metabolic biomarkers together may predict inter-individual lipid level responsiveness to PS-intervention, and thus could be useful in devising individualized cholesterol lowering strategies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Inter-individual responsiveness to dietary plant sterol (PS) intake varies greatly in human subjects in terms of plasma cholesterol lowering. For a given intervention, certain subjects show a marked response while others do not respond at all, even under controlled diet conditions [1–4]. An increasing body of evidence points to factors such as genetic polymorphisms of sterol transporter genes playing a role in influencing the individual responsiveness to PS intervention [5, 6].
ABCG5/G8 is made up of two half-transporter proteins that function together as a hetero-dimer [7, 8]. Investigation of sitosterolemia, a rare recessive disease caused by a genetic defect of ABCG5/G8, has shed light on the role of this transporter [9]. Current understanding of the role of ABCG5/G8 has been furthered as a result of studies on the tissue-specific expression of this transporter and the changes in circulatory cholesterol levels that occur after PS supplementation. Taken together, the normal function of ABCG5/G8 is suggested to limit intestinal uptake and promote biliary secretion of non-cholesterol sterols [10]. From a clinical perspective, common sequence variations such as single nuclear polymorphisms (SNPs) in ABCG5/G8 genes may have subtle effects on sterol metabolism. SNPs in ABCG5/G8 may also contribute to inter-individual variation in sterol absorption and circulatory concentrations of non-cholesterol sterols. Berge et al. observed that lower baseline PS concentrations were associated with two common sequence variations, 145 G > C (D19H) and 1289 C > A (T400 K) of the ABCG8 half-transporter gene [11]. Other researchers found that variations in T400 K may explain cross-sectional differences in plasma PS concentrations and determine the responsiveness for changes in plasma PS concentrations [12]. Further, variations in D19H may be associated with responsiveness to atorvastatin therapy [6]. In addition, these SNPs may also explain the inter-individual responsiveness to dietary PS [12] or cholesterol [3, 13] interventions in humans. Such findings implicate SNP variations in ABCG5/G8 as playing key roles in regulating circulatory sterol concentrations. It remains nevertheless unclear whether ABCG5/G8 polymorphisms could also affect sterol absorption and synthesis kinetics in response to PS intervention.
The NPC1L1 protein is a key modulator of cholesterol influx from micelles into intestinal mucosal cells [1, 4, 14]. Variations in the NPC1L1 gene have been shown to be associated with an improved LDL-C lowering effect [4], and may explain inter-individual variations in LDL-C level response to ezetimibe treatment [1, 15, 16]. Several rare genotype variations in NPC1L1 are associated with reductions in sterol absorption and circulatory LDL-C concentrations [1]. Some common SNPs in NPC1L1 such as 872 C > G (L272L) have shown to be associated with inter-individual variation in ezetimibe response [1, 16]. In terms of PS supplementation, however, human trials have yet to be performed to address whether NPC1L1 polymorphisms play a role in the cholesterol lowering responsiveness.
Moreover, no data are currently available to identify the combined effects of the ABCG5/G8 and NPC1L1 genotype SNP variations on changes in sterol absorption, cholesterol synthesis and plasma sterol concentrations in context of PS intervention. Subsequently, the aim of the present study was to investigate in 82 hypercholesterolemic men whether the SNP variations in ABCG5/G8 and NPC1L1 are individually or mutually associated with (1) basal absorption and circulatory concentrations of cholesterol and PS, (2) with changes in absorption and circulatory concentrations of cholesterol and PS after supplementation with 2 g/day of PS, and (3) with inter-individual variation in cholesterol lowering response to PS intervention.
Experimental Procedure
PS Enriched Diet Intervention and Blood Lipid Analyses
A randomized, crossover design was employed with two 4-week intervention phases, separated by a 4-week washout period in 82 hypercholesterolemic men characterized by high vs. low basal plasma PS concentrations. The experimental protocol was approved by the Ethics Committee of the Faculty of Medicine at McGill University. Details of volunteer recruitment, study diet, blood collection and analysis for testing serum concentrations of total cholesterol (TC), high density lipoprotein (HDL), LDL, triacylglycerol (TG) as well as plasma PS concentrations have been previously described by Houweling et al. [17].
Analyses of Sterol Absorption and Synthesis
On day 25, subjects were randomly designated to receive a single bolus of either 100 mg of D7-campesterol (n = 43) or D7-sitosterol (n = 39) within a 10 g aliquot of margarine in order to measure campesterol or sitosterol absorption. Simultaneously, 75 mg of 13C2-cholesterol was orally given to all subjects for measurement of cholesterol absorption. On day 28, subjects also received a 25 g oral dose of D2O (isotope purity > 99%), to measure cholesterol synthesis rate during the following 24-h period. All isotope chemicals were purchased from CDN Isotope, Pointe-Claire, Quebec, Canada.
The absorption indices of campesterol, sitosterol and cholesterol in the red blood cell (RBC) free sterol pool were assessed using a single stable isotope tracer method, which has been validated previously [18]. Total sterols were extracted and separated with the method as reported previously [19]. Free cholesterol 13C enrichments were measured by differential isotope ratio mass spectrometry (IRMS), using an automated dual-inlet system (SIRA 12; Isomass, Cheshire, UK). Free PS deuterium (D) enrichments were measured by differential IRMS, using a dual-inlet system (VG Isomass 903 D; Cheshire, England). The absorption indices of campesterol and sitosterol were expressed as the averaged D enrichments between 24–72 h over baseline (0 h), relative to standard mean ocean water, in the RBC free sterol pool. The absorption index of cholesterol was expressed as the averaged 13C enrichments between 24 and 96 h above the baseline level (0 h) in the RBC free sterol pool. Cholesterol fractional synthesis rate (FSR) was defined as the rate of incorporation of D from body water into RBC free cholesterol during the last 24 h of each treatment phase, and expressed as FSR in pools per day (pool per day) as previously described [19, 20].
Analyses of ABCG5/G8 and NPC1L1 Genotype SNPs
The ABCG5/G8 polymorphisms, 1950 G > C (Q604E), 145 G > C (D19H), 1289 C > A (T400 K) and 1572 (A632 V), as well as the NPC1L1 polymorphisms, 872 C > G (L272L) and 3929 G > A (Y1291Y), were screened from the published SNP data demonstrating an established functional significance for cholesterol modulation. DNA was extracted from 0.5 to 1.0 mL of plasma by QIAamp DNA Blood Mini Kit (Qiagen Inc, Canada). SNPs in ABCG5/G8 and NPC1L1 were determined using PCR-based TaqMan allele discrimination assays (Applied Biosystems, Foster City, CA, USA). The primers used for PCR have been described previously [6, 21–23]. A 7500 Real Time PCR thermal-cycler (Applied Biosystems, Foster City, CA, USA) was used for PCR analysis. Reactions were initially subjected to 92 °C for 10 min, and then 40 cycles, each of which was started at 95 °C for 15 s and 60 °C for 1 min for absolute quantification and then 60 °C for 1 min for allelic discrimination.
Statistical Analyses
Subjects were classified according to the criteria of (1) the screening sum of basal circulatory plasma PS concentrations (campesterol + sitosterol) into a high PS group (>50th percentile, n = 41) and a low PS group (<50th percentile, n = 41), or (2) responsiveness in serum lipid profiles to PS intervention into PS responders and non-responders. Subjects demonstrating a placebo adjusted reduction in both TC and LDL in response to PS intake were classified as responders; they were otherwise classified as non-responders. The SNP variations whose allele frequencies were abiding by the Hardy–Weinberg distribution equation were included in the statistical analysis. Prior to the analysis of diet–SNP interaction, the minor homozygous variants (mutant homozygote, n ≤ 4) were collapsed to the heterozygote group. Similarly, in analyzing the combined effect of two transporter genes, due to the limited number of participating subjects and the similarity in phenotypes in terms of cholesterol metabolism, NPC1L1 haplotypes with either or both heterozygous L272L and Y1921Y were combined into one heterozygous category. For serum TC, LDL-C, HDL-C and TG concentrations, data at baseline (day 1) and endpoint (day 29) of each phase were compared by performing analysis of covariance (ANCOVA) of proc mixed linear mode (SAS 9.1, Cary, NC, USA) to identify treatment effects and their interactions with high vs. low basal plasma PS concentrations and genotype variations. When treatment effect was identified as significant, Duncan’s post hoc tests were utilized at particular time points. The normality distribution was evaluated with Shapiro–Wilk test (p > 0.05). Unpaired one-tailed t-test or one-way ANOVA was employed between individuals with high and low basal plasma PS concentrations or among the different common polymorphisms within the same phase where appropriate. A two-way ANOVA was employed to examine the interaction of metabolic parameters with different common polymorphisms. The distribution patterns of two factors were analyzed by chi-square test followed by one-sided Fisher’s exact test. All data are expressed as mean ± standard error of the mean. The level of significance was established at α = 0.05, unless otherwise noted.
Results
Responders and Non-Responders to PS Intake
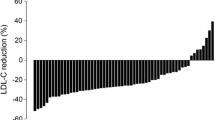
Eighty-two hypercholesterolemic men completed the crossover study with consumption of a placebo spread or a spread delivering 2 g/day of PS. Responders were those who showed a reduction (placebo adjusted) in both TC and LDL-C; otherwise they were classified as non-responders in that at least one of TC and LDL-C was not reduced. Responders (n = 51, 62%) and non-responders (n = 31, 38%) clearly manifested differing serum cholesterol responses to PS intervention for both TC (−12.7 ± 1.2% vs. 4.42 ± 1.2%, respectively, p < 0.0001) and LDL-C (−18.3 ± 2.0% vs. 9.41 ± 2.5%, respectively, p < 0.0001) (Table 1).
Absorption indices of campesterol, sitosterol and cholesterol did not differ among responders and non-responders (Table 2). In terms of cholesterol synthesis rate expressed as FSR, responders demonstrated a 20.7% lower FSR (4.68 ± 0.27% vs. 5.65 ± 0.43%, p < 0.05) in comparison to non-responders during the control phase. In the phase of PS intake, however, the difference in FSR values between responders and non-responders became very narrow (6.30 ± 0.37% vs. 6.64 ± 0.48%), because the responders achieved a greater percentage increase in FSR (38.5 ± 4.8% vs. 24.3 ± 5.9%, p < 0.05) than did non-responders.
Table 2 also indicates that subjects with low basal PS plasma concentrations were characterized as possessing low sterol absorption and high cholesterol FSR, a pattern that was reversed in subjects with high basal plasma PS concentrations. We also noticed a trend (p = 0.086, chi-square test, followed by Fisher’s exact test) of responders converging in the high basal PS group vs. non-responders in the low basal PS group. Among responders there were less individuals categorized with low basal PS (43% of total 51 responders) than identified with high basal PS concentrations. Inversely, in the group of non-responders, there were more individuals possessing low basal PS levels (61% of total 31 non-responders).
Relation of ABCG5/G8 Gene Polymorphism Variations with Responsiveness to PS Intake
The genotype frequencies of ABCG5/G8 common polymorphisms, T400 K, D19H and A632 V, were identified to abide with Hardy–Weinberg equilibrium [24]. As listed in Table 3, individuals with high and low basal plasma PS concentrations were almost equally distributed across the majority of the wild type homozygote SNP cohorts examined. However, in the heterozygote SNP cohorts, individuals with low basal PS out-numbered those with high basal PS concentrations. In terms of responsiveness to PS intervention, non-responders of heterozygous individuals were predominantly clustered within the low basal PS, but not within the high basal PS group. Most typically, for the ABCG8 T400 K polymorphisms, TT and TK/KK, individuals with high and low basal PS concentrations were differently distributed (p < 0.05). Among homozygote (TT) carriers, 61 and 39% were categorized as high and low basal PS individuals, respectively. Among heterozygote (TK/KK) carriers, this distribution was reversed to be 33 and 67% in individuals with high and low basal PS concentrations, respectively.
In view of the distribution of responders and non-responders among different ABCG8 T400 K polymorphisms, the numbers of responders and non-responders were not different (p = 0.38) among the high vs. low basal PS groups possessing TT polymorphism. However, for the TK/KK polymorphism, 10 of 11 non-responders were concentrated in the low basal PS group and only one non-responder was characterized as having a high basal PS concentration (p < 0.05; Fig. 1). This pattern was consistently reflected in cholesterol response to PS intake. Individuals carrying the TT genotype manifested a similar cholesterol response among the high vs. low basal PS groups (Fig. 2). In the individuals carrying TK/KK genotypes, those in the high basal PS group presented a 2.5-fold greater response in TC (−10.4 ± 2.3% vs. −3.0 ± 3.4%, p < 0.05) and a 3.9-fold greater response in LDL-C (−16.6 ± 6.3% vs. −3.4 ± 5.7%, p < 0.05) as compared with those in the low basal PS group.

Number of responders and non-responders with high and low basal plasma PS concentrations among different ABCG8 T400 K polymorphisms R responder, Non-R non-responder. For description of H_PS and L_PS groups, see Table 2. Subject distributions between basal PS levels (H_PS vs. L_PS) and responsiveness (R vs. Non-R) in different SNP variations (TT vs. TK/KK) were analyzed by Chi-square test, followed by one-side Fisher’s exact test (SAS 9.1). Significance of difference was set at * p < 0.05

Changes in plasma TC and LDL in response to PS intervention among subjects with different ABCG8 T400 K polymorphisms. Analysis of covariance with mix linear mode (SAS 9.1) was used to analyze the interaction of PS levels and SNP variation in response to PS intervention. Main treatment p < 0.0001, interaction of SNP and PS levels (H_PS vs. L_PS), p = 0.079 for TC and p = 0.016 for LDL. Significance of difference in %TC and %LDL (both placebo adjusted) was set at * p < 0.05
ABCG8 T400 K polymorphisms were also identified to be associated with variations in basal plasma PS concentration. With the T400 K polymorphism, TT carriers presented higher plasma concentrations of campesterol (12.2 ± 0.8 μmol/L vs. 9.7 ± 0.9 μmol/L, p < 0.05), sitosterol (6.5 ± 0.4 μmol/L vs. 5.1 ± 0.5 μmol/L, p < 0.05) and sum of campesterol and sitosterol (18.7 ± 1.2 μmol/L vs. 14.8 ± 1.4 μmol/L, p < 0.05), respectively, as compared with TK/KK carriers (Fig. 3).

Basal plasma PS concentrations among subjects with different ABCG8 T400 K polymorphisms. Unpaired t-test for differences among polymorphisms, significance of the difference was set at * p < 0.05
Relation of NPC1L1 Gene Polymorphism Variations with Cholesterol Responsiveness to PS Intake
Two sets of NPC1L1 common polymorphisms, L272L and Y1291Y, were identified to abide with Hardy–Weinberg equilibrium and thus further analyzed. Results show that these SNPs were not related to basal cholesterol concentrations, nor with PS or cholesterol absorption indices (data not shown). Moreover, the numbers of responders and non-responders possessing different SNP variations were not statistically different (Table 4). However, heterozygous carriers demonstrated a trend of an enhanced cholesterol lowering effect in response to PS intervention, as compared to homozygous counterparts. With L272L polymorphisms, the mutant G allele carriers (n = 37) showed a trend of a greater reduction in TC (−9.8 ± 2.0% vs. −4.1 ± 1.6%, p = 0.057) and LDL-C (−14.5 ± 3.3% vs. −4.4 ± 2.5% p = 0.082) in comparison with their wild type counterparts (C/C, n = 42). Similarly, for the Y1291Y polymorphism, carriers of the mutant A allele (n = 24) showed a trend toward a greater TC lowering effect (−9.4 ± 2.1% vs. −5.6 ± 1.6%, p = 0.073) compared with their wild type counterparts (n = 55).
In terms of haplotypes of L272L and Y1291Y, individuals with either heterozygous L272L or heterozygous Y1291Y manifested a similar trend (0.05 < p < 0.1, two-way ANOVA) of greater reductions in TC and LDL-C as compared to their homozygous counterparts (Table 4). Subsequently, all haplotypes with any heterozygous SNPs were merged into one heterozygote category. TC concentrations in these individuals were lowered 1.3-fold more (−9.3 ± 1.8% vs. −4.1 ± 1.7%, p < 0.05) than those of homozygous subjects. Similarly, LDL-C was reduced 2.4-fold more (−13.4 ± 3.0 vs. −3.9 ± 2.9, p < 0.05).
Interactions of ABCG8 and NPC1L1 Polymorphism Variations with Cholesterol Responsiveness to PS Intake
Since the functions of ABCG5/G8 and NPC1L1 transporters are counter-opposing, when the two genotype variations coexist in one subject, the contribution of an individual SNP variation to phenotype cannot be correctly appreciated unless background effects are adjusted. Subjects were hence categorized into four subgroups according to the heterozygosity of polymorphisms and phenotype characteristics: (1) Ho_Ho (ABCG8 T400T + NPC1L1 homozygote); (2) He_Ho (ABCG8 T400 K + NPC1L1 homozygote); (3) Ho_He (ABCG8 T400T + NPC1L1 heterozygote); (4) He_He (ABCG8 T400 K + NPC1L1 heterozygote) (Table 5).
These four subgroups showed an overall difference in PS induced alterations in plasma LDL-C concentration (p < 0.05, two-way ANOVA). It was further revealed that individuals with ABCG8 T400 K heterozygous genotypes against homozygous NPC1L1 background (He_Ho) were the most refractory cohort to PS intervention, exhibiting a minimal change in LDL-C. Indeed, LDL-C levels in these individuals were slightly increased (+1.6 ± 7.2%) as a result of PS intake. In contrast, individuals with NPC1L1 heterozygous genotypes against homozygous ABCG8 background (Ho_He) displayed the most pronounced LDL-C lowering effect (−13.6 ± 4.0%). The LDL-C response in these two subgroups presented a striking contrast (p < 0.05). A similar difference (p < 0.05) was also seen for TC. As He_Ho classified individuals demonstrated a limited reduction in TC (−1.9 ± 4.4%), whereas Ho_He individuals showed a more enhanced reduction in TC concentrations (−9.3 ± 2.5%).
Discussion
The present work represents the first investigation of the relationship between genotype polymorphism variations in two important sterol transporter genes, ABCG5/G8 and NPC1L1, and their response in cholesterol absorption and synthesis kinetics, as well as serum cholesterol concentrations, to dietary PS intervention. Results indicate that variations in both ABCG5/G8 and NPC1L1 polymorphisms have a profound effect on inter-individual responsiveness of cholesterol concentrations.
Inter-individual variation in PS-induced cholesterol response exists as a re-occurring problem encountered in clinical trials [1–4]. In this trial approximately one third of subjects (38%) were non-responders. It has been postulated that genetic predispositions could be attributable for response variations. ABCG5/G8 transporters have been suggested to limit sterol absorption by both pumping the sterol back to the intestinal lumen and promoting biliary secretion from the liver [9, 10]. The results of the current study with hypercholesterolemic men indicate that different SNP profiles of ABCG5/G8 are related to varying serum cholesterol response. Our results exemplify that homozygous carriers of ABCG8 T400 K polymorphisms are more likely to be responders, whereas carriers of heterozygous polymorphisms showed a trend to be classified as non-responders. ABCG8 T400 K was previously suggested by Plat et al. [12] to explain the inter-individual variation in PS metabolism in healthy volunteers after consumption of PS esters. These investigators observed that TT carriers possessed higher plasma campesterol and sitosterol concentrations in comparison to TK/KK carriers, a finding consistent with the results observed in the present study. In view of polymorphism distribution, it was further noticed that individuals with high basal plasma PS concentrations were more likely to possess the TT polymorphism, whereas individuals with low basal PS were predominantly carrying the TK/KK polymorphism. In terms of cholesterol response to PS intervention, our study further revealed that the varying cholesterol response among carriers with T400 K polymorphisms were likely associated with basal plasma PS concentrations. A poor responsiveness to PS intervention is associated with heterozygous polymorphism (TK/KK) of ABCG8 T400 K in addition to a low basal plasma PS concentration.
NPC1L1 is another important sterol transporter protein that plays a critical role in intestinal uptake of both PS and cholesterol [14, 24]. NPC1L1 protein is also the postulated target for ezetimibe intervention, by which cholesterol absorption is suppressed [2]. Previously, Hegele et al. observed that NPC1L1 haplotype variations were associated with inter-individual differences in plasma LDL-C response to ezetimibe [1]. However, whether NPC1L1 polymorphism variations also explain the suppression in cholesterol absorption and plasma concentration as a result of PS intake remains unclear. The present study reveals the trends indicating that polymorphisms in NPC1L1 L272L and Y1291Y augment the extent of PS-induced cholesterol lowering in comparison to wild type counterparts. There is an understanding that under certain circumstances, haplotypes may be a useful way to reduce the complexity of the candidate-gene association analyses [25], which is consistent with our findings that haplotypes of two SNP L272L and Y1291Y mutant alleles elicited a similar response to PS intervention. Obviously, our results are consistent with NPC1L1 being closely involved in inter-individual variation in response to PS intervention, as it has been observed with ezetimibe therapy [1].
Another novel finding of the present study is the description of the combined effect of ABCG8 and NPC1L1 transporter genotype variations on the response to PS intervention. Kajinami et al. suggested that combined analysis of different polymorphisms is more informative than single locus analysis for defining the responsiveness of a patient to statin therapy [6]. These authors found that polymorphisms in ABCG8 and CYP7A1, both of which are functionally significant in the secretion of cholesterol from the liver into bile, interact in an allele-cumulative manner in atorvastatin-treated subjects. However, in the present study, the combined actions of ABCG8 T400 K and NPC1L1 haplotypes of L272L/Y1291Y seem more complex than simply being cumulative; the phenotype expression of each individual polymorphism may interfere with the concurrence of two counteracting transporter gene polymorphisms. To more specifically expose the characteristics of target SNP variations, we singled out target SNP variants and pooled in common wild type background polymorphisms to more specifically portray the characteristics of target SNP variations.
Very recently, a case–control study by Rudkowska et al. [26] also tested the same sets of SNPs in ABCG5/G8 and NPC1L1 among 26 hyperlipidemic subjects after PS intervention, but small sample size in their study design made the results ineligible for statistical analysis. In extending of Rudkowska et al.’s [26] work, our trial recruited more subjects, and plasma lipid response was analyzed in context of background adjusted SNPs of ABCG8 and NPC1L1. Subsequently, the results of the present trial managed to unravel that heterozygous ABCG8 T400 K genotypes attenuate the cholesterol lowering response, while heterozygous haplotypes of NPC1L1 L272L/Y1291Y enhance cholesterol lowering response to PS, in comparison with their respective wild type homozygous counterparts.
Limitations of this study include the fact that SNPs represent the most frequent form of polymorphism in the human genome [24]. According to the National Center for Biotechnology Information database, so far, 280 of ABCG5/G8 and 70 of NPC1L1 common polymorphism variations have been identified in the human genome. This study involves less than ten common polymorphism candidates that have known or predicted functional consequences with sterol metabolism based on previous studies [1, 4, 12, 13, 15]. Whether these individual or combined common polymorphisms are adequate to fully explain inter-individual variations of sterol metabolism cannot be fully identified from previous [1, 4, 12, 13, 15] and the present studies.
In conclusion, this study examined the role of ABCG5/G8 and NPC1L1 transporter gene common polymorphisms in explaining inter-individual responsiveness to PS intervention in the context of their impact on cholesterol absorption and synthesis. In the ABCG8 T400 K polymorphism, heterozygous carriers with low basal plasma PS concentrations showed a minimal cholesterol reduction as compared to homozygote carriers. In contrast, among NPC1L1 L272L/Y1291Y haplotypes, heterozygous carriers manifested a maximal cholesterol reduction as compared to homozygote carriers. Such a pattern was more obviously demonstrated after background SNP adjustment. Results suggest that common polymorphisms of sterol transporter genes, together with basal circulating plasma PS concentrations, are indicative of the expected cholesterol lowering effect induced by dietary PS intake.
References
Hegele RA, Guy J, Ban MR, Wang J (2005) NPC1L1 haplotype is associated with inter-individual variation in plasma low-density lipoprotein response to ezetimibe. Lipids Health Dis 4:16
Wang J, Williams CM, Hegele RA (2005) Compound heterozygosity for two non-synonymous polymorphisms in NPC1L1 in a non-responder to ezetimibe. Clin Genet 67:175–177
Herron KL, McGrane MM, Waters D, Lofgren IE, Clark RM, Ordovas JM, Fernandez ML (2006) The ABCG5 polymorphism contributes to individual responses to dietary cholesterol and carotenoids in eggs. J Nutr 136:1161–1165
Cohen JC, Pertsemlidis A, Fahmi S, Esmail S, Vega GL, Grundy SM, Hobbs HH (2006) Multiple rare variants in NPC1L1 associated with reduced sterol absorption and plasma low-density lipoprotein levels. Proc Natl Acad Sci USA 103:1810–1815
Sehayek E, Nath C, Heinemann T, McGee M, Seidman CE, Samuel P, Breslow JL (1998) U-shape relationship between change in dietary cholesterol absorption and plasma lipoprotein responsiveness and evidence for extreme interindividual variation in dietary cholesterol absorption in humans. J Lipid Res 39:2415–2422
Kajinami K, Brousseau ME, Nartsupha C, Ordovas JM, Schaefer EJ (2004) ATP binding cassette transporter G5 and G8 genotypes and plasma lipoprotein levels before and after treatment with atorvastatin. J Lipid Res 45:653–656
Gylling H, Hallikainen M, Pihlajamaki J, Agren J, Laakso M, Rajaratnam RA, Rauramaa R, Miettinen TA (2004) Polymorphisms in the ABCG5 and ABCG8 genes associate with cholesterol absorption and insulin sensitivity. J Lipid Res 45:1660–1665
Field FJ, Born E, Mathur SN (2004) Stanol esters decrease plasma cholesterol independently of intestinal ABC sterol transporters and Niemann-Pick C1-Like 1 protein gene expression. J Lipid Res 45:2252–2259
Bhattacharyya AK, Connor WE (1974) Beta-sitosterolemia and xanthomatosis. A newly described lipid storage disease in two sisters. J Clin Invest 53:1033–1043
Klett EL, Patel S (2003) Genetic defenses against noncholesterol sterols. Curr Opin Lipidol 14:341–345
Berge KE, von Bergmann K, Lutjohann D, Guerra R, Grundy SM, Hobbs HH, Cohen JC (2002) Heritability of plasma noncholesterol sterols and relationship to DNA sequence polymorphism in ABCG5 and ABCG8. J Lipid Res 43:486–494
Plat J, Bragt MC, Mensink RP (2005) Common sequence variations in ABCG8 are related to plant sterol metabolism in healthy volunteers. J Lipid Res 46:68–75
Weggemans RM, Zock PL, Tai ES, Ordovas JM, Molhuizen HO, Katan MB (2002) ATP binding cassette G5 C1950G polymorphism may affect blood cholesterol concentrations in humans. Clin Genet 62:226–229
Davis HR Jr, Zhu LJ, Hoos LM, Tetzloff G, Maguire M, Liu J, Yao X, Iyer SP, Lam MH, Lund EG et al (2004) Niemann-Pick C1 Like 1 (NPC1L1) is the intestinal phytosterol and cholesterol transporter and a key modulator of whole-body cholesterol homeostasis. J Biol Chem 279:33586–33592
Simon JS, Karnoub MC, Devlin DJ, Arreaza MG, Qiu P, Monks SA, Severino ME, Deutsch P, Palmisano J, Sachs AB et al (2005) Sequence variation in NPC1L1 and association with improved LDL-cholesterol lowering in response to ezetimibe treatment. Genomics 86:648–656
Temel RE, Tang W, Ma Y, Rudel LL, Willingham MC, Ioannou YA, Davies JP, Nilsson LM, Yu L (2007) Hepatic Niemann-Pick C1-Like 1 regulates biliary cholesterol concentration and is a target of ezetimibe. J Clin Invest 117:1968–1978
Houweling AH, Vanstone CA, Trautwein EA, Duchateau GSMJE, Jones PJH (2007) Baseline plasma plant sterol concentrations do not predict changes in serum lipids, C-reactive protein (CRP) and plasma plant sterols following intake of a plant sterol-enriched food. Eur J Clin Nutr. Epub ahead of print. doi:10.1038/sj.ejcn.1602969
Wang Y, Vanstone CA, Parsons WD, Jones PJ (2004) Validation of a single-isotope-labeled cholesterol tracer approach for measuring human cholesterol absorption. Lipids 39:87–91
Jones PJ, Raeini-Sarjaz M, Ntanios FY, Vanstone CA, Feng JY, Parsons WE (2000) Modulation of plasma lipid levels and cholesterol kinetics by phytosterol versus phytostanol esters. J Lipid Res 41:697–705
Jeske DJ, Dietschy JM (1980) Regulation of rates of cholesterol synthesis in vivo in the liver and carcass of the rat measured using [3H]water. J Lipid Res 21:364–376
McGuigan FE, Ralston SH (2002) Single nucleotide polymorphism detection: allelic discrimination using TaqMan. Psychiatr Genet 12:133–136
McGuigan F, Salmon K (2005) Pre-event discussion and recall of a novel event: how are children best prepared? J Exp Child Psychol 91:342–366
Hubacek JA, Berge KE, Cohen JC, Hobbs HH (2001) Mutations in ATP-cassette binding proteins G5 (ABCG5) and G8 (ABCG8) causing sitosterolemia. Hum Mutat 18:359–360
Altmann SW, Davis HR Jr, Zhu LJ, Yao X, Hoos LM, Tetzloff G, Iyer SP, Maguire M, Golovko A, Zeng M et al (2004) Niemann-Pick C1 Like 1 protein is critical for intestinal cholesterol absorption. Science 303:1201–1204
Carlson CS, Eberle MA, Rieder MJ, Yi Q, Kruglyak L, Nickerson DA (2004) Selecting a maximally informative set of single-nucleotide polymorphisms for association analyses using linkage disequilibrium. Am J Hum Genet 74:106–120
Rudkowska I, Abumweis SS, Nicole C, Jones PJ (2008) Association between non-responsiveness to plant sterol intervention and polymorphisms in cholesterol metabolism genes: a case-control study. Appl Physiol Nutr Metab 33(4):728–734
Acknowledgments
This project was supported by grants from Unilever R&D, Vlaardingen, the Netherlands, and by the Canadian Institutes of Health Research—Provincial Partnership Program. The authors thank Brian Sithoo for his technical support in SNP analysis and Iwona Rudkowska for her comments on discussion.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Zhao, H.L., Houweling, A.H., Vanstone, C.A. et al. Genetic Variation in ABC G5/G8 and NPC1L1 Impact Cholesterol Response to Plant Sterols in Hypercholesterolemic Men. Lipids 43, 1155–1164 (2008). https://doi.org/10.1007/s11745-008-3241-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11745-008-3241-y