
Abstract
The use of robotic surgery for colorectal cancer continues to increase. However, not all organizations offer patients the option of robotic intervention. This study seeks to understand organizational characteristics associated with the utilization of robotic surgery for colorectal cancer. We conducted a retrospective study of hospitals identified in the United States, State of Florida Inpatient Discharge Dataset, and linked data for those hospitals with the American Hospital Association Survey, Area Health Resource File and the Health Community Health Assessment Resource Tool Set. The study population included all robotic surgeries for colorectal cancer patients in 159 hospitals from 2013 to 2015. Logistic regressions identifying organizational, community, and combined community and organizational variables were utilized to determine associations. Results indicate that neither hospital competition nor disease burden in the community was associated with increased odds of robotic surgery use. However, per capita income (OR 1.07 95% CI 1.02, 1.12), average total margin (OR 1.01, 95% CI 1.001, 1.02) and large-sized hospitals compared to small hospitals (OR: 5.26, 95% CI 1.13, 24.44) were associated with increased odds of robotic use. This study found that market conditions within the U.S. State of Florida are not primary drivers of hospital use of robotic surgery. The ability for the population to pay for such services, and the hospital resources available to absorb the expense of purchasing the required equipment, appear to be more influential.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
An increasing trend in the use of minimally invasive surgery (MIS) has been observed in the United States since the early 1990s [1]. There are two modalities for conducting MIS, the first is advanced robotic systems, and the second is non-robotic or laparoscopic surgery. Non-robotic MIS has been supported through numerous academic studies and is a common expectation from patients seeking care [2]. The benefits associated with the use of laparoscopic surgical procedures have been well established [3,4,5]. Studies such as the Clinical Outcomes of Surgical Therapy study COST trial [6]. Colorectal Cancer Laparoscopic or Open Resection (COLOR) trial [7], COLOR II trial [8], Comparison of Open versus laparoscopic surgery for mid or low REctal cancer After Neo-adjuvant chemoradiotherapy (COREAN) trial [9], and Conventional versus Laparoscopic-Assisted Surgery in Colorectal Cancer (CLASICC) trial [10] demonstrated that laparoscopic surgical procedures have resulted in improved short-term benefits for colon and rectal cancer when compared to open surgical approach. However, there is inconclusive evidence-based research in support of the use of robotic surgery as superior to other forms of MIS in colorectal cancer care [11]. Some studies have shown that the use of robotics systems may be advantageous compared to laparoscopic approaches in terms of shorter length of stay (LOS) and a lower rate of conversion to open [12,13,14,15,16,17]. However, patient demands for robotic surgery [18], as well as improvements in organizational response to providing the care needed by a community has resulted in increased diffusion of robotic surgery use in colorectal cancer care [19, 20].
Use of robotic surgery
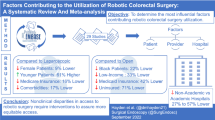
Not all patients have equal access to facilities that offer this surgical option [19, 20]. Multiple factors influence the use of robotic surgery in clinical settings, which may be patient-, provider- or hospital-related. Based on previous studies, patient-related characteristics such as metastatic cancer, presence of comorbidities, Medicaid insurance, race, and rural residence is associated with a decreased utilization of robotic surgery for colorectal cancer treatment [19]. There are patient-level regional differences such as racial disparities that have shown to impact the use of robotic surgery for colorectal cancer [19].
Hospital- and community-related factors
However, these studies have not accounted for the modulating effect of factors external to the patient, such as hospital- and community-related factors. For example, patients are unlikely to have the equal access to robotic technologies as the equipment may not be available at treating facilities or communities because of the prohibitive cost, and possibly, lack of training of the surgeons employed at said facility [21, 22]. For hospitals, its community includes the populations the hospital serves, other organizations, as well as the regulatory and political environments. For example, colorectal cancer professional societies have promoted greater use of minimally invasive surgery (MIS) such as robotic surgery to improve the quality of care as well as the speed of recovery for colorectal and other forms of cancer patients [23]. Thus, hospitals have increased their use of robotic surgeries over the past decade [1, 19].
Additionally, particularly in the U.S., hospitals are continuously seeking opportunities to achieve competitive advantage or reduce perceived advantages other hospitals in the same market hold [24]. As the market becomes more saturated with hospitals providing like services, there is an increased need to encourage preferred customers to seek services at their locations. This encourages behaviors or structures to be adopted that are preferential to patients [24]. Since surgical encounters are often profitable for hospitals, advanced surgical technologies are likely prime targets for organizations seeking to achieve competitive advantages over other hospitals in the market. More specifically, more competitive markets are likely more active in their attempts to obtain a competitive advantage by offering services the other hospitals are not and/or reduce the perceived competitive advantage other hospitals within the market hold through offering similar services [24]. As such, this study seeks to define the organizational and community characteristics that promote hospital usage of robotic surgical options for colorectal cancer patients.
Methods
Data source
This study utilized the U.S. State of Florida Inpatient Discharge Dataset (FIOD), American Hospital Association (AHA), Medicare Hospital Cost Report, Area Health Resource File (AHRF), and the Florida Health Community Health Assessment Resource Tool Set (CHARTS) data for the years 2013–2015, see Table 1. All inpatient hospital discharges throughout the state of Florida are reported in the FIOD [25]. The Medicare Hospital Cost Report contains information hospitals report to the Center for Medicare and Medicaid Services concerning facility utilization, as well as financial and cost information [26]. Hospital characteristics were also collected from the AHA Annual survey, which includes data points concerning hospital type, size, and services offered [27]. The AHRF includes data concerning healthcare facilities, providers, and population descriptors linked to U.S. county and state locations [28]. Finally, the CHARTS data are population health data collected and distributed by the Florida Department of Health, Division of Public Health Statistics and Performance Management which include data concerning hospitalizations, births, deaths, reportable disease and behavioral risk factors for the State of Florida [29].
Population
This study focused on defining which hospitals in the U.S. State of Florida provide robotic surgeries associated with a colorectal cancer diagnosis. As such, we utilized the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9CM) codes defining diagnosis of colorectal cancer, and surgical interventions associated with colorectal cancer to identify (1) the hospitals providing these services, and (2) the types of procedures provided (open, endoscopic, robotic). Hospitals that did not have patients who were diagnosed with colorectal cancer and did not provide related surgical procedures were excluded from this study.
Dependent variable
The dependent variable for this study was the provision of robotic surgery at the hospital. If any patient received a robotic surgery for the treatment of colorectal cancer during the 3 years of the study, the hospital in which they received the surgery was identified as offering robotic surgery. If only endoscopic or open techniques were used during this time period, the hospital was classified as not offering robotic surgery.
Independent variables
Hospital variables were merged with the FIOD using the Centers for Medicare and Medicaid Services provider identification codes. In the U.S., hospitals are identified by their structural characteristics. Therefore, hospital-level characteristics included in the study were hospital ownership designations, hospital size, teaching status, Medicare and Medicaid rates Elixhauser comorbidity score, average operating margin, and average total margin. Hospital ownership, size, teaching, and Medicare and Medicaid rate were defined through the AHA dataset. Hospital ownership identifies if ownership is by the non-federal (state or local) government or is operated by a for-profit or not-for-profit group. Hospital size is defined by the identified by the number of beds operated by the facility (small < 99 beds, medium < 300 beds, large > 299 beds). Teaching status indicates whether or not the hospital provides medical education and training. Medicare and Medicaid rates define the percentage of discharges paid by the Centers for Medicare and Medicaid Services and are operationalized by the number of discharges that are Medicare and Medicaid, respectively, divided by the total number of discharges at the hospital. These variables indicate the payer mix (more governmental pay vs. commercial pay) of the hospitals providing colorectal cancer surgery. The average comorbidity score for the hospital is derived from the FIOD data utilizing the Elixhauser Comorbidity index associated with the patients who received colorectal cancer surgery during the 3 years of the study. The average number of comorbidities associated with colorectal cancer patients undergoing surgery at each hospital was calculated and utilized to help adjust for disease severity. Next, total operating margin, total margin, and teaching status were collected from the CMS Cost Report data. These variables provide insight into the financial health and mission of the organization.
Health Services Areas (HSA) were utilized to define the service area of the hospitals in the dataset. Health Service Areas (HSAs) are defined as local health markets that consist of a single or cluster of contiguous counties where most of the residents receive care and hospitalization from the hospitals in that area. There is a total of 3246 HSAs in the U.S. and 114 in the State of Florida. Population demographics were aggregated to the HSA-level to identify characteristics that may influence a hospital’s choice in using robotic equipment for colorectal cancer surgery. The following characteristics were considered: per capita income, number of individuals within the area with a 4-year college education, percentage of the population white, percent black, percent Hispanic, number uninsured, number of colorectal cancer deaths (2013–2015), the Herfindal-Hershman Index (HHI) of the HSA as well as the population size within the HSA. Per capita income, the number with a 4-year college education, the percentage of the population that are white, black or Hispanic, the number uninsured, and population size were collected from the AHRF. The number of colorectal cancer deaths within the HSA was obtained from the CHARTS data. Finally, the HHI, which is a measure of market concentration, identifies how competitive the HSA is with regard to the number of hospitals and their market share in the area. This information was obtained using overall inpatient discharges from each of the hospitals within the dataset. This information was then used to calculate the market share of each hospital (accounting for system hospitals) held within the HSA. The average market competition is defined by the ratio of hospitals total inpatient days divided by the HSA’s total inpatient days. The resulting index is a continuous variable ranging from 0 to 1, whereby 0 is indicative of a competitive market and 1 of a monopolistic market.
Statistical analysis
Means and percentages were utilized to describe the study population. Kruskal–Wallis and Pearson χ2 were used to assess continuous and categorical variables, respectively. Univariate logistic regression was used to determine associations between the hospital and HSA characteristics and the use of robotic surgery. Next, three multivariable logistic models were utilized. The first model only contained hospital-level variables, and the second contained only community variables at the HSA level. In both cases, variables that were not identified as statistically significantly associated with the use of robotic procedures within the univariate model were excluded using the principles outlined by Raudenbush and colleagues [30]. For the final combined model, only variables that were significantly associated with robotic surgery from the hospital or HSA models were included. Relevant fit indices were judged by the criteria from Boedeker [31]. Indices used were AIC, Schwartz Criterion, and likelihood ratio tests [32, 33]. All tests of significance were two-sided, and odds ratios, 95% Confidence Intervals, and p values were reported. The level of statistical significance was set at p value < 0.05. Analyses were performed using SAS version 9.4 (SAS Institute Inc.).
Results
In all, there are 159 hospitals included in the analysis; 71 did not provide robotic surgery, while 88 did (see Table 2). Small hospitals and medium hospitals had a lower frequency of offering robotic surgery (20–40%, respectively), while larger hospitals had a greater frequency of offering robotic surgery (63%). Teaching hospitals (77%), and hospitals with a greater average total margin between 2013 and 2015 (55%), also had a larger frequency of offering robotic surgery. However, hospitals seeing patients with a greater median Elixhauser comorbidity score had a lower frequency of offering robotic surgery (2.8 vs. 2.5 for non-robotic and robotic, respectively). Hospitals located in HSAs with greater median per capita income (38.4 vs. 40.7), greater 4-year education (77,242 vs. 176,251), greater percent black (11.3 vs. 17), greater number of uninsured (65,922 vs. 133,024), larger population size per 100,000 (6.8 vs. 18.7) and in areas of greater hospital competition (HHI: 0.7 vs. 0.3) more frequently offered robotic surgery.
Considering the univariate analysis (Table 3), large compared to small hospitals demonstrated a 6.82 increase in odds of offering robotic surgery (95% CI 1.82–25.49); however, there was no difference when considering small vs. medium-sized organizations. Hospitals identified as teaching hospitals had a 4.10 increase in the odds of offering robotic surgery (95% CI 1.94–8.67). Similarly, hospitals with a greater 3-year average total margin had increased odds of providing robotic surgery (OR: 1.01, 95% CI 1.002–1.02). However, hospitals with a greater Medicaid rate (OR: 0.95, 95% CI 0.93–0.98) or those which saw patients with a greater number of comorbidities (OR: 0.29, 95% CI 0.15–0.58) had reduced odds of offering robotic surgery. HSA characteristics associated with increased odds of offering robotic surgery include the percent of the population that identified as black in the HSA (OR: 1.07, 95% CI 1.02–1.12), 4-year education (OR 1.03, 95% CI 1.01–1.05) and per capita income (OR 1.08, 95% CI 1.03–1.13). However, there were also several HSA characteristics associated with decreased odds of offering robotic surgery. These include: a larger percent of the HSA, which identifies as white (OR 0.95, 95% CI 0.92–0.99) and HHI, which indicates less competition is associated with a reduced odd of offering robotic surgery (OR 0.43, 95% CI 0.20–0.93).
The multivariable analysis assessed only the variables that were significant from the univariate model (see Table 4). In the hospital level analysis, large hospitals compared to small hospitals (OR: 6.24, 95% CI 1.40–27.82), and hospitals with a greater 3-year average total margin (OR 1.01, 95% CI 1.00–1.02) had increased odds of offering robotic surgery. However, hospitals with a greater Elixhauser comorbidity score had reduced odds of offering robotic surgery (OR 0.31, 95% CI 0.14–0.68). When considering the model only reviewing HSA level factors, per capita income was positively associated with increased odds of providing robotic surgery (OR 1.09, 95% CI 1.04–1.15). Finally, the combined Hospital and HSA level model demonstrated that when adjusting for the other variables, large hospitals had increased odds of 5.26 (95% CI 1.13–24.44) for offering robotic surgery compared to small hospitals. In addition, both average total margin (OR 1.01, 95% CI 1.001–1.02) and per capita income in the HSA (OR 1.07, 95% CI 1.02–1.12) were associated with increases in the odds of offering robotic surgery holding all else equal. On the other hand, hospitals with a greater Medicare discharge rate (OR 0.96, 95% CI 0.92–0.99) or with a greater comorbidity score as identified by the Elixhauser score (OR 0.32, 95% CI 0.14–0.69) were associated with a decreased odd of providing robotic surgery holding all else equal.
Discussion
Colorectal cancer is one of the leading causes of cancer in the United States [34]. Surgery remains the most important component in treating colorectal cancer, and MIS is considered the gold standard of surgical care in colorectal cancer [35]. While initially robotic surgery was used most commonly by urologists, the advent of the XI DaVinci robot, with multi-quadrant surgery capability, increased its utilization, and now it is commonly used by colorectal surgeons trained in its use. As such, robotic surgery is the latest advancement within MIS, and has definite advantages when used in the correct setting by trained surgeons; however, there are definite barriers to its utilization. Here we demonstrate that those barriers are formed by complex interactions between the characteristics of the hospitals, as well as the community attributes in which the organization resides.
Although we found that hospital organizational and hospital service area factors to be associated with the use of robotic surgery, our analysis suggests that hospital market competition and the number of mortalities associated with colorectal cancer in the larger population are not key drivers in the decision for hospitals to provide robotic surgery. In our combined model, the main drivers indicating organizational use of robotic surgery for colorectal cancer include hospital size, Elixhauser comorbidity index, Medicare discharge rate, average total margin, and HSA per capita income.
Previous studies have highlighted the strong relationship between hospital competition and diffusion of innovation [36, 37]. Wright et al.’s 2016 study did find an association between the use of robotic surgery and regional hospital competition. They found that across five commonly performed procedures, patients seeking treatment at hospitals in a competitive region were 2–5 times more likely to receive a robotic-assisted surgery. Indicating that regional competition (northeast, Midwest, south, and west) has a greater influence on a hospital’s decision to procure a surgical robot [37]. However, this and similar studies have been conducted on different types of surgeries, and none have been conducted specifically on colorectal cancer robotic surgery. Hospital competition research has also shown that competitive markets have led to an increase in health care costs and with strong policy forces incentivizing against cost increases. As such, hospitals are more likely to explore cost-effective alternatives to robotic-assisted surgery, which may explain the difference in findings for the current study [38].
Second, we found that mortality rate and patient comorbidities, measured by the Elixhauser comorbidity index, are not drivers for hospital adoption of robotic platforms. Based on these findings, hospitals may not consider these technologies to provide additional benefit, perceive robotic surgery to improve organizations’ competitive advantage or consider these components when determining whether to offer robotic surgery. However, previous research provides some indication for considering both when deciding whether to offer robotic surgery. For example, previous studies found that patient mortality increased as comorbidities and age increased [39], and comorbidities along with age were key factors that influenced physicians’ decision on treatment procedure selected [40]. Another study of colorectal cancer patients found that postoperative morbidity was significantly decreased through the use of minimally invasive surgery (MIS), and the lowest morbidity was associated with the use of robotic surgery [41]. However, there are inconsistent results on the long-term and short-term outcomes of the use of robotic surgery [42, 43]. The costs associated with the use of a robotic platform to assist in surgery, such as the Da Vinci robotic system, range from $3000 to $6000 more than traditional MIS, such as laparoscopic surgery [35]. One study found that the use of robotic surgery adds approximately $3500 per procedure and over $2.5 billion annually to the national health expenditure with a lack of evidence of improved patient outcomes compared to laparoscopic methods [44].
Third, an examination of the health insurance market has shown that insurers are less likely to reimburse robotic surgery at a higher rate than laparoscopic approaches [40]. The dual effect of the increased cost of the procedure and lack of sufficient reimbursement may explain our findings indicating the lack of association of competition and robotic surgery and the positive association found between increased availability of hospitals performing robotic surgery and income per capita. Similarly, the associated total margin and increased odds of using robotic surgery also point to a potential increase in profit through the usage of the robotic equipment. However, it may be more likely that larger hospitals, in areas that have a better payor mix and that have a better total margin, can afford the expensive equipment.
Limitations
Several factors limit the current study. We have used secondary data and multiple data sources to identify organizational characteristics associated with the use of robotic surgery. We are limited to evaluating associations and cannot more definitively articulate causation. We are also limited to evaluating hospital use of robotic surgery and cannot examine the impact of the adoption of advanced robotic systems. The study is also potentially at risk due to biases associated with self-report, as in the AHA survey, misclassification or data entry errors associated with claims data, and a lack of more granular organization and community factors. Additionally, the focus on organizations in the State of Florida also potentially reduces generalizability due to the populations, policies, organizational competition, and legislative realities present in the State. Similarly, there are instances where limited numbers in certain categorical variables provide reduced accuracy in our analysis, as can be seen by wide confidence intervals.
However, despite these limitations, the current study provides an important assessment of factors that influence organizational behaviors focused on the provision of advanced care techniques. Our methodological approach has utilized data sources that are well established, and our analytical approach has sought to reduce bias through careful operationalization of variables used in previous research. Additionally, previous work has utilized these datasets as well as datasets derived from those used here [45]. Furthermore, we have utilized the entire population of inpatient hospitals providing surgical colorectal cancer care as defined by discharge data over 3 years. This analysis represents a robust State-level assessment of hospital and community characteristics influencing the provision of these services. Although the primary data source is from the United States, similar trends can be expected in any healthcare system where unequal access to care exists, be it from a patient, institution, or health care system perspective.
Conclusion
In conclusion, this study finds that market conditions are not primary drivers of hospital use of robotic surgery. What likely drives utilization of robotic surgery is the ability for the patients to pay for such services, and the hospital resources available to absorb the capital expense of purchasing the required equipment. Future research should seek further exploration of geographic variation in the use of this technology.
References
Tsui C, Klein R, Garabrant M (2013) Minimally invasive surgery: national trends in adoption and future directions for hospital strategy. Surg Endosc 27(7):2253–2257
Narain AS et al (2018) Patient perceptions of minimally invasive versus open spine surgery. Clinical Spine Surg 31(3):E184–E192
Abu Gazala M, Wexner SD (2017) Re-appraisal and consideration of minimally invasive surgery in colorectal cancer. Gastroenterol Rep 5(1):1–10
Hollis RH et al (2016) Understanding the value of both laparoscopic and robotic approaches compared to the open approach in colorectal surgery. J Laparoendosc Adv Surg Tech 26(11):850–856
Moghadamyeghaneh Z et al (2016) Comparison of open, laparoscopic, and robotic approaches for total abdominal colectomy. Surg Endosc 30(7):2792–2798
Group, C.O.o.S.T.S (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. New Engl J Med 350(20):2050–2059
Group, C.C.L.o.O.R.S (2005) Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol 6(7):477–484
van der Pas MH et al (2013) Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol 14(3):210–218
Jeong S-Y et al (2014) Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol 15(7):767–774
Green B et al (2013) Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer. Br J Surg 100(1):75–82
Schootman M et al (2016) Adoption of robotic technology for treating colorectal cancer. Dis Colon Rectum 59(11):1011–1018
Al-Temimi MH et al (2019) Robotic versus laparoscopic elective colectomy for left side diverticulitis: a propensity score-matched analysis of the NSQIP database. Int J Colorectal Dis 34(8):1385–1392
Hopkins MB et al (2019) Comparing pathologic outcomes for robotic versus laparoscopic surgery in rectal cancer resection: a propensity adjusted analysis of 7616 patients. Surg Endosc 34(6):2613–2622. https://doi.org/10.1007/s00464-019-07032-1
Li L et al (2019) Robotic versus laparoscopic rectal surgery for rectal cancer: a meta-analysis of 7 randomized controlled trials. Surg Innov 26(4):497–504. https://doi.org/10.1177/1553350619839853
Liao G et al (2019) Comparison of pathological outcomes between robotic rectal cancer surgery and laparoscopic rectal cancer surgery: a meta-analysis based on seven randomized controlled trials. Int J Med Robot 15(5):e2027. https://doi.org/10.1002/rcs.2027
Milone M et al (2019) Completeness of total mesorectum excision of laparoscopic versus robotic surgery: a review with a meta-analysis. Int J Colorectal Dis 34(6):983–991
Phan K et al (2019) Laparoscopic vs. robotic rectal cancer surgery and the effect on conversion rates: a meta-analysis of randomized controlled trials and propensity-score-matched studies. Tech Coloproctol 23(3):221–230
Iacopino V, Mascia D, Cicchetti A (2018) Professional networks and the alignment of individual perceptions about medical innovation. Health Care Manage Rev 43(2):92–103
Osayande O et al (2019) Trends in the use of laparoscopy and robotics for colorectal cancer in Florida. J Laparoendosc Adv Surg Tech 29(7):926–933
Osagiede O et al (2018) Disparities in minimally invasive surgery for colorectal cancer in Florida. Am J Surg 218(2):293–301. https://doi.org/10.1016/j.amjsurg.2018.11.019
Chen R et al (2019) A comprehensive review of robotic surgery curriculum and training for residents, fellows, and postgraduate surgical education. Surg Endosc 34(1):361–367. https://doi.org/10.1007/s00464-019-06775-1
Beane M (2019) Shadow learning: building robotic surgical skill when approved means fail. Adm Sci Q 64(1):87–123
Carmichael JC et al (2017) Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American society of colon and rectal surgeons and society of American gastrointestinal and endoscopic surgeons. Dis Colon Rectum 60(8):761–784
Agwunobi A, Osborne P (2016) Dynamic capabilities and healthcare: a framework for enhancing the competitive advantage of hospitals. California Manag Rev 58(4):141–161
Administration, A.f.H.C. Florida health finder. 2020 [cited 2020 March 14]; Available from: https://www.floridahealthfinder.gov/index.html
CMS. Cost reports. 2020 [cited 2020 March 14]; Available from: https://www.cms.gov/Research-Statistics-Data-and-Systems/Downloadable-Public-Use-Files/Cost-Reports
AHA (2020) The go-to destination for reliable and consistent data about the nation’s hospitals. https://www.ahadata.com/why-aha-data. Accessed 18 Feb 2020
Resources, H.a.H (2020) Area health resources file. https://data.hrsa.gov/topics/health-workforce/ahrf. Accessed 20 Feb 2020
CHARTS. FLHealthCHARTS.com: getting started. FLHealthCHARTS 2019 [cited 2020; Available from: https://www.flhealthcharts.com/Charts/documents/training/CHARTSGettingStarted_Sep2019.pdf
Raudenbush SW, Bryk AS (2020) Hierarchical linear models: applications and data analysis methods, vol 1. Sage Publications, Thousand Oaks, CA
Boedeker P (2017) Hierarchical linear modeling with maximum likelihood, restricted maximum likelihood, and fully Bayesian estimation. Prac Assess Res Eval 22(1):2
Hamadi H et al (2019) medicare’hospital-acquired condition reduction program and community diversity in the united states: the need to account for racial and ethnic segregation. Hosp Top 97(4):148–155
Spaulding A et al (2019) A community health case for psychiatric care: a cross-sectional study of county health rankings. Gen Hosp Psychiatry 57:1–6
Cronin KA et al (2018) Annual report to the nation on the status of cancer, part I: national cancer statistics. Cancer 124(13):2785–2800
Cheng CL, Rezac C (2018) The role of robotics in colorectal surgery. BMJ 360:j5304. https://doi.org/10.1136/bmj.j5304
Dor A et al (2012) Pricing of surgeries for colon cancer: patient severity and market factors. Cancer 118(23):5741–5748
Wright JD et al (2016) Effect of regional hospital competition and hospital financial status on the use of robotic-assisted surgery. JAMA Surg 151(7):612–620
Melnick GA, Fonkych K (2016) Hospital prices increase in California, especially among hospitals in the largest multi-hospital systems. INQUIRY J Health Care Org Prov Finan 53:0046958016651555
Van Eeghen EE et al (2015) Impact of age and comorbidity on survival in colorectal cancer. J Gastrointest Oncol 6(6):605–612
Wilensky GR (2016) Robotic surgery: an example of when newer is not always better but clearly more expensive. Milbank Quart 94(1):43–46
Addae JK et al (2017) A comparison of trends in operative approach and postoperative outcomes for colorectal cancer surgery. J Surg Res 208:111–120
Batool F et al (2018) A Regional and national database comparison of colorectal outcomes. JSLS J Soc Laparoendosc Surg 22:4
Tam MS et al (2016) A population-based study comparing laparoscopic and robotic outcomes in colorectal surgery. Surg Endosc 30(2):455–463
Shukla PJ, Scherr DS, Milsom JW (2010) Robot-assisted surgery and health care costs. N Engl J Med 363(22):2174
Whyte JL et al (2015) An evaluation of algorithms for identifying metastatic breast, lung, or colorectal cancer in administrative claims data. Med Care 53(7):e49–e57
Funding
This work was supported by the Robert D. and Patricia E. Kern Center for Science of Health Care Delivery. The funder had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The authors have no other financial relationships.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Spaulding, Dr. Hamadi, Dr. Osagiede, Dr. Lemini, Mr Cochuyt, Mr. Watson, Dr. Naessens and Dr. Colibaseanu declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Spaulding, A.C., Hamadi, H., Osagiede, O. et al. Hospital robotic use for colorectal cancer care. J Robotic Surg 15, 561–569 (2021). https://doi.org/10.1007/s11701-020-01142-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-020-01142-y