
Abstract
Sustained interest and an increase of possible indications endorse the role of robot-assisted surgery of the head and neck region. However, broad clinical application is impeded by substantial extra cost, time exposure and a supposed deficit of haptic and tactile feedback. The role of haptic feedback has barely been examined in this context, and literature provides only limited objective validation. This point of criticism applies to all commercially available systems. We created an experimental setup to evaluate, quantify and compare the performance of surgical systems. The daVinci system (Intuitive Surgical), the Flex system (Medrobotics) and standard rigid instruments (23 cm laryngoscopic grasper, Karl Storz) were compared with the human hand by head and neck surgeons (n = 15), performing a variety of surgical tasks. Specific samples with different rigidity were sorted with all devices, and the resulting orders were analyzed by permutation analysis, indicating differences in precision and accuracy of haptic and tactile feedback. The human hand was superior in all trials, acting as reference modality. The flexible instruments of the Flex system performed better than the electro-mechanically decoupled instruments of the daVinci system for the majority of measures recorded, suggesting a benefit in terms of haptic and tactile feedback in this context. While not all aspects of haptic and tactile feedback were accessible, this first objective comparison endorses the inferiority of robot-assisted surgery in terms of haptic and tactile feedback, compared to the human sense or standard surgical tools. Furthermore, the immediate force transmission of the Flex system seems to be superior to the electro-mechanical transformation of the daVinci system, indicating an advantage in terms of haptic and tactile feedback in immediate comparison. This study is providing a basis for further experiments and the development of robotic surgery towards an implementation in clinical routine.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite major developments over the past 15 years and increased implementation of transoral robot-assisted surgery (TORS) in the head and neck area, these innovative techniques still fail to supersede traditional access via rigid endoscopy, transoral laser microsurgery and the open transcervical approach as standard surgical procedures of this specific region [1]. Various limitations prevent broad application and acceptance in clinical routine. These include: (I) substantial extra cost, which is currently not covered by the Diagnosis Related Groups (DRG) pricing system in Germany as well as in several other European countries [2], (II) considerable additional time exposure due to set-up time and extended general effort and furthermore (III) a presumed deficiency of haptic and tactile feedback, preventing higher acceptance especially among professionals [3]. These limitations apply to all established and commercially available robot-assisted surgical systems. Currently, the daVinci system (Intuitive Surgical Inc., Sunnyvale, USA) and the Flex system (Medrobotics Corp., Raynham, USA) are approved for head and neck surgery in Europe and North America [4, 5]. Both systems have been extensively described in previous publications [6,7,8]. While tactile feedback is defined as the passive sensibility, e.g., perceived by the receptors of the human hand, haptic feedback emerges from active exploration. Referring to surgical work, these two aspects are perceived as an inseparable, subjective and highly individual cognition of the human senses, and are not easy to approach in terms of conducting a sophisticated investigation. Though, the aspects of haptic and tactile feedback undoubtedly affect surgical work, and different tools, transferring the surgeon´s actions to the patient, have different characteristics in terms of haptic and tactile feedback. Lederman and Klatzky defined the perception of haptic as a combination of the following procedures to explore objects: lateral motion (sweeping over a surface), pressure, enclosure and contour following [9]. Another considerable aspect is the visual feedback, transferred through the visible deformation of an object or, for example, the depth of an incision, effecting from a defined applied force [10]. In summary, absolute quantification of this multimodal sensory impression is not possible. Until today, the literature offers limited objective validation on this topic for the head and neck region. While we find several technical surveys, e.g., comparing specific robotic tools [11], the available robot-assisted surgical systems have never been compared in terms of haptic and tactile feedback in a quantifiable experimental setup. Thus, in our primary approach, we aimed at investigating the two basic modalities of all surgical techniques, pressure and extension. Assessment and reproducibility of these forces were compared in terms of haptic and tactile feedback in a quantifiable and simple experimental setup using two recently discussed robot-assisted surgical systems, the daVinci System and the Flex System. In addition, tasks were performed by hand and with standard laryngoscopic instruments as reference modalities.
Materials and methods
Experimental setup
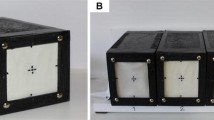
Assessment and reproducibility of pressure and extension were examined separately. To assess for pressure, six custom build silicone cushions with defined rigidity (Silicones ShA 0 with 1.06 g/cm3 density, ShA 13 with 1.07 g/cm3, ShA 33 with 1.10 g/cm3 in different ratio) were positioned by the study participants according to the rigidity from soft to hard by touching samples with the respective surgical device. Silicone samples were visually identical (Fig. 1a). To assess for extension, five steel tension springs with defined rigidity (0.1–2.8 N/mm) were put in order according to degree of rigidity from soft to hard (Fig. 1b). Springs were built into optically identical black boxes (Fig. 2). In both experiments, samples have been approached from above at an angle of 90°. A total of 15 study participants, all head and neck residents or consultants, performed both experiments using these modalities: (I) by hand, without any tool, as the assumed tactile reference, (II) employing a standard rigid laryngoscopic grasper for transoral surgery (23 cm, Karl Storz, Tuttlingen, Germany), (III) using a suitable rigid Maryland grasper of the daVinci system and (IV) by means of a suitable flexible fenestrated grasper of the Flex system (Fig. 3a, b).

a Custom built silicone cushions and b tension spring boxes to evaluate haptic and tactile feedback of robot-assisted surgical systems for head and neck surgery

Evaluation of haptic and tactile feedback of the daVinci system (Intuitive Surgical Inc.). The surgical system is tested using a standardized investigation procedure

a Setup of the Medrobotics Flex system, a computer-assisted flexible endoscope. b The endoscope tip features a 2D-HD camera and compatible flexible instruments are forwarded through accessory working channels. Cordially provided by Medrobotics Corporation
Analysis
To exclude learning effects, the initial order of samples and the order of modalities applied were randomized for every participant. Visual feedback via immediate eye contact or the visualization screen of the robotic systems was not disabled. The respective result order was recorded for each participant and evaluated by permutation analysis. Four key measures were recorded: (I) absolute success of the set task as a binary feature (yes/no), (II) highest number of samples arranged in the correct order (in series), (III) maximum number of samples put on the correct place number, independent from the order (accuracy), (IV) largest number of samples positioned on incorrect place number, independent from the order (mistakes). Standard statistical measures were compared and significance was validated using the Chi Square, Fisher-Exact and Kruskal–Wallis tests. Calculations were performed by a certified statistician using the ‘R’-software (open source software, www.r-project.org).
Results
The assessment of haptic and tactile feedback in transoral robot-assisted surgery was feasible with all tested surgical tools in the presented setup. The robot-assisted surgical tools showed no system failure. All samples were appropriate and showed no relevant wear marks during the investigation. Table 1 displays the numeric results of the permutation analysis in a simplified depiction. The results of the human hand were superior in all trials. Therefore, the human hand applies as reference modality in this study. As described above, depending on the respective key measure, we found significant differences between the competitive systems. In detail, the absolute discharge of the set task was successfully performed by significantly more participants with the Flex instruments, compared to the daVinci system for the evaluation of extension. For the assessment of pressure, no significant differences were found for this specific measure. Concerning the maximum number of samples in a correct order, the comparison of medians indicates a significant benefit for the daVinci system in the assessment of extension, while differences in the pressure attempt are even and not statistically significant. Looking at the correct placement of samples, once more the Flex systems shows advantages in accuracy for the assessment of pressure with a significantly higher median, while results for the assessment of extension are equivalent between the systems for this particular measure. Finally, analyzing the number of incorrectly placed samples, with a higher mistake rate in median, more participants failed for the set task using the daVinci system, especially exercising pressure to the samples in this experiment. Again, Fisher-Exact and Chi Square proved significance of these findings, except for the absolute result and the maximum order for the evaluation of pressure (Figs. 4, 5).

Result presentation (binary feature) of haptic and tactile feedback of robot- assisted systems for transoral surgery compared to standard instruments and the human hand in terms of absolute success of the set task for evaluation of (a) extension and (b) pressure (yes = successfully completed; no = not successfully completed)

Result presentation (dotplot) of haptic and tactile feedback of robot- assisted systems for transoral surgery compared to standard instruments and the human hand in terms of the maximum number of samples placed in correct order for evaluation of (a) extension and (b) pressure. The maximum number of samples put on the correct place number, independent from the order, for evaluation of (c) extension and (d) pressure. The largest number of samples positioned on incorrect place number, independent from the order, for evaluation of (e) extension and (f) pressure. Each point represents the result of one participant, black lines enable a comparison of the respective medians
In conclusion, the flexible instruments of the Flex system performed better than the rigid and electro-mechanically decoupled instruments of the daVinci system for the majority of measures, suggesting a benefit in terms of haptic and tactile feedback in this context. Standard rigid instruments showed similar results to the human hand for most measures and consequently were superior to both of the robot-assisted systems.
Discussion
The initial idea of surgical robots is to facilitate highly challenging interventions and to compensate, where human capabilities are inevitably restricted, for example by suppressing the surgeon´s tremor in cochlear implantation [12]. However, since the introduction of robot-assisted surgery in terms of automated or semi-automated systems, it is generally assumed, that in terms of haptic and tactile feedback, these innovative systems are inferior to the surgeon´s hand with its natural properties of human sense [13]. Although there are various definitions of haptic and tactile feedback in literature, the terms are mostly considered a measure of the controllability and reproducibility of the forces applied, especially when used in a clinical context. While the daVinci system meets the actual definition of a medical robot with a real master–slave principle, the Flex system is rather a computer-assisted endoscope with mechanical instruments [14]. Therefore, the impression of haptic and tactile feedback is transferred electromechanically for the daVinci system, and mechanically without conversion for the Flex system. Undoubtedly, this leads to major differences in the transmission of haptic and tactical feedback. However, since the array of possible indications and the value in clinical application of both systems are very similar, an objective comparison seems useful. A number of research teams as well as manufacturers themselves have attempted to equip robot-assisted surgical systems with special sensors to record and analyze forces and torques applied, e.g. for the daVinci system [15, 16]. However, to date, very few of the attempts facilitate clinical use in a significant way. Additional scales and other information interfer with the visualization of the surgical site, decrease the surgeon´s concentration and are barely intuitive. The use of surgical tools is necessarily accompanied by a loss of haptic and surgical control, which is confirmed by the results of our study. In the presented setup, the human hand was at all times superior to the standard rigid surgical tools or the robot-assisted operating systems used. Of considerable interest in particular are the differences between the competing robot-assisted surgical systems. Here, the Flex system seems to benefit from immediate force transmission via the flexible tools. Transmission of movements and forces is only reduced by insignificant deformation of the instrument. In comparison, for the daVinci system, the controller and the effector tool are decoupled by electro-mechanical transformation of movements and forces, resulting in a decreased haptic and tactile feedback. Even respecting the system differences in terms of construction and function, this can lead to a disadvantage in clinical use. A major limitation of the presented study is the role of optical feedback, which is not analyzed in the presented setup. The established robot-assisted surgical systems are mostly based on an image-guided construction with 2D-HD or 3D visualization [17]. To allow the execution of the experiments in this setup, visual feedback could not be disabled. Therefore, the role of optical feedback could not be sufficiently examined in the current setup and the differentiation between the effects of optical and tactical feedback needs further definition.
Conclusion
The aspects of haptic and tactile feedback in robot-assisted surgery remain controversial. Our study acknowledges the inferiority of robot-assisted surgery in terms of haptic and tactile feedback compared to the human sense or standard surgical tools. Furthermore, this first objective comparison of commercially available systems ascertains an advantage of the Flex system over the daVinci system. Future projects should evaluate the role of haptics and tactile feedback in terms of a more complex coverage and closer to clinical application. Especially the role of optical feedback is not adequately defined in the current setup and has to be further evaluated.
References
Friedrich DT, Scheithauer MO, Greve J, Hoffmann TK, Schuler PJ (2016) Recent advances in robot-assisted head and neck surgery. Int J Med Robot Comput Assist Surg MRCAS doi:10.1002/rcs.1744
Dombree M, Crott R, Lawson G, Janne P, Castiaux A, Krug B (2014) Cost comparison of open approach, transoral laser microsurgery and transoral robotic surgery for partial and total laryngectomies. Eur Arch Otorhinolaryngol 271(10):2825–2834. doi:10.1007/s00405-014-3056-9
Enayati N, De Momi E, Ferrigno G (2016) Haptics in robot-assisted surgery: challenges and benefits. IEEE Rev Biomed Eng 9:49–65. doi:10.1109/RBME.2016.2538080
Genden EM, Desai S, Sung CK (2009) Transoral robotic surgery for the management of head and neck cancer: a preliminary experience. Head Neck 31(3):283–289. doi:10.1002/hed.20972
Schuler PJ, Duvvuri U, Friedrich DT, Rotter N, Scheithauer MO, Hoffmann TK (2015) First use of a computer-assisted operator-controlled flexible endoscope for transoral surgery. The Laryngoscope 125(3):645–648. doi:10.1002/lary.24957
Friedrich DT, Scheithauer MO, Greve J, Duvvuri U, Sommer F, Hoffmann TK, Schuler PJ (2015) Potential advantages of a single-port, operator-controlled flexible endoscope system for transoral surgery of the larynx. Ann Otol Rhinol Laryngol. doi:10.1177/0003489415575548
Schuler PJ, Hoffmann TK, Veit JA, Rotter N, Friedrich DT, Greve J, Scheithauer MO (2016) Hybrid procedure for total laryngectomy with a flexible robot-assisted surgical system. Int J Med Robot Comput Assist Surg MRCAS doi:10.1002/rcs.1749
O’Malley BW Jr, Weinstein GS, Hockstein NG (2006) Transoral robotic surgery (TORS): glottic microsurgery in a canine model. J Voice 20(2):263–268. doi:10.1016/j.jvoice.2005.10.004
Lederman SJ, Klatzky RL (1993) Extracting object properties through haptic exploration. Acta Psychol (Amst) 84(1):29–40
Reiley CE, Akinbiyi T, Burschka D, Chang DC, Okamura AM, Yuh DD (2008) Effects of visual force feedback on robot-assisted surgical task performance. J Thorac Cardiovasc Surg 135(1):196–202. doi:10.1016/j.jtcvs.2007.08.043
Hoffmann TK, Schuler PJ, Bankfalvi A, Greve J, Heusgen L, Lang S, Mattheis S (2014) Comparative analysis of resection tools suited for transoral robot-assisted surgery. Eur Arch Otorhinolaryngol 271(5):1207–1213. doi:10.1007/s00405-013-2615-9
Liu WP, Azizian M, Sorger J, Taylor RH, Reilly BK, Cleary K, Preciado D (2014) Cadaveric feasibility study of da Vinci Si-assisted cochlear implant with augmented visual navigation for otologic surgery. JAMA Otolaryngol Head Neck Surg 140(3):208–214. doi:10.1001/jamaoto.2013.6443
Okamura AM (2009) Haptic feedback in robot-assisted minimally invasive surgery. Curr Opin Urol 19(1):102–107. doi:10.1097/MOU.0b013e32831a478c
Schuler PJ, Hoffmann TK, Duvvuri U, Rotter N, Greve J, Scheithauer MO (2016) Demonstration of nasopharyngeal surgery with a single port operator-controlled flexible endoscope system. Head Neck 38(3):370–374. doi:10.1002/hed.23910
Tavakoli M, Patel RV, Moallem M (2005) Haptic interaction in robot-assisted endoscopic surgery: a sensorized end-effector. Int J Med Robot Comput Assist Surg MRCAS 1(2):53–63. doi:10.1002/rcs.16
Liu C, Moreira P, Zemiti N, Poignet P (2011) 3D force control for robotic-assisted beating heart surgery based on viscoelastic tissue model. Conf Proc Ann Int Conf IEEE Eng Med Biol Soc IEEE Eng Med Biol Soc Conf 2011:7054–7058. doi:10.1109/IEMBS.2011.6091783
Byrn JC, Schluender S, Divino CM, Conrad J, Gurland B, Shlasko E, Szold A (2007) Three-dimensional imaging improves surgical performance for both novice and experienced operators using the da Vinci Robot System. Am J Surg 193(4):519–522. doi:10.1016/j.amjsurg.2006.06.042
Author information
Authors and Affiliations
Contributions
DTF, PJS and JG designed the study, executed the experiments and wrote the manuscript. LD, SH and FS designed and manufactured samples and ensured technical realization. JH edited data and figures, BM developed and performed the statistical analysis. TKH executed experiments, edited and corrected the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
DTF, TKH, PJS and JG have published on the Flex system (Medrobotics) before. These took part as investigators in the clinical study evaluating the Flex system without receiving financial compensation. A fee was payed to Medrobotics per case. DTF, PJS and TKH have received travel expenses for cadaver labs with the Flex system. For these authors, there is no additional financial commitment or dependent relationship. LD, BM, SH, FS and JH declare, that they have no conflict of interest. Permission was obtained from the respective manufacturers for publication of all figures.
Rights and permissions
About this article

Cite this article
Friedrich, D.T., Dürselen, L., Mayer, B. et al. Features of haptic and tactile feedback in TORS-a comparison of available surgical systems. J Robotic Surg 12, 103–108 (2018). https://doi.org/10.1007/s11701-017-0702-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-017-0702-4