
Abstract
Robot-assisted surgery for colon cancer has been reported in many studies, most of which worked on right and/or sigmoid colectomy. The aim of this study was to report our experience of robotic transverse colectomy with an intracorporeal anastomosis, provide details of the surgical technique, and present the theoretical benefits of the procedure. This is a retrospective review of prospectively collected data of robotic surgery for colorectal cancer performed by a single surgeon between May 2007 and February 2011. Out of 162 consecutive cases, we identified three robotic transverse colectomies, using a hand-sewn intracorporeal anastomosis. Two males and one female underwent transverse colectomies for malignant or premalignant disease. The mean docking time, time spent using the robot, and total operative time were 5, 268, and 307 min, respectively. There were no conversions to open or conventional laparoscopic technique. The mean length of specimen and number of lymph nodes retrieved were 14.1 cm and 6.7, respectively. One patient suffered from a wound seroma and recovered with conservative management. The mean hospital stay was 8.7 days. After a median follow-up of 72 months, there were no local or systemic recurrences. Robotic transverse colectomy seems to be a safe and feasible technique. It may minimize the necessity of mobilizing both colonic flexures, with facilitated intracorporeal hand-sewn anastomosis. However, further prospective studies with a larger number of patients are required to draw firm conclusions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The introduction of laparoscopic techniques has contributed greatly to the improvement of short-term outcomes after surgery. However, several technical limitations have also been noted for the laparoscopic approach, including poor ergonomics, limited range of motion, lack of three-dimensional visualization, and tremor. These limitations led to the emergence of robotic systems, which were expected to overcome the pitfalls of conventional laparoscopic techniques. Since robot-assisted colectomy using the da Vinci® Surgical System (Intuitive Surgical Inc., Sunnyvale, CA) was first reported in 2002 [1], it has been used increasingly in colorectal surgery, and a number of studies have demonstrated the safety and feasibility of robotic colorectal procedures including right and left/sigmoid colectomies [2–4]. However, few reports of robotic transverse colectomy exist, and the results of its use for lesions in transverse colon remain largely unreported.
The aim of this study was to report our experience of robotic transverse colectomy with an intracorporeal anastomosis, provide details of the surgical technique, and present the theoretical benefits of the procedure.
Methods
Patients
This is a retrospective review of prospectively collected data on the robotic colorectal resections performed using the da Vinci® S Surgical System (Intuitive Surgical Inc.) by a single surgeon between May 2007 and February 2011. Out of 162 consecutive cases, three transverse colectomies with a hand-sewn intracorporeal anastomosis were identified. The patients’ demographics, operative details, histopathologic results, and postoperative outcomes were reviewed.
Surgical technique
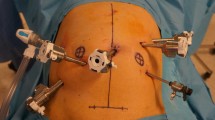
Figure 1 shows the operating room configuration and port placement for a robotic transverse colectomy. The procedure was carried out with a full robotic technique. A 12-mm trocar for the camera was placed just below the umbilicus. Three 8-mm trocars for the robotic arms were placed on the right anterior axillary line, the right midclavicular line, and the left midclavicular line at the umbilical level, respectively. Another 12-mm trocar was placed in the left lower quadrant for the assistant. The robotic surgical cart was docked from the cephalic side of the patient.

a Operating room configuration and b port placement for a robotic transverse colectomy. C 12-mm port for camera; A 12-mm port for assistant; R1, R2, R3 8 mm trocars for first, second, and third robotic arms
We used a 30-degree stereoscopic telescope, an ultrasonic energy instrument, or monopolar scissors in the first robotic arm, a fenestrated Maryland bipolar forceps in the second arm, and Cadiere forceps in the third arm. The lesion was localized with preoperative tattooing (Fig. 2a) or intraoperative laparoscopic ultrasonography (Fig. 2b). Laparoscopic ultrasonography was performed by a radiologist before the surgical cart was docked to detect the tumor itself or clips which were applied during preoperative colonoscopy. After identifying the lesion, the procedure began with detachment of the greater omentum from the transverse colon using an ultrasonic energy device. The transverse mesocolon was then lifted and spread with the third arm and an atraumatic grasper through the assistant port. The middle colic vessels were identified by its pulsation and contour at the root of the mesentery. The peritoneal layer of the mesentery was incised at the level of the origin of the middle colic vessels, and meticulous dissection around the vessels, including accurate lymphadenectomy, was conducted (Fig. 3a). The middle colic artery and vein were isolated and ligated with 5-mm clips that were introduced through the assistant port (Fig. 3b). The transverse mesocolon was divided from the root of the middle colic vessels to the border of the transverse colonic wall. With sufficient proximal and distal margins, the transverse colon was divided using two endolinear cutting staplers. The specimen was covered with an endoscopic vinyl bag and placed beside the liver during the anastomosis. The anastomoses were performed intracorporeally in all cases. After placing three tagging sutures on the antimesenteric border, the mesenteric border, and their midpoint, the stapled lines on both cutting edges were removed. A single-layer end-to-end anastomosis was fashioned, using full-thickness interrupted sutures of 3-0 polyglactin (Fig. 4). The specimen was retrieved at the end of the procedure through a small extension of the camera port site.

Localization of tumor: a preoperative tattooing and b intraoperative laparoscopic ultrasonography

Dissection and ligation of the middle colic vessels: a meticulous dissection around the vessels, including accurate lymphadenectomy and b ligation with 5-mm clips

A single-layer end-to-end anastomosis using full-thickness interrupted suture of 3-0 polyglactin
Results
During the study period, two males and one female underwent transverse colectomies for malignant or premalignant disease. The patients’ demographics and operative details are summarized in Table 1. The age of the patients was 57, 68 and, 54 years, respectively, and the BMI was 26.4, 22.7, and 29.2 kg/m2. All of the tumors were located in the middle third segment of the transverse colon on the abdomino-pelvic computed tomography. The premalignant lesion failed to be removed by colonoscopic intervention before surgery. The clinical stage of both malignant lesions was T2N0M0, according to the American Joint Committee on Cancer TNM staging system. The docking time defined as the time for docking the four robotic arms onto the trocars was 5 min in all cases. The time spent using the robot was 350, 190, and 265 min for each patient. The total operative time was 408, 307, and 297 min. There were no intraoperative complications and no conversions to conventional laparoscopic technique.
Table 2 shows the histopathologic and postoperative outcomes of the patients. The final histopathologic reports revealed that patient 1 and 3 had adenocarcinoma of pT3N0 and pT2N0, respectively. Patient 2 had 4.0 cm-sized tubular adenoma with high-grade dysplasia. The proximal resection margin was 3.0, 6.5, and 3.5 cm and the distal resection margin was 10.0, 5.5, and 2.5 cm, respectively. The number of lymph nodes retrieved was 6, 8, and 6 in each patient. Patient 3 developed a wound seroma and recovered with conservative management. All patients were discharged within 9 days. After a median follow-up of 72 months, there were no local or systemic recurrences.
Discussion
Laparoscopic colorectal resection has proven to be safe and effective based on several large randomized trials and has been accepted as an alternative method to the traditional open procedure for the past two decades [5, 6]. However, the majority of studies on laparoscopic colectomy have excluded patients with transverse colon or colonic splenic flexure lesions because of technical complexities [7–9]. Although there have been several studies, including a meta-analysis which demonstrated that laparoscopic resection of transverse colon tumor is a safe and effective technique compared with open procedure [10], the evidence is still limited.
Robotic technology, which provides high-definition three-dimensional vision with magnification, seven degrees of freedom of instrumental movement, tremor reduction, and comfortable ergonomics [11], was expected to reduce the technical difficulties of conventional laparoscopy and has been actively adopted for colorectal operations. There have been many reports of robot-assisted colectomies and most of them had concluded that the procedure was safe and feasible [2–4, 12–15]. However, most of the literature has focused on consecutive series of right hemicolectomy, anterior resection, and low anterior resection, and reports of robotic transverse colectomies are scarce.
Technically, it is generally accepted that laparoscopic anterior resection or right hemicolectomies are easier to perform than laparoscopic transverse colectomy. Separate dissection of the middle colic vessels and the harvest of lymph nodes, and full mobilization of hepatic and splenic flexure of colon, which are essential elements of laparoscopic transverse colectomy, are more challenging than other laparoscopic colectomies. Moreover, the patient population requiring a transverse colectomy is usually too small to overcome the long learning curve associated with a laparoscopic procedure. Because of this high technical demand, the advantages of robotic surgery can be maximized in a transverse colectomy. Dissection of the root of the middle colic vessels can be facilitated and performed more safely under stable three-dimensional magnified view and meticulous surgeon-controlled countertraction.
In every case, we carried out an intracorporeal end-to-end hand-sewn anastomosis. Currently, the majority of laparoscopic colectomies adopt an extracorporeal anastomosis. For this approach, the transverse colonic mesentery must be fully mobilized and both colonic flexures should be taken down to reach the minilaparotomy site, which is usually made with a small extension of the umbilical incision for the camera port. When adopting an intracorporeal end-to-end hand-sewn anastomosis, we can avoid excessive dissection and colonic flexure takedown to retract the specimen with the mesenteries [16]. Moreover, it may result in reduction of the incision length because the specimen could be extracted in a single linear shape instead of a double loop shape. This advantageous aspect may be exaggerated in obese patients who have thick abdominal wall and short transverse mesocolon [16, 17]. The hand-sewn anastomosis can be challenging with conventional laparoscopy; however, the robotic approach might provide specific advantages for this procedure with its improved ergonomics [18]. Patient 1 was the third case out of a total 162 consecutive series of robotic colectomies and, therefore, the total operation time was quite long, but the operator did not feel lots of technical difficulties during the hand-sewn intracorporeal anastomosis. The endo-wrist function of robotic instruments makes the suturing and tying process as easy as in open surgery. One of the limitations with da Vinci® Surgical System is the absence of tactile sensation, which was realized as frequent breaks of threads during knot-tying in our procedure. This is because the tensile strength on the thread is not transferred to the master console, so that the operator cannot properly control the strength in tightening the knots. However, after several trials and errors even in the first patient, the operator could achieve the proper skill of knot-tying with visual feedback, that is, observing the degree to which the colonic wall is compressed by the knots. Colonic bowel preparation was established with laxatives in all patients, and there was no inconvenience due to fecal spillage during the anastomosis.
In addition, because all procedures are performed in the peritoneal cavity without tactile sensation, precise localization of the tumor is a critical aspect of robotic transverse colectomy. We identified the lesion with preoperative tattooing or intraoperative ultrasonography. In all cases, the localization procedure was not difficult and worked well. Preoperative clipping and intraoperative X-ray are other possible options.
Transverse colectomy is not a surgery performed frequently, because tumor location in mid-transverse colon is rare and extended right or left hemicolectomy is carried out for advanced mid-transverse colon cancer to eradicate possible lymph nodes metastases around the right colic or left colic artery, respectively [19, 20]. So, we planned transverse colectomy with robotic approach for patients who had premalignant tumor which could not be removed by colonoscopic intervention or malignant lesion of early stage (cT2N0M0) which was located in the mid-transverse colon. However, one of them was finally reported to have pT3N0 cancer. Although at least 5 cm of surgical resection margin was allowed intraoperatively [21], histopathologic examination revealed proximal or distal resection margins less than 5 cm, owing to shortening of the bowel length during fixation and, concordantly, the number of harvested lymph nodes less than 12. Histopathologic results reflecting oncological radicality were suboptimal [22], but all three patients were alive without evidence of recurrence at the last follow-up date. It seems that a careful selection of patients with early mid-transverse colon cancer is required to perform this procedure, especially at the beginning period.
In conclusion, three consecutive cases of robotic transverse colectomy were successfully performed and, although small in number, we could find the theoretical benefits of robotic transverse colectomy combined with an intracorporeal anastomosis. We suggest that patients with early mid-transverse colon cancer are good candidates for this type of surgery.
References
Weber PA, Merola S, Wasielewski A, Ballantyne GH (2002) Telerobotic-assisted laparoscopic right and sigmoid colectomies for benign disease. Dis Colon Rectum 45:1689–1694 (discussion 95–6)
Antoniou SA, Antoniou GA, Koch OO, Pointner R, Granderath FA (2012) Robot-assisted laparoscopic surgery of the colon and rectum. Surg Endosc 26:1–11
Baik SH, Kwon HY, Kim JS, Hur H, Sohn SK, Cho CH et al (2009) Robotic versus laparoscopic low anterior resection of rectal cancer: short-term outcome of a prospective comparative study. Ann Surg Oncol 16:1480–1487
Pigazzi A, Luca F, Patriti A, Valvo M, Ceccarelli G, Casciola L et al (2010) Multicentric study on robotic tumor-specific mesorectal excision for the treatment of rectal cancer. Ann Surg Oncol 17:1614–1620
Chapman AE, Levitt MD, Hewett P, Woods R, Sheiner H, Maddern GJ (2001) Laparoscopic-assisted resection of colorectal malignancies: a systematic review. Ann Surg 234:590–606
Chung CC, Tsang WW, Kwok SY, Li MK (2003) Laparoscopy and its current role in the management of colorectal disease. Colorectal Dis 5:528–543
Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ et al (2005) Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol 6:477–484
Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM et al (2005) Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet 365:1718–1726
Clinical Outcomes of Surgical Therapy Study Group (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350:2050–2059
Chand M, Siddiqui MR, Rasheed S, Brown G, Tekkis P, Parvaiz A et al (2014) A systematic review and meta-analysis evaluating the role of laparoscopic surgical resection of transverse colon tumours. Surg Endosc 28(12):3263–3272
Lanfranco AR, Castellanos AE, Desai JP, Meyers WC (2004) Robotic surgery: a current perspective. Ann Surg 239:14–21
D’Annibale A, Pernazza G, Morpurgo E, Monsellato I, Pende V, Lucandri G et al (2010) Robotic right colon resection: evaluation of first 50 consecutive cases for malignant disease. Ann Surg Oncol 17:2856–2862
Park YA, Kim JM, Kim SA, Min BS, Kim NK, Sohn SK et al (2010) Totally robotic surgery for rectal cancer: from splenic flexure to pelvic floor in one setup. Surg Endosc 24:715–720
deSouza AL, Prasad LM, Park JJ, Marecik SJ, Blumetti J, Abcarian H (2010) Robotic assistance in right hemicolectomy: is there a role? Dis Colon Rectum 53:1000–1006
Baek SK, Carmichael JC, Pigazzi A (2013) Robotic surgery: colon and rectum. Cancer J 19:140–146
Stein SA, Bergamaschi R (2013) Extracorporeal versus intracorporeal ileocolic anastomosis. Tech Coloproctol 17(Suppl 1):S35–S39
Pigazzi A, Garcia-Aguilar J (2010) Robotic colorectal surgery: for whom and for what? Dis Colon Rectum 53:969–970
Hellan M, Anderson C, Pigazzi A (2009) Extracorporeal versus intracorporeal anastomosis for laparoscopic right hemicolectomy. JSLS 13:312–317
Park IJ, Choi GS, Kang BM, Lim KH, Jun SH (2009) Lymph node metastasis patterns in right-sided colon cancers: is segmental resection of these tumors oncologically safe? Ann Surg Oncol 16:1501–1506
Pusztaszeri M, Matter M, Kuonen A, Bouzourene H (2009) Nodal staging in colorectal cancer: should distant lymph nodes be recovered in surgical specimens? Hum Pathol 40:552–557
Watanabe T, Itabashi M, Shimada Y, Tanaka S, Ito Y, Ajioka Y et al (2012) Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer. Int J Clin Oncol 17:1–29
Edge SB, Byrd BD, Comptom CC, Fritz AG, Greene FL, Trotti A (2010) AJCC cancer staging manual, 7th edn. Springer, New York, pp 145–166
Conflict of interest
Kyung Uk Jung, Yoonah Park, Kang Young Lee, and Seung-Kook Sohn declare that they have no conflict of interest.
Ethical standard
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study (retrospective study), formal consent is not required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Jung, K.U., Park, Y., Lee, K.Y. et al. Robotic transverse colectomy for mid-transverse colon cancer: surgical techniques and oncologic outcomes. J Robotic Surg 9, 131–136 (2015). https://doi.org/10.1007/s11701-015-0502-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-015-0502-7