
Abstract
The background of this study is to compare prospectively the oncological and functional results of open radical prostatectomy (OP) and robotic prostatectomy (RP) from the experience of a single surgeon. Between June 2002 and June 2007, 422 patients underwent radical prostatectomy (OP 199, RP 223). We divided OP patients into 89 early cases (OP-I) and 110 late cases (OP-II) before and after introduction of a robotic system, and RP patients into 35 early cases (RP-I) and 188 late cases (RP-II). Functional outcomes were measured by use of validated questionnaires completed by the patients. There were no significant differences in preoperative characteristics among the four groups, except that RP-I patients had lower biopsy Gleason scores. In the RP groups the mean estimated blood loss was lower and mean durations of hospital stay and bladder catheterization were shorter compared to those of the OP groups. The frequency of intraoperative complications was significantly lower in the RP-II group. The positive surgical margin rates in the RP-II group were similar to or lower than those in the OP groups when stratified by pathologic stage T2 and T3. From one month after surgery, RP-II patients had higher continence rates than OP-II patients. For patients ≥60 years old, recovery of potency was better in the RP-II group. To conclude, RP by an experienced surgeon may have a similar or lower positive surgical margin rate than OP. Additionally, RP may lead to a shorter duration of bladder catheterization and hospital stay and better recovery of continence and potency than obtainable by OP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Surgical treatment for localized prostate cancer has evolved tremendously in the past 25 years. Since Walsh et al. [1] introduced the nerve-sparing technique in 1982, open radical retropubic prostatectomy (OP) has been an increasingly used treatment option. With the advent of prostate-specific antigen (PSA) testing in 1987 and the accompanying increase in newly diagnosed localized cases, the use of radical prostatectomy has continued to expand.
In the past decade there have been many advances in radical surgery for prostate cancer, and results from the new surgical techniques are similar to or superior to those from the reference standard surgical therapy. Laparoscopic radical prostatectomy (LP) has a success rate equivalent to OP but leads to a shorter hospital stay, shorter time to full recovery, and reduced risk of blood loss. Even so, the technical difficulty of the procedure still prevents many urologists from attempting the operation [2–7].
The introduction of the da Vinci robotic system has allowed urologists without advanced laparoscopic skills to perform LP safely. As a result, robotic radical prostatectomy (RP) is increasingly being used. Although many studies have compared OP and RP, the surgical benefits of RP are still controversial [8–11]. Most studies have compared the results of OP and RP as performed by several different surgeons; few have examined the experiences of a single surgeon with both OP and RP. Moreover, to the best of our knowledge, there have been no studies comparing, prospectively, functional outcomes using validated questionnaires completed by the patients, from the experience of a single surgeon.
Accordingly, this study was designed to verify prospectively the surgical benefits of RP compared with OP, especially functional outcomes, by using validated questionnaires, based on the experiences of a single surgeon.
Materials and methods
From June 2002 to June 2007, a total of 422 patients received a radical prostatectomy from one surgeon (CY) after being diagnosed with prostate cancer without distant metastases. The surgeon, who had previously performed 89 OP cases using the standard retropubic approach before the introduction of the robotic system, performed 110 OP cases and 223 RP cases after the introduction of the da Vinci robotic system in July 2005, without any prior experience in LP.
The preoperative examination included a digital rectal examination, bone scan, and computed tomography or magnetic resonance imaging of all patients. We used the 2002 TNM classification for clinical staging, and the upper normal limit for pelvic lymphadenopathy by computed tomography was 1 cm. The surgical approach was chosen by each patient after thorough discussion of the merits and drawbacks of each procedure. Otherwise no particular selection criteria were used. All patients granted informed consent when required by the institutional review board.
OP was performed by the standard retropubic approach and RP by the transperitoneal approach using four robotic arms. In all cases we performed a bilateral lymphadenectomy including the obturator, external iliac, and internal iliac lymph nodes (LNs). A nerve-saving procedure was performed in preoperatively potent patients with preoperative clinical T stage ≤T2 and preoperative PSA levels ≤10 ng/ml. In some clinically locally advanced cases, a unilateral nerve-saving procedure was selectively performed in patients who desired the preservation of potency when unilateral extracapsular extension (ECE) was suspected in the intraoperative finding. An indwelling drainage tube was placed in all patients and removed when there was less than 50 ml of drained fluid in OP cases and less than 100 ml of drained fluid in RP cases. We made it a rule to remove the urethral Foley on postoperative day 7 in all cases, but we prolonged the duration of bladder catheterization in cases of severe adhesion around the prostate, severe bleeding, difficulties in urethrovesical anastomosis, or a sustained amount of drainage fluid. Moreover, we reduced the duration of bladder catheterization if there was no specific problem. We did not perform a cystogram while removing the urethral Foley if there was no recovery-related problem. All patients were discharged at their own discretion depending on their general condition after removal of the drainage tube.
After introducing the robotic system, we prospectively assessed clinical outcomes and changes from baseline by use of a validated questionnaire assessing urinary (International Continence Society questionnaire: ICSmaleSF) and sexual (International Index of Erectile Function: IIEF) function, completed at home by the patient every three months postoperatively for 12 months, and mailed back to the data-management office. Patients were considered continent when they replied that they did not experience any leakage or were pad-free, and potency was defined as the ability to have erections sufficient for intercourse with or without the help of phosphodiesterase type 5 inhibitors.
We divided the OP group into 89 early cases (OP-I, before the introduction of the robotic system), and 110 late cases (OP-II, after the introduction of the robotic system), and the RP group into 35 early cases (RP-I) and 188 late cases (RP-II) to compare differences related to surgeon experience [12]. We prospectively compared functional results (urinary continence and sexual function) between OP-II and RP-II after excluding 35 early cases (RP-I).
We used the chi-squared test, Fisher’s exact test, Student’s t test, and ANOVA to compare preoperative, intraoperative, and postoperative variables between the RP and OP groups. Statistical analysis was performed using Statistical Software for the Social Sciences, version 12 (SPSS, Chicago, IL, USA), and p values <0.05 were considered statistically significant.
Results
Apart from one instance of system malfunction, there was no conversion to OP during RP due to technical difficulty. The preoperative clinical characteristics of OP and RP patients are summarized in Table 1. There were no significant differences in mean age (p = 0.149), body mass index (p = 0.171), preoperative PSA level (p = 0.592), or clinical stage (p = 0.072) among the four groups, but RP-I patients had significantly lower biopsy Gleason scores (p = 0.002) compared with patients in the other groups and there was a significant difference in biopsy Gleason scores between the OP-II and RP-II groups (p = 0.047).
There were significant differences in prostatectomy Gleason scores (p < 0.001), pathologic T stage (p = 0.002), LN invasion rate (p = 0.003), and ECE (p = 0.038) among the four groups. Between the OP-II and RP-II groups there were significant differences in prostatectomy Gleason scores (p < 0.001), pathologic T stage (p < 0.001), but no differences in LN invasion rate and ECE. Nerve-saving procedures were performed less often in the RP-I group and more often in the RP-II group compared with the OP groups. There was a significant difference in the positive surgical margin rate for cases overall among the four groups (p < 0.001). When T2 and T3 stages were evaluated separately, however, there was only a significant difference between groups for pathologic stage T2, but not pathologic stage T3 (p = 0.007, p = 0.249, respectively). In the analysis of pathologic stage T2 cases alone, the positive surgical margin rate in the RP-II group was comparable with that in the OP-II group (p = 1.000), and both OP-II and RP-II groups had significantly lower positive surgical margin rates compared with the other groups. In the analysis of pathologic stage T3 cases alone, the positive surgical margin rate in the RP-II group was slightly lower than in the other groups, but the trend did not reach statistical significance (for cases overall among the four groups, p = 0.249, between OP-II and RP-II, p = 1.000). Estimated blood loss (EBL) was significantly smaller in the RP group, especially the RP-II group (OP-I: 1,080.3 ± 328.0 ml, OP-II: 748.3 ± 211.9 ml, RP-I: 647.1 ± 211.8 ml, RP-II: 333.3 ± 213.7 ml, p < 0.001). There were significant differences in the postoperative normal diet start day (OP-I: 2.3 ± 0.7 days, OP-II: 1.8 ± 0.6 days, RP-I: 1.8 ± 0.4 days, RP-II: 1.4 ± 0.5 days, p < 0.001), the duration of hospital stay (OP-I: 8.9 ± 1.9 days, OP-II: 6.6 ± 0.6 days, RP-I: 5.2 ± 0.8 days, RP-II: 3.6 ± 0.6 days, p < 0.001), and bladder catheterization (OP-I: 8.7 ± 0.6 days, OP-II: 7.7 ± 0.7 days, RP-I: 8.0 ± 1.0 days, RP-II: 7.3 ± 0.6 days, p < 0.001) among the four groups. The complication rate differed among the four groups (p < 0.001). Complications tended to be more frequent in the RP-I group because of lack of surgical experience, and less frequent in the RP-II group (Table 2).
Table 3 compares the postoperative continence rates between the OP-II and RP-II groups using the strict criteria defined above (no leakage and no pad). None of the patients was regarded as incontinent before surgery. Full continence rates were significantly higher in the RP-II group from 1 to 12 months after surgery (postoperative 1 month: p = 0.007, 3 months: p = 0.005, 6 months: p = 0.009, 12 months: p = 0.008).
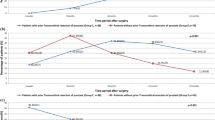
Postoperative potency rates are shown in Table 4. A majority of patients (76.7 and 87.3% in the OP-II and RP-II groups, respectively) had preoperative potency with or without the help of phosphodiesterase type 5 inhibitors. In patients 60 years or younger, there was no difference in the recovery of potency 12 months after surgery between OP-II and RP-II groups for overall cases, even when cases with nerve-saving procedures were analyzed separately. In patients 60 years or older, however, potency at 12 months after surgery was significantly better in the RP-II group compared with the OP-II group for overall cases (p < 0.001). When the use of a nerve-saving procedure was taken into account, potency was improved when a bilateral nerve-saving procedure was performed in the RP-II group (p = 0.002, Table 4).
Discussion
The introduction of robotic systems has enabled surgeons with experience with OP only to successfully use RP. Nevertheless, the surgical benefits of RP are still under debate. We prospectively compared the various methods of radical prostatectomy for oncological and functional outcomes, and process-related and recovery-related variables, from the experience of a single surgeon.
According to recent studies comparing OP, LP, and RP, it is difficult to make meaningful comparisons of overall or disease-specific survival because of the recent introduction of the robotic system and the slow progression of prostate cancer. After controlling for pathologic stage and grade between OP and RP groups, past studies have found no early differences in biochemical recurrence rates [13, 14]. Although positive surgical margin rates are also similar in direct comparisons of the two techniques, the OP cohorts from those studies were treated earlier in the PSA era and generally had higher-volume disease. Consequently, positive surgical margin rates should be determined by expert surgeons in each approach, and stratified by pathologic stage [13, 14]. The following variables are related to intraoperative and postoperative recovery: duration of hospital stay and bladder catheterization, EBL, degree of postoperative pain, and time to full recovery. Only EBL and time to full recovery are reportedly superior in patients treated with RP [3, 8, 13], and treatment with OP or RP does not lead to definite differences in the functional outcomes of potency recovery and continence [5, 11, 15].
The major drawback to these reports is that they each compared the outcomes of several different open surgeries with the outcomes of varied robotic surgeries performed by different surgeons. A comparison of the two surgical techniques from different surgeons invites bias with regard to the variability of training and technique, as well as surgeon experience and skill. To date, few studies in the literature have compared OP and RP based on the experience of a single surgeon. Moreover, there have been no studies comparing, prospectively, functional outcomes using validated questionnaires completed by the patients. Ahlering et al. [16] reported that RP had oncological and urinary outcomes that were at least equal to those of OP. At the same time, the surgeon in that study had 18 years of experience with OP, which potentially benefitted the results of the OP group, because the authors compared 60 recent OP cases with 60 RP cases performed after 45 initial cases of RP. Moreover, they reported the continence rate after only 3 months of follow-up, an insufficient interval to evaluate urinary function and sexual function.
In our study, we compared the results of OP and RP performed by one surgeon with three years of OP experience and divided the OP cases into 89 early cases, which were performed before the introduction of the robotic system and 110 late cases, which were performed after its introduction. The RP cases were also divided into 35 early cases and 188 late cases to examine differences related to experience. We prospectively compared oncological and postoperative functional outcomes by using a confidential, self-administered questionnaire regarding urinary continence and potency before and 1, 3, 6, and 12 months after surgery after the introduction of the robotic system. Although using the date that the robotic system became available to divide open cases into early versus late is highly arbitrary, the surgeon could be out of his learning curve for OP after the early 89 cases, and we have collected the prospective data for comparison of OP and RP since the introduction of the robotic system. Several programs have reported that surgeons with minimal or no laparoscopic experience have mastered the learning curve with the robotic system after 10–20 cases [17, 18], but 10–20 cases were not enough in our experience. Accordingly, we divided the RP cases into 35 early cases and 188 late cases, as described by Rozet et al. [12].
There were no significant differences in clinical variables between the OP and RP groups, except that the RP-I group patients had lower biopsy Gleason scores. Although there was no statistical significance, the clinical stage in the RP-I group was almost always localized because of concerns about minimal surgical experience during the early introduction of the robotic system. Positive surgical margin rates in the RP-II group, which consisted of patients who received treatment after the surgeon had gained experience, were similar to or lower than those of the OP-II group. The improvements even included patients with pathologic stage T3 prostate cancer, although there were only a few such patients. These findings contradict the results of two contemporary European series using different surgical approaches stratified by the final pathologic stage in which there appeared to be a trend towards lower positive margin rates in patients who underwent OP for pathologic stage T3 disease [19, 20]. This important finding clearly requires further study. Moreover, the postoperative “recovery”-related variables were all lower in the RP groups, especially the RP-II group. The frequency of complications was greater during the early introduction of the robotic system, but it dropped significantly in the RP-II group compared with the OP groups after the surgeon had mastered the robotic system. Although our postoperative follow-up period was limited to 12 months, the postoperative recovery of continence was greater in the RP-II group. In patients 60 years or older, recovery of potency was also better in the RP-II group when a nerve-saving procedure was performed.
The superior results we observed for all variables in the RP group remain debatable (except for the EBL). Nonetheless, they could be explained by the fact that we were able to maintain an excellent surgical visual field throughout the RP because of the reduced EBL due to use of the robotic system. The lack of tactile feedback, a potential disadvantage of RP, was overcome by adapting to the robotic system through experience.
Although a prospective randomized control trial remains the ideal way to compare two different treatments, it would be difficult to apply such an approach to actual patients in this clinical setting. In our cohorts, each patient chose a surgical approach after thorough discussion of the merits and drawbacks of each method. There was a probable bias in patient selection, in that the clinical stage in the RP-I group was almost always localized because of concerns about minimal surgical experience during the early introduction of the robotic system. We tried to overcome this limitation by comparing positive surgical margin rates in each approach, stratified by pathologic stage.
Although longer follow-up of oncological outcomes, such as prostate cancer-specific death and the recovery of continence and potency, is needed for more patients, the use of RP in the surgical treatment of prostate cancer is sure to expand as surgeons gain experience with the robotic system and other advances in technology using robotic instruments.
References
Walsh PC, Donker PJ (1982) Impotence following radical prostatectomy: insight into etiology and prevention. J Urol 128:492–497
Guillonneau B, el-Fettouh H, Baumert H et al (2003) Laparoscopic radical prostatectomy: oncological evaluation after 1,000 cases a Montsouris Institute. J Urol 169:1261–1266. doi:10.1097/01.ju.0000055141.36916.be
Bhayani SB, Pavlovich CP, Hsu TS et al (2003) Prospective comparison of short-term convalescence: laparoscopic radical prostatectomy versus open radical retropubic prostatectomy. Urology 61:612–616. doi:10.1016/S0090-4295(02)02416-0
Boccon-Gibod L (2006) Radical prostatectomy: open? Laparoscopic? Robotic? Eur Urol 49:598–599. doi:10.1016/j.eururo.2006.01.023
Hara I, Kawabata G, Miyake H et al (2003) Comparison of quality of life following laparoscopic and open prostatectomy for prostate cancer. J Urol 169:2045–2048. doi:10.1097/01.ju.0000063961.99940.6c
Jaffe J, Stakhovsky O, Cathelineau X et al (2007) Surgical outcomes for men undergoing laparoscopic radical prostatectomy after transurethral resection of the prostate. J Urol 178:483–487. doi:10.1016/j.juro.2007.03.114
Touijer K, Guillonneau B (2006) Laparoscopic radical prostatectomy: a critical analysis of surgical quality. Eur Urol 49:625–632. doi:10.1016/j.eururo.2006.01.018
Menon M, Tewari A, Baize B et al (2002) Prospective comparison of radical retropubic prostatectomy and robot-assisted anatomic prostatectomy: the Vattikuti Urology Institute experience. Urology 60:864–868. doi:10.1016/S0090-4295(02)01881-2
Nelson B, Kaufman M, Broughton G et al (2007) Comparison of length of hospital stay between radical retropubic prostatectomy and robotic assisted laparoscopic prostatectomy. J Urol 177:929–931. doi:10.1016/j.juro.2006.10.070
Webster TM, Herrell SD, Chang SS et al (2005) Robotic assisted laparoscopic radical prostatectomy versus retropubic radical prostatectomy: a prospective assessment of postoperative pain. J Urol 174:912–914. doi:10.1097/01.ju.0000169455.25510.ff
Tewari A, Srivasatava A, Menon M (2003) A prospective comparison of radical retropubic and robot-assisted prostatectomy: experience in one institution. BJU Int 92:205–210. doi:10.1046/j.1464-410X.2003.04311.x
Rozet F, Jaffe J, Braud G et al (2007) A direct comparison of robotic assisted versus pure laparoscopic radical prostatectomy: a single institution experience. J Urol 178:478–482. doi:10.1016/j.juro.2007.03.111
Rassweiler J, Seemann O, Schulze M et al (2003) Laparoscopic versus open radical prostatectomy: a comparative study at a single institution. J Urol 169:1689–1693. doi:10.1097/01.ju.0000062614.56629.41
Salomon L, Levrel O, de la Taille A et al (2002) Radical prostatectomy by the retropubic, perineal and laparoscopic approach: 12 years of experience in one center. Eur Urol 42:104–110. doi:10.1016/S0302-2838(02)00360-3
Walsh PC, Marschke P, Ricker D et al (2000) Patient-reported urinary continence and sexual function after anatomic radical prostatectomy. Urology 55:58–61. doi:10.1016/S0090-4295(99)00397-0
Ahlering TE, Woo D, Eichel L et al (2004) Robot-assisted versus open radical prostatectomy: a comparison of one surgeon’s outcomes. Urology 63:819–822. doi:10.1016/j.urology.2004.01.038
Ahlering TE, Skarecky D, Lee D et al (2003) Successful transfer of open surgical skills to a laparoscopic environment using a robotic interface: initial experience with laparoscopic radical prostatectomy. J Urol 170:1738–1741. doi:10.1097/01.ju.0000092881.24608.5e
Menon M, Shrivastava A, Tewari A et al (2002) Laparoscopic and robot assisted radical prostatectomy: establishment of a structured program and preliminary analysis of outcomes. J Urol 168:945–949. doi:10.1016/S0022-5347(05)64548-X
Palisaar RJ, Noldus J, Graefen M et al (2005) Influence of nerve-sparing (NS) procedure during radical prostatectomy (RP) on margin status and biochemical failure. Eur Urol 47:176–184. doi:10.1016/j.eururo.2004.09.002
Rassweiler J, Hruza M, Teber D et al (2006) Laparoscopic and robotic assisted radical prostatectomy—critical analysis of the results. Eur Urol 49:612–624. doi:10.1016/j.eururo.2005.12.054
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ham, W.S., Park, S.Y., Kim, W.T. et al. Open versus robotic radical prostatectomy: a prospective analysis based on a single surgeon’s experience. J Robotic Surg 2, 235–241 (2008). https://doi.org/10.1007/s11701-008-0111-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-008-0111-9