
Abstract
Background
Validated equations for body composition analysis using bioelectrical impedance (BIA) in morbidly obese (MO) subjects are scarce. Thus, our aim was to develop new equations from physical and BIA parameters to estimate whole-body and segmental body composition in MO subjects, with dual-energy X-ray absorptiometry (DXA) as the reference method.
Methods
A cross-sectional study on 159 Caucasian MO subjects (female 78%, age 43.5 ± 11.8 years, BMI 45.6 ± 4.9 kg/m2) divided in two groups was conducted: model building cohort (n = 110) and model validation cohort (n = 49). Stepwise regression analysis was used to develop specific fat free mass (FFM) and fat mass (FM) equations.
Results
Gender, body weight, and height2/impedance accounted, respectively, for 89.4% (p < 0.001) and 89.3% (p < 0.001) of the variability of DXA-total FFM in the two cohorts. Using the new equation, the mean difference between the DXA-FFM and BIA-FFM estimates was +0.180 kg (95% CI: -0.34 to +0.7 kg, p = NS), and the resulting limits of agreement were +6.76 and −6.40 kg. Similarly, good estimates of DXA truncal-, android-, and gynoid-FM from anthropometric and BIA parameters could be obtained from weight, height2/impedance, and waist and hip circumferences (respectively, R 2 adjusted: 0.657, 0.776, and 0.770; p < 0.001).
Conclusions
The new equations derived from physical and BIA parameters provide accurate estimates of body composition in MO subjects.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prevalence of morbid obesity has increased in recent years in Western countries [1]. Morbid obesity is characterized by an excessive amount of body fat, and total body fat and its distribution have been shown to be important determinants of the health burden associated with excessive body weight in this group of subjects [2, 3]. Therefore, there is now a need for convenient methods to evaluate the body composition and body fat distribution of morbidly obese individuals both in clinical practice and as part of research programs.
Many technologies are available to measure body composition [4]. Dual-energy X-ray absorptiometry (DXA) is used extensively for the assessment of body composition and is considered valid and reliable [5]. DXA use in morbidly obese subjects has been limited by weight restrictions of the instruments and, in some cases, by limitations in physically fitting the patient into the measurement compartment [4]. These limitations have been improved in current DXA equipments [6]. Nonetheless, the wide application of DXA for body composition analysis is limited by requirements for expensive equipment, trained technicians, and dedicated facilities. Alternatively, bioelectrical impedance analysis (BIA) is a non-invasive, inexpensive, easy, and portable method to evaluate body composition suitable for field use [4, 7, 8]. Interestingly, technological advances in BIA have made now available not only total body fat mass estimates but also information on body fat distribution [9]. However, BIA is considered unreliable for body composition assessment in morbid obesity since studies have shown that BIA devices tend to overestimate fat free mass (FFM) and underestimate fat mass (FM) in this specific population [10–14]. Nonetheless, previous studies have relied on equations for body composition estimation that had not been validated in subjects with a BMI > 35 kg/m2. Surprisingly, a few studies have compared BIA and reference methods to develop equations that specifically predict body fat in severely obese subjects [15]. Furthermore, to our knowledge, there are no reports on specific equations for regional body fat distribution applicable to the morbidly obese population.
Against this background, the central aim of our study was to develop new equations to accurately estimate total FFM and segmental FM in morbidly obese patient from physical and BIA parameters. For that purpose, whole-body and segmental FFM and FM estimates were obtained with DXA as the reference method, and whole-body impedance was obtained using the Tanita BC 418 MA BIA device. The Tanita BC 418 MA is a single-frequency BIA equipment incorporating eight electrodes, providing estimates of total and regional body composition. Thus, as a secondary aim, we evaluated the performance of the Tanita BC 418 MA in estimating whole-body as well as segmental body composition analysis in morbidly obese subjects as compared to the DXA analysis.
Materials and Methods
Subjects
A total of 159 (male, n = 35; female, n = 124) Caucasian morbidly obese subjects participated in our study. The study participants were selected among the consecutive subjects referred to our University Hospital Obesity Unit from February 2009 to April 2010. Eligible participants had to be 18 or older, with stable weight (body weight change ± 2 kg) for a period of three months prior to enrollment. Subjects weighing ≥200 kg were excluded because BIA evaluation was not possible. Based on clinical history, persons with serious metabolic, cardiovascular, or endocrine diseases (i.e., cancer, heart failure, pulmonary insufficiency, chronic kidney disease, and impaired thyroid function) were also excluded from the study. Furthermore, exclusion criteria included pregnancy, breast-feeding, being on a diet, and the use of medications known to cause dehydration, water retention, electrolyte disturbance, or changes in body weight. Finally, the presence of lower limb edema apparent on physical examination was excluded in the selected population. The first 110 subjects consecutively enrolled in the study served as a model building cohort (group 1). The remaining 49 served as a model validation cohort (group 2). The Ethical Committee of our Institution approved the study, and study participants gave informed consent prior to examination.
Methods
Anthropometric Measurements
Patients underwent anthropometrical and body composition assessments following an overnight fasting. Participants were weighted with light clothes and without shoes to the nearest 0.1 kg. Height was determined using a fixed wall stadiometer to the nearest 0.1 cm. Waist circumference was measured to the nearest 0.5 cm, at the level of the iliac crest, with a standard flexible, inelastic measuring tape. Hip circumference was measured to the nearest 0.1 cm at the maximum extension at the buttocks level. Body mass index (BMI) was calculated as weight (kg) divided per squared height (meters).
Dual-Energy X-ray Absorptiometry
DXA scans were performed using the whole-body scanner GE Lunar iDXA (GE Healthcare, Madison, WI) according to the manufacturer's specifications. The iDXA is a narrow fan-beam DXA instrument with a high weight limit (204 kg) and a relatively wide scanning space (66 cm) designed to accommodate obese subjects. The subjects were positioned at the center of the table for each scan. Appropriateness of patient's position is further assessed by the DXA software by means of an automatic detection system. The instrument has three scan modes that adjust the X-ray attenuation for the thickness of each patient. For this study, scans were performed using the default scan mode automatically selected by the DXA software. The GE Lunar Body Composition Software enCORE TM 2008 GE Healthcare version 12.30.008 was used to obtain lean tissue mass (LTM), bone mineral content (BMC), and FM measurements, as well as their segmental (trunk, right and left upper limbs, right and left lower limbs, android, and gynoid) distribution. Total and segmental FFM from DXA was considered as the corresponding sum of LTM and BMC.
Bioelectrical Impedance Analysis (BIA)
The Tanita BC 418 MA Segmental Body Composition Analyzer (Tanita, Japan) is a single-frequency (50 kHz) BIA device incorporating eight electrodes. BIA measurements were carried out according to manufacturer's manual. Information on subject age, height, and body type (all routinely were classified as “standard” body type) were manually entered into the equipment. Subjects were required to adhere to standard BIA testing guidelines [7]. BIA was performed in subjects wearing light clothes, standing erect, and with bare feet on the analyzer's footpads. The BIA provided data for whole-body and segmental (upper limbs and lower limbs) impedance and estimates of FM (in kg and as percentage of total body weight), FFM (in kg), and TBW (in kg), as wells as segmental (trunk, right and left upper limbs, and right and left lower limbs) FM and FFM estimates. The exact formula for total and segmental FM and FFM are proprietary and thus not accessible.
Statistical Analysis
Descriptive statistics are expressed as mean ± standard deviation unless stated otherwise. For our secondary endpoint, simple regression analysis was performed to test the correlation between total and segmental FFM measurements obtained from DXA and BIA estimates as provided by the Tanita BC 418 MA device. Furthermore, Student's t test was used to test differences between the two methods, and the agreement between the DXA and BIA body composition estimates was assessed using the Bland–Altman analysis (limits specified as mean of the difference ± 1.96 standard deviation). To develop new predictive equations, the central aim of our study, a stepwise multivariate linear regression analysis was used based on the building model cohort (group 1). For that purpose, gender, age, weight, height2/impedance, and waist or hip circumference were considered as independent predictors of total and segmental DXA-FFM or FM measurements. The equations obtained in group 1 were then tested in the validation sample (group 2). Sample size was calculated according to Tabachnick and Fidell [16]. Furthermore, we performed a post-hoc calculation of the statistical power of our analysis based on our sample size (n = 110) and on the correlation coefficients found between the studied variables. Statistical power was >99% for total FFM, android-FM, and gynoid-FM estimates and 77% for truncal-FM estimate. Statistical analysis was performed using SPSS 16.0 (Chicago, ILL, US). Statistical significance was set at p < 0.05.
Results
The clinical characteristics and data on body composition from BIA (as retrieved from the Tanita BC 418 MA) and DXA of the 159 study participants are shown in Table 1. The study population was composed of 33 males and 126 females. Age ranged from 18 to 70 years, and BMI ranged from 35.0 to 62.4 kg/m2. Gender, age, and BMI distribution were not significantly different when the model building cohort (group 1) and the model validation cohort (group 2) were compared. Likewise, the two cohorts were not significantly different in any of the body composition parameters obtained from DXA or BIA analysis.
A good correlation was found between the DXA-FFM measurement and the FFM-estimate provided by the Tanita BC 418 MA (R 2 = 0.883, p < 0.001). Furthermore, Bland–Altman plot analysis showed an agreement between DXA- and BIA-FFM (Fig. 1). However, as compared to the DXA-FFM, total FFM was overestimated by 3.9 kg (95%CI 3.12–4.75 kg) when BIA was used (paired Student’s t test: p < 0.001). The 95% confidence interval for limits of agreement ranged from 12.32 to −4.45 kg. Moreover, a systematic bias was found (R 2 = 0.183, p < 0.001) so that BIA resulted in a larger overestimation of FFM with increasing FFM (Fig. 1).

Bland–Altman analysis of the whole-body fat free mass (FFM) assessed by dual-energy X-ray absorptiometry (DXA) and bioimpedance (BIA), as provided by the Tanita BC 418 MA, in the model building cohort (group 1, n = 110). The horizontal solid line represents the mean, the dashed line represents the ± 2 standard deviation for the whole sample, and each dot represents an individual. The regression line represents the systematic bias in the fat free mass (FFM) estimate with larger FFM (R 2 = 0.183)
To construct a predictive equation for DXA-FFM, stepwise multivariate linear regression analysis was used in group 1, with FFM from DXA as the dependent variable. Gender, age, and height2/whole-body impedance as obtained from BIA, body weight, and waist circumference were used as predictors. The predictive equation derived from stepwise multivariate linear regression was as follows: BIA-FFM (kg) = 18.240-[4.395*gender (male = 1, female = 2)] + [0.137*weight (kg)]+ [5,865.274*height2/impedance (m2/ohms)].
The variables included in the model (gender, body weight, and height2/whole-body impedance) accounted for 89.4% (R 2 adjusted = 0.894, p < 0.001) of the variability of DXA total FFM (kg). Of note, 86.3% of the variance of DXA-FFM in our model was accounted for height2/impedance. Neither age nor waist circumference was a significant predictor of DXA-FFM in our cohort. When the resulting new equation was applied to the validation sample (group 2), the adjusted correlation coefficient (R 2) was 0.893 (p < 0.001). Thus, no shrinkage in the prediction was observed when the equation derived from group 1 was validated in group 2 [17]. Using the new equation, the mean difference between the DXA-FFM and new BIA-FFM estimates in group 2 was +0.180 kg (95% CI: -0.34 to +0.7 kg) (Fig. 2). The DXA-FFM and BIA-FFM estimates predicted with the new equation were not significantly different when compared using a paired Student’s t test. The resulting limits of agreement were +6.76 and −6.40 kg, and no systematic bias was found.

Bland–Altman analysis of the whole-body fat free mass (FFM) assessed by dual-energy X-ray absorptiometry (DXA) and bioimpedance (BIA), using the new equation, in the model validation cohort (group 2, n = 49). The solid line represents the mean, the dashed line represents the ± 2 standard deviation for the whole sample, and each dot represents an individual
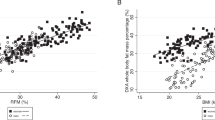
Data on segmental body composition analysis as measured by DXA and obtained from the Tanita BC 418 MA are shown in Table 1. Linear correlation coefficients for the different regions obtained from the two assessments are shown in Table 2. Although the segmental FM BIA estimates were significantly correlated with those from DXA, the adjusted R 2 was generally low. We observed a significant underestimation of truncal-FM and an overestimation of FM in upper and lower limbs when estimates from the Tanita BC 418 MA were considered (Table 2, paired Student’s t test: p < 0.001). Furthermore, we evaluated the correlation between DXA android- and DXA gynoid-FM with related estimates from BIA (respectively, truncal-FM and mean FM in the lower limbs). In both cases, although statistically significant, the adjusted R 2 was low [R 2 adjusted: 0.485 (p < 0.001) and 0.373 (p < 0.001), respectively].
To construct predictive equations for DXA truncal-, DXA android-, and DXA gynoid-FM, we used again stepwise multivariate linear regression analysis including age, gender, weight, height2/whole-body impedance, waist circumference, and hip circumference as predictors. The new predictive equations for DXA truncal-, DXA android-, and DXA gynoid-FM are shown in Table 3. Weight, hip circumference, waist circumference, and height2/whole-body impedance yielded a good estimates of DXA truncal-FM (R 2 adjusted = 0.657, p < 0.001), DXA android-FM (R 2 adjusted = 0.776, p < 0.001), and DXA gynoid-FM (R 2 adjusted = 0.770, p < 0.001). Nonetheless, the BIA-derived parameter (height2/whole-body impedance) explained only 4.8%, 1.3%, and 6.1%, respectively, of the variance of these segments of DXA-FFA. Age and gender were not significant predictors of neither DXA truncal nor DXA android fat nor DXA gynoid fat. The three segmental FM equations (truncal, gynoid, and android) developed in the building cohort were next tested in the validation sample. We did not observe shrinkage in the prediction (R 2 adjusted: 0.657, 0.770, and 0.775, respectively; all p < 0.001), and the estimates were not significantly different when compared using a paired t test. The prediction of the DXA gynoid-FM was not improved when the mean of lower limb impedance as obtained from BIA was used (data not shown).
Discussion
In this study, we describe a new equation that allows for an accurate estimate of total FFM in Caucasian morbidly obese adult subjects using BIA and anthropometric parameters. Likewise, a stepwise linear regression approach allowed us to provide equations for good estimates of DXA truncal-, android-, and gynoid-FM using whole-body impedance and anthropometric measurements. Furthermore, we found that the assessment of BIA total FFM resulting from the Tanita BC 418 MA BIA manufacturer equation not only yields an overestimation of the FFM compartment in Caucasian morbidly subjects but also results in a systematic bias with larger FFM when compared to DXA measurements obtained with the Lunar iDXA. Finally, we have shown a weak correlation between segmental FM estimates from the Tanita BC 418 MA BIA device and those obtained from DXA.
The BIA of body composition is a convenient approach for routine clinical practice use [7–9]. However, the availability of specific equations for morbidly obese subjects is scarce [15]. In agreement with previous studies, we found that in morbidly obese subjects, the BIA results obtained with a commercially available device result in an overestimation of FFM and underestimation of FM when compared to data obtained from DXA as the reference method [11–14]. Studies have shown that these results are independent of the BIA device used (four/eight electrode or single frequency/multifrequency). Furthermore, as in our study, previous reports showed an underestimation of FM in overweight and obese populations and larger discrepancies with increasing adiposity [11, 14]. Among others, BIA estimation of body composition is based on the assumption that total body water (TBW) constitutes a fixed percentage of lean mass [7]. However, studies have proved this assumption incorrect in morbidly obese subjects [14, 18]. Thus, a higher level of hydration in morbidly obese subjects could result in overestimation of FFM in this specific population when non-specific equations are used.
In the present study, we report a new equation to estimate whole-body FFM based on weight, gender, height, and impedance, which accurately predicts total FFM in Caucasian morbidly obese adult subjects. The new FFM estimate is not associated with a systematic bias with increasing DXA-FFM. Interestingly, in our study, age was not a significant predictor of FFM. This is in contrast with the equation developed by Horie et al. in morbidly obese subjects using air displacement pletismography (ADP) as a reference method [15]. It is well established that FFM declines with aging in normal weight subjects [19]. However, a previous study by Monda et al. [20] suggests a different behavior in severely obese women, showing a decrease in resting energy expenditure and FFM with aging in lean and moderately obese women (BMI 20.0 to 34.9 kg/m2), but not in severely obese women (BMI > 40 kg/m2). Furthermore, differences in the estimates of FFM between ADP and DXA could also partially explain the different significance of age in our equation as compared to that from Horie et al. [21].
It is well established that fat distribution is an important determinant of cardiovascular risk in obese subjects [2, 3]. Although technical advances make now possible to estimate body fat distribution from BIA [9], our data show that the validity of the FM estimates obtained from the manufacturer's BIA equations is weak. A modest correlation between DXA and BIA estimates of abdominal fatness, with significant underestimation of truncal-FM (as a percent of total body weight) and larger discrepancies with increasing adiposity, has previously been shown in abdominally obese women [11]. Similarly, Sato et al. reported an underestimation and a systematic bias of truncal-FM estimates (expressed in kilograms or as percent of total body weight) when compared with DXA truncal-FM in a group of moderately obese patients [22]. The assumptions made on body build for the BIA estimation of body composition may not be applicable to the morbidly obese population [6, 8], thus underpinning the weak correlation between the parameters obtained from the two methods evaluated in our study.
In the present study, we were able to derive good correlates of truncal-, android-, and gynoid-DXA-FM based on anthropometric and impedance parameters. Notably, the DXA android to gynoid ratio has been associated with several components of the metabolic syndrome in women with a BMI > 35 kg/m2 [2]. Importantly, in the stepwise linear regression analysis in our study population, waist circumference, weight, and hip circumference accounted for 76.3% of the variance of the DXA android fat mass, and the addition of height2/impedance contributed marginally. Likewise, waist and hip circumference together with weight accounted most of the variance of DXA gynoid-FM (70.9%). The addition of height2/impedance added only 6.1% to the DXA gynoid-FM prediction model. This is in sharp contrast with the results that we obtained for total FFM estimates as mentioned previously. Therefore, our findings underscore the importance of anthropometric indices in the evaluation of regional fat distribution also in morbidly obese individuals [2, 23].
We acknowledge that our study has several limitations. First, we used DXA as the reference method for body composition analysis. It has been reported that the use of DXA could result in an overestimation of FM and an underestimation of FFM when compared to a four compartment model of body composition [24, 25]. Second, our study population was predominantly composed of women (78%), only a small proportion was older than 60 years (5%), and all of the participants were Caucasian. Thus, our results do not allow for clarification of potential gender, age, or ethnic specific differences. Third, it could be argued that the efforts made to exclude patients based on medical history and physical examination findings did not allow us to rule out conditions that may have hampered the validity of BIA. In contrast, the strengths of our analysis include the validation of the equations obtained in an independent sample of individuals and the analysis of the clinically relevant aspect of body fat distribution.
In summary, herein we report new equations based on anthropometric parameters and whole-body impedance that allow for good estimates of DXA total FFM and DXA total, truncal-, android-, and gynoid-FM in Caucasian morbidly obese subjects. At a time of increasing prevalence of morbid obesity, the availability of accurate estimates of body composition may facilitate the development of studies relating body composition and health outcomes in morbidly obese subjects.
References
Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US adults, 1999–2008. JAMA. 2010;303:235–41.
Ledoux S, Coupaye M, Essing M, et al. Traditional anthropometric parameters still predict metabolic disorders in women with severe obesity. Obesity. 2010;18:1026–32.
Nordstrand N, Gjevestad E, Dinh KN, et al. The relationship between various measures of obesity and arterial stiffness in morbidly obese patients. BMC Cardiovasc Dis. 2011;11:7.
Das SK. Body composition measurement in severe obesity. Curr Opin Clin Nutr Metab Care. 2005;8:602–6.
Kelly TL, Wilson KE, Heymsfield SB. Dual energy X-ray absorptiometry body composition reference values from NHANES. PLoS One. 2009;4:e7038.
Hull H, He Q, Thornton J, et al. iDXA, Prodigy, and DPXL dual-energy X-ray absorptiometry whole-body scans: a cross-calibration study. J Clin Densitom. 2009;12:95–102.
Kyle UG, Bosaeus I, De Lorenzo AD, et al. Lilienthal Heitmann B, Kent-Smith L, Melchior JC, Pirlich M, Scharfetter H, Schols A, Pichard C, ESPEN. Bioelectrical impedance analysis—part I: review of principles and methods. Clin Nutr. 2004;23:1226–43.
Leal LL, Faintuch J, Morais AA, et al. Bioimpedance analysis: should it be used in morbid obesity? Am J Hum Biol. 2011;23:420–2.
Pietrobelli A, Rubiano F, St-Onge MP, et al. New bioimpedance analysis system: improved phenotyping with whole-body analysis. Eur J Clin Nutr. 2004;58:1479–84.
Coppini LZ, Waitzberg DL, Campos AC. Limitations and validation of bioelectrical impedance analysis in morbidly obese patients. Curr Opin Clin Nutr Metab Care. 2005;8:329–32.
Neovius M, Hemmingson E, Freyschuss B, et al. Bioelectrical impedance underestimates total and truncal fatness in abdominal obese women. Obesity. 2006;14:1731–8.
Alvarez VP, Dixon JB, Strauss BJG, et al. Single frequency bioelectrical impedance is a poor method for determining fat mass in moderately obese women. Obes Surg. 2007;17:211–21.
Peteyjohns I, Brinkworth G, Buckley J, et al. Comparison of three BIA methods with DXA in overweight and obese men. Obesity. 2006;14:2064–70.
Das SK, Roberts SB, Kehayias JJ, et al. Body composition assessment in extreme obesity and after massive weight loss induced by gastric by-pass surgery. Am J Physiol Endocrinol Metab. 2003;284:1080–8.
Horie LM, Barbosa-Silva MC, Torrinhas RS, et al. New body fat prediction equations for severely obese patients. Clin Nutr. 2008;27:350–6.
Tabachnick BG, Fidell LS. Using multivariate statistics. 5th ed. Massachusetts: Allyn and Bacon; 2006.
Sun SS, Chumlea WC. Statistical methods. In: Heymsfield SB, Lohman TG, Wang ZM, Going SB, (eds). Human body composition. Champaign, IL 61825–5076: Human Kinetics 2005:151–60.
Waki M, Kral JG, Mazariegos M, et al. Relative expansion of extracellular fluid in obese vs nonobese women. Am J Physiol. 1991;261:E199–203.
Bosy-Westphal A, Eichhorn C, Kutzer D, et al. The age-related decline in resting energy expenditure in humans is due to the loss of fat-free mass and alteration in its metabolically active components. J Nutr. 2003;133:2356–62.
Monda M, Messina G, Mangoni C, et al. Resting energy expenditure and fat-free mass do not decline during aging in severely obese women. Clin Nutr. 2008;27:657–9.
Lazzer S, Bedogni G, Agosti F, et al. Comparison of dual-energy X ray absorptiometry, air displacement pletismography, and bioelectrical impedance analysis for the assessment of body composition in severely obese Caucasian children and adolescents. Brit J Nut. 2008;100:918–24.
Sato S, Demura S, Kitabayashi T, et al. Segmental body composition assessment for obese Japanese adults by single-frequency bioelectrical impedance analysis with 8-point contact electrodes. J Physiol Anthropol. 2007;26:533–40.
Huxley R, Mendis S, Zheleznyakov E, et al. Body mass index, waist circumference and waist:hip ratio as predictors of cardiovascular risk—a review of the literature. Eur J Clin Nutr. 2010;64:16–22.
Williams JE, Wells JC, Wilson CM, et al. Evaluation of Lunar Prodigy dual-energy absorptiometry for assessing body composition in healthy persons and patients by comparison with the criterion 4-components model. Am J Clin Nutr. 2006;83:1047–54.
Wells JC, Haroun D, Williams JE, et al. Evaluation of DXA against the four-component model of body composition in obese children and adolescents aged 5–21 years. Int J Obes (Lond). 2010;34:649–55.
Acknowledgments
We are thankful to Judith Viaplana for the technical assistance. Grant support was obtained from Fundación Mútua Madrileña.
Disclosure
All contributing authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jiménez, A., Omaña, W., Flores, L. et al. Prediction of Whole-Body and Segmental Body Composition by Bioelectrical Impedance in Morbidly Obese Subjects. OBES SURG 22, 587–593 (2012). https://doi.org/10.1007/s11695-011-0570-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-011-0570-3