
Abstract
Background
Although bariatric surgery is the most common procedure used to induce weight loss in morbidly obese patients, its effect on plasma satiety factors (leptin, ghrelin, and apolipoprotein (apo)-AIV) is controversial. The aim of this work was to analyze these parameters before and at different times after surgery.
Methods
Plasma was obtained from 34 patients before undergoing Roux-en-Y gastric bypass and during weight loss in the 12 months following surgery.
Results
Morbidly obese patients had significantly higher values (147%) of leptin than normal-weight (NW) persons, while their ghrelin levels were 46% less than NW. Apo-AIV levels had approximately the same value in both groups (obese and NW). During weight loss, leptin decreased by 75% and ghrelin increased by 78%. Both parameters reached values less than or near NW, respectively, at 1 year after surgery. During the first month after surgery, apo-AIV plasma levels decreased (47%) but later increased and finally returned to preoperative values. Apo-AIV levels were correlated negatively with leptin and positively with ghrelin. High-density lipoprotein (HDL) levels were positively correlated with those of ghrelin and apo-AIV.
Conclusions
During weight loss, plasma leptin and ghrelin could be good markers of total fat decrease. Ghrelin could also indicate gastric mucous improvement, whereas apo-AIV could indicate the recovery of intestinal function. Changes produced in the HDL levels of morbidly obese patients during weight loss suggest a decreased risk of coronary disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Surgical weight loss approaches are based on intestinal malabsorption and gastric reduction. “Success” has been defined as a maintained weight loss of ≥50% of excess body weight, which in turn is defined as the difference between body weight and ideal weight (for a given patient’s gender and height) [1]. The Roux-en-Y gastric bypass (RYGBP) has become the gold standard of bariatric surgery. It represents a mixed technique, combining restriction derived from leaving a small stomach pouch near the esophagogastric junction by excluding the greater curvature, together with a small malabsorptive component derived from bypassing most of the stomach and duodenum [1].
Leptin and ghrelin are peripheral signals that contribute to the central regulation of food intake. Body mass index (BMI) is the best predictor of circulating leptin concentrations. Unlike total body fat, the amount of upper or lower body adiposity or visceral fat has been found not to influence basal leptin concentrations [2]. Despite the strong correlation between body fat and leptin concentrations, there is great heterogeneity in leptin concentrations for all body fat indices [3, 4].
Leptin, a hormone released by adipocytes, provides information about energy status to hypothalamic regulatory centers [5]. In humans, circulating leptin levels decrease or increase in response to acute caloric shortage or surplus, respectively [6]. There is some evidence linking leptin to direct regulation of adipose tissue metabolism through inhibition of lipogenesis and stimulation of lipolysis [7]. Circulating leptin concentrations are elevated in obesity and decrease after weight loss [8].
Ghrelin, a peptide produced predominantly by the stomach and particularly in the fundus [9], is involved in energy balance regulation. However, in contrast to the anorexigenic effects of leptin, ghrelin stimulates appetite [10]. In human obesity, ghrelin concentrations are low. This might be related to high caloric intake, as body weight reduction in obese patients increases the concentration of ghrelin [8].
The observed reduction of circulating ghrelin concentrations in obese patients at 6 months after RYGBP surgery is not determined by active weight loss or improved insulin sensitivity but rather depends on the surgical bypass of the ghrelin-producing cell population of the fundus [11]. Other investigators have reported that stomach bypass surgery decreases ghrelin concentrations, suggesting that the size of the stomach might correlate directly with ghrelin concentrations [12]. However, other reports have shown a significant increase of serum ghrelin 12 months after biliopancreatic diversion [13]. Some reports have found that insulin is a physiological and dynamic modulator of plasma ghrelin levels and that insulinemia may mediate the effects of nutritional status on ghrelin concentration [14], whereas other reports have shown no relationship between ghrelin levels and other parameters [15]. Following the hypothesis of Cummings et al. [16] that ghrelin has a role in the long-term regulation of body weight, multiple studies have demonstrated increased [12], decreased [17], or unchanged [18] ghrelin levels after weight loss. Recently, it was reported that an immobilized form of ghrelin could specifically bind to different types of HDL associated with plasma sterase, paraoxonase, and clusterin [19].
Human apolipoprotein (apo)-AIV is synthesized and secreted exclusively by the small intestine into enterocytes. The jejunum is the major site of apo-AIV synthesis, but apo-AIV is also produced in the duodenum and ileum. Apo-AIV secretion is stimulated by lipid absorption [20]. Apo-AIV synthesis and secretion into the lymph are associated with chylomicron formation, as digested lipids are processed in mucosal cells. The majority of apo-AIV in the circulation exists as free protein with the remainder associated with circulating HDL [21]. Apo-AIV is also synthesized in the hypothalamus and has been proposed as an important signal for satiety in the central nervous system [22]. The effects of leptin and apo-AIV combine, perhaps synergistically, to reduce food intake [23]. Vergès et al. [24] have demonstrated a strong correlation between plasma apo-AIV and postprandial triacylglyceride (TAG) metabolism in both normoponderal and obese subjects, but these results could not be confirmed by other investigators [25]. Plasma apo-AIV decreases markedly in overweight adolescents undergoing short-term weight reduction, but this decrease is not related to the degree of weight loss, BMI, or plasma leptin. It has been demonstrated that common apo-AIV variants are associated with differences in BMI and body fat percentage [25, 26].
The main objective of this study was to investigate changes in hormone levels (leptin, ghrelin, and insulin) in morbidly obese patients before and after RYGBP and to study the relationship of plasma apo-AIV levels with other components of the lipid plasma profile and anthropometric parameters. We followed the patients’ progress through 1 year of weight loss.
Methods
Patient Selection
A group of 34 morbidly obese patients (24 women and ten men) aged between 27 and 61 years and with a BMI > 40 kg/m2 were recruited from the Vall d’Hebron Hospital in Barcelona, Spain. The obesity criterion was in accordance with the Spanish consensus for the diagnosis of obesity [27]. Sixty-eight percent of patients had metabolic syndrome (Adult Treatment Panel III Criteria).
All subjects were free of inflammatory and infectious diseases and none were receiving anti-obesity or anti-inflammatory drugs at the time of the study. Patients were excluded if they had neoplastic, renal, hepatic, or active systemic diseases, hypothyroidism or endocrine diseases other than diabetes, or if they had been on a restrictive diet during the week previous to the study. All patients reported that their weight was stable during the previous 3 months. None of the diabetic patients were being treated with insulin. The study protocol was reviewed and accepted by the hospital ethics committee and all subjects gave their written informed consent to participate.
For 2 days before the study, all subjects were placed on an isocaloric diet calculated on the basis of individual requirements. The diet was made up of 50% carbohydrates, 20% protein, and 30% fat. Blood samples were taken under fasting conditions at 8:00 and 10:00 am 1 month before surgery (in tables and graphs: OB) and 1, 3, 6, 9, and 12 months after surgery (in tables and graphs: 1M, 3M, 6M, 9M, 12M). Plasma was separated immediately by centrifugation (2,000×g, 30 min, 4°C) and aliquots were frozen at −80°C for subsequent analysis.
After surgery and during the study, the patients’ diet was: during the first month, a liquid diet of 810 kcal/day (45% carbohydrates, 33% protein, and 22% fat); during the second month, a triturated diet of 839 kcal/day (44% carbohydrates, 38% protein, and 18% fat); during the third month, a solid diet of 844.5 kcal/day (41% carbohydrates, 31% protein, and 28% fat); during the rest of the study, the patients were placed on a maintenance diet of 825 kcal/day (44% carbohydrates, 34% protein, and 22% fat).
Seven patients with normal weight were used as controls (in tables and graphs, NW). These patients were euthyroid (12 h fasted), normolipidemic, without digestive system disease, and underwent a laparotomy at the same time as blood was drawn.
Anthropometric and Body Composition Measurements
Body weight, excess weight, height, and waist and hip circumferences were measured according to standard procedures [28]. Weight and height were determined for all subjects, and the BMI was then calculated. Waist circumference was taken midway between the lower rib margin and the iliac crest. Hip circumference was determined as the widest circumference measured on the great trochanter. The waist-to-hip ratio (WHR) was then calculated. The percentage of body fat was calculated from the equation proposed by Deurenberg et al. [29], and the quantity of total subcutaneous and visceral fat was calculated from equations proposed by Bonora et al. [30].
Blood Assays
Insulin levels were determined using an IMMULITE 2500 autoanalyzer (Siemens Medical Diagnostics) in an immunometric chemiluminescent test with two binding sites (noncompetitive) on solid phase. Ghrelin (total: acylated and deacylated) was determined by competitive radioimmunoassay (catalog no H-4864, Peninsula Laboratories, Inc., Bachem, San Carlos, CA, USA) using 125I and a double antibody as markers. This process requires the previous purification and concentration of the sample by chromatography on a Sep-Pak C18 (Waters) column. Leptin was determined by direct competitive radioimmunoassay with a double antibody and 125I as the radioisotope (DRG Instrument GmbH, Germany).
Plasma protein was determined using the method developed by Bradford [31]. Fasting plasma glucose, TAG, nonesterified fatty acid (NEFA), total cholesterol (TC), and high- (cHDL) and low-density (cLDL) lipoprotein cholesterol were measured enzymatically in the hospital’s routine chemistry laboratory. Total HDL quantification was done with a commercial kit for agarose gel electrophoresis (MIDIGEL LIPO Kit made by BIOMIDI, Toulouse, France). The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as previously described [32].
Apo-AIV Western Blot
We ran a single gel for each patient that was loaded with samples from before (obese) and after surgery (during weight loss) and plasma sample from NW as a control. Western blot (WB) assays to detect apo-AIV were run using 10% sodium dodecyl sulfate gel electrophoresis and transferred to Immobilon membranes of Millipore®. IgG anti-human apo-AIV obtained from rabbits in our laboratory was used as the primary antibody at 1/500 dilution (with blocking solution). Several years ago, our group was issued a patent on the use of human apo-AIV antibodies for clinical diagnosis [33]. Horseradish peroxidase (HRP)-conjugated pig anti-rabbit IgG at 1/15,000 dilution (with blocking solution) was used as the secondary antibody (Dako, Glostrup, Denmark). Non-specific binding was prevented using a blocking solution (phosphate-buffered saline (PBS) with bovine serum albumin (BSA)) at 2% (w/v, BSA/PBS). WBs were developed using the SuperSignal WestPico Chemiluminescent substrate for HRP detection (Pierce®, Rockford, IL, USA). Relative quantities were estimated by densitometric scanning (Phoretix 1D gel Analysis Software Non-linear Dynamics, Newcastle, UK).
Statistical Analysis
Results are given as mean ± SEM. Statistical differences between mean values for obese and NW (control) at 1, 3, 6, 9, or 12 months after surgery (weight loss) were assessed using a one-way analysis of variance (ANOVA). Individual comparisons were made using Tukey’s multiple-comparison test. Statistical differences between women and men at different months after surgery (weight loss) were assessed by a two-way ANOVA and Bonferroni posttests. Correlations between independent variables were determined by Spearman’s correlation coefficient (rho). Statistical comparisons were considered significant at p < 0.05.
All statistical analyses were computed using GraphPad Prism version 4.00 software for Windows (GraphPad Software, San Diego CA, USA, https://doi.org/www.graphpad.com).
Results
Clinical Characteristics of Patients
The characteristics of the studied patients are shown in Table 1. The loss of body weight was already significant at 1 month after surgery and weight loss continued until it reached 37% after 1 year. The observed decrease represented a loss of 71% of the excess weight (calculated as the difference between the theoretical ideal weight and the patient’s actual weight), a 27% decrease in the circumference of the waist, a 19% decrease in hip circumference (see Table 1), and a significant decrease in WHR.
Of the total body weight (Table 1), 61% corresponded to fat, and 73% of this percentage corresponded to subcutaneous fat and 27% to visceral fat. The percentage of fat loss during the first 6 months after bariatric surgery was similar for total fat, subcutaneous fat, and visceral fat (39%, 40%, and 38%, respectively). Over the next 6 months, the total fat loss was decreased: 15% of total or visceral fat and 11% of subcutaneous fat. In all cases, the changes were highly significant (Table 1).
Biochemical Plasma Parameters
TC in morbidly obese patients was significantly higher than in NW subjects, but during the first month after surgery this parameter completely recovered to normal levels (Table 2). During weight loss, cHDL remained at similar levels and was even higher than in NW subjects, whereas cLDL levels diminished throughout the months after surgery, reaching even lower values than in control subjects (Table 2). The largest difference was observed in plasma NEFA concentrations, which were twofold higher in morbidly obese patients as compared to NW subjects. NEFA levels even increased during the first month and remained elevated to a similar degree as the initial obese state throughout the study period (Table 2).
Glucose and the insulin levels in the morbidly obese patients were significantly above those of NW subjects (Table 2), but during the first month after surgery the glycemic level diminished to 24% and then remained at that level during the rest of the studied period (Table 2). Insulin diminished by 43% during the first month but after 3 months remained stable for the rest of the study period (Table 2). HOMA-IR reference values considered to represent insulin resistance are around 3.5–3.8 [33]. In the present study, morbidly obese patients had HOMA-IR values more than 3.5-fold higher than those of NW subjects. However, from the first month after bariatric surgery, HOMA-IR decreased by 57% to a point where we considered there was no insulin resistance (Table 2).
Leptin and Ghrelin Levels in Obese Patients Before and After RYGBP
Fig. 1 (top panel) shows that leptin levels in obese patients before surgery was 60% higher than in NW subjects (dotted line in the middle of the shaded zone showing mean ± SEM; 15.0 ± 0.9 ng/ml plasma). At 6 months after surgery, leptin levels had already recovered to NW levels and continued to decrease to approximately 50%.

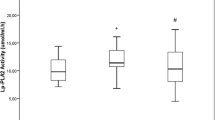
Plasma leptin, ghrelin, and apo-AIV. Results are expressed as mean ± SEM. Statistics were computed using one-way ANOVA and individual comparisons were made using Tukey’s multiple-comparison test between groups. The numbers in the left and right corner of each panel depict the ANOVA result. The results of the apo-AIV graph represent the mean ± SEM densitometry values for all gels (one for each patient) in arbitrary units. The NW value for each graph is indicated by a dotted line in the middle of a shadow zone that indicates mean ± SEM. N = 34 patients for each graph. Symbols denote differences between NW (control) and different groups (c); between obese (OB) and 1, 3, 6, 9, or 12 months (M) after surgery classified by (o), 1M vs. remaining months (1), 3M vs. remaining of months (3). One symbol: p < 0.05; two symbols: p < 0.01; three symbols: p < 0.001
The ghrelin profile (Fig. 1, middle panel) was nearly the opposite of that observed for leptin. The dotted line in the middle of the shaded zone indicates the mean ± SEM for NW values: 132.0 ± 0.3 pg/ml plasma. In obese patients, ghrelin levels were 46% lower than in NW subjects but began to increase only 1 month after surgery. After 1 year, ghrelin levels had recovered completely to NW levels; the difference was significant only at this point due to high variability. The correlation between leptin and ghrelin was negative (rho = −0.16) and significant (p < 0.05).
Leptin levels in obese patients were positively and significantly correlated with the BMI (rho = 0.49, p < 0.01), percentage of body fat (rho = 0.59, p < 0.001) and, to a lesser extent, with subcutaneous fat (rho = 0.44, p < 0.05). Ghrelin levels in the morbidly obese were not correlated with any of these parameters. Thus, where leptin levels were positively and significantly correlated with weight loss in all cases (p < 0.001; Table 3), ghrelin levels were negatively and significantly correlated with weight loss (p < 0.01) only in several cases (Table 3).
Apolipoprotein AIV and HDL Levels in Obese Patients and After RYGBP
The levels of plasma apo-AIV in obese patients (Fig. 1, bottom panel) were similar to those of NW individuals (dotted line in the middle of the shaded zone indicates mean ± SEM; 2.02 ± 0.3 arbitrary units). One month after surgery, however, these apo-AIV levels in obese patients had decreased by 47% and then began to recover gradually until they had returned to NW levels after a year. In obese patients, correlations with other parameters were not observed; however, during weight loss, apo-AIV levels were correlated negatively with those of leptin (rho = −0.33, p < 0.05) and positively with those of ghrelin (rho = 0.89, p < 0.001). Additionally, other correlations were observed for anthropometric or biochemical parameters (Table 3).
In order to verify that apo-AIV and HDL levels were related in obese individuals as described in other studies [20], we used agarose gels (0.5%) dyed with Sudan black (specific for lipids) to detect the total amount of plasma lipoprotein. Fig. 2 shows that the total amounts of HDL and apo-AIV (obtained by Western blotting) were nearly identical. The correlation between both parameters was rho = 0.82 (p < 0.01).

Plasma apo-AIV and HDL. Results represent the mean ± SEM densitometry values for all gels (one for each patient) in arbitrary units. Statistics were computed using one-way ANOVA and individual comparisons were made using Tukey’s multiple-comparison test between groups. The numbers in the top or bottom corner represent ANOVA results for apo-AIV (squares) and HDL (dots), respectively. Arrow shows the application line of plasma. N = 34 patients for each graph. Symbols denote differences between NW (control) and different groups (c); between obese (OB) and 1, 3, 6, 9, or 12 months (M) after surgery classified by (o), 1M vs. remaining months (1), 3M vs. remaining months (3). One symbol: p < 0.05; two symbols: p < 0.01; three symbols: p < 0.001
Discussion
This study presents, for the first time, changes in the plasma profile of several satiety factors as well as lipid parameters for morbidly obese patients receiving RYGBP surgery. The evolution of these factors and parameters was studied for 1 year after surgery, and we observed a recovery towards NW individual levels that was concomitant with the normalization of anthropometric measurements (body weight, body fat, etc.).
It should be noted that bariatric surgery is one of the most effective techniques for weight loss in morbidly obese patients and also makes it possible to quickly recover insulin sensitivity and correct dyslipidemia [34]. In the present study, subjects lost approximately 37% of their body weight in the year after surgery, as well as 47% of their subcutaneous fat and the same amount of visceral fat; correspondingly, HOMA-IR was reduced by 48% in the first month. The use of other techniques, such as individualized diets with simultaneous physical exercise [35] or liquid diets to maintain a “baseline weight” [36], does not improve other co-morbidities. Phillips et al. [37] reported that, 3 months after adjustable laparoscopic gastric banding surgery in obese patients, no improvement in insulin sensitivity was seen despite 20% and 15% reductions of subcutaneous and visceral fat, respectively. Reinehr et al. [38] observed decreased leptin and improved insulin resistance, which we also observed in the present study.
During weight loss, we observed a great improvement in plasma lipid profile (TAG, TC, and cHDL) similar to that described by other investigators [39] for the same type of surgery. In contrast to other studies that did not observe any relationship with decreased BMI, body fat, glucose, triacylglycerides, cholesterol, insulin, or leptin in patients who received RYGBP [40], we observed that all these parameters had changed significantly by 1 month after surgery and continued to change throughout at least the first year after surgery.
Leptin and Ghrelin
Total plasma leptin usually reflects the amount of fat present in the body, and lower levels have been consistently reported in patients losing weight [41]. Our study showed that significant reduction of leptin levels occurred early: 1 month after surgery, when BMI and total adipose tissue were still high but significantly different from the pre-surgical (obese) state. A similar result was reported previously in a 9-month study [34], but we additionally observed that leptin levels continued to decrease up to at least 1 year after surgery. Contrary to other reports [42], leptin levels were correlated with BMI, the total fat percentage, subcutaneous fat, and visceral fat, both in the obese state and after surgery. Moreover, the progressive decrease in plasma leptin levels did not appear to depend on the type of diet or on the number of ingested calories. According to the literature, changes in plasma leptin during weight loss mainly reflect changes in metabolic rate, decreased adipose tissue, decreased size of ingested meals, etc. [43]. Liou et al. [44] recently reported that leptin levels in morbidly obese patients were significantly reduced at 1, 3, 6, and 12 months after laparoscopic minigastric bypass surgery, similar to the present results; however, ghrelin concentrations were not significantly changed after surgery in contrast to our results.
Frübeck et al. [11] found that reduced circulating ghrelin concentrations 6 months after RYGBP surgery were not generated by active weight loss or improved insulin sensitivity but rather by the decreased size of secretory zone of the hormone (the fundus of the stomach) [11]. In our study, the disappearance of a large part of the stomach after RYGBP (the stomach was reduced to about 200 cm3, but a portion of the fundus might have remained active) was likely not enough to result in reduced plasma ghrelin. Additionally, ghrelin levels were lower in morbidly obese patients than in NW subjects but increased to NW levels during weight loss. We therefore consider that loss of the fundus likely did not cause the reduction of ghrelin levels because this effect was not seen at all times studied. Nevertheless, we cannot discard that other intestinal cells could also secrete ghrelin, resulting in a net increase in plasma levels. In the present study, ghrelin levels were significantly correlated not only with weight loss but also with decreased insulin resistance; these results are in accord with previous studies [13, 45].
Although many studies [45, 46] have shown that ghrelin levels are downregulated in human obesity, the existing data on ghrelin levels during weight loss are contradictory. For example, after biliopancreatic diversion surgery, some investigators have observed increased ghrelin levels [13], whereas others observed diminished levels [46]. Still other investigators [47] have found that, during weight loss, ghrelin levels increase by 12% in the first 6 months, whereas in the present study we observed a larger increase (39%) in the same time interval. Other studies did not observe any substantial changes in ghrelin levels during weight loss in children and obese adolescents submitted to a low-fat high-carbohydrate diet, nor did they observe any correlation with insulin levels [39]. In the present study, we observed a negative correlation between ghrelin and leptin or insulin levels.
We also observed significant differences between women and men in plasma leptin at all times after surgery but not in plasma ghrelin. Although women had higher leptin levels than men (p < 0.001), ghrelin levels were similar across genders. Gender explained 23% of the variation in leptin levels; this result was similar that observed by Saad et al. [47].
Apo-AIV and HDL
Few data in the literature describe the relationship between apo-AIV and obesity, and the majority of this work was done in rodents. It was only recently suggested that apo-AIV could act as a satiety factor [22], but current evidence supports an important role in the regulation of food intake [48]. In the present study, morbidly obese patients had apo-AIV levels similar to those of NW individuals, but, as with HDL, levels decreased by 50% within 1 month after surgery. This decrease was not only related to reduced duodenum size, as the duodenum is not the primary source of apo-AIV; rather the observed decrease in apo-AIV was likely the result of the general (not only lipids, which stimulate the apo-AIV secretion) decrease in caloric ingestion [49]. We observed 1 month after surgery that plasma apo-AIV levels began to increase until they reached NW levels. Similarly, HDL levels increased. However, during this period, patients did not increase their lipid ingestion. Therefore, the change in apo-AIV levels might have resulted from increased total intestinal absorption due to increased numbers of enterocytes or development of vellosities. Although not addressed in the present study, our research group has previously described that, in human intestinal atrophy, plasma apo-AIV diminishes [31, 50] due to reduced activity or numbers of enterocytes. The present HDL and apo-AIV data further reinforce the concept that human plasma apo-AIV is synthesized exclusively by the intestine and is at least partly associated with HDL as previously described [51].
Some investigators [25] studying weight loss in children and obese adolescents enrolled in a low-fat diet did not observe any relationship between plasma levels of apo-AIV and TAG; this finding agrees with our data. However, the same study found no correlation between levels of apo-AIV and changes in BMI or plasma leptin; these findings are in contrast to ours.
In ob/ob mice and human small intestine epithelial CACO-2 cells, respectively, Shen et al. [23] and Morton et al. [52] observed decreased apo-AIV levels after leptin administration. We also found a relationship between leptin and apo-AIV levels; women had higher plasma leptin and lower apo-AIV levels, and men showed the opposite.
Thus, circulating leptin levels increase as individuals become more obese, whereas the intestinal apo-AIV response to lipids is attenuated [20]; during weight loss, this situation is inverted. It is possible, as suggested by other investigators, that the effects of leptin and apo-AIV combine, perhaps synergistically, to reduce food intake [23].
In the present study, plasma apo-AIV levels significantly varied between women and men at all times after surgery. Men had higher apo-AIV levels than women (p < 0.05), and gender explained 10% of the variance in plasma apo-AIV levels. Van Aalst-Cohen et al. [53] genotyped a cohort of 1,002 heterozygous familial hypercholesterolemia patients for polymorphisms in the gene encoding apo-AIV and other lipid genes. Multiple linear regressions showed that, together, polymorphisms could explain only 3.9% of the variation in HDL-C plasma levels. Application of a regression model that also incorporated sex, smoking, alcohol use, body mass index, and concomitant beta-blocker use as covariates increased the single-nucleotide-polymorphism-attributed variation of cHDL plasma levels to 32.5% [53]. Recently, a link was suggested between ghrelin and HDL subtypes; some investigators [19] have also proposed a limited number of binding sites for ghrelin in HDL. However, we only observed a good correlation between ghrelin and HDL levels over time. As only one study [19] has thus far examined relationships between these factors in detail, a future extensive study about apo-AIV and HDL levels and their relationship with obesity and cardiovascular diseases is important.
Conclusion
The present study found that morbidly obese patients who underwent the RYGBP procedure to reduce body weight had a greatly improved lipid profile at 1 year after surgery, likely resulting in decreased risk of coronary disease. In addition, they showed decreased resistance to insulin. The study of changes in plasma levels of leptin, ghrelin, and apo-AIV after surgery might allow better diagnosis of fat loss and recovery of gastro-intestinal functionality, which is important for clinical monitoring of patients.
Abbreviations
- HOMA-IR:
-
homeostasis model assessment of insulin resistance
- NEFA:
-
nonesterified fatty acid
- TC:
-
total cholesterol
References
Deitel M. Overview of operations for morbid obesity. World J Surgery 1998;22:913–8.
Gale SM, Castracane VD, Mantzoros CS. Energy homeostasis, obesity and eating disorders: recent advances in endocrinology. J Nutr 2004;134:295–8.
Thomas T, Burguera B, Melton LJ, et al. Relationship of serum leptin levels with body composition and sex steroid and insulin levels in men and women. Metabolism 2000;49:1278–84.
Meier U, Gressner AM. Endocrine regulation of energy metabolism: review of pathobiochemical and clinical chemical aspects of leptin, ghrelin, adiponectin, and resistin. Clin Chem 2004;50:1511–25.
Ahima RS, Saper CB, Flier JS, et al. Leptin regulation of neuroendocrine systems. Front Neuroendocrinol 2000;21:263–307.
Chin-Chance C, Polonsky KS, Schoeller G. Twenty-four-hour leptin levels respond to cumulative short-term energy imbalance and predict subsequent intake. J Clin Endocrinol Metab 2000;85:2685–91.
Wang MY, Lee Y, Unger RH. Novel form of lipolysis induced by leptin. J Biol Chem 1999;274:17541–4.
van’t Dielen FM, van’t Veer C, Buurman WA, et al. Leptin and soluble leptin receptor levels in obese and weight-losing individuals. J Clin Endocrinol Metab 2002;87:1708–16.
Ariyasu H, Takaya K, Tagami T, et al. Stomach is a major source of circulating ghrelin, and feeding state determines plasma ghrelin-like immunoreactivity levels in humans. J Clin Endocrinol Metab 2001;86:4753–8.
van der Lely AJ, Tschöp M, Heiman ML, et al. Biological, physiological, pharmacological pathophysiological, and aspects of ghrelin. Endocr Rev 2004;24:426–57.
Frühbeck G, Rotellar F, Hernandez-Lizoain JL, et al. Fasting plasma ghrelin concentrations 6 months after gastric bypass are not determined by weight loss or changes in insulinemia. Obes Surg 2004;14:1208–15.
Holdstock C, Engström BE, Ohrvall M, et al. Ghrelin and adipose tissue regulatory peptides: effect of gastric bypass surgery in obese humans. J Clin Endocrinol Metab 2003;88:3177–83.
Adami GF, Cordera R, Andraghetti G, et al. Changes in serum ghrelin concentration following biliopancreatic diversion obesity. Obes Res 2004;12:684–7.
Saad MF, Bernaba B, Hwu CM, et al. Insulin regulates plasma ghrelin concentration. J Clin Endocrinol Metab 2002;87:3997–4000.
Krsek M, Rosická M, Haluzík M, et al. Plasma ghrelin levels in patients with short bowel syndrome. Endocr Res 2002;28:27–33.
Cummings DE, Weigle DS, Frayo RS, et al. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Engl J Med 2002;346:1623–30.
Morínigo R, Casamitjana R, Moizé V, et al. Short-term effects of gastric bypass surgery on circulating ghrelin levels. Obes Res 2004;12:1108–16.
Faraj M, Havel PJ, Phélis S, et al. Plasma acylation-stimulating protein, adiponectin, leptin, and ghrelin before and after weight loss induced by gastric bypass surgery in morbidly obese subjects. J Clin Endocrinol Metab 2003;88:1594–602.
Beaumont NJ, Skinner VO, Tan TM, et al. Ghrelin can bind to a species of high density lipoprotein associated with paraoxonase. J Biol Chem 2003;278:8877–80.
Doi T, Liu M, Seeley RJ, et al. Effect of leptin on Intestinal apolipoprotein AIV in response to lipid feeding. Am J Physiol Regul Integr Comp Physiol 2001;281:753–9.
Ghiselli G, Crump WL, Gotto AM. Binding of apo-AIV-phospholipid complexes to plasma membranes of rat liver. Biochem Biophys Res Commun 1986;139:122–8.
Tso P, Liu M. Apolipoprotein A-IV, food intake, and obesity. Physiol Behav 2004;83:631–43.
Shen L, Tso P, Woods SC, et al. Hypothalamic apolipoprotein A-IV is regulated by leptin. Endocrinology 2007;148:2681–9.
Vergès B, Guerci B, Durlach V, et al. Increased plasma apo-AIV level is a marker of abnormal postprandial lipemia: to study in normoponderal and obese subjects. J Lipid Res 2001;42:2021–9.
Lingenhel A, Eder C, Zwiauer K, et al. Decrease of plasma apolipoprotein A-IV during weight reduction in obese adolescents on a low fat diet. Int J Obes Relat Metab Disord 2004;28:1509–13.
Lefevre M, Lovejoy JC, DeFelice SM, et al. Common apolipoprotein A-IV variants are associated with differences in body mass index levels and percentage body fat. Int J Obes Relat Metab Disord 2000;24:945–53.
Sociedad Española para el estudio de la Obesidad (SEEDO). SEEDO’2000 consensus for the evaluation of overweight and obesity and the establishment of criteria for therapeutic intervention. Sociedad Española para el Estudio de la Obesidad. Med Clin 2000;115:587–97.
Lohman TG, Roche AF, Martorell R, editors. Standardization of anthropometric measurements: The Airlie (VA) Consensus Conference. Champaign: Human Kinetics; 1988. p. 20–37.
Deurenberg P, Weststrate JA, Seidell JC. Body mass index as a measure of body fatness: age- and sex-specific prediction formulas. Br J Nutr 1991;65:105–14.
Bonora E, Micciolo R, Ghiatas AA, et al. Is it possible to derive a reliable estimate of human visceral and subcutaneous abdominal adipose tissue from simple anthropometric measurements? Metabolism 1995;44:1617–25.
Bradford MM. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal Biochem 1976;72:248–54.
Matthews DR, Hosker JP, Rudenski AS, et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412–9.
López Tejero MD, Través Polo MC. Diagnostic method of human intestinal atrophy in a given patient of any age. 2002, PCT patent (año 2003), reference: P200201609; registre: exp. 32333. UBAR-Universitat de Barcelona, Centro de Patentes de la Universidad de Barcelona.
Rubino F, Gagner M, Gentileschi P, et al. The early effect of the Roux-en-Y gastric bypass on hormones involved in body weight regulation and glucose metabolism. Ann Surg 2004;240:236–42.
Tintera J, Harantova P, Suchanek P, et al. Quantification of intra-abdominal fat during controlled weight reduction: assessment using the water-suppressed breath-hold MRI technique. Physiol Res 2004;53:229–34.
Schwartz RS, Brunzell JD. Increase of adipose tissue lipoprotein lipase activity with weight loss. J Clin Invest 1981;67:1425–30.
Phillips ML, Lewis MC, Chew V, et al. The early effects of weight loss surgery on regional adiposity. Obes Surg 2005;15:1449–55.
Reinehr T, Roth CL, Alexy U, et al. Ghrelin levels before and after reduction of overweight due to a low-fat high-carbohydrate diet in obese children and adolescents. Int J Obes 2005;29:362–8.
Brolin RE, Kenler HA, Wilson AC, et al. Serum lipids after gastric bypass surgery for morbid obesity. Int J Obes 1990;14:939–50.
Frühbeck G, Diez-Caballero A, Gil MJ, et al. The decrease in plasma ghrelin concentrations following bariatric surgery depends on the functional integrity of the fundus. Obes Surg 2004;14:606–12.
Wallace AM, Sattar N, McMillan DC. Effect of weight loss and the inflammatory response on leptin concentrations in gastrointestinal cancer patients. Clin Cancer Res 1998;4:2977–9.
Minocci A, Savia G, Lucantoni R, et al. Leptin plasma concentrations are dependent on body fat distribution in obese patients. Int J Obes Relat Metab Disord 2000;24:1139–44.
Klok MD, Jakobsdottir S, Drent ML. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: a review. Obes Rev 2007;8:21–34.
Liou JM, Lin JT, Lee WJ, et al. The serial changes of ghrelin and leptin levels and their relations to weight loss after laparoscopic minigastric bypass surgery. Obes Surg 2008;18:84–9.
Kotidis EV, Koliakos G, Papavramidis TS, et al. The effect of biliopancreatic diversion with pylorus-preserving sleeve gastrectomy and duodenal switch on fasting serum ghrelin, leptin and adiponectin levels: is there a hormonal contribution to the weight-reducing effect of this procedure? Obes Surg 2006;16:554–9.
Hansen TK, Dall R, Hosoda H, et al. Weight loss increases circulating levels of ghrelin in human obesity. Clin Endocrinol 2002;56:203–6.
Saad MF, Damani S, Gingerich RL, et al. Sexual dimorphism in plasma leptin concentration. J Clin Endocrinol Metab 1997;82:579–84.
Tso P, Liu M, Kalogeris TJ, et al. The role of apolipoprotein A-IV in the regulation of food intake. Annu Rev Nutr 2001;21:231–54.
Hayashi H, Fujimoto K, Cardelli JA, et al. Fat feeding increases size, but not number, of chylomicrons produced by small intestine. Am J Physiol 1990;259:709–19.
Través C, Coll O, Cararach V, et al. Clinical approach to intestinal maturation in neonates prenatally exposed to alcohol. Alcohol Alcohol 2007;42:407–12.
Duverger N, Ghalim N, Ailhaud G, et al. Characterization of apo-AIV-containing lipoprotein particles isolated from human plasma and interstitial fluid. Arterioscler Thromb 1993;13:126–32.
Morton NM, Emilsson V, Liu YL, et al. Leptin action in intestinal cells. J Biol Chem 1998;273:26194–201.
Van Aalst-Cohen ES, Jansen AC, Boekholdt SM, et al. Genetic determinants of plasma HDL-cholesterol levels in familial hypercholesterolemia. Eur J Hum Genet 2005;13:1137–42.
Funding Source
This research was funded by the Fondo de Investigaciones Sanitarias del Instituto de Salud Carlos III of the Ministerio de Sanidad y Consumo (PI030042, PI030024, and PI0700079). Both R. Llamas and E. Pardina were awarded grants from this institution.
Writing Assistance
English grammar and language have been corrected by American Journal Experts (https://doi.org/www.journalexperts.com).
Conflict of Interest
The authors declare that no conflict of interest exists.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pardina, E., López-Tejero, M.D., Llamas, R. et al. Ghrelin and Apolipoprotein AIV Levels Show Opposite Trends to Leptin Levels During Weight Loss in Morbidly Obese Patients. OBES SURG 19, 1414–1423 (2009). https://doi.org/10.1007/s11695-008-9793-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9793-3