
Abstract
Summary
The main objective of this study was to explore whether vertebral fracture characteristics or posture is independently associated with physical performance. Posture was significantly associated with physical performance but fracture characteristics were not, suggesting posture should be the focus of physical performance variance.
Purpose
The main objective of this study was to explore whether vertebral fracture characteristics (number, severity, location) or occiput-to-wall distance (OWD) is independently associated with physical performance.
Methods
This was a secondary data analysis using baseline data from a randomized controlled trial, of community-dwelling women aged 65 years and older with a suspected vertebral fragility fracture. Lateral thoracic and lumbar spine radiographs were used to determine the number, location, and severity of fracture. The dependent variables were timed up and go (TUG), five times sit-to-stand, four-meter walk, and step test. The independent variables were number, severity, location of fracture, and OWD. Pain during movement and age were covariates. Multivariable regression analyses determined the association between each of the dependent and independent variables.
Results
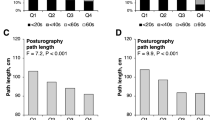
Participants’ (n = 158) mean (standard deviation [SD]) age was 75.9 (6.5) years. They had a mean (SD) BMI, OWD, and number of fractures of 26.7 (5.3) kg/m2, 5.7 (4.6) cm, and 2.2 (1.8), respectively. OWD was independently associated with TUG (estimated coefficient [B] = 0.29, 95% confidence interval [CI] = 0.16, 0.42), five times sit-to-stand (B = 0.33, 95% CI = 0.12, 0.55), four-meter walk (B = 0.09, 95% CI = 0.05, 0.13), and step test (B = − 0.36, 95% CI = − 0.50, − 0.23) in the unadjusted model. OWD was independently associated with TUG (B = 0.25, 95% CI = 0.12, 0.38), five times sit-to-stand (B = 0.29, 95% CI = 0.07, 0.50), four-meter walk (B = 0.08, 95% CI = 0.03, 0.12), and step test (B = − 0.22, 95% CI = − 0.47, − 0.19) in the adjusted model.
Conclusion
OWD was significantly associated with physical performance but fracture characteristics were not. These analyses were exploratory and require replication in future studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vertebral fragility fractures are the most common osteoporotic fracture [1]. The risk of sustaining a vertebral fracture increases with age. The prevalence of vertebral fractures in women aged 50–59 is 5–10%, but it increases to greater than 30% in women over 80 years of age [2]. The risk of future fracture doubles [3, 4] in the year after the initial vertebral fracture [5]. Vertebral fractures lead to further consequences such as back pain [3], reduced physical activity, balance impairments [6], impaired gait [7], height loss [8], and postural changes [9].
The number, severity, and location of vertebral fractures have been associated with head posture, as measured by occiput-to-wall distance (OWD) [10,11,12]. Increased severity of fracture (as measured by the Genant fracture assessment) [13] and number of fractures have been shown to increase OWD [10]. As well, the location of fracture seems to contribute to OWD, such that thoracic vertebral fractures are significantly associated with an increase in hyperkyphosis, which is defined as an increase in the natural thoracic curvature of the spine, and may contribute to postural changes [9]. Individuals with thoracic vertebral fractures had a greater kyphotic angle and OWD than those without thoracic vertebral fractures [13].
Both vertebral fractures and hyperkyphosis have been associated with back pain [11], poor physical function [12], muscle weakness [12], and fear of falling [14], which may contribute to impaired physical performance in individuals with osteoporotic vertebral fractures. Hyperkyphosis has been reported to be an independent risk factor for falls [15], due to a forward shift in the center of mass and center of pressure decreasing stability [7]. It has been proposed that, to counter forward flexion, individuals with hyperkyphosis would create a counterbalance by flexing the knees and tilting the pelvis posteriorly, to bring the head and shoulders back [7]. Example strategies to improve stability during walking include shorter stride length, slower gait velocity, and slower cadence, which create irregular trunk acceleration, decreased static, and dynamic balance [1], and exacerbate instability and fall risk. Incidence of vertebral fractures increases with age [2], and vertebral fractures can result in acute and chronic pain [11]. Individuals in pain adopt forward flexed postures [7], which may contribute further to changes in gait and balance. To date, no studies have explored the independent contributions of number, severity, location of fractures, forward head posture, or pain to physical performance. Understanding if posture contributes to physical performance variability independent of vertebral fracture characteristics would provide support the use of postural interventions among individuals with osteoporotic vertebral fractures, in addition to other pharmacological and non-pharmacological strategies to reduce future fracture risk.
Therefore, the main objective of this study was to explore whether vertebral fracture characteristics, particularly number, severity, location, or OWD, are independently associated with physical performance in a variety of physical performance measures including timed up and go, five times sit-to-stand, four-meter walk, and step test.
Methods
Study design
This exploratory cross-sectional study was a secondary analysis of baseline data from the Build Better Bones with Exercise (B3E) trial. B3E was a one-year, multi-site (seven sites: St. Mary’s Hospital-University of Waterloo, McMaster University, University of Toronto/Toronto General Hospital, Western University/St. Joseph’s Health Care, University of British Columbia, Broadmeadows Health Service in Australia, and Royal Melbourne Hospital/University of Melbourne in Australia), randomized controlled trial of thrice-weekly home exercise compared with control (equal attention) in women aged 65 years or older with at least one, radiographically confirmed, vertebral fracture, [16]. The study protocol has been published (NCT01761084) [16]. For the current study, we used data from participants screened for the inclusion in the B3E randomized control trial.
Outcome measures
We used occiput-to-wall distance (OWD) (cm) to measure forward head posture, a proxy measure for hyperkyphosis [1]. OWD is measured by having the participant stand with their heels and hips flat against a wall. The evaluator measures the distance from the occiput to the wall. OWD has a high correlation (r = 0.902, p < 0.001) with the Flexicurve measure of kyphosis, indicating strong concurrent validity [17]. The sensitivity and specificity of OWD to detect prevalent thoracic fractures encountered in the clinical practice were 41% and 92%, respectively, and an OWD greater than 5 cm is indicative of hyperkyphosis [18]. OWD has strong inter-rater reliability [19].
All participants had lateral thoracic and lumbar spine radiographs in a hospital or clinic by an X-ray technician, unless the participant had a recent (within six months) X-ray as part of usual clinical care. A single musculoskeletal radiologist examined all radiographs to identify the number, location (from T4–L5), and the severity of vertebral fracture(s). Participants were not screened for other potentially confounding spine disorders like scoliosis and ankylosing spondylitis. The radiologist reviewing the X-rays was a musculoskeletal radiologist with fellowship training and 17 years of experience.
Fracture severity
The severity of the fracture was categorized based on the Genant vertebral fracture classification [20], which has a three-point scale classification (grade 1, grade 2, and grade 3). We classified only grade 2 (25–40% compressed) and grade 3 (greater than 40% compressed) fractures as morphometric fractures [21], as we were concerned about the accuracy and reliability of classifying grade 1 fractures (20–25% compressed) [21]. Fracture severity was considered a categorical variable, such that participants were grouped into one of the three categories: grade 0–1 fracture(s), one or more grade 2 fracture(s), or at least one grade 3 fracture. Therefore, individuals with multiple fractures of different severity would be grouped into the highest severity category, regardless of the number of fractures.
Fracture location
We created three fracture location variables based on three regions of the spine: fractures occurring in the mid-thoracic region (T4-8), fractures occurring between the thoracolumbar junction (T9-L1), and in the lumbar region (L2-L5). This was determined based on clinical relevance and previous studies identifying fractures occurring within these locations [8, 9]. If an individual had a fracture in the location, it was coded with a 1 and if there was no fracture in the location it was coded with a zero. For example, a participant with a fracture at T8, T9, and L1 was coded: T4-T8 = 1, T9-L1 = 1, L2-L5 = 0. The location variable was binary, not categorical. This was done to try to avoid addressing the number and location of fractures in the same variable.
Number of fractures
The number of fractures was determined as the number of prevalent grade 2 or 3 fractures for each participant.
Physical assessments
Four physical performance assessments were selected as measures of functional mobility, lower extremity strength and power, and dynamic balance. The timed up and go (TUG) test was selected as a measure of functional mobility, dynamic balance, and obstacle avoidance (by walking around a cone), which have been shown to decrease in individuals with increased postural sway and decreased leg muscle strength [22]. The TUG has shown excellent test-retest reliability [23], inter/intra-rater reliability [24]. The test measures the time it takes for an individual to stand up from a chair, walk three meters, walk back, and sit down in the chair again. A chair of 45-cm height and armrest height of 65 cm was used. A line was marked on the floor three meters from the chair. The participant was instructed to wear their usual footwear. The participant starts with their back against the chair, using their arms resting on the armrests and could use a walking aid if they chose. The participant was instructed to stand up, walk at their usual pace to the line on the floor, turn, return to the chair, and sit down again. The time began when the research assistant told the participant to “go”. If the test was not completed the first time, the test could be repeated. The time is recorded in seconds for the first attempt if it was successfully completed. If a second attempt was required, the time for attempt one and two should be recorded in seconds.
The five times sit-to-stand was selected as a measure of functional lower extremity power and strength [25], with adequate test-retest reliability [26] and adequate construct validity [27]. The participant was initially instructed to perform a single chair stand test to determine the safety of performing the five times sit-to-stand. The participant was seated in a stable chair, 45-cm high and 47.5-cm deep, with a straight back and a solid seat. The participant was asked to stand up from the chair with their arms folded across their chest and feet on the floor. If the participant could not stand without using their arms, they did not perform the five times sit-to-stand. If it was safe to try the five times sit-to-stand, the participant was told to stand up straight as quickly as possible five times, without stopping in between. The participant was asked to keep their arms folded across their chest. The participant was timed from the initial sitting position to the final standing position, at the end of the fifth stand, to see how quickly they could perform five times sit-to-stand. The test was stopped if the participant used their arms or did not completely rise from the chair in 1 min or if there was a concern for the participant’s safety.
The four-meter walk test was selected as a measure of mobility [28], with adequate inter-rater reliability [29] and adequate validity [29]. The step test was selected as an assessment of dynamic balance. A four-meter straight walking path was marked using tape on the floor. A 1-m distance both before and after the four-meter walking path was marked, to minimize the effect of acceleration and deceleration. The participant could use a walking aid if they chose. The test was timed beginning when the first foot crossed the leading edge of the piece of tape that constituted the 4-m line. The timer was stopped when the foot crossed the end of the four-meter marked path. The participant was instructed to walk the distance twice (there and back), and the fastest time was recorded.
Step test has not been validated in patients with osteoporosis but has shown excellent test-retest reliability [30] and inter/intra-rater reliability [31]. The step test is the most challenging balance test of the physical performance assessments in B3E due to the dynamic movement on a single leg stance, while further requiring muscle strength to clear the step [30]. The participant stood unsupported with their shoes removed, feet parallel and 10 cm apart with a block 5 cm directly in front of them. The participant was advised to step with one leg at a time. The participant was instructed to place the whole foot on the block and then to return it fully back down to the floor repeatedly as fast as possible for 15 s. One complete step comprises placing the foot fully up onto then down off the block. The number of steps was recorded. If the participant lost their balance during the test, the number of steps was recorded up to that point and the test was stopped. After the number of steps for one foot was completed, the same procedure was done for the other foot. The number of steps completed in 15 s is recorded for each foot individually; an average number of steps were used in the analysis.
Potential confounding variables that were considered for inclusion in the regression models were age and pain. Pain and age have been shown to contribute to both vertebral fractures and OWD [32]. Pain was assessed using a visual analogue scale (VAS), which asked participants to rate their pain during movement, in the past week, on a scale from 0 to 10, with zero being no pain at all and 10 being unbearable pain. Age was self-reported.
Statistical analysis
All analyses were performed with SPSS version 23 for Windows (IBM SPSS statistics, Armonk, NY). Descriptive statistics, such as age (years), body mass index (kg/m2), height (cm), weight (kg), occiput-to-wall distance (cm), number of fractures, each physical performance measure, number of medications and supplements, and number of comorbidities, were reported as mean and standard deviation. The frequencies of location and severity of vertebral fractures were presented as counts and percentages.
The main objective was to determine the association between vertebral fracture characteristics (number, severity, and location), posture (OWD), and the four physical performance measures (timed up and go, five times sit-to-stand, four-meter walk Test, and step test). Multivariable linear regression analyses were performed with fracture characteristics and OWD as independent variables. Each physical performance test was a dependent variable. A model for the unadjusted and adjusted for age and pain during movement was generated. No variables were removed based on p values as previous work suggests that when determining an association between variables, removing variables based on significance adds bias [33]. In the final models, a p value of < 0.05 was considered statistically significant. Due to the exploratory nature of this study, all variables of interest were forced into the model to gain insight into the associations of the independent variables with the dependent variable. All requisite assumptions were tested.
Results
A total of 181 participants were screened and underwent an X-ray, and 22 (12%) were excluded or withdrew consent and were not included in the current analysis. One participant attended the baseline visit but chose to not participate in the physical performance measures, because she felt unsafe performing the tasks, and was therefore excluded from the analyses. The current analyses were completed using data from 158 participants. The mean (standard deviation) age of the participants was 76 (6.5) years, with a BMI of 26.7 (7.1) kg/m2 (Table 1). On average, participants had 2.2 (1.8) fractures (Fig. 1), with 142 of the participants having a grade 2 or higher fractures. Most of the fractures were in the grade 3 severity category (n = 95) and in the T9–L1 location (n = 107) (Table 1; Fig. 2). The participants had, on average, 2.5 (2.4) comorbidities and were taking 5.3 (4) medications and supplements (Table 1). The average OWD was 5.7 cm (Fig. 3). The mean time for the TUG test was 11.9 (3.9) seconds. For participants that reported using a gait aid, the mean TUG time was 17.93 s (5.1, n = 30), which is above the 13.5 s cutoff score for fall risk (Table 2).

Frequency of fractures, representing the number of participants with the number of fracture ranging from 0 to 8 fractures

Frequency of fractures by location of vertebral fracture, representing the number of participants with a fracture in each location from T1–L5

Frequency of occiput-to-wall distance, representing the number of participants with the distance from their occiput bone to the wall ranging from 0 to 21.5 cm
Timed up and go test
In the unadjusted multivariable regression, 15% of the variance in the TUG was explained by the independent variables (p < 0.001). OWD was the only variable that was significantly associated with TUG (p < 0.001). For every centimeter increase in OWD, TUG time increased by 0.29 s (Table 3). None of the fracture variables were associated with TUG in the unadjusted regression (p > 0.05).
The adjusted multivariable regression model, for the TUG test, was statistically significant (p < 0.001) and accounted for 20% of the variability in TUG. OWD and pain during movement were independently associated with TUG. For every centimeter increase in OWD, TUG time increased by 0.25 s. Age and fracture characteristics were not associated with TUG performance (Table 3).
Five times sit-to-stand test
In the unadjusted multivariable regression model, 13% of the variance in the five times sit-to-stand was explained by the independent variables (p < 0.001). OWD was the only variable that was significantly associated with five times sit-to-stand (p < 0.001). For every centimeter increase in OWD, five times sit-to-stand time increased by 0.33 s (Table 3).
In the adjusted multivariable regression model, 16% of the variance was explained when age and pain during movement were included in the model. OWD was the only variable that was independently associated (p < 0.01) with five times sit-to-stand performance. For every centimeter increase in OWD, five times sit-to-stand test increased by 0.29 s. Although L2-L5 was not statistically significant, the magnitude of the association is large, such that for every fracture in L2–L5, five times sit-to-stand time increased by 2.84 s (Table 3).
Four-meter walk test
The unadjusted multivariable regression model was statistically significant and accounted for 18% of the variability in the four-meter walk test. OWD and fracture severity were statistically significant at p < 0.001 and p = 0.03, respectively (Table 3).
The adjusted multivariable regression model was statistically significant, accounting for 24% of the variability in the four-meter walk test (p < 0.001). OWD (p < 0.001) and fracture severity (p < 0.01) were significantly associated with the four-meter walk test when accounting for pain and age in the model (Table 3).
Step test
The unadjusted multivariable regression model was statistically significant and accounted for 18% of the variability in the step test. OWD was the only variable that was statistically significant in the unadjusted model (p < 0.001), such that for every centimeter increase in OWD, the number of steps decreased by 0.36 (Table 3).
Adjusting for age and pain during movement in the regression model accounted for 21% of the variance in the step test (p < 0.001). OWD and pain during movement were statistically significant explanatory variables, such that for every centimeter increase in OWD, the number of steps decreased by 0.38, and for every grade category increase in fracture severity, step test number decreased by 0.29 steps (Table 3).
Discussion
Our exploratory analyses suggest that OWD explains a greater proportion of variance in physical performance than do fracture characteristics in older women with a suspected vertebral fracture, particularly for the TUG and four-meter walk tests. It is unclear from the current study whether the poor physical performance was a cause or consequence of increased forward flexed posture. The associations between OWD, fracture characteristics, and physical performance measures were weak, suggesting that other factors beyond fracture characteristics and posture contribute to physical performance variability, such as osteoarthritis or neurological disorders. We also noted that the presence of pain during movement may be an important variable to consider when assessing physical performance in women with a suspected vertebral fracture.
Individuals with vertebral fractures may limit their physical activity to attempt to reduce pain [34]. Individuals with lumbar fractures report more severe pain, partially due to the weight-bearing nature of the lumbar vertebrae and the increased moments, shear, and compression forces around those vertebrae [35]. The lumbar vertebrae have a high threshold and slow conduction velocity mechanosensitive afferent units, which may serve as nociceptors in the lumbar facet joints, resulting in low back pain [36]. Pain during movement was significantly associated with performance on the TUG, four-meter walk, step test, and approached statistical significance in the five times sit-to-stand, suggesting that pain may need to be addressed when designing interventions to improve physical performance.
Greater OWD or hyperkyphosis is independently associated with mobility impairments (e.g., slower TUG and four-meter walk time) [1, 7, 37]. Katzman et al. (2011) demonstrated that hyperkyphosis significantly contributed to TUG performance [38], such that per every standard deviation increase in kyphosis angle, TUG time increased by 0.11 s. We demonstrated that for every standard deviation increase in OWD, TUG time increased by 0.32 s. The average TUG time was 11.9 s, and a TUG time of 10 s is a suggested cutoff score indicating risk of falls for individuals with hip osteoarthritis [39], and therefore, 30% of our sample would be classified as at risk of falling using this time cutoff score. Hyperkyphosis may result in balance impairments from a forward flexed posture [1, 6, 37] and gait unsteadiness from an increase in gait variability [7]. In our study, OWD explained more variance in four-meter walk test than other variables known to influence mobility including pain, age, and vertebral fractures. Individuals with osteoporosis and hyperkyphosis typically have slower gait and shorter stride length [37], increasing fall risk. However, 52 participants reported using a gait aid during their daily activities, but only 11 participants used gait aid during the TUG test. Individuals with more variable gait patterns are more cautious [40], contributing to a slower performance time on the TUG and four-meter walk tests.
A sense of instability may result in worse performance on assessments involving lower extremity strength, such as the five times sit-to-stand or the TUG, which was observed in the current study. Individuals with osteoporosis and hyperkyphosis have been shown to have decreased lower extremity strength [6, 12, 37]. Lower extremity strength is associated with an impaired ability to control the center of mass within the base of support, resulting in more mediolateral displacement and greater mediolateral velocity [37]. Individuals with osteoporosis and hyperkyphosis typically demonstrate reduced hip abductor strength, knee extensor strength, ankle dorsiflexion, grip strength [37], and quadriceps strength [41] compared with controls without osteoporosis or hyperkyphosis. OWD was independently associated with five times sit-to-stand performance in both the unadjusted and adjusted models in our study, suggesting that performance variability is linked to lower extremity strength.
Dynamic balance may be impaired in the presence of hyperkyphosis in women with osteoporosis because the center of mass is closer to the edge of the limits of stability. In our study, OWD was shown to modestly contribute to the step test performance, a measure of dynamic balance. A score of less than 10 steps is considered clinically relevant [42], and the average number of steps in our sample was 11.8, but with every standard deviation increase in OWD, the number of steps performed decreased by 0.4, suggesting that an increase in OWD can clinically decrease the ability to perform step test. Older adults have a diminished ability to transfer weight from one leg to the other due to a disruption in the timing of forces being generated and the rate of change [40]. Furthermore, studies by Lynn et al. [6] and Jonsson [40] exhibited that older adults may unload too soon with respect to displacement of the center of mass (COM), leading to more postural adjustments in order to be able to control the COM. In contrast, younger adults demonstrate a longer unloading phase and larger temporal delay between the attainment of the maximal vertical and lateral forces [6, 40]. Thus, it is not surprising that OWD was associated with dynamic balance assessments in our study.
Fracture characteristics were either not associated or modestly associated with physical performance, which is in contrast with findings from previous studies [4, 43]. Discrepant findings may be due to a different grading system for fractures [4] or did not account for posture [43]. For example, the risk of poor performance in the chair stand and walking test was found to increase with an increasing number of fracture (OR = 1.60) [4, 43]. Exercise interventions targeting posture have been shown to improve posture, and our study suggests that we should explore their efficacy for improving physical performance [44].
There were several limitations to this study. Firstly, this was an exploratory nature and therefore the conclusions should be interpreted with caution. Future studies should confirm the findings with larger sample size. The use of OWD to assess hyperkyphosis may not be sensitive enough to detect subtle posture changes; however, OWD represents a cheaper and less burdensome measure of posture for use in a clinical setting. This study was cross-sectional in nature and therefore cannot provide inferences on causality. Future work should examine longitudinal relationships between posture and physical performance in individuals with vertebral fractures. Further, there is strong evidence to suggest that balance is impaired in individuals with hyperkyphosis [13]; however, static balance was not assessed in isolation in this study. The results cannot be generalized to men, and the women in this study may be more physically impaired or present with greater OWD than women without a suspected vertebral fracture. Number, severity, and location were used, in this study, to categorize vertebral fractures; however, whether the anterior, middle, or posterior portion of the vertebral body was compressed was not taken into account.
Conclusion
OWD was significantly associated with each of the physical performance tests measured in this study of older women with suspected vertebral fractures. OWD was statistically significantly associated with TUG, five times sit-to-stand, four-meter walk, and step test, whereas vertebral fracture characteristics were not. Number and severity of fractures were associated with physical performance, in particular, the four-meter walk test, but only explained a modest amount of variance. Future analyses should continue to study the effect with larger sample size.
References
Balzini L, Vannucchi L, Benvenuti F, Benucci M, Monni M, Cappozzo A, Stanhope SJ (2003) Clinical characteristics of flexed posture in elderly women. J Am Geriatr Soc 51(10):1419–1426
Ensrud KE (2013) Epidemiology of fracture risk with advancing age. J Gerontol A Biol Sci Med Sci 68(10):1236–1242
Melton Iii L, Atkinson E, Cooper C, O’Fallon W, Riggs B (1999) Vertebral fractures predict subsequent fractures. Osteoporosis Int 10(3):214–221
van der Jagt-Willems HC, van Hengel M, Vis M, van Munster BC, van Campen JP, Tulner LR et al (2012) Why do geriatric outpatients have so many moderate and severe vertebral fractures? Exploring prevalence and risk factors. Age Ageing 41(2):200–206
Lindsay R, Silverman SL, Cooper C, Hanley DA, Barton I, Broy SB et al (2001) Risk of new vertebral fracture in the year following a fracture. J Am Med Assoc 285(3):320–323
Lynn SG, Sinaki M, Westerlind KC (1997) Balance characteristics of persons with osteoporosis. Arch Phys Med Rehabil 78(3):273–277
De Groot MH, van der Jagt-Willems HC, van Campen JPCM, Lems WF, Beijnen JH, Lamoth CJC (2014) A flexed posture in elderly patients is associated with impairments in postural control during walking. Gait Posture 39(2):767–772
Siminoski K, Warshawski RS, Jen H, Lee K (2003) Accuracy of physical examination using the rib-pelvis distance for detection of lumbar vertebral fractures. Am J Med 115(3):233–236
Cortet B, Roches E, Logier R, Houvenagel E, Gaydier-Souquières G, Puisieux F, Delcambre B (2002) Evaluation of spinal curvatures after a recent osteoporotic vertebral fracture. Joint Bone Spine 69(2):201–208
Kado DM, Miller-Martinez D, Lui L, Cawthon P, Katzman WB, Hillier TA et al (2014) Hyperkyphosis, kyphosis progression, and risk of non-spine fractures in older community dwelling women: the Study of Osteoporotic Fractures (SOF). J Bone Miner Res 29(10):2210–2216
Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ III (1992) Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985-1989. J Bone Miner Res 7(2):221–227
Liu-Ambrose T, Eng JJ, Khan KM, Carter ND, McKay HA (2003) Older women with osteoporosis have increased postural sway and weaker quadriceps strength than counterparts with normal bone mass: overlooked determinants of fracture risk? J Gerontol Ser A Biol Sci Med Sci 58(9):862–866
Siminoski K, Warshawski RS, Jen H, Lee K (2011) The accuracy of clinical kyphosis examination for detection of thoracic vertebral fractures: comparison of direct and indirect kyphosis measures. J Musculoskelet Neuronal Interact 11(3):249–256
Baert V, Gorus E, Mets T, Bautmans I (2015) Motivators and barriers for physical activity in older adults with osteoporosis. J Geriatr Phys Ther 38:105–114
Kado DM, Huang MH, Nguyen CB, Barrett-Connor E, Greendale GA (2007) Hyperkyphotic posture and risk of injurious falls in older persons: the Rancho Bernardo Study. J Gerontol A Biol Sci Med Sci 62(6):652–657
Giangregorio LM, Thabane L, Adachi JD, Ashe MC, Bleakney RR, Braun EA, Cheung AM, Fraser LA, Gibbs JC, Hill KD, Hodsman AB, Kendler DL, Mittmann N, Prasad S, Scherer SC, Wark JD, Papaioannou A (2014) Build better bones with exercise: protocol for a feasibility study of a multicenter randomized controlled trial of 12 months of home exercise in women with a vertebral fracture. Phys Ther 94(9):1337–1352
Wongsa S, Amatachaya P, Saengsuwan J, Amatachaya, S (2012) Concurrent validity of occiput-wall distance to measure Kyphosis in communities. J Clin Trials, 2(10.4172), 2167–0870
van der Jagt-Willems HC, de Groot MH, van Campen JP, Lamoth CJ, Lems WF (2015) Associations between vertebral fractures, increased thoracic kyphosis, a flexed posture and falls in older adults: a prospective cohort study. BMC geriatrics, 15(1), 34
Shipe NK, Billek-Sawhney B, Canter TA, Meals DJ, Nestler JM, Stumpff JL (2013) The intra-and inter-rater reliability of the tragus wall distance (TWD) measurement in non-pathological participants ages 18–34. Physiother Theory Pract 29(4):328–334
Genant HK, Jergas M, Palermo L, Nevitt M, San Valentin R, Black D et al (1996) Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis. J Bone Miner Res 11(7):984–996
Johansson H, Odén A, McCloskey E, Kanis J (2014) Mild morphometric vertebral fractures predict vertebral fractures but not non-vertebral fractures. Osteoporosis Int 25(1):235–241
Podsiadlo D, Richardson S (1991) The timed ‘Up and Go’: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39(2):142–148
Kennedy DM, Stratford PW, Wessel J, Gollish JD, Penney D (2005) Assessing stability and change of four performance measures: a longitudinal study evaluating outcome following total hip and knee arthroplasty. BMC Musculoskelet Disord 6(1):3
Wright AA, Cook CE, Baxter GD, Dockerty JD, Abbott JH (2011) A comparison of 3 methodological approaches to defining major clinically important improvement of 4 performance measures in patients with hip osteoarthritis. J Orthop Sports Phys Ther 41(5):319–327
Meretta BM, Whitney SL, Marchetti GF, Sparto PJ, Muirhead RJ (2006) The five times sit to stand test: responsiveness to change and concurrent validity in adults undergoing vestibular rehabilitation. J Vestibular Res Equilib Orientat 16(4–5):233–243
Tiedemann A, Shimada H, Sherrington C, Murray S, Lord S (2008) The comparative ability of eight functional mobility tests for predicting falls in community-dwelling older people. Age Ageing 37(4):430–435
Lord SR, Murray SM, Chapman K, Munro B, Tiedemann A (2002) Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J Gerontol Ser A Biol Med Sci 57(8):M539–M543
Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, Scherr PA, Wallace RB (1994) A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 49(2):M85–M94
Kim HJ, Park I, Lee HJ, Lee O (2016) The reliability and validity of gait speed with different walking pace and distances against general health, physical function, and chronic disease in aged adults. J Exerc Nutr Biochem 20(3):46–50
Hill KD, Bernhardt J, McGann AM, Maltese D, Berkovits D (1996) A new test of dynamic standing balance for stroke patients: reliability, validity and comparison with healthy elderly. Physiother Can 48(4):257–262
Hong S, Goh EY, Chua SY, Ng SS (2012) Reliability and validity of step test scores in subjects with chronic stroke. Arch Phys Med Rehabil 93(6):1065–1071
Antonelli-Incalzi R, Pedone C, Cesari M, Di Iorio A, Bandinelli S, Ferrucci L (2007) Relationship between the occiput-wall distance and physical performance in the elderly: a cross sectional study. Aging Clin Exp Res 19(3):207–212
Sun G, Shook TL, Kay GL (1996) Inappropriate use of bivariable analysis to screen risk factors for use in multivariable analysis. J Clin Epidemiol 49(8):907–916
Liu-Ambrose T, Eng JJ, Khan KM, Mallinson A, Carter ND, McKay HA (2002) The influence of back pain on balance and functional mobility in 65- to 75-year-old women with osteoporosis. Osteoporosis Int 13(11):868–873
Briggs AM, Wrigley TV, Van Dieën JH, Phillips B, Lo SK, Greig AM et al (2006) The effect of osteoporotic vertebral fracture on predicted spinal loads in vivo. Eur Spine J 15(12):1785–1795
Yamashita T, Minaki Y, Oota I, Yokogushi K, Ishii S (1993) Mechanosensitive afferent units in the lumbar intervertebral disc and adjacent muscle. Spine 18(15):2252–2256
Sinaki M, Brey RH, Hughes CA, Larson DR, Kaufman KR (2005) Balance disorder and increased risk of falls in osteoporosis and kyphosis: significance of kyphotic posture and muscle strength. Osteoporosis Int 16(8):1004–1010
Katzman WB, Vittinghoff E, Kado DM (2011) Age-related hyperkyphosis, independent of spinal osteoporosis, is associated with impaired mobility in older community-dwelling women. Osteoporosis Int. 22(1):85–90
Arnold CM, Faulkner RA (2007) The history of falls and the association of the timed up and go test to falls and near-falls in older adults with hip osteoarthritis. BMC Geriatr 7(1):1
Jonsson E (2006) Effects of healthy aging on balance: A quantitative analysis of clinical tests. Institutionen för klinisk neurovetenskap, arbetsterapi och äldrevårdsforskning (NEUROTEC)/Department of Clinical Neuroscience, Occupational Therapy and Elderly Care Research (NEUROTEC)
Herman T, Giladi N, Gurevich T, Hausdorff JM (2005) Gait instability and fractal dynamics of older adults with a "cautious" gait: why do certain older adults walk fearfully? Gait Posture 21(2):178–185
Blennerhassett JM, Dite W, Ramage ER, Richmond ME (2012) Changes in balance and walking from stroke rehabilitation to the community: a follow-up observational study. Arch Phys Med Rehabil 93(10):1782–1787
Pluijm S, Tromp A, Smit J, Deeg D, Lips P (2000) Consequences of vertebral deformities in older men and women. J Bone Miner Res 15(8):1564–1572
Bansal S, Katzman WB, Giangregorio LM (2014) Exercise for improving age-related hyperkyphotic posture: a systematic review. Arch Phys Med Rehabil 95(1):129–140
Funding
The research was funded by a CIHR Operating grant (MOP: 123445). Dr. Giangregorio received funding from an Ontario Ministry of Health Research and Innovation- Early Researcher Award, CIHR New Investigator Award, the Canadian Foundation for Innovation, and the Bloomberg Manulife Prize. Dr. Ashe acknowledges the support of the Canada Research Chairs program. Dr. Cheung is supported by a Tier 1 CRC in Musculoskeletal and Postmenopausal Health as well as the Lillian Love Chair in Women’s Health at the University of Toronto and University Health Network. Dr. Gibbs received funding from a CIHR Fellowship Award.
Author information
Authors and Affiliations
Contributions
Christina M.D. Ziebart, Jonathan D. Adachi, Maureen C. Ashe, Robert R. Bleakney, Angela M. Cheung, Jenna C. Gibbs, Keith D. Hill, David L. Kendler, Aliya A. Khan, Sandra Kim, Caitlin McArthur, Nicole Mittmann, Alexandra Papaioannou, Sadhana Prasad, Samuel C. Scherer, Lehana Thabane, John D. Wark, and Lora M. Giangregorio have all provided meaningful contributions to this manuscript.
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ziebart, C., Gibbs, J.C., McArthur, C. et al. Are osteoporotic vertebral fractures or forward head posture associated with performance-based measures of balance and mobility?. Arch Osteoporos 14, 67 (2019). https://doi.org/10.1007/s11657-019-0626-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-019-0626-x