
Abstract
Several factors increase the risk of fragility fracture, including low bone mineral density, falls, and poor physical performance. The associations among these factors have been investigated; however, most of the subjects of previous studies were either elderly men or elderly women, and the associations were controversial. The aim of this study was to evaluate the associations between physical performance and bone mineral density, and the history of falls and fractures, stratified by gender and age group. We analyzed 5368 subjects who were aged 50 years or older, including 1288 younger men (younger than 70 years), 1615 younger women (younger than 70 years), 1087 older men (70 years or older), and 1378 older women (70 years or older). We used the one-leg standing time (OLST) for assessing static balance and the timed up-and-go test (TUGT) for assessing dynamic balance. The subjects in the worst performance quartile for the OLST were more likely to have osteoporosis than those in the best performance quartile. Additionally, women who had experienced a fracture during the past 2 years were 1.68 times more likely to be in the worst performance quartile for the OLST than women without a previous fracture. Although the TUGT time was not associated with either the incidence of osteoporosis or the fracture history, the odds ratios for falling were 1.51 and 1.28 as the TUGT time increased by one standard deviation in younger men and younger women, respectively. The findings of the present study show that the OLST was associated with the incidence of osteoporosis and previous fracture and that the TUGT time was associated with the incidence of falling.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The prevalence of osteoporosis and osteoporotic fracture is dramatically increasing owing to the rapid aging of the population in most developing and developed countries [1, 2]. In South Korea, the prevalence of osteoporosis is 8.8 and 39.1 % in men and menopausal women, respectively, aged 50 years or older [3]. Although the number of patients receiving care for osteoporosis has gradually increased (1.07 million, 1.20 million, and 1.33 million people in 2005, 2006, and 2007, respectively), the recognition of and treatment rates for osteoporosis are relatively lower than those of other chronic diseases [4, 5]. Low bone mineral density (BMD) can be used as the primary indicator of the risk of osteoporotic fractures [6]. Low BMD is correlated with low physical function, as poor physical function reduces mechanical loading and leads to a loss of BMD [7]. Although the assessment of bone strength is considered essential to provide an indication of a subject’s risk of osteoporotic fracture, the propensity to fall has also been recognized as an important predictor of osteoporotic fractures [8]. Therefore, decreased balance is also an important risk factor for fractures [6] because falls can be caused by mobility impairments, such as gait and balance disorders [9].
Several reports have analyzed the relationships among BMD, physical performance, falls, and fractures. A higher BMD has a tendency to correlate with better physical performance, although some studies have shown that this relationship depends on sex, race, and body compartment [10]. Additionally, there are several reports describing decreased balance and physical function a few years after a fracture [11, 12]. Most studies evaluating the relationship between physical performance and bone quality have focused on either elderly men or elderly women, because the body composition, hormonal status, and patterns of physical activity differ between genders and among age groups. Various assessment techniques measure physical performance in older adults. One of these techniques measures postural sway during quiet standing to quantify static balance. Another approach measures the ability to anticipate changes and coordinate muscle activity in response to perturbations of stability to quantify dynamic balance [13]. We chose the one-leg standing time (OLST) to evaluate static balance, and the timed up-and-go test (TUGT) to evaluate dynamic balance [14, 15]. The aim of this study was to determine which performance measures could predict the risk of osteoporosis, falls, and fractures in Korean subjects. We evaluated the associations between the time taken to perform each measure and the incidence of osteoporosis, falls during the past 12 months, and fractures in the past 2 years. The subjects were stratified by gender and age group for the analyses.
Materials and methods
Study population
The Chungju Metabolic Disease Cohort (CMC) study is an ongoing community-based study of metabolic diseases, including diabetes, metabolic syndrome, and osteoporosis, in a population aged 40 years or older living in the rural area of Chungju City, Korea. The details of the CMC study are described elsewhere [16]. The baseline examination with dual-energy X-ray absorptiometry was performed from May 2007 to March 2011 on 2513 men and 4090 women who were selected by stratified random cluster sampling. We excluded (1) women in the premenopausal or perimenopausal state or with a history of hysterectomy or unilateral oophorectomy, (2) men younger than 50 years, and (3) individuals using medications known to influence bone metabolism within the past 2 years (e.g., corticosteroids, bisphosphonates, calcium supplements, and hormone replacement therapy). Menopause was defined as the absence of menstruation for at least 12 months. The remaining 5466 subjects (2375 men and 2993 women) were analyzed in this study. We stratified the participants on the basis of age (younger group, younger than 70 years; older group, 70 years or older) and gender (men, women). The institutional review board at the Catholic University of Korea approved this study (no. KC14EASI0230). Written informed consent was obtained from all participants.
Measurements
Physical performance measures
Two measures were used to assess physical performance: OLST and TUGT. Time was measured using a stopwatch and rounded to the nearest tenth of a second.
OLST: The subjects were allowed to practice before testing and were free to choose which leg they preferred to lift since only one leg was tested [17]. The participant stands on the preferred leg with the opposite leg raised while the time is recorded in seconds, stopping when the participant touches any supporting surface. The test was performed twice, and the longest trial time was recorded. The maximum time counted was 30 s per trial. As shown in other studies, the OLST is a widely used clinical tool for assessing static balance and has good reliability for assessing both cognitive and physical functions [15, 18, 19].
TUGT: The patient rises from a chair, walks 3 m, turns around, returns to the chair, and sits down. The test was repeated two times, and the shortest time was recorded. As shown in other studies, the TUGT is a clinical method for assessing dynamic balance [14] and has high test–retest reliability [20] and excellent intrarater and interrater reliability [21].
Bone density measurements
The BMD of the lumbar spine, femoral neck, and total hip was measured in grams per square centimeter using dual-energy X-ray absorptiometry (QDR-4500C, Hologic, Waltham, MA, USA). According to the manufacturer, the coefficient of variation used for precise assessment of the BMD measurements was 1.23 % for the lumbar spine, 2.3 % for the femoral neck, and 1.0 % for the total hip. In accordance with the WHO criteria, osteoporosis was defined as having a T-score of −2.5 or less at the lumbar spine (L1–L4), femoral neck, or total hip. Osteopenia was defined as having a T-score of between −1 and −2.5 at the lumbar spine (L1 L4), femoral neck, or total hip. Owing to the absence of national guidelines for South Korea, the reference data used to determine the T-scores were reference values for the Japanese population provided by Hologic.
Other assessments
Weight and height were measured with the participants wearing light clothes at the time of the bone densitometry measurements. The body mass index (BMI) was calculated as body weight (kg)/height (m2). During the investigation, standardized questionnaires were used to obtain demographic characteristics, medical history, and lifestyle behavior data. Data on whether the participants were currently smoking (yes/no), consuming alcohol (yes/no), and performing exercise at least once a week (yes/no) were collected. The experience of falls was also investigated, and the subjects who had fallen within the year before this study were referred to as “fallers.” The fracture history, which includes age at the time of fracture, fracture location, and fracture cause, was obtained from each participant. A clinically prevalent fracture was present if the fracture occurred because of low-energy trauma (falling from standing height or lower) after the age of 50 years. All fractures that were considered nonosteoporotic (i.e., fractures due to cancer or an accident and all fractures of the fingers, faces, skull, and toes) were excluded. The total energy and dietary calcium intakes were estimated from a 98-item semiquantitative food frequency questionnaire that has been validated previously [22].
Statistical analysis
Baseline characteristics are expressed as the mean ± the standard deviation for continuous variables and the number and percentage for categorical variables. Stratification by both gender and age group was performed because of known differences in physical capacity between genders and age groups. The age-group stratification was based on the mean age of each gender. To compare the principal characteristics of the study subjects among the four groups, ANOVA for continuous variables and the chi square test for categorical variables were used. To determine whether test times were associated independently with BMD at various sites, a multiple regression model was used that made adjustments for age, gender, and BMI. The time taken to perform each test was divided into quartiles of the population (lower quartile represents better performance). The physical performance quartiles were gender specific and age group specific, as all data were stratified by gender and age group. To examine the association between physical performance and the risk of osteoporosis, the subjects were classified as having osteoporosis, on the basis of a sex-specific T-score, or not having osteoporosis. First, gender- and age-group-specific univariate logistic regressions were performed with bone density (osteoporotic/nonosteoporotic) as the outcome variable to estimate odds ratios with 95 % confidence intervals (CIs). Second, multivariate logistic regression analyses adjusted for all covariates that were significant in the univariate analysis were performed. Third, the subjects were classified into four groups (groups 1–4) according to their combined performance measures to determine whether there was an additive relationship between the two measures for predicting the risk of osteoporosis. To examine the association between physical performance and the risk of falling, gender- and age-group-specific multivariate logistic regressions were performed after adjustment for all associated covariates. To determine the relationship between physical performance and previous fractures, univariate logistic regression was performed with physical performance (lowest-performance/non-lowest-performance group based on the quartile of each performance measure) as the outcome variable. Next, a multivariate logistic regression analysis that adjusted for all covariates that were significant in the univariate analysis was performed. All analyses were two-tailed and SAS version 9.3 (SAS Institute, Cary, NC, USA) was used. Results with p values less than 0.05 were considered statistically significant.
Results
Baseline characteristics of the study population
The baseline characteristics of the subjects stratified by gender and age are shown in Table 1. We stratified the subjects into an older group (70 years or older) and a younger group (younger than 70 years) on the basis of the mean age of each gender group (men, 67.6 years; women, 67.8 years). After stratification by gender and age group, the mean ages were 61.6 years for the younger men, 61.8 years for the younger women, and 74.8 years for the older men and women. Weight, height, BMI, OLST, TUGT time, dietary calcium intake, percentage of subjects with osteoporosis, current drinking, and the occurrence of any falls during the past 12 months were significantly different among the four groups. Older women had the lowest physical performance and the highest percentage of osteoporosis (71.2 %). This group also had a higher number of pregnancies (6.6 ± 2.4) and a longer time since menopause (27.1 ± 6.5 years) than younger women. Compared with men, more women did not exercise and had experienced at least one fracture during the past 2 years.
Association of physical performance with the BMD at various skeletal sites and the risk of osteoporosis
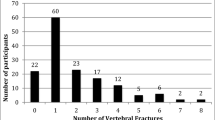
After adjustment for age and BMI, the BMDs of all measured skeletal sites were associated with the OLST and the TUGT time in the younger men. The BMDs of the femoral neck and total hip were associated with the OLST in the younger women and the TUGT time in the older women (Table 2). When the subjects were grouped into four groups according to the time taken to perform each test, the association between the OLST and the incidence of osteoporosis persisted after adjustment for all covariates (p < 0.05) in univariate analyses. Younger men, younger women, and older men in the highest quartile for the OLST were 1.67 times (95 % CI 1.06–2.66, p = 0.029), 1.59 times (95 % CI 1.12–2.24, p = 0.009), and 2.01 times (95 % CI 1.22–3.31, p = 0.006), respectively, more likely to have osteoporosis than those in the lowest quartile. The odds ratios were 1.24 (95 % CI 1.03–1.48, p = 0.020), 1.15 (95 % CI 1.11–1.30, p = 0.038), and 1.20 (95 % CI 1.01–1.43, p = 0.042) as the OLST decreased by one standard deviation in younger men, younger women, and older men, respectively. Although the TUGT time alone was not associated with the incidence of osteoporosis in either univariate or multivariate analysis, younger men, younger women, and older men in the highest quartile for both measures (group 4) were more likely to have osteoporosis than those in the highest quartile for the OLST alone (group 3) (Table 3). Additionally, the rate of osteoporosis seemed to increase as the TUGT quartile increased in the subjects in the same OLST performance quartile (Fig. 1). Subjects in the highest quartile for the TUGT and the second or third quartile for the OLST were 1.62 times (95 % CI 1.07–2.44, p = 0.022) to 1.66 times (95 % CI 1.10–2.50, p = 0.016) more likely to have osteoporosis than those in the lowest quartile for the TUGT (Table 4).

The rate of osteoporosis according to the quartiles of both the one-leg standing time (OLST) and the timed up-and-go test (TUGT). The rate of osteoporosis increased as the TUGT quartile increased in the subjects in the same OLST performance quartile
Association between physical performance and falls
Younger men and women in the highest quartile for the TUGT were 3.05 times (95 % CI 1.67–5.57, p < 0.001) and 2.46 times (95 % CI 1.46–4.17, p = 0.001) more likely to have experienced a fall within the last 12 months than those in the lowest quartile. The odds ratios were 1.51 (95 % CI 1.28–1.78, p < 0.001) and 1.28 (95 % CI 1.11–1.48, p = 0.001) as the TUGT time increased by one standard deviation in younger men and younger women, respectively. However, the association between the OLST and the fall incidence during the past 12 months was diminished after adjustment for other covariates. Younger men and women in the highest quartile for both measures (group 4) were more likely to have fallen than those in the highest quartile for the TUGT only (group 3) (Table 5). Further logistic regression analysis of the falling incidence according to the TUGT quartiles stratified by the OLST quartiles showed no association (data not shown).
Association between physical performance and previous fractures
The association between physical performance and previous fractures was investigated only in women because of the low prevalence of fracture during the past 2 years in men (Table 1). The proportion of women in the highest quartile for the OLST was significantly higher among women with a previous fracture than among those without a previous fracture (p = 0.015). However, among the women in the highest quartile for the TUGT, the proportions of participants with and without a previous fracture were similar (Table 6). Therefore, a further analysis was performed with the subjects in the highest quartile for the OLST as the only outcome variable. Women with a previous fracture, advanced age, diabetes, current smoking status, lack of exercise, and long postmenopausal duration (19 years or more) were more likely to be in the highest performance quartile for the OLST. After adjustment for all covariates that were significant (p < 0.05) in the univariate analyses, women with a previous fracture were 1.68 times more likely to be in the highest performance quartile for the OLST than women without a fracture (95 % CI 1.076–2.628, p = 0.023) (Table 7).
Discussion
We stratified the participants into four groups on the basis of gender and age group. The mass, quality, and function of both muscle and bone show a parallel decline with age [23], and these features are quite different between genders [24]. Bone responds to local mechanical forces, adapting to usual, everyday strain, which is likely reflected in measures of physical performance [25]. However, the relationship between BMD and physical performance is unclear and depends on sex, race, and body compartment [7, 10, 26]. Therefore, both age and gender should be taken into account when studying the relationship between physical performance and BMD.
We evaluated the association between physical performance and BMD across the measured sites after adjustment for age and BMI. We showed that there were different associations between the physical performance measures and the BMD of various skeletal sites according to the gender and age group. In women, the physical performance seemed to have a stronger relationship with the BMD of hip than with that of the spine. This result is consistent with a previous report that the relationship between OLST and BMD was stronger in the hip than in the spine in 606 older Finnish women [10, 27]. The hip bone has a significant cortical compartment. For the femur, long-term weight-bearing physical activity has been associated with a greater total and cortical bone area and cortical bone mineral content [28]. Individuals who can stand on one leg for longer periods of time may have not only better static balance but also more muscle mass and greater muscle strength around the hip. This increased muscle loading may lead to higher BMD. In men, physical performance was significantly related to the BMD in younger men, but not in older men. This result is consistent with another study that focused on 3041 subjects aged 70–79 years, which demonstrated that the relationship between physical performance and the BMD of the femoral neck was significant in women but not in men. These findings suggest the possibility that women have higher rates of disability than men in a given age group, which affects function in body systems and actions [7, 29]. However, we could not find another study evaluating the relationship between physical performance and BMD in men aged 50–70 years.
We evaluated the association between physical performance and the risk of osteoporosis after adjustment for all covariates. In all of the subjects except the older women, a shorter OLST was associated with an increased incidence of osteoporosis. In one study, physical activity, mainly consisting of light household tasks, is associated with reduced 6-year fracture risk. However, physical performance including one-leg standing was not related to bone quality or fracture risk in older women (mean age 75.8 ± 6.6 years) [26]. Another study showed that daily walking steps had a stronger association than the maximal walking speed with bone mineral status measured by quantitative ultrasound assessment in the right heel of Japanese women aged 75 years or older. Daily walking steps represents the level of physical movement in daily life, but it does not reflect mobility capability [30]. In this regard, it could be assumed that BMD is more strongly associated with daily physical activity than maximal physical performance in women older than 70 years. In contrast to the younger women, the older women in our study showed no association between OLST and the risk of osteoporosis. In addition, hip BMD of the older women was associated with the TUGT time, although that of the younger women was associated with OLST. Therefore, in our older women, it could be supposed that the TUGT time was associated with daily life activities, whereas OLST was not. However, we could not demonstrate these relationships between daily life activities with both physical performances, because daily life activities were not measured in this cohort study.
In our study, the TUGT time alone was not associated with the incidence of osteoporosis. However, subjects in the highest quartile for both the TUGT and the OLST were more likely to have osteoporosis than those in the highest quartile for the OLST alone. This result suggests that the TUGT time in combination with the OLST provides a better prediction of the risk of developing osteoporosis. The TUGT time has been independently associated with BMD in previous studies, but the subjects were not Asian, and instead included 484 Moroccan women aged 55.1 ± 9.6 years [12], 1126 Australian women older than 70 years [31], and 104 Australian postmenopausal women aged 71.3 ± 5.8 years [32]. To our knowledge, only one study has focused on the relationship between BMD and physical performance, comparing the TUGT time and the OLST in community-dwelling Asians (90 Japanese women whose mean age was 54.7 years). The OLST was a significant factor associated with BMD in the elderly, although the TUGT time was not [33]. Because the relationship between BMD and physical performance depended on race [10], the TUGT appeared to have a minor but additive role in identifying Asian people at a high risk of osteoporosis.
The fall history during the past 12 months was significantly associated with the TUGT time, but not with the OLST. This result is consistent with a previous study that showed the TUGT time predicted the occurrence of falling, in contrast to the OLST, in Taiwanese people aged 65 years or older [34]. The TUGT was developed to quantify dynamic balance of the senior population and has been used widely to screen for fall risk in community-dwelling seniors by assessing gait and balance [35–37]. However, there has been controversy about its ability to screen seniors at risk of falling, particularly in a healthy and highly functioning population [38]. In contrast, the present study showed that the TUGT time was associated with falls during the past 12 months in younger subjects, who were relatively healthier than older subjects. One possibility is that the unbalanced gait of the older subjects in our study might have been concealed by the TUGT [39]. The occurrence of previous falls is considered the gold standard for predicting future falls, so screening for the risk of falling during the clinical examination begins with determining whether the patient has fallen in the past year [40]. In this regard, the TUGT could be used to discriminate between individuals who are at risk of falling and those who are not in community-dwelling 50–70-year-old subjects, at least in Korea.
In contrast to the TUGT time, the OLST alone was not independently associated with the rate of falling. However, younger subjects in the highest quartile for both measures were more likely to have fallen than those in the highest quartile for the TUGT alone. This finding suggests that combining the OLST with the TUGT time results in improved prediction of fall risk in subjects younger than 70 years. It has been suggested that static balance is maintained with advancing age until significant functional declines occur, whereas losses in dynamic balance tend to occur much earlier. Dynamic balance tests stress the balance control systems more; therefore, greater losses in balance are typically observed during these types of tests [13]. This difference might be related to the association of the OLST and the TUGT time with the incidence of osteoporosis and falls, respectively.
We found that women with a previous fracture were 1.68 times more likely to be in the highest quartile for the OLST compared with women with no history of fracture during the past 2 years. Some studies have suggested that the OLST might be associated with previous fractures. A longitudinal case-cohort study reported that individuals with a hip, arm, or clinical spinal fracture showed declines in the OLST compared with individuals with no fracture [41]. The Romberg test, which includes the OLST, can discriminate between women with and without previous fractures [11]. Women with a previous fracture would be expected to have poorer balance than those with no history of fracture, as the OLST provides information about balance [18, 19]. There are several possible explanations for the relationship between a history of fracture and the OLST. First, fear of falling because of an earlier fall could lead to physical inactivity and impaired balance and postural sway [42]. Second, the fracture-associated muscles might atrophy because of prolonged bed rest or inactivity, leading to impaired balance [12]. A shorter OLST has been associated with higher rates of future fracture. Two cohort studies demonstrated that the OLST was useful for assessing the risk of hip fracture risk in 351 women living in Sweden (aged 69–79 years) [43] and in 261 Caucasian women living in Finland (mean age, 59.1 ± 2.9 years) [44]. To our knowledge, no study has reported an association between the OLST and fracture risk in Asian women. The risk of future hip, wrist, and vertebral fracture is increased by the occurrence of various types of previous fractures [45, 46]. The gap between the time of a previous fracture and the measurement of physical performance in our study was modest (2 years or less). Therefore, it could be postulated that a worse OLST is associated with an increased fracture risk in Asian women.
There are several strengths of the present study. First, this was a population-based study with a large sample size that included both genders and two age groups (younger than 70 years, and 70 years or older). Second, we evaluated four criteria together: BMD, physical performance, falls, and previous fractures. There are a number of limitations that should be considered when interpreting the results. The cross-sectional design limited any attempt to determine the causal directions of the identified associations. Next, the fracture and fall data were retrospectively collected and were not confirmed through medical records or X-rays. Nonetheless, although the positive predictive value depends on the site and severity of the fracture, the validity of self-reported fractures is generally high [47]. Finally, the results of the study may not apply to other ethnicities because the cohort included only Asians.
In summary, this study suggested which performance measures could predict the risk of osteoporosis, falls, and fractures in Korean subjects. The OLST, which measures static balance, was associated with the incidence of osteoporosis and the occurrence of a previous fracture. In contrast, the time from the TUGT, which measures dynamic balance, was associated with the incidence of falling in subjects younger than 70 years. Therefore, the OLST could be used to predict the risk of osteoporosis and fracture, and the TUGT time could be used to predict fall risk. Additionally, the OLST and TUGT measures can be combined to give more accurate predictions of the risk of falling or of osteoporosis.
References
Johnell O, Kanis J (2005) Epidemiology of osteoporotic fractures. Osteoporos Int 16(Suppl 2):S3–S7
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726–1733
Lee J, Lee S, Jang S, Ryu OH (2013) Age-related changes in the prevalence of osteoporosis according to gender and skeletal site: the Korea National Health and Nutrition Examination Survey 2008–2010. Endocrinol Metab (Seoul) 28:180–191
Jang S, Park C, Jang S, Yoon H-K, Shin CS, Kim D-Y, Ha Y-C, Lee S-S, Choi HJ, Lee Y-K, Kim B-T, Choi J-Y (2010) Medical service utilization with osteoporosis. Endocrinol Metab (Seoul) 25:326–339
Choi HJ, Shin CS, Ha YC, Jang S, Jang S, Park C, Yoon HK, Lee SS (2012) Burden of osteoporosis in adults in Korea: a national health insurance database study. J Bone Miner Metab 30:54–58
Nguyen T, Sambrook P, Kelly P, Jones G, Lord S, Freund J, Eisman J (1993) Prediction of osteoporotic fractures by postural instability and bone density. BMJ 307:1111–1115
Taaffe DR, Simonsick EM, Visser M, Volpato S, Nevitt MC, Cauley JA, Tylavsky FA, Harris TB (2003) Lower extremity physical performance and hip bone mineral density in elderly black and white men and women: cross-sectional associations in the Health ABC Study. J Gerontol A Biol Sci Med Sci 58:M934–M942
Albrand G, Munoz F, Sornay-Rendu E, DuBoeuf F, Delmas PD (2003) Independent predictors of all osteoporosis-related fractures in healthy postmenopausal women: the OFELY study. Bone 32:78–85
Lord SR, Menz HB, Tiedemann A (2003) A physiological profile approach to falls risk assessment and prevention. Phys Ther 83:237–252
Shin H, Panton LB, Dutton GR, Ilich JZ (2011) Relationship of physical performance with body composition and bone mineral density in individuals over 60 years of age: a systematic review. J Aging Res 2011:191896
Gerdhem P, Ringsberg KA, Akesson K (2006) The relation between previous fractures and physical performance in elderly women. Arch Phys Med Rehabil 87:914–917
Khazzani H, Allali F, Bennani L, Ichchou L, El Mansouri L, Abourazzak FE, Abouqal R, Hajjaj-Hassouni N (2009) The relationship between physical performance measures, bone mineral density, falls, and the risk of peripheral fracture: a cross-sectional analysis. BMC Public Health 9:297
Takeshima N, Islam MM, Rogers ME, Koizumi D, Tomiyama N, Narita M, Rogers NL (2014) Pattern of age-associated decline of static and dynamic balance in community-dwelling older women. Geriatr Gerontol Int 14:556–560
Persad CC, Cook S, Giordani B (2010) Assessing falls in the elderly: should we use simple screening tests or a comprehensive fall risk evaluation? Eur J Phys Rehabil Med 46:249–259
Lee K, Lee S, Song C (2013) Whole-body vibration training improves balance, muscle strength and glycosylated hemoglobin in elderly patients with diabetic neuropathy. Tohoku J Exp Med 231:305–314
Lee SH, Kwon HS, Park YM, Ha HS, Jeong SH, Yang HK, Lee JH, Yim HW, Kang MI, Lee WC, Son HY, Yoon KH (2014) Predicting the development of diabetes using the product of triglycerides and glucose: the Chungju Metabolic Disease Cohort (CMC) study. PLoS One 9:e90430
Jonsson E, Seiger A, Hirschfeld H (2004) One-leg stance in healthy young and elderly adults: a measure of postural steadiness? Clin Biomech (Bristol, Avon) 19:688–694
Carlsson H, Rasmussen-Barr E (2013) Clinical screening tests for assessing movement control in non-specific low-back pain. A systematic review of intra- and inter-observer reliability studies. Man Ther 18:103–110
Padgett PK, Jacobs JV, Kasser SL (2012) Is the BESTest at Its Best? A Suggested Brief Version Based on Interrater Reliability, Validity, Internal Consistency, and Theoretical Construct. Phys Ther 92:1197–1207
Steffen TM, Hacker TA, Mollinger L (2002) Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys Ther 82:128–137
Podsiadlo D, Richardson S (1991) The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39:142–148
Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K, Park C, Kim DH (2007) Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr 61:1435–1441
Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, Simonsick EM, Tylavsky FA, Visser M, Newman AB (2006) The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 61:1059–1064
Makovey J, Naganathan V, Sambrook P (2005) Gender differences in relationships between body composition components, their distribution and bone mineral density: a cross-sectional opposite sex twin study. Osteoporos Int 16:1495–1505
Frost HM (2004) A 2003 update of bone physiology and Wolff’s law for clinicians. Angle Orthod 74:3–15
Furrer R, van Schoor NM, de Haan A, Lips P, de Jongh RT (2014) Gender-specific associations between physical functioning, bone quality, and fracture risk in older people. Calcif Tissue Int 94:522–530
Karkkainen M, Rikkonen T, Kroger H, Sirola J, Tuppurainen M, Salovaara K, Arokoski J, Jurvelin J, Honkanen R, Alhava E (2009) Physical tests for patient selection for bone mineral density measurements in postmenopausal women. Bone 44:660–665
Daly RM, Bass SL (2006) Lifetime sport and leisure activity participation is associated with greater bone size, quality and strength in older men. Osteoporos Int 17:1258–1267
Verbrugge LM, Jette AM (1994) The disablement process. Soc Sci Med 38:1–14
Sun W, Watanabe M, Tanimoto Y, Kono R, Saito M, Hirota C, Kono K (2009) Assessment of the best gait parameter in relation to bone status in community-dwelling young-old and old-old women in Japan. Arch Gerontol Geriatr 49:158–161
Zhu K, Devine A, Lewis JR, Dhaliwal SS, Prince RL (2011) ‘Timed up and go’ test and bone mineral density measurement for fracture prediction. Arch Intern Med 171:1655–1661
Tan BK, Price RI, Briffa NK, Dhaliwal SS, Day RE, Singer KP (2008) Assessment of osteoporotic fracture risk in community settings: a study of post-menopausal women in Australia. Health Soc Care Community 16:621–628
Sakai A, Toba N, Takeda M, Suzuki M, Abe Y, Aoyagi K, Nakamura T (2009) Association of unipedal standing time and bone mineral density in community-dwelling Japanese women. Osteoporos Int 20:731–736
Lin MR, Hwang HF, Hu MH, Wu HD, Wang YW, Huang FC (2004) Psychometric comparisons of the timed up and go, one-leg stand, functional reach, and Tinetti balance measures in community-dwelling older people. J Am Geriatr Soc 52:1343–1348
Shumway-Cook A, Brauer S, Woollacott M (2000) Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther 80:896–903
Sletvold O, Tilvis R, Jonsson A, Schroll M, Snaedal J, Engedal K, Schultz-Larsen K, Gustafson Y (1996) Geriatric work-up in the Nordic countries. The Nordic approach to comprehensive geriatric assessment. Dan Med Bull 43:350–359
American Geriatrics Society, British Geriatrics Society, American Academy of Orthopaedic Surgeons Panel on Falls Prevention (2001) Guideline for the prevention of falls in older persons. J Am Geriatr Soc 49:664–672
Schoene D, Wu SM, Mikolaizak AS, Menant JC, Smith ST, Delbaere K, Lord SR (2013) Discriminative ability and predictive validity of the timed up and go test in identifying older people who fall: systematic review and meta-analysis. J Am Geriatr Soc 61:202–208
Nordin E, Lindelof N, Rosendahl E, Jensen J, Lundin-Olsson L (2008) Prognostic validity of the Timed Up-and-Go test, a modified Get-Up-and-Go test, staff’s global judgement and fall history in evaluating fall risk in residential care facilities. Age Ageing 37:442–448
Ganz DA, Bao Y, Shekelle PG, Rubenstein LZ (2007) Will my patient fall? JAMA 297:77–86
Greendale GA, DeAmicis TA, Bucur A, Bretsky P, Rowe JW, Reuben DB, Seeman T (2000) A prospective study of the effect of fracture on measured physical performance: results from the MacArthur Study–MAC. J Am Geriatr Soc 48:546–549
Scheffer AC, Schuurmans MJ, van Dijk N, van der Hooft T, de Rooij SE (2008) Fear of falling: measurement strategy, prevalence, risk factors and consequences among older persons. Age Ageing 37:19–24
Lundin H, Saaf M, Strender LE, Nyren S, Johansson SE, Salminen H (2014) One-leg standing time and hip-fracture prediction. Osteoporos Int 25:1305–1311
Karkkainen M, Rikkonen T, Kroger H, Sirola J, Tuppurainen M, Salovaara K, Arokoski J, Jurvelin J, Honkanen R, Alhava E (2008) Association between functional capacity tests and fractures: an eight-year prospective population-based cohort study. Osteoporos Int 19:1203–1210
Eastell R, Reid DM, Compston J, Cooper C, Fogelman I, Francis RM, Hay SM, Hosking DJ, Purdie DW, Ralston SH, Reeve J, Russell RG, Stevenson JC (2001) Secondary prevention of osteoporosis: when should a non-vertebral fracture be a trigger for action? QJM 94:575–597
Morosano ME, Menoyo I, Caferra DA, Sanchez A, Tomat MF, Bocanera R, Pezzotto SM, Masoni AM (2011) Vulnerability of healthy vertebrae in patients with and without previous vertebral fracture. Bone 48:820–827
Honkanen K, Honkanen R, Heikkinen L, Kroger H, Saarikoski S (1999) Validity of self-reports of fractures in perimenopausal women. Am J Epidemiol 150:511–516
Acknowledgments
This work was supported by a research grant from the Investigator-Initiated Studies Program of Merck & Co., Korea. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors thank all the survey personnel and the officers in Chungju Health Center for continued support.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Lim, Y., Kim, K., Ko, SH. et al. Gender- and age-group-specific associations between physical performance and bone mineral density, falls, and osteoporotic fractures in Koreans: the Chungju Metabolic Disease Cohort study. J Bone Miner Metab 34, 336–346 (2016). https://doi.org/10.1007/s00774-015-0674-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-015-0674-2