
Abstract
Summary
The need for simple self-assessment tools is necessary to predict women at high risk for developing osteoporosis. In this study, tools like the IOF One Minute Test, Fracture Risk Assessment Tool (FRAX), and Simple Calculated Osteoporosis Risk Estimation (SCORE) were found to be valid for Palestinian women. The threshold for predicting women at risk for each tool was estimated.
Purpose
The purpose of this study is to evaluate the validity of the updated IOF (International Osteoporosis Foundation) One Minute Osteoporosis Risk Assessment Test, FRAX, SCORE as well as age alone to detect the risk of developing osteoporosis in postmenopausal Palestinian women.
Methods
Three hundred eighty-two women 45 years and older were recruited including 131 women with osteoporosis and 251 controls following bone mineral density (BMD) measurement, 287 completed questionnaires of the different risk assessment tools. Receiver operating characteristic (ROC) curves were evaluated for each tool using bone BMD as the gold standard for osteoporosis.
Results
The area under the ROC curve (AUC) was the highest for FRAX calculated with BMD for predicting hip fractures (0.897) followed by FRAX for major fractures (0.826) with cut-off values ˃1.5 and ˃7.8%, respectively. The IOF One Minute Test AUC (0.629) was the lowest compared to other tested tools but with sufficient accuracy for predicting the risk of developing osteoporosis with a cut-off value ˃4 total yes questions out of 18. SCORE test and age alone were also as good predictors of risk for developing osteoporosis. According to the ROC curve for age, women ≥64 years had a higher risk of developing osteoporosis. Higher percentage of women with low BMD (T-score ≤−1.5) or osteoporosis (T-score ≤−2.5) was found among women who were not exposed to the sun, who had menopause before the age of 45 years, or had lower body mass index (BMI) compared to controls. Women who often fall had lower BMI and approximately 27% of the recruited postmenopausal Palestinian women had accidents that caused fractures.
Conclusions
Simple self-assessment tools like FRAX without BMD, SCORE, and the IOF One Minute Tests were valid for predicting Palestinian postmenopausal women at high risk of developing osteoporosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a disease that causes progressive loss of bone mass and strength with significant morbidity and mortality worldwide. Once osteoporosis has rendered bones brittle and weak, minor injuries and trauma can cause bone lesions and major fractures [1]. Osteoporosis affects women more than men, and its worldwide prevalence is very high; one-third of all women and one fifth of all men over the age of 50 years will suffer from osteoporosis-related fractures in their lifetimes [2–4]. The risk of osteoporotic fractures is higher than the combined risk of breast, ovarian, and womb cancers [5, 6]. The total number of hip fractures in men and women in 1990 has been estimated to 338,000 and 917,000 respectively, with a total of 1.26 million. Assuming no change in age- and sex-specific incidence, the number of hip fractures was estimated to double to 2.6 million by the year 2025, and 4.5 million by the year 2050. The highest predicted burden being in the USA and North Europe, the lowest in Latin America and Africa, and the intermediate in Asia [7]. With modest assumptions concerning secular trends, the number of hip fractures could range between 7.3 and 21.3 million by the year 2050. The major demographic changes will occur in Asia. In 1990, 26% of all hip fractures occurred in Asia, whereas this figure could rise to 37% in 2025 and to 45% in 2050. Consequently, the socioeconomic impact of hip fractures will increase markedly throughout the world, particularly in Asia, indicating an urgent need to develop preventive strategies, especially in the developing countries [7, 8]. The available data showed close parallels between rising rates of hip fractures and urbanization [9]. The variation in hip fracture risk based on Fracture Risk Assessment Tool (FRAX) and fracture probability between countries was greater than tenfold [10]. All osteoporotic fractures result in increased mortality and morbidity, but hip fractures are considered to be the most serious with a threefold higher risk of death with most deaths occurring in the first 3–6 months following the incidence [11, 12].
Lifestyle trends including calcium intake and physical activity account for approximately 20% of the variance in peak bone mass [13]. People who enter adulthood with low peak bone mass are at greatest risk of developing osteoporosis and associated fractures [14]. Medical treatment interventions are unable to reverse the effects of osteoporosis completely. Therefore, encouraging healthy behaviors may maximize maintaining peak bone mass and slow bone loss. Health strategies designed to maximize peak bone mass and reduce bone loss later in life should include prevention through health education, health promotion, and awareness programs [15].
In Palestine, the prevalence of osteoporosis in postmenopausal women at the lumbar spine, femoral neck, and total hip was 24, 14, and 29.7%, respectively, and 41% at any site with inadequate awareness of osteoporosis [16]. These findings affirm that osteoporosis is considerably widespread and emphasize the need for new diagnostic tools to increase the ability to identify subjects at high risk to develop osteoporosis and related fractures later in life. For this purpose, the IOF One Minute Osteoporosis Risk Assessment Test (10 questions in its early version) was introduced by the International Osteoporosis Foundation (IOF) and updated in 2013 to include 18 questions for women and translated into several languages [17]. Several published data studied the validation of the early version (10 questions) of the One Minute Test [18, 19], but none has been reported to evaluate the validity of the updated version (18 questions for women). A FRAX has been developed and validated by the World Health Organization (www.shef.ac.uk/frax/) to predict an individual 10-year risk of hip or major osteoporotic fractures. These findings were used in the development of guidelines for diagnosis and treatment in Lebanon [20], in various Middle East and worldwide populations [21–27]. This tool was based on individual patient models that integrated the risks associated with clinical risk factors as well as BMD at the femoral neck [28]. Another tool used to detect the risk of developing osteoporosis is the Simple Calculated Osteoporosis Risk Estimation (SCORE) [29] as well as age alone [30].
The present investigation focused on evaluating the validity of the One Minute Test, SCORE test as well as age alone to predict the risk of developing osteoporosis in Palestinian postmenopausal women. Our results were compared to the Dual Energy X-ray Absorptiometry (DXA) technology, the gold standard for the diagnosis of osteoporosis worldwide. In addition, our findings were compared to FRAX in order to evaluate the 10-year probability of developing hip or major osteoporotic fractures.
Materials and methods
In this cross-sectional study, 382 postmenopausal women (age ≥45 years) were recruited using cluster sampling method from various clinics and community centers from the central part of the West Bank region of Palestine. All recruited subjects were not previously diagnosed with bone problems or suffered from bone-related health complications. None of the subjects were using any prescription drugs or food supplements (including vitamin D and calcium) that might affect their general bone status.
Bone mineral density of the femoral neck, lumbar spine, and total hip for all participants were assessed using Lunar Prodigy DXA Densitometer (GE Medical Systems). The diagnosis of osteoporosis was made in reference to the WHO criteria for the diagnosis of osteoporosis (T-score ≤−2.5 in at least one of the three sites: total hip, femoral neck, and lumbar L1-L4 spine). Combined NHANES (ages 20–30)/Lunar (ages 20–40) Femur and AP Spine Reference Caucasian Population Database was used. Trained field workers administered the questionnaires to 287 women (83 osteoporotic and 204 controls) for the FRAX and SCORE as well as for the adapted Arabic version of the One Minute Test which includes 18 questions. All women answered yes to age above 45 years and no to drinking alcohol. All study subjects were requested to sign a consent form declaring their agreement to participate in the study.
Statistical analysis. IBM SPSS® v23 and MedCalc® v15.8 were utilized for data entry and analysis including descriptive statistics and Pearson correlations, independent sample t test, Fisher’s exact test, Chi-square test, binary logistic regression, and receiver operating characteristic (ROC) curves. A p value less than 0.05 was considered statistically significant. The ROC curves were evaluated for several variables based on the cut-off value that maximizes both sensitivity and specificity of the test. Differences in the AUCs of the different ROC curves were estimated using StataCorp LP stata ® v14.1.
Results
Table 1 shows the frequency differences between normal and osteoporotic women in their answers to questions in the One Minute Test. The absence of sun exposure (OR = 2.82), menopause before the age of 45 years (OR = 2.43), and being underweight (OR = 5.00) were found to be risk factors for osteoporosis. This indicated that the risk for osteoporosis was five times higher in women being underweight compared to women having normal or overweight. The risk of osteoporosis was two to three times higher in women with no sun exposure or had menopause before the age of 45 years compared to normal women. The rest of the 16 variables tested in Table 1 had no significant effect on the risk for osteoporosis.
Women with menopause before the age of 45 years were older and had significantly lower BMD (total hip, femoral neck, and lumbar spine) and lower BMI compared to women without interruption of menstrual cycle. However, both osteoporosis and control groups were obese with BMI higher than 30 kg/m2. Women who often fall were older compared to controls (64.3 vs. 61.3 years, p = 0.005, respectively) and women who had accidents that caused fractures had lower BMI (30.9 vs. 32.5 kg/m2) and were taller (159 vs. 156 cm) compared to controls. Approximately, 27% of osteoporosis and normal women had accidents that caused fractures. Women not exposed to the sun had significantly lower mean BMD at the three sites (total hip, femoral neck, and lumbar spine) compared to women exposed to the sun and mean BMI was slightly but significantly lower (31.0 vs. 32.5 kg/m2, p = 0.026).
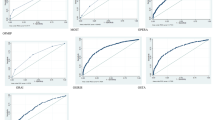
The ROC curves for the One Minute Test, FRAX, SCORE, and age alone for predicting future risk of developing osteoporosis (T-score ≤ −2.5) and fractures are depicted in Fig. 1. All tested tools were valid for detecting the risk of low BMD (T-scores ≤−2.5, −2.0, and −1.5). Table 2 shows the AUC for FRAX calculated with BMD for predicting 10-year risk of hip fractures was significantly higher than the AUC for FRAX calculated with BMD for predicting 10-year risk of major fractures (p < 0.0001). Both FRAX tools with BMD were significantly higher than the FRAX calculated without BMD, SCORE, One Minute Test, or age alone. The AUC for the One Minute Test (0.629) was significantly the lowest compared to other tested tools but with sufficient accuracy (95% CI 0.556 to 0.701, p = 0.0008) for predicting the risk of developing osteoporosis with a cut-off value ˃4 total yes questions out of 18. The FRAX with BMD for both hip and major fractures had the highest LR+ (6.17 and 4.42) and the higher the value of LR+, the greater the information value of the diagnostic test. For each tool, the reported cut-off value is the best value that maximizes both sensitivity and specificity of that tool. The highest sensitivity of 100% was reported for FRAX (hip fracture with BMD) with 83.8% specificity at the cut-off value of >1.5. On the other hand, the highest specificity of 84.1% among the tested tools was found in FRAX (major fracture with BMD) accompanied with a sensitivity of 70.4% at the cut-off value of >7.8. SCORE test and age alone were also as good predictors of developing osteoporosis as the One Minute Test and FRAX without BMD. According to the ROC curve for age, women of 64 years and older had a higher risk of developing osteoporosis.

Receiver operating characteristic curves of osteoporosis and fracture risk assessment tools
Pearson correlation of total yes count in the One Minute Test was negatively correlated with BMD (correlation coefficient, r = −0.178, −0.172, −0.186, p = 0.003, for total hip, femoral neck, and lumbar spine, respectively) and with BMI (r = −0.183, p = 0.002).
Table 3 shows the number of women identified by different tools to be at high risk for developing osteoporosis or fractures and require their BMD measured. Optimum threshold values estimated by FRAX without BMD, SCORE, One Minute Test, and age were used to assess the number of women at risk as compared to the actual number of women at risk (diagnosed with osteoporosis). In addition, two FRAX threshold values, 9.3% used by the US Preventive Services Task Force (USPSTF) [31] and 10% suggested by researchers in Lebanon, a Middle Eastern country, [20] were compared to the optimum threshold values obtained in our subjects. Of the 83 osteoporotic postmenopausal Palestinian women diagnosed by BMD, 57 (41.3%) were identified by FRAX without BMD at the threshold for 10-year risk of a major osteoporotic fracture estimated by our data (˃6.4%). However, 138 women were identified to be at high risk and require BMD measurement. Using the recommended threshold of ≥9.3%, only 74 women were identified to require BMD measurement, and 35 (47.3%) of them had osteoporosis. A threshold of ≥10%, identified 61 women to be at high risk and require BMD measurement and 30 (49.2%) of them had osteoporosis. Eight women were identified by SCORE to be at high risk with 43 (53.8%) had osteoporosis. Age also identified 180 out of 382 women to be at high risk, 91 (50.6%) had osteoporosis.
Discussion
Screening tools including the One Minute Test, FRAX, and SCORE for identifying Palestinian postmenopausal women at high risk of developing low bone density, osteoporosis, or fractures were evaluated and validated. Based on ROC curves, the best risk assessment tool was the FRAX with BMD. However, FRAX without BMD, SCORE, the One Minute Test, and age alone had nearly similar accuracy in identifying postmenopausal Palestinian women at high risk that require their BMD to be measured. Our findings are in agreement with a published report from Denmark that showed similar evaluation results of these tools in women above the age of 40 years [30]. The threshold for FRAX without BMD estimated for the Palestinian postmenopausal women (˃6.4% for major fractures) is nearly similar to the threshold (≥6.8%) estimated by Pecina et al. [31] in a retrospective study at the Mayo Clinic. The estimated threshold of FRAX without BMD (˃6.4% for major fractures) identified nearly the same number of women with osteoporosis as the One Minute Test (57 vs. 62 out of 83). It is worth mentioning that the number of false positive was higher in the One Minute Test compared to FRAX without BMD (102 vs. 81 out of 203). This means that more women will be asked to have their BMD examined based on the One Minute Test. FRAX at higher threshold including ≥9.3 and ≥10% will reduce the number of women required for BMD examination. It will also increase the number of women who are at high risk but not identified by these thresholds (48 and 53, respectively), compared to 26 out of 83 with osteoporosis for threshold ˃6.4%. Concurrently, these thresholds will reduce the number of non-osteoporotic women (164 and 172, respectively), compared to 122 for the same threshold. The threshold of ≥9.3% has low sensitivity (42.1%) in agreement with similar previous studies [23, 31].
Several observations from this study support the validation of the use of updated One Minute Test to identify postmenopausal women at high risk. The negative correlation between the total yes count from the 18 questions and BMD was statistically significant although not strong (r = −0.172 to −0.186 at the three tested sites). Further evaluation of the One Minute Test using the ROC curve indicated that it could be used to predict subjects at risk with low BMD. The risk of having low BMD predicted by the One Minute Test is for women with BMD at least 1.5 standard deviation or more below the mean BMD of healthy women and was not sensitive for women with T-score ≤−1. Based on the ROC curve, the LR+ and Youden Index J, a threshold of more than four yes answers out of 18 questions was the minimum number for the test to be sensitive. However, a LR+ of 1.34 is less than satisfactory; therefore, the power of One Minute Test to rule in the disease was weak but significant to be used with PPV of 70.8% for ruling in low BMD.
Using the USPTF-recommended FRAX threshold of ≥9.3% for major fracture without BMD detected 74 women to be at high risk, 35 of them were postmenopausal women with osteoporosis, and 8 (23%) were below 65 years. Using the recommended FRAX threshold of ˃6.4% calculated from our data increased the number of predicted osteoporotic women from 35 to 57 but also increased the number of total women at high risk who require BMD measurement from 74 to 138. Of the 57 osteoporotic women, 15 (23%) were below 65 years; however, lowering the FRAX threshold to 3.8% increased the sensitivity to 90% and thus increased the number of diagnosed postmenopausal women to 75, where 24 (32%) of them were below 65 years. However, at this threshold, the total number of women at high risk that require BMD measurement increased to 216.
Our data showed that underweight women had five times the probability of getting osteoporosis and experienced more bone fractures. Our findings were consistent with the reports that showed obesity is protective and BMI is positively correlated with BMD while women with osteoporosis had lower mean BMI compared to non-osteoporotic women [32, 33].
In conclusion, simple osteoporosis risk assessment tools like the updated One Minute Test, SCORE, FRAX, and even age by itself are valid tools at different thresholds. FRAX without BMD has a good sensitivity at threshold ˃6.4% that can identify high-risk postmenopausal women for developing osteoporosis and 10-year risk for developing major osteoporotic fractures. The One Minute Test also has a good sensitivity at a threshold of ˃4 and could be used to identify high-risk Palestinian postmenopausal women whereas SCORE has low sensitivity at the optimum threshold of ˃20.5.
References
Kanis JA et al (1994) The diagnosis of osteoporosis. J Bone Miner Res 9(8):1137–1141
Melton LJ 3rd et al (1998) Bone density and fracture risk in men. J Bone Miner Res 13(12):1915–1923
Melton LJ 3rd et al (1992) Perspective. How many women have osteoporosis? J Bone Miner Res 7(9):1005–1010
Kanis JA et al (2000) Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int 11(8):669–674
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359(9319):1761–1767
Cummings SR, Black DM, Rubin SM (1989) Lifetime risks of hip, Colles’, or vertebral fracture and coronary heart disease among white postmenopausal women. Arch Intern Med 149(11):2445–2448
Gullberg B, Johnell O, Kanis JA (1997) World-wide projections for hip fracture. Osteoporos Int 7(5):407–413
Dhanwal DK et al (2011) Epidemiology of hip fracture: worldwide geographic variation. Indian J Orthop 45(1):15–22
Ballane G et al (2014) Secular trends in hip fractures worldwide: opposing trends east versus west. J Bone Miner Res 29(8):1745–1755
Kanis JA et al (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23(9):2239–2256
Black DM, Rosen CJ (2016) Postmenopausal osteoporosis. N Engl J Med 374(21):2096–2097
Panula J et al (2011) Mortality and cause of death in hip fracture patients aged 65 or older: a population-based study. BMC Musculoskelet Disord 12:105
Rubin LA et al (1999) Determinants of peak bone mass: clinical and genetic analyses in a young female Canadian cohort. J Bone Miner Res 14(4):633–643
Hansen MA et al (1991) Role of peak bone mass and bone loss in postmenopausal osteoporosis: 12 year study. BMJ 303(6808):961–964
Mark S, Link H (1999) Reducing osteoporosis: prevention during childhood and adolescence. Bull World Health Organ 77(5):423–424
Abd-Alhameed I, Saba E, Darwish H (2010) Prevalence and awareness of osteoporosis among postmenopausal Palestinian women. Arch Osteoporos 5(1):111–118
http://www.iofbonehealth.org/. IOF ONE-MINUTE OSTEOPOROSIS RISK TEST.
Povoroznjuk V, Dzerovich N, Karasevskaya T (2007) Evaluation of validity of IOF’s one-minute osteoporosis risk test for postmenopausal women. Calcif Tissue Int 80(Suppl. 1):168–169
Povoroznjuk VV, Dzerovich N, Karasevskaya T (2007) Evaluation of validity of IOF’s one-minute osteoporosis risk test for postmenopausal women. Osteoporos Int 18(Suppl. 1):227
Chakhtoura, M., R. Baddoura, and G. El-Hajj Fuleihan. Executive summary—Lebanese FRAX-based osteoporosis guidelines 2013. 2013; Available from: https://www.aub.edu.lb/fm/cmop/downloads/diagnosis-trt.pdf
Marques A et al (2015) The accuracy of osteoporotic fracture risk prediction tools: a systematic review and meta-analysis. Ann Rheum Dis 74(11):1958–1967
Bonaccorsi G et al (2015) Assessment of fracture risk in a population of postmenopausal Italian women: a comparison of two different tools. Calcif Tissue Int 97(1):50–57
Bansal S et al (2015) US Preventative Services Task Force FRAX threshold has a low sensitivity to detect osteoporosis in women ages 50-64 years. Osteoporos Int 26(4):1429–1433
Cheung E et al (2014) Possible FRAX-based intervention thresholds for a cohort of Chinese postmenopausal women. Osteoporos Int 25(3):1017–1023
Leslie WD et al (2013) Selection of women aged 50-64 yr for bone density measurement. J Clin Densitom 16(4):570–578
Gonzalez-Macias J et al (2012) Probability of fractures predicted by FRAX(R) and observed incidence in the Spanish ECOSAP study cohort. Bone 50(1):373–377
Kanis JA et al (2014) Worldwide uptake of FRAX. Arch Osteoporos 9:166
Lydick E et al (1998) Development and validation of a simple questionnaire to facilitate identification of women likely to have low bone density. Am J Manag Care 4(1):37–48
Rubin KH et al (2013) Comparison of different screening tools (FRAX(R), OST, ORAI, OSIRIS, SCORE and age alone) to identify women with increased risk of fracture. A population-based prospective study. Bone 56(1):16–22
Pecina JL et al (2016) Comparison of clinical risk tools for predicting osteoporosis in women ages 50-64. J Am Board Fam Med 29(2):233–239
Poiana C et al (2015) Prevalent osteoporotic fractures in 622 obese and non- obese menopausal women. J Med Life 8(4):462–466
Clark GR, Duncan EL (2015) The genetics of osteoporosis. Br Med Bull 113(1):73–81
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Kharroubi, A., Saba, E., Ghannam, I. et al. Evaluation of the validity of osteoporosis and fracture risk assessment tools (IOF One Minute Test, SCORE, and FRAX) in postmenopausal Palestinian women. Arch Osteoporos 12, 6 (2017). https://doi.org/10.1007/s11657-016-0298-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-016-0298-8